
Abstract
Traumatic brain injury (TBI) has been recently recognized as a common cause of pituitary dysfunction. However, there are not sufficient numbers of prospective studies to understand the natural history of TBI induced hypopituitarism. The aim was to report the results of five years' prospective follow-up of anterior pituitary function in patients with mild, moderate and severe TBI. Moreover, we have prospectively investigated the associations between TBI induced hypopituitarism and presence of anti-hypothalamus antibodies (AHA) and anti-pituitary antibodies (APA). Twenty five patients (20 men, five women) were included who were prospectively evaluated 12 months and five years after TBI, and 17 of them also had a third-year evaluation. Growth hormone (GH) deficiency is the most common pituitary hormone deficit at one, three, and five years after TBI. Although most of the pituitary hormone deficiencies improve over time, there were substantial percentages of pituitary hormone deficiencies at the fifth year (28% GH, 4% adrenocorticotropic hormone [ACTH], and 4% gonadotropin deficiencies). Pituitary dysfunction was significantly higher in strongly AHA- and APA-positive (titers ≥1/16) patients at the fifth year. In patients with mild and moderate TBI, ACTH and GH deficiencies may improve over time in a considerable number of patients but, although rarely, may also worsen over the five-year period. However in severe TBI, ACTH and GH status of the patients at the first year evaluation persisted at the fifth year. Therefore, screening pituitary function after TBI for five years is important, especially in patients with mild TBI. Moreover, close strong associations between the presence of high titers of APA and/or AHA and hypopituitarism at the fifth year were shown for the first time.
Introduction
The mechanisms responsible for long-term hypopituitarism after head trauma are still unclear. Recent prospective clinical studies have demonstrated that pituitary function improves over time in a significant number of patients but it may also rarely worsen over the one-year and three-year period after TBI. 3,5,9 The possible mechanisms underlying the recovery and worsening of the pituitary function remain to be clarified. Nevertheless, the dynamic changes in the pituitary function suggest that head trauma may trigger an ongoing process, such as autoimmunity. 10 Supporting this hypothesis, significant associations between hypopituitarism after head trauma and anti-hypothalamus antibodies (AHA) and/or anti-pituitary antibodies (APA) have been demonstrated in two recent studies. 11,12 However, these significant associations need confirmation in longer term studies and prospective follow-up of the presence of AHA and APA.
To the best of our knowledge, no study has been reported in which the pituitary function of the same patients has been prospectively investigated for more than three years after head trauma. Therefore in this article, we report the results of five-year prospective follow-up of anterior pituitary function in patients with mild, moderate, and severe TBI, aiming to define the natural history of post-traumatic hypopituitarism. Moreover, we have prospectively investigated the associations between TBI-induced hypopituitarism and presence of AHA and APA.
Methods
Fifty-two TBI patients admitted between 2003–2005 to the neurosurgery intensive care unit (NICU) in Erciyes University Medical School Hospital were evaluated 12 months after TBI; these results were previously published. 5 The three-year follow-up results of 30 of these 52 patients also were previously published. 9 At the fifth year after TBI, 52 patients who had already been evaluated were invited to participate in the current study but 27 of them chose not to. In the present study, 25 patients (20 males, 5 females; ages 36.8±2.1 years) were included who were prospectively evaluated 12 months after TBI and five years (median 60 months; minimum, 50 months; maximum, 72 months) after TBI; 17 patients also had a third-year evaluation (Table 1). The study was approved by the Local Committee on Ethics.
GCS, Glasgow Coma Score on admission; TSH, thyroid-stimulating hormone; FSH, follicle-stimulating hormone; LH, luteinizing hormone; ACTH, adrenocorticotropic hormone; GH, growth hormone; M, male; N, normal pituitary hormone; D, deficient pituitary hormone; F, female.
The level of consciousness of the patients was evaluated by the Glasgow Coma Scale (GCS) as soon as the patient was admitted to the NICU. A score of 13–15 is considered mild TBI, 9–12 moderate TBI, and ≤8 severe TBI. 13 None of the patients had history of any known pituitary disorder and none of the patients were taking medications that affect hypothalamo-pituitary function.
Basal hormonal evaluation
All patients underwent a basal hormonal evaluation at one, three, and five years of TBI. Blood samples were taken between 8.00–9.00 h. Before the blood samples were collected, no patients received glucocorticoids, dopamine, ketoconazole or calcium channel blockers. Basal hormone levels including free triiodothyronine, free thyroxine (fT4), thyroid-stimulating hormone (TSH), prolactin, cortisol, adrenocorticotropic hormone (ACTH), follicle-stimulating hormone (FSH), luteinizing hormone (LH), insulin-like growth factor 1 (IGF-I), growth hormone (GH), and total and free testosterone in males or estradiol in females were measured. Menstrual history also was obtained in female patients. The diagnosis of gonadotropin (FSH/LH), TSH, GH and ACTH deficiencies were made as previously reported. 5
In males, gonadotropin deficiency was defined by both basal total and free testosterone levels below the normal range (total testosterone <134 ng/dL and free testosterone <11.5 pg/mL) in the presence of normal or low values of gonadotropins. In premenopausal females, gonadotropin deficiency was defined by a serum estradiol level of less than 11 pg/mL, with the presence of an inappropriately low serum gonadotropin concentration. In postmenopausal women, gonadotropin levels in the premenopausal range were used to diagnose the deficiency. 14,15
TSH deficiency was defined by low serum fT4 level (<8 pg/mL) without appropriate elevation in serum TSH. 14,15
Evaluation of the somatotropic and corticotropic functions by dynamic tests
During the follow-up period, none of the patients were on hormone replacement therapy and the patients with hormone deficiencies at the first and third year evaluations were closely monitored. Particularly, the ACTH-deficient patients were informed that they might need steroid replacement to avoid adrenal crisis during an intercurrent illness or surgery. They were strongly advised to present to the emergency clinic in the case of hypotension, nausea, or any other symptom related to the adrenal insufficiency, and these ACTH-deficient patients were periodically evaluated during the follow-up. None of them had any significant illness or surgery during this period.
An ACTH deficiency was suggested when the basal cortisol level was below 7 μg/dL and it was confirmed by low-dose ACTH stimulation test. A low-dose ACTH stimulation test was performed by using 1 μg tetracosartin (Synacthen, Novartis Pharma, Lyon, France). Intravenous (IV) and serum samples were obtained for cortisol measurement at baseline () and at 30, 60, 90, and 120 min. A peak cortisol level lower than 18 μg/dL was considered to be ACTH deficiency. 16
GH deficiency was investigated by the growth-hormone-releasing hormone (GHRH)+growth hormone releasing hexapeptide (GHRP-6) test in all patients. For the combined test, a peak value of ≤10 μg/L was considered to be GH deficiency, while a peak higher than 20 μg/L was considered a normal response. GH peak values between 11 and 19 μg/L were considered to be uncertain. After having basal sample at -15 min, the combined test (IV bolus injection of 1 μg/kg of GHRH [GRF 1–29 NH2, GerefSerono, Madrid, Spain], immediately followed by an IV injection of 1 μg/kg of GHRP-6 [His- DTrp-Ala-Trp-DPhe-Lys-NH2; Clinalfa Laufelfinger, Switzerland])was administered at 0 min, and further samples obtained at 15, 30, 45, 60, 90, and 120 min of injection. 17,18
We defined GH deficiency in the uncertain group (GH peak values between 11 and 19 μg/L after combined test) by performing glucagon stimulation test (1 mg intramuscular Glucagon; Novonordisk, Bagsvaerd, Denmark). The subjects in the uncertain group according to GHRH +GHRP-6 tests were considered normal if the GH responses exceeded the cut-off value after glucagon test. To establish the normal GH response to glucagon stimulation, the cut-off value was estimated from the GH responses of 22 healthy controls as previously described. 19 Therefore, we considered a cut-off of 1.18 μg/L as a normal GH response after glucagon administration.
The same analytic methods were performed and the same commercial kits were used throughout the five-year follow-up as described previously. 5,9
Analytical methods for hormonal measurements
Serum GH levels were measured by using immunoradiometric assay with a commercial kit (DSL, Webster, Texas), intra-assay and inter-assay coefficients of variation (CV) were 3.1% and 5.9%, respectively and GH standards were calibrated according to the World Health Organization reference standard 88/624. IGF-I level was measured by immunoradiometric assay after formic acid-ethanol extraction; intra-assay and inter-assay CV were 3.4% and 8.2%, respectively.
All the other serum hormones, except TSH (IRMA), ACTH (IRMA) and estradiol (chemiluminescent assay), were measured by using radioimmunoassay with commercial kits as we published previously. 5,9
Evaluation of anti-hypothalamus antibodies (AHA) and anti-pituitary antibodies (APA)
AHA and APA were investigated in 25 patients at the fifth year of TBI (17 of these patients had AHA and APA evaluation prospectively at the third year and fifth years of TBI; Table 1) and in 50 sex/age-matched healthy subjects.
APA and AHA were evaluated by simple indirect immunofluorescence method on cryostat sections of young baboon pituitary glands supplied by Halifax spa (Polverara, Pordenone, Italy) and of young baboon hypothalamus (Biomedis s.r.l., Porto San Giorgio, Italy), respectively, as previously described. 20 –22 In particular, fluorescein isothiocyanate conjugated with goat antihuman immunoglobulins was used to detect the presence of APA and AHA; they were considered positive starting at dilution of 1:8.
The collaborators performing the immunological evaluation were blinded to the pituitary deficiency status of the patients. The control group was recruited from healthy volunteers from Turkey who had no meningitis history, no previous hospitalization history due to head trauma, and no other known causes of pituitary dysfunction; moreover, none of them had an individual or familial history of autoimmune diseases.
Statistical Analysis
Statistical analysis was performed by using the SPSS 15.0 program (SPSS, Inc., Chicago, IL). All data were subjected to the Kolmogrov–Smirnov test for normality and are presented as mean±SEM. The differences between the groups were compared by Mann-Whitney U test. The categorical data were shown as percentages and compared to χ2 test. Odds ratios (ORs) and 95% confidence intervals (CI) were calculated; p<0.05 was considered statistically significant.
Results
Pituitary hormone deficiencies at one, three, and five years after TBI
Twenty-five patients were evaluated at the first and fifth year after TBI, and 17 of them had a third year evaluation (Table 1). According to initial GCS, 16 patients (64%) had mild TBI, five (20%) had moderate TBI, and four (16%) had severe TBI.
Percentages of the pituitary hormone deficiencies throughout the follow-up period are summarized in Figure 1. At one year of TBI, one of 25 patients (4%) had TSH deficiency, and at the third and fifth years, none of the patients had TSH deficiency. One year of TBI, two of 25 patients (8%) had FSH/LH deficiency. These two patients were not evaluated at the third year (Table 1) and none of the 17 evaluated patients had FSH/LH deficiency at the third year. At the fifth year of TBI, one of the patients who had gonadotropin deficiency at the first year recovered (patient 19, Table 1) and one of 25 patients (4%) had FSH/LH deficiency. At the first year, four of 25 patients had ACTH deficiency (16%); three of them recovered at the third year (patients 4, 10, and 12; Table 1) and one (patient 21) was not screened at the third year. Therefore, all the evaluated 17 patients at the third year were normal regarding ACTH deficiency. At the fifth year, one of 25 patients (4%) had ACTH deficiency and this patient (patient 24; Table 1) had new-onset (normal at the first year) ACTH deficiency. At the first year of TBI, 11 of 25 patients (44%) had GH deficiency. At the third year, four of the 17 evaluated patients (23%) had GH deficiency, and at the fifth year of TBI seven of 25 (28%) had GH deficiency. After individual evaluation of GH deficiency one year to five years after TBI (Table 1), six of 11 (54.5%) GH-deficient patients at the first year recovered after five years of TBI and GH deficiency detected at the fifth year in two patients was new onset.
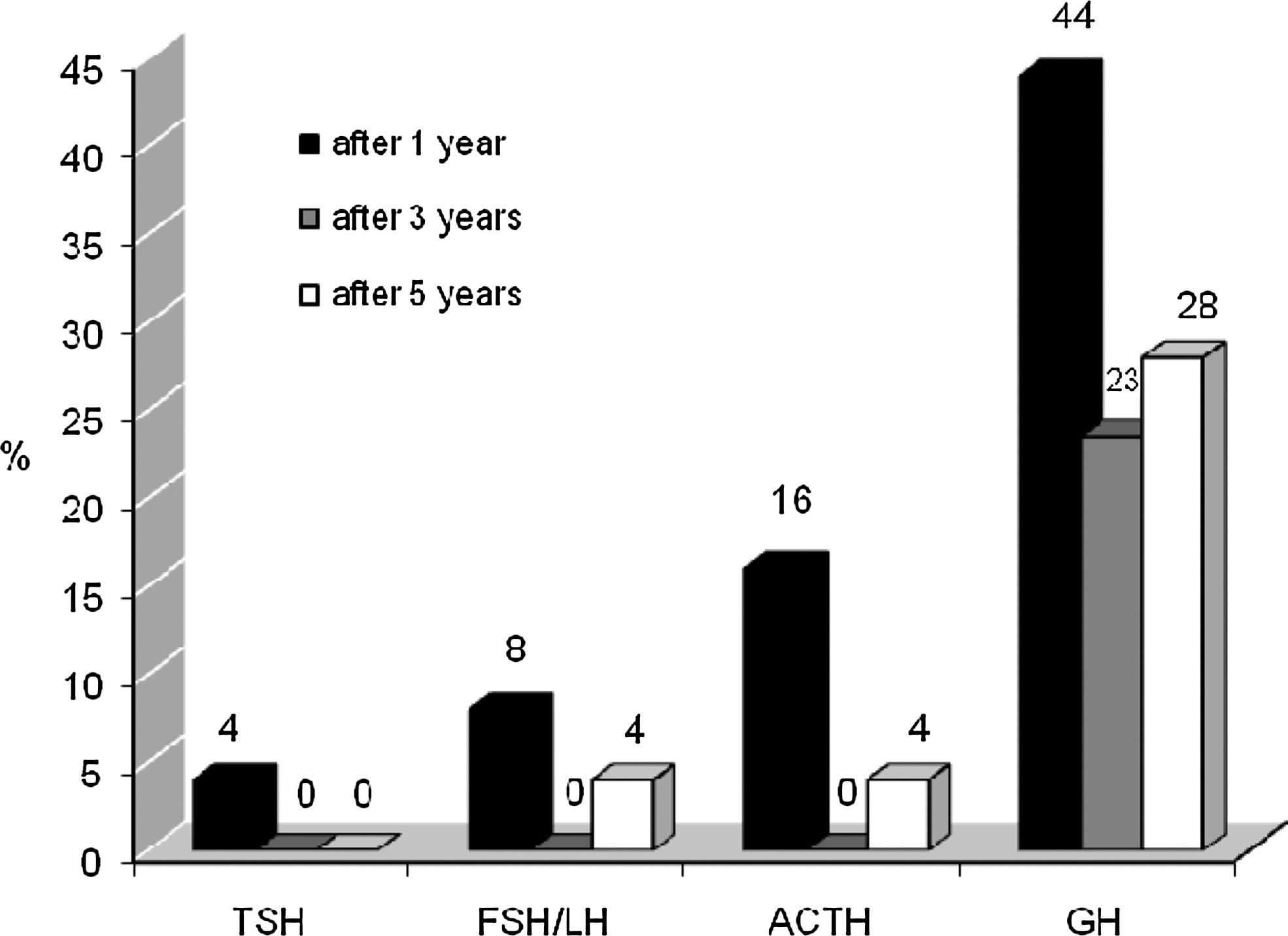
Percentages of pituitary hormone deficiencies at one, three, and five years after TBI.
Overall, all the percentages of the pituitary hormone deficiencies decreased significantly throughout the follow-up period (Figure 1), and at the end of the fifth year the most common pituitary hormone deficiency was GH deficiency. At the fifth year of TBI, six of 25 patients had isolated GH deficiency, one of 25 patients had isolated ACTH deficiency, and one patient had combined FSH/LH and GH deficiencies (Table 1). With regard to GH and ACTH axes, the dynamic hormonal changes (mainly recovery, but rarely new onset deficiency) were still present throughout five years in patients with mild and moderate TBI. However, in patients with severe TBI, the hormonal status at the first year persisted at the third and fifth years (Table 1).
Comparisons between GH-deficient and GH-sufficient patients
Comparisons between GH-deficient and GH-sufficient patients at the fifth year of TBI were summarized in Table 2.
TBI, traumatic brain injury; GH, growth hormone; GCS: Glasgow Coma Score on admission; BMI, body mass index; IGF-I, insulin-like growth factor 1; LDL, low-density lipoprotein; HDL, high-density lipoprotein; GST, Glucagon Stimulation Test.
There were no significant differences between age and initial GCS between the groups. The mean first-year IGF-I and body mass index (BMI) levels were similar in GH-deficient and GH-sufficient patients at the fifth year of TBI (p>0.05). However, BMI was significantly higher in GH-deficient patients at the fifth year of TBI, compared with GH-sufficient patients (p<0.05; Table 2). The mean waist circumference was substantially higher in GH-deficient patients than in GH-sufficient patients at the fifth year but the difference did not reach statistical significance (p=0.07). Additionally, total cholesterol and triglyceride levels were significantly higher in GH-deficient patients at the fifth year of TBI, compared with GH-sufficient patients (p<0.05; Table 2). Mean IGF-I level at the fifth year was significantly lower in GH-deficient patients; and mean peak GH levels after the dynamic tests (GHRH+GHRP-6 and glucagon stimulation) were significantly lower in GH-deficient patients, compared with GH-sufficient patients (p<0.05; Table 2).
Evaluation of anti-hypothalamus antibodies (AHA) and anti-pituitary antibodies (APA)
The behaviors of AHA and APA in all patients at the fifth year of TBI and normal controls are depicted in Figures 2A and 2B, respectively. Immunostaining of AHA-positive and AHA-negative sera, and APA-positive and APA-negative sera are depicted in Figures 3A and 3B, respectively. Individual titers of APA and AHA are listed in Table 1.

Anti-hypothalamus antibodies in traumatic brain injury (TBI) patients at the third year and fifth year after TBI, and in 50 normal controls.
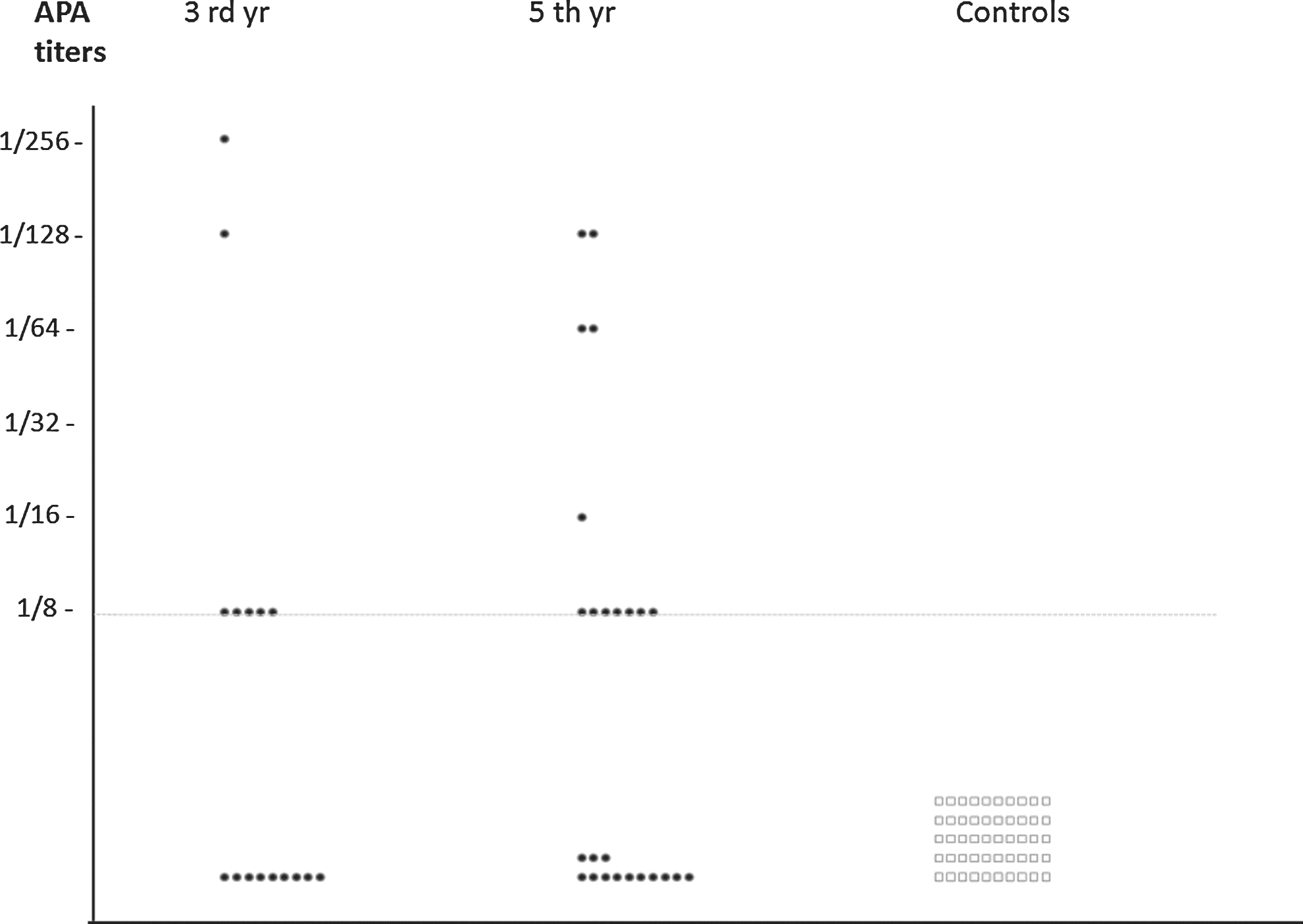
Anti-pituitary antibodies in traumatic brain injury (TBI) patients at the third year and fifth year after TBI, and in 50 normal controls.
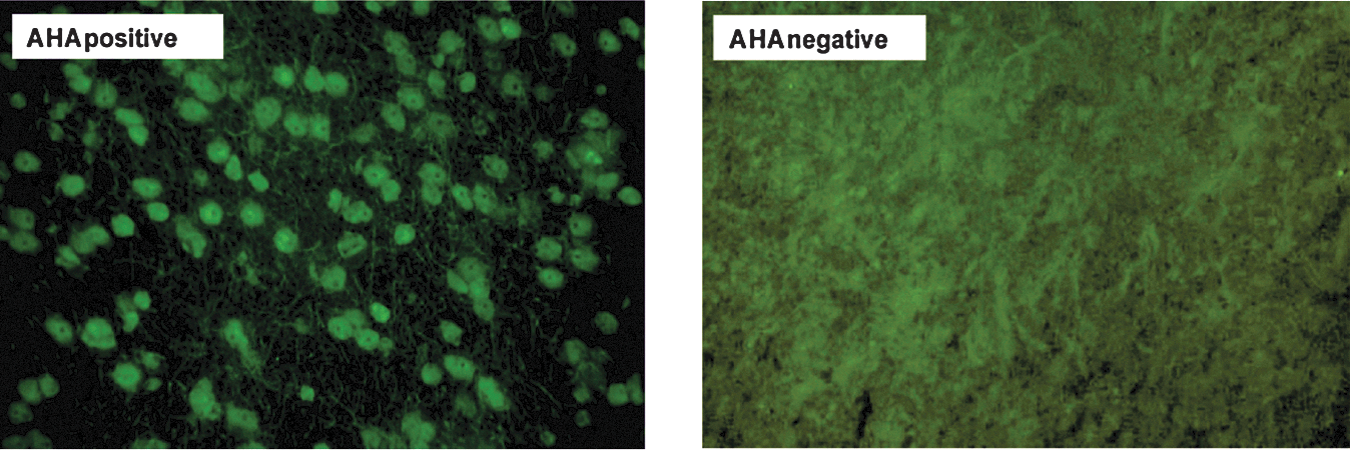
Serum sample positive antibodies to hypothalamic cells detected by immunofluorescence in a traumatic brain injury patient at the fifth year, in comparison with a negative control serum.
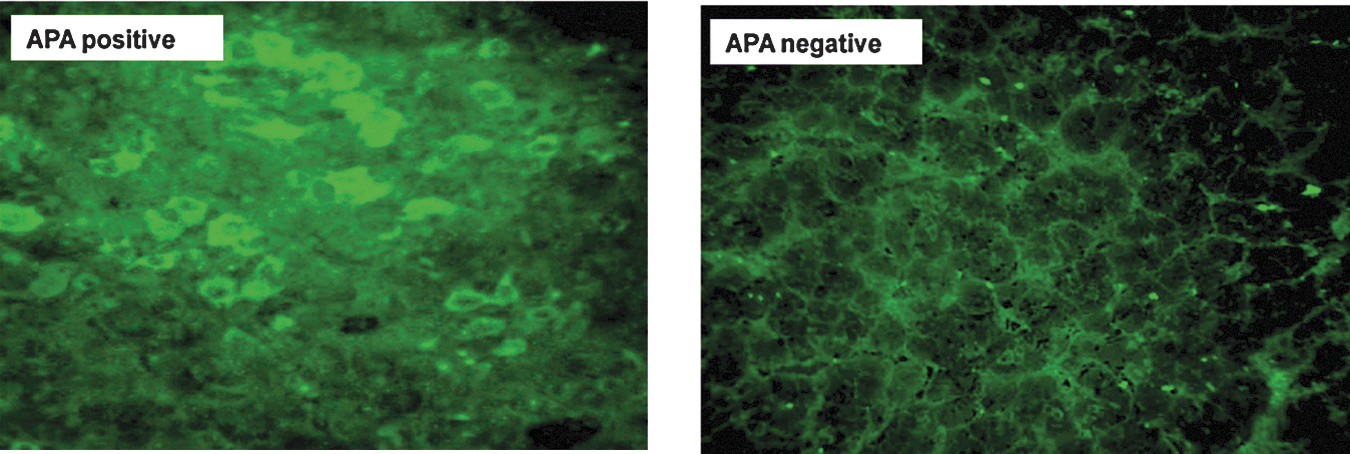
Serum sample positive antibodies to pituitary cells detected by immunofluorescence in a traumatic brain injury patient at the fifth year, in comparison with a negative control serum.
At the fifth year of TBI, AHA were detected in 15 of 25 (60%) patients but in none of the controls. Among the 15 AHA-positive patients, eight (53.3%) were weakly positive (titer=1/8), while seven (46.7%) were strongly positive (titer ranging from 1/16 to 1/64; Table 1; Figure 2A). Although there was no any significant association between AHA positivity and development of pituitary dysfunction at the fifth year of TBI (p>0.05), pituitary dysfunction was significantly higher in strongly AHA-positive patients (71.4%), compared with AHA-negative and weakly AHA-positive (titer=1/8) patients (16.7%; Table 1; p=0.008). The corresponding OR was 5.3 (95% CI 1.3, 21.7), showing that the relative chance of having hypopituitarism after TBI increased five times when the patient had strong AHA positivity.
At the fifth year of TBI, APA were detected in 12 of 25 (48%) patients, but in none of the controls. Among the 12 APA positive patients, seven (58.3%) were weakly positive (titer=1/8), while five (41.7%) were strongly positive (titer ranging from 1/16 to 1/128; Table 1; Fig. 3A). Although there was no any significant association between APA positivity and development of pituitary dysfunction at the fifth year of TBI (p>0.05), pituitary dysfunction was significantly higher in strongly APA-positive patients (80%), compared with APA negative and weakly APA positive (titer=1/8) patients (20%; Table 1; p=0.01). The corresponding OR was 8.5 (95% CI 1.2, 64.3), showing that the relative chance of having hypopituitarism after TBI increased eight-fold when the patient had strong APA positivity.
When we compared the fifth year APA and AHA levels according to trauma severity (16 patients with mild TBI versus nine patients with moderate and severe TBI), there were no significant differences in both mean APA and AHA titers between mild and moderate/severe TBI patients (p>0.05).
AHA and APA could prospectively be evaluated in 17 patients at the third year and fifth year of TBI (Table 1). In all who had persistent pituitary hormone deficiency from the third year to the fifth year (patients 2, 14, and 17; Table 1) strong positivity of APA and/or AHA was present at the third year. Moreover, in the patient who recovered from the third year to the fifth year (patient 2; Table 1), APA and AHA were negative at the third year. Pituitary dysfunction at the fifth year was significantly more severe in patients with strongly positive APA and/or AHA in the third year (100%), compared with patients with negative and weakly positive APA and/or AHA in the third year (7.7%; Table 1; p=0.0001).
Discussion
The present study is the first prospective follow-up study from a single center evaluating anterior pituitary function at one, three, and five years after TBI. It has been clearly demonstrated that although most of the pituitary hormone deficiencies improve over time, there is a substantial percentage of pituitary hormone deficiencies—GH deficiency in particular—five years after TBI. Moreover, close associations between autoimmunity and TBI-induced hypopituitarism at the fifth year were shown.
Until now, six prospective studies evaluating pituitary function 12 months after TBI were published from different centers. 3 –8 In the majority of these studies GH deficiency was the most frequent hormone deficiency, ranging from 10% to 30%. Additionally, in four of these six prospective studies, it has been demonstrated that pituitary function improves over 12 months' time in a considerable number of patients but, although rarely, also may worsen (new onset hormone deficiencies). 3 –5,8 In the single three-year prospective study published, we have reported that GH deficiency (23.3%) was the most common pituitary hormone deficit three years after TBI. The dynamic hormonal changes (mainly recovery and rarely new hormone deficiencies) have continued in patients with mild and moderate TBI during three years' follow-up. 9 In the present study, we found GH deficiency in 28% of the patients at the fifth year of TBI, which is the most common pituitary hormone deficiency, and most of the patients had isolated GH deficiency. ACTH and FSH/LH deficiencies were the second most common (4%) hormone deficiencies. Consistent with a previous third-year prospective study, 9 dynamic hormonal changes were continued throughout the five-year follow-up period (Table 1). In patients with mild and moderate TBI, ACTH and GH deficiencies may improve over time in a considerable number of patients; however, although rarely, also may worsen over the five-year period. But in severe TBI, ACTH and GH status of the patients detected at the first-year evaluation persisted at the fifth year. The possible pathogenesis of the ongoing dynamic hormonal changes will be discussed later in this section. Nevertheless, from the clinical point of view based on the present findings, it is tempting to speculate that in mild TBI patients, screening the pituitary function after TBI for five years is crucial. But it is difficult to make similar recommendations in moderate and severe TBI due to the limited number of patients in the present study. Future long-term prospective studies including large numbers of moderate and severe TBI patients need to be done.
GH/IGF-I axis plays an important role in the regulation of body composition and lipid metabolism throughout life. 23,24 Abnormal body composition (increased fat mass, especially in the abdominal region, increased waist/hip ratio, increased BMI) and impaired lipid profile have been reported in adults with a low IGF-I level due to GH deficiency. 23,25,26 In our previous three-year prospective TBI study, there was no significant difference in BMI between GH-deficient and GH-sufficient patients. 9 In the present study, BMI was significantly higher in GH-deficient patients, and although the difference did not reach a significant level, waist circumference was substantially higher in GH-deficient patients, compared with GH-sufficient patients. The mean IGF-I levels at the first year of TBI were similar in GH-deficient and GH-sufficient patients (Table 2) but mean IGF-I level at the fifth year of TBI was significantly lower in GH-deficient patients. This finding clearly suggests that IGF-I levels decrease over time in GH-deficient patients. With regard to lipid profile, significantly high total cholesterol and triglyceride levels were present in GH-deficient patients five years after TBI. Based on the present findings, we can speculate that body composition and lipid profile changes due to GH deficiency become clinically important long-term after persistent GH deficiency. However, there is not enough data in the literature regarding the effects of GH replacement therapy on metabolic changes due to TBI induced GH deficiency.
Several mechanisms have been suggested for the hypothalamic-pituitary dysfunction due to TBI, including hypoxic insult or direct mechanical injury to the hypothalamus, pituitary stalk, or the pituitary gland; compression from hemorrhage, edema, or increased intracranial pressure; and vascular injury to the hypothalamus or the pituitary gland. 27,28 However, none of these mechanisms have been proven by experimental and clinical studies, and the pathogenesis of pituitary dysfunction long-term after head trauma is still unclear. Recent prospective clinical studies have demonstrated that pituitary function improves over time in a significant number of patients but it may also rarely worsen over the one- and three-year period after TBI. 3,5,9
The present study also revealed that dynamic hormonal changes still continue until five years after TBI, particularly in patients with mild TBI. The dynamic changes in the pituitary function suggest that head trauma may trigger an ongoing process, such as autoimmunity. 10 In an experimental study, naturally-occurring immunoglobulin G autoantibodies against dying neurons in the injured brain have been detected in adult rats following a cortical lesion, and it has been proposed that autoantibody binding may participate in the phagocytosis and removal of the injured neurons. 29 Furthermore, autoreactive antibodies against neurons and basal lamina have been found in serum following experimental TBI in rats. The authors concluded that presence of autoreactive antibodies against neurons and basal lamina after TBI could play a pathogenic role in the delayed neuron degeneration. 30 However, in these experimental studies, the effects of head trauma on hypothalamo-pituitary region and the presence of APA and/or AHA have not been investigated. Regarding human studies, presence of APA and AHA has been shown in patients with Sheehan's syndrome even many years after the onset of hypopituitarism. The authors concluded that an autoimmune process involving both the hypothalamus and pituitary gland may contribute to late pituitary dysfunction. 22 In a collaborative cross-sectional study, we demonstrated previously the presence of APA in TBI patients three years after head trauma. In that study, the pituitary dysfunction development ratio was significantly higher in APA-positive patients (titer≥1/8; 46.2%), compared with APA-negative ones (12.5%; p=0.04). 11 In the present study, there were significant associations (p≤0.01) between strong AHA and APA positivity (titer ranging from 1/16 to 1/128) and development of hypopituitarism. These findings clearly suggest that titers of the autoantibodies become more important with longer duration after head trauma, and autoimmunity may play a role in the pathogenesis of TBI-induced hypopituitarism.
Additionally, most of the patients with persistent pituitary insufficiency had higher titers of AHA and/or APA at three and five years of TBI (Table 1), and most of the patients who recovered had negative or low titers (titer=1/8) of AHA and/or APA. These findings may imply that dynamic hormonal changes might be closely related to the presence or absence of the possible ongoing processes, such as autoimmunity and/or neuroinflammation. Future mechanistic experimental and clinical studies are warranted to clarify molecular mechanisms. Moreover, in the present study, all the patients who had strong APA and/or AHA positivity had hypopituitarism at the fifth year of TBI, suggesting that APA and AHA could be used a useful clinical screening tool predicting the pituitary damage due to head trauma. However, it is too early to propose these antibodies for routine clinical practice and more clinical studies with large number of patients need to be done.
In the present study, we have used the same dynamic hormonal tests, screening protocol, laboratories, and commercial hormonal kits throughout the five-year period. However, the most important limitation of our study was low numbers of patients, especially in moderate and severe TBI groups.
In conclusion, our data demonstrated that GH deficiency is the most common pituitary hormone deficit at one, three, and five years after TBI. Although most of the pituitary hormone deficiencies improve over time, there are substantial percentages of pituitary hormone deficiencies at the fifth year. In patients with mild and moderate TBI, ACTH and GH deficiencies may improve over time in a considerable number of patients but, although rarely, may also worsen over the five-year period. However, in severe TBI, ACTH, and GH status of the patients at the first year evaluation persisted at the fifth year. Therefore, screening the pituitary function after TBI for five years is important, especially in patients with mild TBI. Moreover, close strong associations between the presence of high titers of APA and/or AHA and hypopituitarism at the fifth year were shown for the first time.
Footnotes
Author Disclosure Statement
No competing financial interests exist.