
Abstract
The relationship between previous mild traumatic brain injury/injuries (MTBI) and recovery from a subsequent MTBI may be complex. The present study investigated three factors hypothesized to influence this relation: (1) the number of prior MTBIs, (2) the interval between MTBIs, and (3) the certainty level of previous MTBIs. The study design was retrospective cross-sectional. Participants (N=105) were evaluated at a concussion clinic on average 1 month after sustaining an MTBI, defined by World Health Organization diagnostic criteria. Approximately half the sample had at least one previous MTBI. Subgroups with 0, 1, or 2+ previous MTBIs did not differ in levels of current post-concussion symptom reporting on the British Columbia Post-Concussion Symptom Inventory. Time since the most recent previous MTBI was significantly associated with current post-concussion symptom reporting. This relation was best characterized as logarithmic; i.e., the impact of previous MTBI(s) lessens exponentially as time elapses to a subsequent MTBI. Defining previous MTBIs with a higher certainty level (i.e., probable versus possible) was not consistently associated with greater post-concussion symptom reporting. In conclusion, participants with multiple MTBIs did not report more post-concussion symptoms than those with no history of MTBI. Previous MTBI(s), however, were associated with increased symptom reporting from a subsequent MTBI to the extent they occurred closer in time. Having one or two previous remote MTBIs was not associated with worse outcome from subsequent MTBI in this sample.
Introduction
Several variables have been hypothesized to explain the diversity in outcomes from multiple MTBIs. Perhaps the most widely considered variable is the number of previous MTBIs. At one extreme, having numerous MTBIs and subconcussive injuries (e.g., a lengthy professional boxing career) is a possible cause of dementia, 3,4 or may diminish the threshold for expression of dementia from other etiologies. 5 Incurring at least three previous sport-related concussions appears to be associated with lingering neuropsychological deficits and symptoms in some athletes. 6 –11 Most persons with a history of previous MTBI(s), however, tend to have only one to two previous injuries. 2 Some athlete studies 12 –14 but not all 15 –18 report that a second MTBI is associated with a worse outcome relative to a first-ever MTBI. Nonetheless, the threshold for the number of previous MTBIs necessary to adversely impact recovery from a subsequent MTBI is not clear. Because all of the above-reviewed evidence comes from athletes with sport-related MTBI, the clinical significance of MTBI history in other settings is especially uncertain. Trauma patients with chronic symptoms after MTBI, identified in prospective cohort studies or because they present at a clinic, may have a higher rate of previous MTBI than patients who recover well, 19,20 but several studies have found similar 21 –23 or even lower rates. 24
In addition to the number of previous MTBIs, the interval between those injuries may help explain the diversity in outcomes from repeated MTBI. 2,9 In other words, the recency of a previous MTBI may determine its clinical significance. Injuries sustained in very close succession are thought to be of particular concern, based on several lines of research. MTBI appears to induce a cascade of neurometabolic events that devote much of the brain's energy consumption to restorative and homeostatic processes. 25 Normalization of neurometabolic derangement may take several weeks. 26,27 Rat models with experimentally induced MTBI support that sustaining a second injury during this vulnerable period has synergistic deleterious effects. 28 –30 Taken together, incurring a subsequent MTBI within days to weeks of an initial MTBI may be associated with poor outcome. Although the duration between an initial and subsequent MTBI often falls within this period for competitive athletes 31,32 (but see 14 ) and deployed military personnel, 33 this might be less true for those involved in recreational sport, who on average do not incur a subsequent MTBI for at least 1 year. 34 Persons who are injured in nonsport settings may have their MTBIs spaced even further apart, on average. The neurobiologic consequences and clinical significance of repeated MTBIs spaced months to years apart are poorly understood.
Few observational studies have examined whether the interval between two MTBIs influences outcome from the second injury. In a sample of professional football players (n=160) who sustained two MTBIs on average 1 year apart (range=0 to 5 years), the interval between MTBIs did not correlate significantly with increases in symptoms from the initial to second injury. 14 In military service members (n=113) with repeated MTBIs on average 40 days apart (range 2 to 753 days), time since the previous MTBI did not alter severity indicators of the second injury (e.g., loss of consciousness duration) or healthcare utilization after the second injury. 33 In these studies, there is little evidence to support a strong linear relation between the recency of a previous MTBI and recovery from the current MTBI. A nonlinear relation remains possible; i.e., a relatively recent previous MTBI may be of disproportionate significance.
A third variable that may influence the relationship between MTBI history and outcome from subsequent MTBI is the criterion used to retrospectively identify previous MTBIs. 9,35 Research studies have, with few exceptions, 14 relied on participant self-report to elicit information about previous, often very remote, MTBIs. There are several reasons to doubt the accuracy of retrospective self-report, such as post-traumatic amnesia limiting first-hand recounts and normal forgetting processes that degrade event memory. 36 Even if accuracy is assumed, in some cases, the information provided by the patient offers less than compelling support for a diagnosis of MTBI (e.g., an unwitnessed event with an equivocal alteration in consciousness). To the extent that such a questionable injury event is considered by the researcher to constitute a previous MTBI, past studies may have underestimated the clinical significance of MTBI history. The discrepant and often not explicitly stated diagnostic criteria for previous MTBI in studies to date make this difficult to determine, further hindering our understanding of prognosis after repeated MTBI.
The purpose of this study is to determine whether the clinical significance of repeated MTBIs varies depending on (1) the number of previous MTBIs, (2) the interval between MTBIs, and (3) the certainty level of previous MTBIs in a heterogeneous sample of patients referred to a concussion clinic after MTBI. We hypothesized that: (1) there will be an exposure-response relationship between the number of previous MTBIs and current symptom reporting, (2) more recent previous MTBIs will have a stronger effect on current symptom reporting than a remote previous MTBI, and (3) self-reported injuries to the head that involved medical indicators of MTBI (“probable”) will have a stronger effect on current symptom reporting than those without these features (“possible” MTBI).
Methods
Participants
Participants were 105 persons who met World Health Organization Neurotrauma Task Force diagnostic criteria for MTBI 37 and were evaluated at a median of 32 days (M=55.2, standard deviation [SD]=59.9, interquartile range (IQR)=20 to 65, range=2 to 321) after injury. Participants were selected from a larger sample of 137 consecutive cases of physician-diagnosed TBI referred to two specialty concussion clinics within the Greater Vancouver Regional District (British Columbia, Canada)—the G.F. Strong Early Response Concussion Clinic and Fraser Health Concussion Clinic—between January 2007 and December 2009. Participants were excluded if they had a duration of post-traumatic amnesia greater than 24 hours (n=21), Glasgow Coma Scale score of less than 13 after 30 min (n=1), or missing data on the primary outcome variable (n=10). The demographic characteristics of the sample and the clinical features of their presenting MTBI are summarized in Table 1. Note that the present MTBI sample overlaps with samples reported previously. 38,39 For many patients, complete medical records were not available for review. For these patients, classification of MTBI was based on self-reported mechanism of injury, loss of consciousness (LOC), and post-traumatic confusion or post-traumatic amnesia (PTA).
SD=standard deviation.
Measures
All participants completed the British Columbia Post-Concussion Symptom Inventory (BC-PSI), a self-report measure of post-concussion symptoms. 40 Participants rated symptoms on two dimensions, frequency and intensity, over the past 2 weeks. The BC-PSI has strong internal consistency and test-retest reliability, 40,41 and has been used in numerous clinical studies. 39,42 –46 Higher scores indicate greater symptom severity. Previous studies have generated various scores from the BC-PSI. We focused on the BC-PSI total score, which is created by (1) multiplying intensity by frequency ratings for each item, (2) converting the product to a scale from 0 to 4, and (3) summing the scaled items scores from the first 13 items. This score has known psychometric properties and is least prone to skewness in clinical samples. Of note, repeating all of the below analyses with another common BC-PSI score (i.e., the number of symptoms endorsed as mild or greater) did not alter the pattern of findings.
Information regarding the participant's demographic background, pre-injury medical and psychiatric history, the day-of-injury events, and compensation-seeking status were obtained by the service coordinator using a structured interview. As part of this interview, information regarding previous MTBIs was obtained. The interviewee was first queried about previous MTBIs (“Have you ever had a concussion or mild traumatic brain injury?”). Participants were offered definitions of these terms. If the participant answered positively, the interviewer asked follow-up questions about the injury mechanism, alterations in consciousness, post-traumatic amnesia, medical treatment sought, and the timing of the injury.
Procedure
As part of a clinical intake assessment, all participants completed a battery of standardized questionnaires (that included the BC-PSI) and underwent a structured interview (described above). Previous head trauma events identified by an affirmative response to the initial query (“Have you ever had a concussion or mild traumatic brain injury?”) were further classified into probable versus possible previous MTBI. Previous head trauma events were classified as “probable” MTBI if they included an unequivocal loss of consciousness or period of post-traumatic amnesia, or admission to an emergency department for suspected concussion or MTBI. If a previous head trauma event included none of these features, or if medical records were unavailable and the participant stated that they did not know or could not recall these details, a “possible” previous MTBI was classified. Medical records were generally not available for remote previous injuries.
After potentially eligible participants completed the clinical intake assessment, their informed consent was sought to include their (de-identified) data in a research database. This research was approved by the University of British Columbia Behavioral Research Ethics Board and Fraser Health Research Ethics Board.
Results
Approximately half (52.4%) of the participants presented with their first-ever MTBI. When considering MTBI of any certain classification (i.e., probable or possible previous MTBI), 28.6% (n=30) had sustained one previous MTBI and 19.0% (n=20) had sustained two or more previous MTBIs. When considering probable previous MTBIs only, 11.4% (n=12) had one previous MTBI, and 8.6% (n=9) had two or more previous MTBIs. The time between the current and most recent previous MTBI ranged from 1 week to 55 years, with a median of 7.0 years (M=11.3, SD=13.5, IQR=2 to 13 years, range=0.02 to 55). Only two participants (1.9%) had a repeated MTBI within 2 weeks.
To determine whether the number of previous MTBIs was associated with outcome from the current MTBI, we compared subgroups with 0, 1, or 2+ previous MTBIs (i.e., combined probable and possible previous MTBIs). The group mean, standard deviations, and effect sizes are presented in Table 2. A one-way analysis of variance with a three-level independent variable (i.e., 0, 1, or 2+ previous MTBIs) and BC-PSI total score as the dependent variable was non-significant, F(2, 102)=0.486, p=0.617. Restricting prior MTBIs to “probable” classification yielded a similar null main effect, F(2, 102)=0.196, p=0.822. In summary, subgroups with 0, 1, or 2+ previous MTBIs had very similar levels of current post-concussion symptom reporting, regardless of using probable versus possible classification criteria to define previous MTBIs.
SD, standard deviation; MTBI, mild traumatic brain injury.
Of all the demographic and clinical variables listed in Table 1, the groups with 0, 1, or 2+ previous MTBIs were significantly imbalanced only on litigation status (lawyer involved vs. not), chi-square (2)=11.61, p=0.003. Litigants were half as likely to report a previous MTBI (28% vs. 56%). They also reported greater current post-concussion symptoms [M=29.3, SD=11.8 vs. M=22.3, SD=11.2; t(100)=2.99, p=0.004, d=0.61]. To rule out litigation as a confound for the above-reported null effect of previous MTBI history, it was not possible to examine interaction effects because of insufficient cell sizes (n=1 for litigants with 2+ previous MTBIs). Therefore, those in litigation were excluded. For participants who were not in litigation, there was no significant difference in symptom reporting between those with 0, 1, or 2+ previous MTBIs, F(2, 62)=1.161, p=0.320. Descriptive statistics for non-litigants are also presented in Table 2. Note that mechanisms of injury were evenly distributed between participants with 0, 1, or 2+ previous MTBIs (chi-square[2]=1.31, p=0.521) even though litigants were disproportionately likely to have been injured in a motor vehicle accident (chi-square[1]=32.63, p<0.001; 66% vs. 14% for non-litigants).
To examine the relation between outcome and the time interval between multiple MTBIs, participants (n=50) were selected who had sustained at least one previous MTBI of any certainty classification (probable or possible MTBIs). Thirteen of these participants had missing data for the time since the previous MTBI and were excluded from further analyses (n=37 remained). In this subgroup, the time since the previous MTBI (in years) was significantly correlated with current BC-PSI total scores, r(37)=− 0.42, p=0.010, indicating that more remote previous MTBI(s) were associated with lesser current symptom reporting. A scatter plot of these data is presented in Figure 1. Time since previous probable MTBI correlated somewhat stronger with current BC-PSI total scores r(17)=−0.53, p=0.029. As a group, participants who sustained a previous MTBI of any certainty classification within the last 7 years (i.e., below the median split) had greater current BC-PSI total scores (n=21, M=28.9, SD=9.8) than participants whose most recent previous MTBI was more than 7 years previous to the subsequent injury (n=16, M=19.6, SD=7.7; t[35]=3.13, p=0.004, Cohen d=1.06 [large effect]).
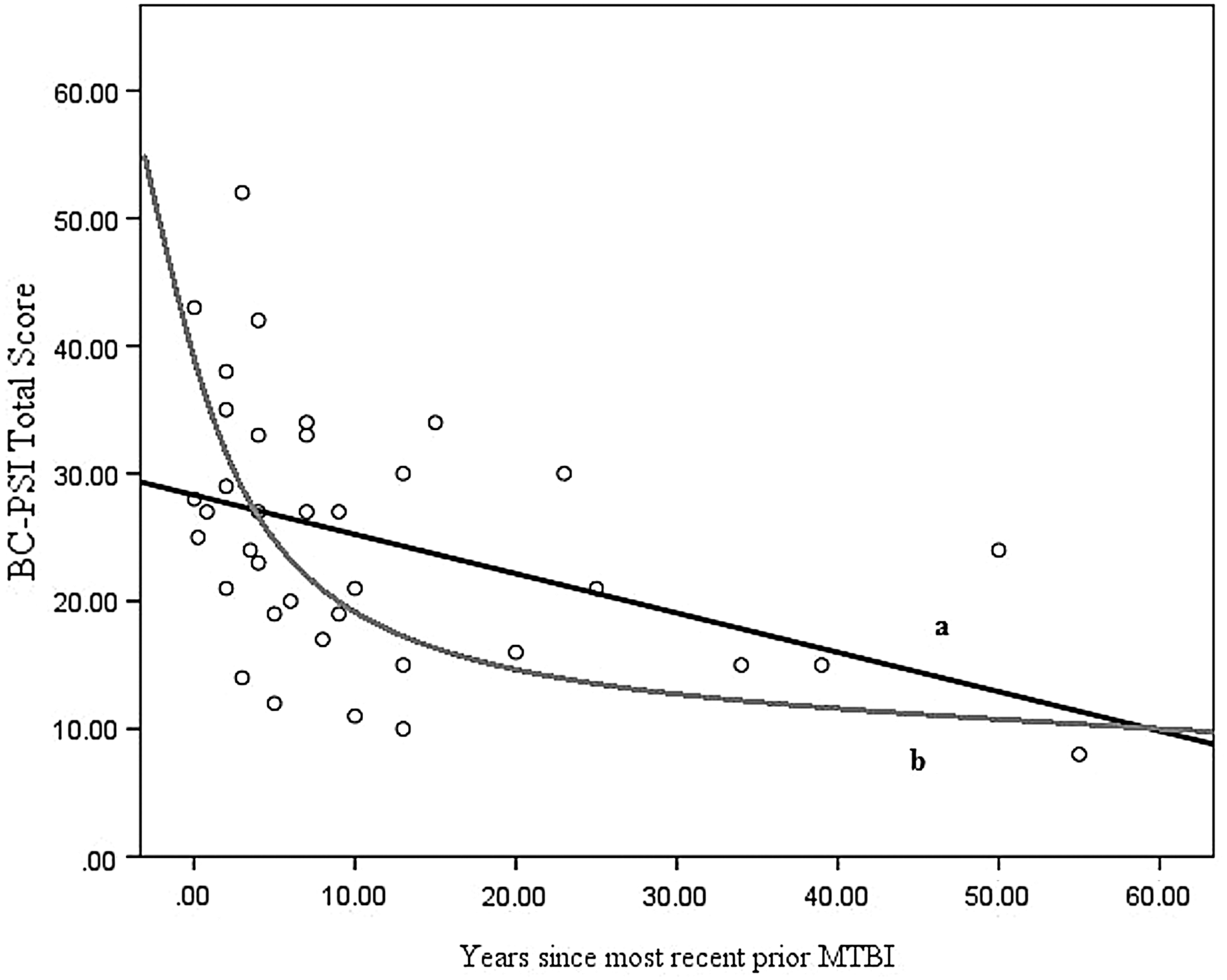
Current post-concussion symptom severity (British Columbia Post-Concussion Symptom Inventory [BC-PSI] total scores) plotted against time since previous mild traumatic brain injury (MTBI).
Generalized linear models were used to explore whether the relation between time since previous MTBI (any certainty level) and current post-concussion symptom reporting was non-linear. We fitted both a standard Gaussian model and a Gaussian model with a log link and compared them. A Gaussian model with a log link fit the data somewhat better than a Gaussian model with an identity link (i.e., ordinary least squares regression), based on a markedly lower Bayesian Information Criterion (3279.3 vs. 3337.9), comparable Akaike Information Criterion (7.31 vs. 7.33), and less heteroskedasticity in the residuals. This pattern suggests that the relation between time since previous MTBI and current post-concussion symptom reporting may be best characterized by a logarithmic function. That is, the impact of previous MTBI(s) lessens exponentially as time elapses to a subsequent MTBI. This is consistent with a visual inspection of the scatter plot. Line (b) in Figure 1 appears to fit the data better than line (a).
To examine the unique contribution of the number, recency, and certainty of previous MTBIs, variables representing each were evaluated as predictors in a regression model. BC-PSI total score was the response variable. Because of its promise in the above-described univariate analyses, time since last previous MTBI was entered in the initial block. This step was significant, R 2 =0.416, F(1, 35)=7.33, p=0.010. Two variables were simultaneously entered in a second block—certainty classification of the most recent previous MTBI (possible or probable) and total number of previous MTBIs that the participant incurred (as a continuous variable). This step did not significantly improve the model, R 2 change for block=0.03, F(2, 33)=0.706, p=0.501. In other words, the variables reflecting the certainty classification of the most recent MTBI and how many MTBIs preceded the current one added minimal useful information over and above the time since the most recent previous MTBI.
In a final analysis, we aimed to understand the influence of a recent previous MTBI on post-concussion symptom reporting relative to factors with a previously established association with high symptom severity. We entered recent previous MTBI (<7 years vs. >7 years or no previous MTBI), litigation (lawyer involved vs. not), sex, age, and current MTBI with positive day-of-injury CT scan (vs. negative or not available) as predictors in a regression model with BC-PSI total score as the response variable. Loss of consciousness and post-traumatic amnesia duration were not considered because they have been consistently shown to be unrelated to MTBI outcome. 47 The overall model was significant, F(4, 96)=4.921, p<0.001. Greater symptom reporting was significantly associated with litigation status (t=2.853, p=0.005) and normal/not available CT (t=−2.175, p=0.032). There were also trends for recent previous MTBI (t=1.932, p=0.056) and female sex (t=1.971, p=0.052). Age had very weak unique predictive power in this model (t=0.985, p=0.327).
Discussion
Approximately one-third of patients who present to a trauma center with MTBI have had at least one previous MTBI, 19,21,48 –51 and yet the clinical significance of MTBI history is not well established, especially outside of sports. The present study aimed to better understand factors that might influence the relation between previous MTBI(s) and outcome from a subsequent MTBI. Specifically, these clinically important questions were addressed: (1) how many previous MTBIs does it take to alter outcome from a new MTBI? (2) does it matter how recent the last MTBI was? and (3) what constitutes a previous head trauma event of clinical significance?
Inconsistent with the first hypothesis, participants with previous MTBIs did not report more post-concussion symptoms compared with those who did not have a history of MTBI. There were no differences in post-concussion symptom reporting, at an average of 32 days post-injury, across subgroups classified with 0, 1, or 2+ previous MTBIs. Because participants in litigation were overrepresented in the subgroup with no previous MTBIs and they reported greater post-concussion symptoms, we considered litigation status as a potential confound. Removing the patients who were in litigation did not alter the findings, however. If not from chance, the finding that litigants reported fewer previous MTBIs is novel and intriguing. Having personal experience recovering well from a past MTBI may make someone less likely to seek compensation for a subsequent MTBI. Alternatively, litigants may underreport previous MTBIs, intentionally or through unconscious processes, to strengthen the causal link between their current symptoms and compensable MTBI. These interpretations are necessarily speculative and are offered only to guide future research.
The present study complements a recent meta-analysis of athlete studies that found a non-significant effect of 0 versus 1+ previous MTBIs on symptom-reporting after a subsequent MTBI 2 by showing a similar null effect in a sample with heterogeneous injury mechanisms. Thus, the best available evidence, at present, suggests that having one or more previous MTBIs does not necessarily confer risk of poor symptomatic recovery from a subsequent MTBI. Note that the present study, like those included in the meta-analysis by Belanger and coworkers, 2 included few participants (13%) with 3+ previous MTBIs, which has been more consistently linked to possible residual effects in some persons. 6 –11 Given our cross-sectional design, we also cannot rule out that patients with and without a history of repeated MTBIs have different recovery trajectories—they may only begin to diverge at later post-injury time points.
Our second hypothesis, that more recent previous MTBIs are associated with worse outcome, was supported. There was modest evidence to favor a non-linear (logarithmic) characterization of this relationship (depicted by line [b] in Figure 1), suggesting that the association between a previous MTBI and symptom reporting after a subsequent MTBI weakens as the time between them increases, rapidly at first and slower thereafter. Using a median split based on time since previous injury, those injured in the past 7 years had much higher total scores on the BC-PSI than those injured more than 7 years ago (d=1.06).
These findings need replication, but could have important implications. It highlights the need for caution in extrapolating sport-related concussion research to other MTBI populations, because athletes tend to have repeated MTBIs more closely spaced 31,32 (but see 14 ), which may overestimate the effect of previous MTBIs in non-athletes. It also points to a knowledge gap that needs attention. Neurobiological mechanisms proposed to underlie recovery from close proximity MTBIs (i.e., between injury intervals of less than 2 weeks) 26,52 appear unable to explain how a previous MTBI can adversely impact recovery from a subsequent MTBI months to years later, as was the case in our study.
We also hypothesized that different criteria used to identify previous MTBIs might explain significant variability in outcomes from subsequent MTBI. It was assumed that past head traumas associated with loss of consciousness, post-traumatic amnesia, or an emergency department admission would increase the likelihood that a previous head trauma event was actually an MTBI. Retrospectively reported previous head trauma events with these features (i.e., probable MTBI) should have a greater impact on outcome than previous MTBIs without these features. The findings were mixed. Probable previous MTBIs were not associated with a stronger exposure-response effect, but did strengthen the recency effect somewhat. Most previous studies did not make the distinction between likely MTBIs and other minor head trauma events, suggesting that extra caution is warranted in interpreting their findings.
A diverse range of biopsychological factors have been previously shown to correlate with post-concussion symptom reporting, such as litigation and, with less consistency, age, sex, and CT abnormalities. 40,47 In this broader context, a history of MTBI within the past few years had unique importance. Its relation with post-concussion symptom reporting after a subsequent MTBI in the present sample could not be explained by litigation, sex, age, or severity of the subsequent MTBI (defined by presence/absence of intracranial abnormalities). In other words, the effect of MTBI history was not overshadowed when considered alongside these empirically established covariates. Recent previous MTBI may therefore represent another characteristic of the minority of patients who recover more slowly and/or less completely from MTBI. 53
The present study involved a heterogeneous clinic-referred sample, where most participants had fewer than three previous concussions, without medical documentation, spaced over years, incurred in various settings (e.g., motor vehicle accident, fall, recreational sport). The results should therefore generalize to patients presenting to a concussion clinic or community-based rehabilitation center. Several limitations need to be considered, however. The present study did not comprehensively examine potential moderators of outcome from repeated MTBI. The recency of a previous MTBI may be one of several moderating factors. Age at first injury and genetic factors (e.g., APOE E4 allele status), for example, may also contribute to the heterogeneity in outcomes. 54 We also did not obtain objective measures of neurological recovery (e.g., magnetic resonance spectroscopy, neuropsychological testing) or consider the full range of potentially important adverse outcomes from repeated MTBI, such as increased risk of incurring further MTBIs or development of dementia. 55 Rather, we focused on post-concussion symptom severity at first clinic visit after a subsequent MTBI. Our findings are therefore limited to this narrow aspect of MTBI outcome.
A further limitation of our study was the unavailability of detailed medical records for both current and previous MTBIs in most participants, necessitating an overreliance on self-report. This is a methodological limitation in the vast majority of studies involving recurrent MTBI in athletes, civilians, and service members. To improve the reliability of our MTBI ascertainment method, we used medical records when available. A disadvantage of this mixed method approach is that previous MTBI could be confirmed with differing levels of certainty across participants. Although a strong reliance on self-report is likely reflective of clinical practice (i.e., supports external validity), it further attenuates the strength of our conclusions. The field needs a standardized and comprehensive method of assessing MTBI history. The Ohio State University TBI Identification Method is one solution for this need. 56 Its adoption as a Common Data Element in MTBI research 57 should facilitate its widespread use, particularly in future studies of repeated MTBI. Finally, like virtually all previous studies of repeated MTBI, our cross-sectional design precludes causal inferences. 9
With these limitations in mind, the present study revealed no clear evidence of cumulative effects of 1 to 3 previous MTBIs on post-concussion symptom reporting in trauma patients presenting to clinic, when collapsing across time since the previous injury. Those injured in the past few years, however, compared with those with more remote previous injuries, reported greater symptoms at their first clinic visit for a subsequent MTBI. We tentatively conclude that previous MTBI(s) appear to complicate symptom resolution from a subsequent MTBI to the extent they occur more recently, versus remotely. The underlying mechanisms relating to increased post-acute symptom reporting, in those who had previous injuries in recent years, are unknown and might be biopsychosocial.
The present study has clinical implications. It highlights the need for a detailed assessment of previous MTBI exposure and to specifically consider the timing of previous MTBI(s) in prognosis and treatment planning. Whereas a more recent history of MTBI (months or few years) might be related to symptom reporting and recovery, remote MTBIs may be of less significance in most patients. Until a more definitive evidence-base emerges, however, a relatively guarded prognosis and conservative clinical management is reasonable for patients with repeated MTBI.
Footnotes
Acknowledgments
The Vancouver Coastal Health Research Institute provided salary support for Dr. Silverberg but was not involved in the writing of the article or the decision to submit it for publication. The authors wish to thank the staff at the G.F. Strong Early Response Concussion Clinic and Fraser Health Concussion Clinic for their assistance with data collection, and in particular, Mr. Jerry Stanger, Director of the Acquired Brain Injury Program of Fraser Health.
Author Disclosure Statement
Grant Iverson, Ph.D., has been reimbursed by the government, professional scientific bodies, and commercial organizations for discussing or presenting research relating to mild TBI and sport-related concussion at meetings, scientific conferences, and symposiums. He has a clinical and consulting practice in forensic neuropsychology involving persons who have sustained mild TBIs (including professional athletes). He has received research funding from several test publishing companies, including ImPACT Applications, Inc., CNS Vital Signs, and Psychological Assessment Resources (PAR, Inc.). The remaining authors have no competing financial interests.