
Abstract
The present study tested a hypothesis that early identification of injury severity with quantitative magnetic resonance imaging (MRI) provides biomarkers for predicting increased seizure susceptibility and epileptogenesis after traumatic brain injury (TBI). TBI was induced by lateral fluid percussion injury (FPI) in adult rats. Quantitative T2, T1ρ, and diffusion were assessed with MRI at 9 days, 23 days, or 2 months post-TBI in the perilesional cortex, thalamus, and hippocampus. Seizure susceptibility was assessed at 12 months after TBI using the pentylenetetrazol seizure-susceptibility test. At 9 and 23 days post-TBI, a change in T1ρ of the perilesional cortex showed the greatest predictive value for increased seizure susceptibility at 12 months post-TBI [area under the curve (AUC), 0.929 and 0.952, respectively; p<0.01]. At 2 months post-TBI, Dav in the thalamus was the best of the biomarkers analyzed (AUC, 0.988; p<0.05). The highest predictive value of all biomarkers was achieved by combining the measurement of Dav in the perilesional cortex and the thalamus at 2 months post-TBI (AUC, 1.000; p<0.01). Our results provide proof-of-concept evidence that clinically relevant MRI biomarkers predict increased seizure susceptibility after experimental TBI.
Introduction
Approximately 10–20% of acquired epilepsy is caused by traumatic brain injury (TBI), 4 with the 30-year cumulative incidence of epilepsy being 2.1% for mild, 4.2% for moderate, and 16.7% for severe injuries. 5 Among TBI patients presenting with penetrating head injury (e.g., bullet wounds), up to 53% develop epilepsy. In approximately 80% of cases, epilepsy develops within 2 years, but the elevated risk extends for longer than 10 years post-TBI. 6 Similarly, experimental studies in animal models have shown that only a subpopulation of rats and mice with different types of TBI develop epilepsy during the follow-up. 7
Because epilepsy develops in only a subpopulation of animals and patients, and because the delay between TBI and the manifestation of epilepsy is so variable, conducting both pre-clinical and clinical trials that test antiepileptogenic treatments provides a costly challenge. To make progress, it is critical to identify biomarkers that can be used to enrich the study population to target treatment toward those with the highest likelihood of epileptogenesis. 8 So far, there are no biomarkers that predict increased susceptibility for post-traumatic epileptogenesis.
TBI induced by lateral fluid percussion injury (FPI) is an animal model widely used to investigate the mechanisms of TBI-induced brain injury and test novel, recovery-enhancing treatments. 9 At least 50% of rats with lateral FPI develop epilepsy over a 1-year follow-up, and 80% of rats show increased seizure susceptibility in the pentylenetetrazol (PTZ) test—findings that have been reproduced by many laboratories. 10 Because the severity of TBI is the most significant risk factor for post-traumatic epilepsy (PTE), we tested a hypothesis that early identification of injury severity by using quantitative T2, T1ρ, and diffusion magnetic resonance imaging (MRI) would provide diagnostic biomarkers for increased post-traumatic seizure susceptibility and epileptogenesis later in life.
This is an extended reanalysis of data presented previously. 11 Induction of TBI with lateral FPI in adult male Spague-Dawley rats (34 injured and 16 controls) and methodology for MRI have been described in detail earlier. 11,12 Dav (one third of the trace of the diffusion tensor that is an orientation-independent measure of water diffusion), T1p (a longitudinal relaxation in the rotating frame, which can be assumed to be similar to T1 relaxation in the very low magnetic field, thus probing interaction between water and macromolecules in the tissue), and T2 were analyzed from cortical, thalamic, and hippocampal data sets measured at clinically relevant time points (9, 23, and 60 days post-TBI). The following four cortical areas were analyzed both ipsi- and contralaterally: (1) somatosensory cortex (S1); (2) dorsal perilesional cortex; (3) ventral perilesional cortex; and (4) perirhinal cortex (PRh; Fig. 1A). In addition, we assessed Dav, T1ρ, and T2 in the thalamus and hippocampus bilaterally. Regions of interest (ROIs) were manually outlined in T2-weighted images and transferred to T2 maps and diffusion maps. We also reanalyzed data from a different cohort of animals 11 that was imaged at 7 months post-TBI. In all rats in both cohorts, seizure susceptibility was assessed once at 12 months post-TBI using the PTZ test under continuous video electroencephalography (EEG) monitoring. 11 All animal procedures were approved by the animal ethics committee of the Provincial Government of Southern Finland and carried out in accord with the guidelines of the European Community Council Directives (86/609/EEC).
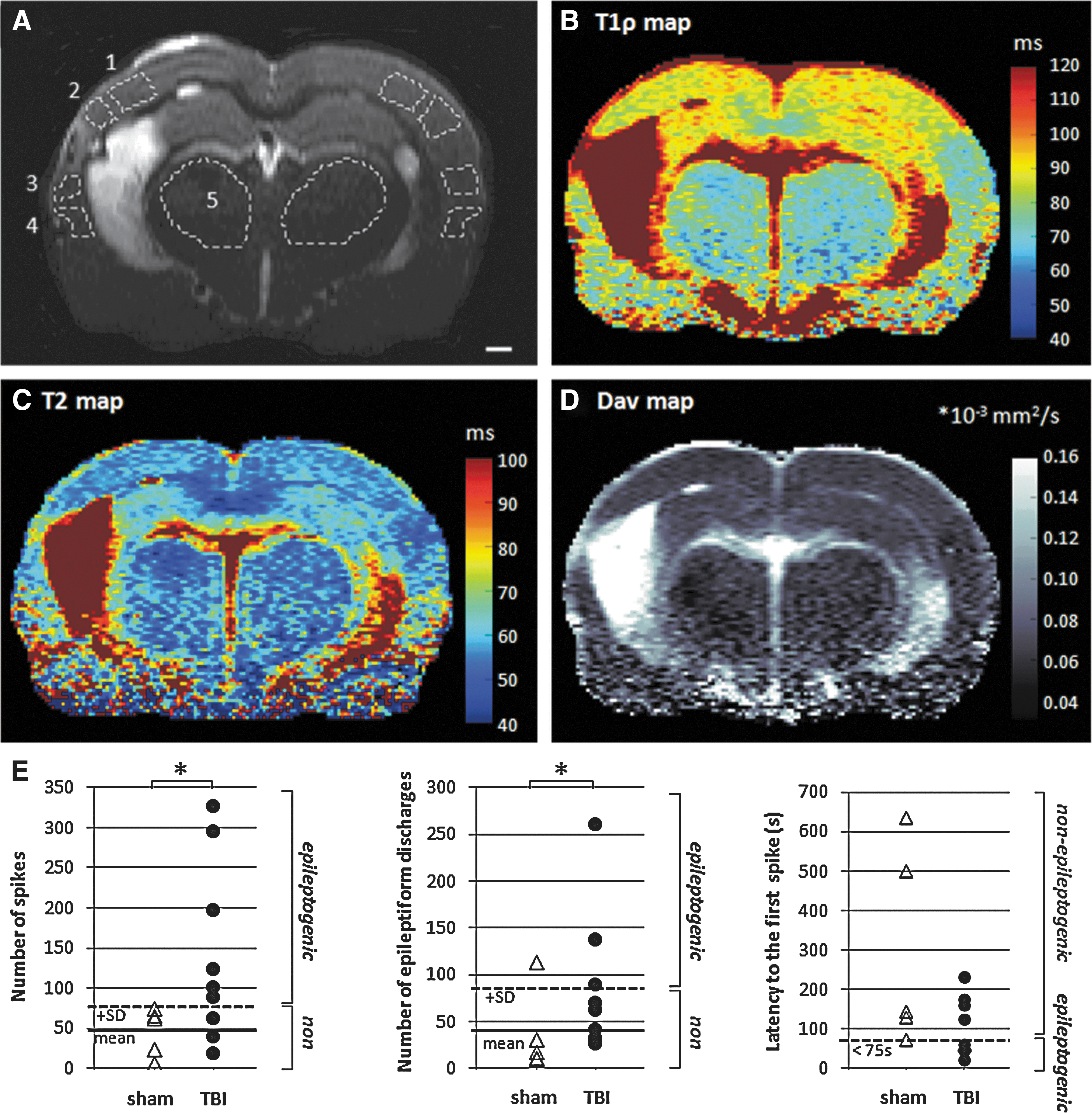
Coronal slice from the center of the brain after lateral fluid-percussion–induced traumatic brain injury (TBI), imaged at 23 days post-TBI. (
Statistical analysis was done using SPSS software (version 19; IBM SPSS Statistics, Armonk, NY). The total number of spikes counted during the 60 min after PTZ injection was used for dividing animals with TBI into “unchanged seizure susceptibility” (uSS) versus “increased seizure susceptibility” (iSS) groups in ROC (receiver operating characteristic) analysis. In the uSS group, the number of spikes was found to be lower, and in the iSS group, the number of spikes was higher than the mean plus 1 standard deviation of controls (Fig. 1E). ROC curves for epileptogenesis were drawn for MRI findings that showed correlations (Spearman's rank correlation coefficient) with the number of spikes in the PTZ test. ROC curve characteristics, including area under the curve (AUC), sensitivity, and specificity, were assessed for each MRI biomarker at different time points. Using the direction (i.e., increase or decrease) of the pathological MRI changes found as a priori knowledge, the “combined biomarkers” were created by multiplying two or three single markers. A p value<0.05 was considered significant.
Representative images and data from the PTZ test in individual animals are summarized in Figure 1. At 12 months post-TBI, 67% of rats with TBI had developed increased seizure susceptibility. Dav, T1ρ, and T2 in different brain areas at various time points after TBI are summarized in Supplementary Figure 1 (see online supplementary material at

Summary of receiver operating characteristic (ROC) for parameters assessed at 9 days, 23 days, or 2 months postinjury, which predicted increased seizure susceptibility (iSS) at 12 months post-TBI (traumatic brain injury). A diagonal line represents 50% probability for correct prognosis. Area under the curve (AUC) and sensitivity at 100% or 90% specificity are shown in Supplementary Table 1 (see online supplementary material at
Reanalysis of MRI parameters derived from the data set of Kharatishvili and colleagues
11
for the hippocampus ipsilateral to the injury showed that the following significant predictions, T1ρ at 9 days (AUC, 0.857; p<0.05) and Dav at 23 days (AUC, 0.833; p<0.05) and at 2 months (AUC, 0.881; p<0.05) post-TBI, were predictive for increased seizure susceptibility (Supplementary Table 1) (see online supplementary material at
We next assessed the magnitudes of abnormalities in different parameters that were needed to predict the development of iSS. At 9 days post-TBI, a 5% increase in T1ρ in the S1 predicted seizure susceptibility with 83% sensitivity and 71% specificity, whereas a 3% increase in T1ρ in the PRh cortex predicted seizure susceptibility with 83% sensitivity and 86% specificity. At 23 days postinjury, a 4% increase in Dav in the PRh cortex predicted epileptogenesis with 67% sensitivity and 71% specificity. At 2 months post-TBI, a 3% increase in Dav in the S1 gave 83% sensitivity and 77% specificity, whereas a 7% increase in thalamic Dav provided 100% sensitivity and 86% specificity.
This is the first proof-of-concept study to demonstrate that iSS after TBI can be predicted by using MRI biomarkers of cortical and thalamic damage. At 9 days post-TBI, a change in T1ρ of the perilesional cortex showed the greatest predictive value for iSS at 12 months post-TBI. Interestingly, the greatest predictability was found when the cortical analysis was done in the S1 or in the PRh, which reside approximately 1 mm from the lesion core, but not in the cortex immediately adjacent (within 1 mm) to the lesion core, where the greatest changes in MRI parameters occur. It is noteworthy that the cortex nearest to the lesion core contains the tissue that is going to degenerate during the first few weeks postinjury. At later time points (23 days or 2 months post-TBI), the changes in Dav in the S1 and PRh were the best biomarkers for predicting iSS. In contrast, assessment of T2 in cortical ROIs had no predictive value. The best biomarkers at 9 and 23 days post-TBI were those combining T1ρ analysis of the S1 and PRh. The most accurate of all biomarkers was a combinatory biomarker calculated from the Dav in the ipsilateral S1 and thalamus assessed at 2 months post-TBI, reaching 100% sensitivity and specificity. These data suggest that the damage to the perilesional cortex and the thalamus and, consequently, to thalamocortical pathways contributes to the generation of the ictogenic network after TBI. This is in line with our observations using functional MRI in the analysis of induced seizure activity after TBI. 13
The use of the occurrence of spontaneous seizures as a “gold standard” to classify subjects into uSS and iSS groups is problematic because it would require 24/7 video EEG monitoring for a long period of time, which still could not be long enough to demonstrate the lack of epileptogenesis without dispute. Therefore, we chose to use seizure susceptibility at 12 months post-TBI as a classifier in ROC analysis. The major advantage of this approach is that seizure susceptibility can be assessed in every animal at any post-TBI time point by using a single test. The reasoning relies on the idea that an increase in seizure susceptibility precedes the development of epilepsy. Indeed, data from several laboratories using acquired epilepsy models, including status epilepticus (SE) or TBI, suggest that this is true. 14 –16 We recently demonstrated that rats with spontaneous seizures after TBI have the highest seizure susceptibility in the PTZ test. 11,17
The data obtained show that iSS can be predicted with a high sensitivity and specificity by using MRI. Because T1ρ is an established method in the experimental lab that shows much potential in human applications, and because T2 and Dav are already routine clinical MRI modalities, our results provide proof-of-concept evidence for applying MRI in search of biomarkers for post-traumatic epileptogenesis in humans. These data pave the way for subject stratification for antiepileptogenesis studies.
Footnotes
Acknowledgments
This study was supported by the Academy of Finland (to R.I., O.G., and A.P.) and the Sigrid Juselius Foundation (to A.P.).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.