
Abstract
Applied as a bedside test of gross dorsal column function, the testing of light touch (LT) sensation is of high clinical value in the diagnosis of human spinal cord injury (SCI). However, the assessment of overall dorsal column deficit by testing only LT may be limited, because the dorsal column pathway conveys several large diameter afferent modalities (e.g., sensation of touch, two-point discrimination, and proprioception). Therefore, the objective of this study was to compare the epicritic sensation assessed by LT, Semmes–Weinstein monofilament (SWM), and electrical perception threshold (EPT) across cervical dermatomes (C3–C8) in individuals with cervical SCI. A multicenter cross-sectional study was performed at 6 months after cervical SCI, applying combined measures of LT, SWM, and EPT, bilaterally over predefined key sensory points (C3–C8). A total of 300 left- and right-sided dermatomes were tested for each outcome measure in 25 participants. The percentage agreement between classifications according to LT and SWM/EPT testing for all dermatomes between C3 and C8 ranged from 95.5% to 36.2%. The degree of agreement showed considerably variable κ coefficients (−0.1≥kw≤0.7) for each dermatome between C3 and C8. The additional measurements of epicritic sensation by SWM and EPT increased sensitivity by detecting and quantifying differences in sensory thresholds above, at, and below the LT level of injury. This is relevant for early clinical trials (phase 1/2), in which disclosing any biological activity of an intervention may be revealed by subtle sensory changes that might gain a clinical relevance.
Introduction
Testing of sensory function is essential to sufficiently measure the degree of dysfunction and recovery after acute cervical spinal cord injury (C-SCI), which is paramount for setting reasonable goals in rehabilitation, and for accurate stratification in a clinical trial. 1,2 However, difficulties arise in selecting outcome measures that can detect small changes to evaluate the success of rehabilitation, and to test the efficacy of new interventions, for the different sensory modalities and in the interpretation of those test results.
Light touch (LT) and pinprick (PP) assessment examined according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) 3 are used routinely during neurological examination of sensibility in patients with a SCI. However, the sensory assessment by the ISNCSCI might not be sufficiently sensitive to monitor safety and/or to detect subtle therapeutic benefits. 4 Furthermore, it may not be able to elucidate potential mechanisms of recovery. 5 Therefore, additional quantitative sensory assessments, such as the electrical perception threshold (EPT) and the Semmes–Weinstein monofilament (SWM), may be used in combination with LT and PP to improve the sensitivity to discrete sensory changes and robustness of sensibility examination in the clinic and in research. 6 –11 LT, SWM, and EPT assess the posterior column pathway for detecting thresholds for tactile cutaneous sensation and electrical cutaneous sensation. 7,12 –14
So far, SWM remains the only internationally recognized handheld instrument specifically designed to control application force variables, and to meet sensitivity and repeatability requirements for an objective outcome measure of sensation. 10,15 –17 However, to the best of our knowledge, SWM has not been systematically applied in spinal cord disorders, 18 whereas clinical experience in peripheral nerve damage (i.e., nerve repair surgery in upper extremities) has proven its validity and is well established in clinical use. 17,19
The pocket version of SWM consists of five nylon monofilaments with variable stiffness, which apply different amount of grams to quantify cutaneous sensation. The SWM sensory threshold is defined as the force of the lightest filament at which the patient reports sensation. In participants with chronic C-SCI, the SWM has been reported to have high validity and excellent overall inter- and intra-tester reliability (intraclass correlation coefficient [ICC] ranged between 0.84 and 0.95). 8 However, the ICC between individual cervical dermatomes has not been reported. Recently it has been shown that the ICC is fair for the SWM in C4, T1, T8, and L4 dermatomes in healthy subjects. 20 However, ICC values can vary between healthy subjects and patients as a result of inter-individual variations of sensory thresholds as well as differences in sensibility between dermatomes. The determination of the SWM sensory threshold has the advantage of being a simple and unobtrusive/discreet method.
EPT testing has been introduced in the assessment of sensory function in spinal cord disorders, and holds promise in providing sensitive readouts beyond the clinical scaling. 7,12,21 –23 The EPT is defined as the lowest ascending electrical stimulus intensity expressed in mA at which the patient reports sensation. 6,24 The overall inter- and intra-tester reliabilities of EPT appear to be moderate to good in healthy participants 20,21 and participants with incomplete SCI. 24 However, the ICC varied considerably between individual dermatomes in healthy participants. 23 Therefore, there are different normative values for each dermatome. The EPT can be applied to all sensory dermatomes, and results can be interpreted quickly; however, the method is more time consuming than LT testing.
The LT assessment of sensation roughly grades the ability of detecting an LT in the affected dermatome by “absent,” “impaired,” or “normal.” Therefore, detection of subtle improvements in sensation or minor sensory impairments is impossible. The SWM and EPT contain a greater range of discernible response levels for detecting a tactile cutaneous sensation and electrical stimulation and, therefore, have the potential of being more sensitive. 22,25 This encompasses a wide range of degrees of impairment, and can include hypersensitivity as well as hyposensitivity. However, it is unknown if EPT or SWM are more sensitive than is clinical sensory examination (LT) for an individual cervical dermatome.
Although SCI physicians and clinicians have gained great experience of LT testing in the clinical management of patients with SCI, the actual sensitivity of LT testing to assess dorsal column function in patients with SCI is less established. To our knowledge, there is no study that compares epicritic sensation assessed by LT, SWM, and EPT across cervical dermatomes (C3–C8) in participants at 6 months after C-SCI. The following study hypothesized that the segmental assessment of epicritic sensation in human SCI can be improved by additional semiquantitative sensory measures complementary to LT. The latter findings are required for consideration if LT testing can be assumed sensitive enough in interventional studies.
Methods
Study design
This study was a cross-sectional multicenter study in two specialized SCI rehabilitation centers.
Study population
Participants were recruited between March 2010 and May 2011 from two Swiss SCI centers: the University Hospital Balgrist, Zurich and the Swiss Paraplegic Center, Nottwil. Inclusion criteria consisted of traumatic or nontraumatic C-SCI with an American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade A, B, C, or D. 3 Exclusion criteria were any accompanying severe neurological (e.g., traumatic brain injury) or medical disorders and being <16 years of age. The participants were enrolled after having providing written informed consent. The local ethics committees of the two participating centers approved the study.
Procedures
The assessors were clinicans (physicians and occupational therapists) who had long-term experience in working with individuals with SCI. To ensure high-quality and reliable examinations, assessors were trained to perform all applied outcome measures. A standardized protocol that outlined detailed instructions on performing the assessments was followed for each outcome measure. The recording techniques and materials were standardized across both centers. All participants were tested in a quiet room throughout the examinations. For EPT and LT testing, participants were lying in a comfortable supine position, and for SWM testing, participants were seated. First, the testing procedure was explained to the participants. Before testing of cervical dermatomes, the stimuli of the different outcome measures were applied to a dermatome with normal sensation, such as the face, in order for the patient to recognize the sensation. Subsequently, the participants were asked to close both of their eyes, and the testing was started. All outcome measures were assessed in a random order at 6 months after SCI (defined as a time window between 150 and 186 days).
Assessments
The SWM and EPT outcome measures were applied bilaterally over predefined ASIA sensory key points in the dermatomes C3 to C8. The clinical neurological examination of touch sensation was assessed by the ASIA LT testing according to the ISNCSCI protocol for the whole body. 3 The PP assessment involves the anterior column pathway (i.e., spino-thalamic fiber tracts) and is, therefore, not included in the present study. Appreciation of LT sensation at each of the ASIA sensory key points was scored on an ordinal three point scale as follows: 2=normal; 1=impaired, and 0=absent. The LT level of lesion was defined as the last intact sensory level as indicated by normal LT testing. 3
The tactile cutaneous sensation threshold was assessed by the pocket version of SWM 10 (North Coast Medical, Inc, Campbell, Canada) according to a strict and standardized assessment protocol. 10 The sensory threshold of the SWM was defined as the force of the lightest filament at which the individual reported sensation. An ascending method of threshold testing was used, starting with the smallest diameter monofilament (lightest filament, lowest force, most difficult to detect) and continuing in order of increasing diameter if the patient did not respond to the previous filament. Only ASIA sensory key point locations, which did not respond to the previous filament, were tested with the next filament. The examination was continued until the patient recognized a force/touch in all test locations or until it was established that the patient did not feel even the heaviest filament. Two of three applications of the lightest filament had to be felt to obtain a positive result. All the other, heavier filaments were applied only once according to the manufacturer's instructions. 10 In the study of Voerman et al., 13 filament marking 3.61 represented the normal value for sensory thresholds in all cervical dermatomes. In the present study the qualification of normal values was based on the mean threshold and the 95% CI according to Voerman et al. 13 The log of grams of force was represented by numeric values ranging from 0 to 4 as described in the instructions of the SWM mini-kit: 4=filament 3.61; 3=filament 4.31; 2=filament 4.56; 1=filament 6.65; and 0=no response. 10,13,16 In our study, a SWM value of 1, 2, or 3 points was defined as impaired, a value of 4 points was defined as normal, and a value of 0 points was defined as absent.
The EPT 6,22 was assessed according to previous studies, 6,22 using a modified mobile Compex 2 stimulator (Compex Medical SA, Switzerland), which delivered a square shaped stimulus of 0.5 ms duration at 3 Hz. The perceptual threshold was defined as the lowest ascending stimulus intensity (mA) at which the patient reported sensation. The maximal stimulator output and the smallest increment were adjusted to 26.9 mA and 0.21 mA, respectively. The skin was thoroughly cleaned with alcohol wipes, and disposable, self-adhesive electrocardiogram (ECG) electrodes (cathode) with a diameter of 18 mm (3M Red DotTM - type 2248) were applied over the ASIA sensory key points. A large (50×90 mm) inactive electrode (anode; Synapse Electrodes, Ambu, Denmark) was attached to the forearm of the testing side. For every dermatome tested, the stimulus intensity was manually increased and decreased with changes applied exactly once per second, until the patient first reported the sensation (ascending) under the cathode. This was repeated three times, and the lowest EPT (expressed in mA) of the three measurements was included in the analysis. Van Hedel et al. 23 have established the normal values for the electrical perception threshold for each cervical dermatome. In our study, the qualification of normal values was based on the mean value of the upper limits of the 95% CI from the two measurements, which reflects normality according to van Hedel et al. 23 In the present study, an impaired EPT value was defined as any value greater than the normative EPT value. A normal EPT value was defined as any value equal or smaller than the normative EPT value, and the EPT value was considered absent, if the maximum current intensity (threshold at 8.4 mA) was not perceived. A stimulation >8.4 mA was avoided, as at this level of intensity, additional pathways (i.e., nociceptive A-δ or C-fibers) than dorsal column fibers (i.e., A-β fibers) might become effectively stimulated, and could falsify the perceived sensation by the subjects. 12
Statistical analysis
Descriptive statistics were used to determine the frequency, median, and range of the study participants' characteristics, including cause of injury, AIS grade, AIS sensory LT level, sex, and age. For comparison with LT scores, the study participants' SWM and EPT data were classified as normal, impaired, or absent, and scored with 2, 1, or 0, respectively. All comparisons were made for the right and left side combined, because there was no statistically significant difference between the right and left side. Dermatomes were classified as having abolished, impaired, or normal sensation based on LT, SWM, and EPT testing. The frequency and percentage of classification agreement between LT-SWM and LT-EPT for all C3 to C8 dermatomes was determined. Finally, the degree of agreement between the three measures, weighted (Fleiss–Cohen) κ coefficients and CIs were calculated for each dermatome between C3 and C8, as well as for all dermatomes between C3 and C8. Agreement was assessed using the standards as established by Altman: 0.00=poor; 0.01–0.20=slight; 0.21–0.40=fair; 0.41–0.60=moderate; 0.61–0.80=substantial; and 0.81–1.00=almost perfect. 26
All data were analysed using SPSS version 18.0 for Windows and R version 2.15.1 for Windows.
Results
Participants
Table 1 presents the characteristics of the 25 cervical SCI participants with a high percentage of incomplete SCI. SCI was scored as complete (AIS A) in 5 individuals and incomplete in the remaining 20 individuals (AIS B, C, and D). In five individuals, the cervical dermatomes did not reveal any touch sensation disturbance. A total of 300 left- and right-sided dermatomes were tested for each outcome measure between C3 and C8 in all 25 participants.
Demographic and Clinical Characteristics of Participants (n=25)
SCI, spinal cord injury; N, sample size;
AIS, American Spinal Injury Association Impairment Scale.
Distribution of findings in LT, SWM and EPT
Classification of dermatomes according to LT, SWM, and EPT testing are shown in Figure 1. The greatest number of dermatomes was classified as intact when using LT testing (62.7%), whereas applying SWM (44.3%) and EPT (29.3%) revealed fewer intact dermatomes. Accordingly, the number of dermatomes classified as impaired increased from LT (30%) to SWM testing (42.3%), and was greatest for EPT testing (57%) across dermatomes. The number of dermatomes classified as absent was rather similar for SWM and EPT testing (30.3% and 30.7%), and lower for LT (7.3%).
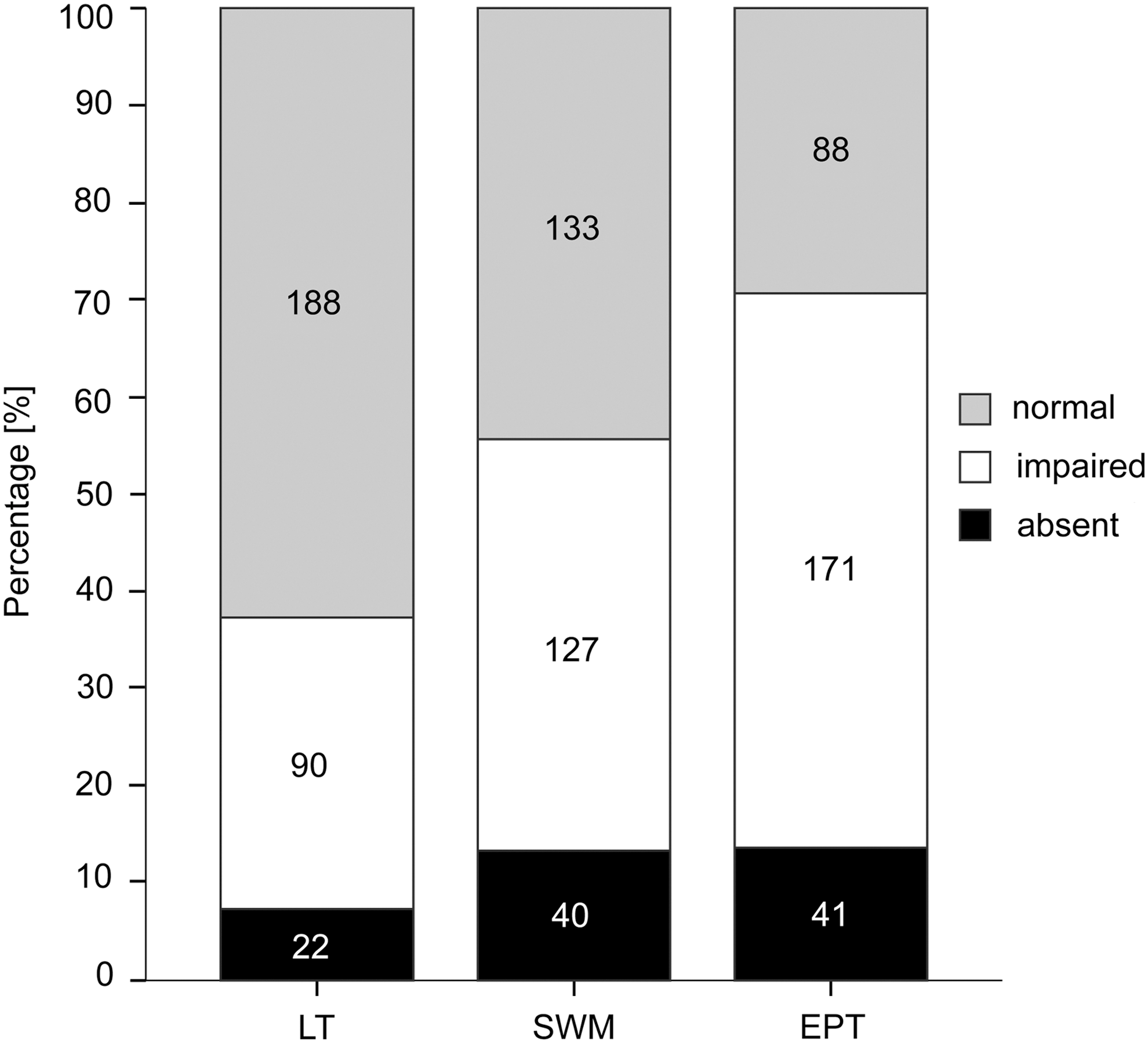
Numbers and percentage of dermatomes in absent, impaired, and normal sensation for light touch (LT), Semmes–Weinstein monofilament (SWM), and electrical perception threshold (EPT). A total of 300 dermatomes for each outcome measure between C3 and C8 were tested.
Agreement of LT and SWM classification
The agreement of classification between LT and SWM for all dermatomes between C3 and C8 is reported in Table 2. The overall agreement of classifications comparing LT and SWM within the same categories was 95.5% (21/22) for absent sensation, 47.8% (43/90) for impaired sensation, and 54.3% (102/188) for normal sensation. In dermatomes with absent LT sensation (LT 0), 4.5% reported some SWM sensation. However in dermatomes with preserved LT, either impaired (LT 1) or normal LT (LT 2), a high degree of discordance was observed compared with SWM. In dermatomes with normal LT, the SWM testing classified 44.1% (83/188) of dermatomes as being impaired. All 83 dermatomes classified by impaired SWM were at and above the LT level of injury. In dermatomes classified with impaired LT scores, SWM testing revealed normal or absent sensation in 34.4% (31/90) and 17.8% (16/90), respectively. All 31 dermatomes classified by normal SWM were below the LT level of injury.
Agreement and Discordance of Frequency of Classification in Absent, Impaired, and Normal Sensation Between LT and SWM (300 Dermatomes)
LT, light touch; SWM, Semmes–Weinstein monofilament.
SWM was grouped in three classes: SWM 0=0, absent; SWM 1,2,3=1, impaired; SWM 4=2, normal.
LT 0, absent (22 dermatomes); LT 1, impaired (90 dermatomes); LT 2, normal (188 dermatomes).
n=Frequency of classification.
Agreement of LT and EPT classification
The agreement of classifications between LT and EPT for all dermatomes between C3 and C8 are reported in Table 3. Overall, the agreement between classifications examined by LT and EPT testing was 90.9% (20/22) for absent of sensation, 52/90 (57.8%) for impaired sensation, and 68/188 (36.2%) for normal sensation. A high discordance of classifications for impaired and normal sensation between LT and EPT was recorded in the remaining dermatomes. In dermatomes with normal LT, the EPT testing classified 62.2% (117/188) of dermatomes as being impaired. All 117 classified by impaired EPT were at and above the LT level of injury. Furthermore, in dermatomes classified with impaired LT scores, EPT testing revealed normal sensation in 22.2% (20/90) and an absent sensation in 20% (18/90). All 20 dermatomes classified by normal EPT were below the LT level of injury.
Agreement and Discordance of Frequency of Classification in Absent, Impaired and Normal Sensation Between LT and EPT (300 Dermatomes)
LT, light touch; EPT, electrical perception threshold.
EPT was grouped in three classes: maximum pain threshold of 8.4 mA not perceived=0, absent; greater than the normative EPT value=1, impaired; equal to or less than the normative EPT value=2, normal.
LT 0, absent (22 dermatomes); LT 1, impaired (90 dermatomes); LT 2, normal (188 dermatomes).
n=Frequency of classification.
Degree of agreement between LT-SWM and LT-EPT
Table 4 shows the level of classification agreement between LT-SWM and LT-EPT for all dermatomes between C3 and C8. The overall weighted κ coefficient between LT and SWM was moderate (0.5) and fair (0.4) for LT-EPT. However, when evaluated for individual dermatomes the agreement varied considerably. In dermatomes C3, C4, and C5, the weighted κ coefficients (≤0.2) revealed that the level of classification agreement between LT and SWM, as well as between LT and EPT, occurred rather by chance. However in dermatomes C6, C7, and C8, the weighted κ coefficients were found to be moderate to substantial (weighted κ range=0.5 to 0.7) between the different testing methods.
Agreement of Classifications Between LT-SWM and LT-EPT for Each Dermatome Between C3 and C8 and for All Dermatomes Between C3 and C8
LT, light touch; SWM, Semmes–Weinstein monofilament; EPT, electrical perception threshold.
C3, cervical dermatome right and left side combined; Kw, weighted κ coefficient (Fleiss-Cohen); 95% CI, the lower and upper limit of the 95% confidence interval.
C3-C8, all dermatomes between C3 to C8, right- and left side combined.
Weighted κ coefficient: 0.00, poor; 0.01–.20, slight; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial; and 0.81–1.00, almost perfect.
Discussion
The study reveals for the first time a comprehensive comparison of epicritic sensation as assessed by LT, SWM, and EPT across cervical dermatomes (C3–C8) in individuals with SCI. The sensory testing focused on the assessment of sensory integrity of distinct predefined dermatomes in patients with C-SCI. Improving the assessment of epicritic sensation will be important in early clinical trials (phase 1/2), in which segmental and subtle changes in sensory function might provide important readouts about the beneficial as well as the detrimental (i.e., descending and ascending levels of lesion, respectively) effects of novel interventions. The presented study provides evidence that the segmental assessment of epicritic sensation can be improved by SWM and EPT.
The challenge of sensory testing
Clinical testing of sensory function is commonly challenged by limitations of test reliability, which is true to some extent for almost all sensory qualities (such as epicritic sensation and prothopatic sensation). 7,9,27,28 This becomes even more demanding when assessing different levels of sensory impairment when the subjective rating of patients is not able to define incremental levels of impairment, but becomes rather limited to a simplified categorical (ordinal scale, e.g., normal, impaired, and abolished sensation) gross scoring. Therefore, the ability to understand minor changes during recovery (improvements or deterioration) is very challenging, and clinical testing of one specific sensory quality (such as LT) within a complex domain of sensory function (such as epicritic sensation conveyed by dorsal column pathways) will be likely of limited sensitivity. One approach to overcome these challenges is to introduce measures with a more defined scaling of sensation (such as SWM testing by applying different sensory modalities) or to combine complementary sensory measures that are considered to reflect to some extent the integrity within similar fiber tracts. The latter approach would require modalities that are not redundant, but are able to reveal subtle differences regarding the integrity of function within an entire sensory system. In this context, the applied measures should also represent the same anatomical areas (i.e., distinct dermatomes), which can be well achieved by using LT, SWM, and EPT testing.
Disparity and sensitivity
The value of combining sensory testing of EPT and SWM complementary LT testing resides in the intention that they provide different insights in the integrity or impairment of epicritic sensation. Accordingly, they should not be just redundant, but reveal changes that cannot be disclosed by LT testing. A mismatch of segmental epicritic sensation was observed, as SWM was classified in 44.1% dermatomes and EPT was classified in 62.2% dermatomes as impaired, whereas LT revealed normal response. Interestingly, those findings were all at or above the LT level according to ISNCSCI, and are for the EPT findings in accordance to other studies. 7,12,22,23 Another discrepancy of segmental epicritic sensation was found below the level of injury according to ISCNSCI. LT revealed impaired response, whereas SWM classified 34.4% dermatomes and EPT classified 22.2% dermatomes as normal. These SWM findings are in agreement with the results of Kalsi-Ryan et al. 8 In their study, they used SWM in individuals with chronic cervical SCI, and observed greater sensitivity when using SWM, because of increased response levels, compared with the values reported when using ISNCSCI LT. The EPT findings are in line with the results of Kramer et al., 21 who observed that individuals with cervical SCI have persisting EPT values below the level of the lesion. 22 The present results suggest that SWM and EPT might be sensitive to small sensory impairments and/or preserved innervation in sensory function above, at, and below the LT level, which are less detectable by LT testing. This degree of sensitivity could be required to assess differences in sensory recovery, especially when improvements might be limited to one or two dermatomes adjacent to the LT level. Obviously, the value of additional sensory testing is most relevant in dermatomes that are clinically considered to be normal or impaired. In dermatomes with abolished sensation, SWM and EPT do not provide additional information to LT testing. (Overall agreement for abolished C3–C8 dermatomes between LT and SWM/EPT testing was ∼95.5% and 90.9%, respectively.)
Statistical analysis (kw≤0.5) confirmed that there is only a limited congruency between the three different assessments addressing epicritic sensation. Interestingly, these findings were not uniform across all dermatomes, and revealed a higher percentage of congruency (moderate to substantial agreement) specifically in the C6, C7, and C8 dermatomes, where a higher percentage of absent sensation was found with all three testing methods. Furthermore, in the C3, C4, and C5 dermatomes, a higher percentage of impaired and normal sensation was reported, which revealed a poor agreement between the three different assessments. These findings emphasize, as has been shown by the different thresholds for SWM and EPT across these dermatomes, that clinical assessment using LT is of limited sensitivity to disclose segmental differences in sensory function. Differences in findings across cervical (and thoracic) dermatomes are not specific for epicritic sensation, but have been also shown for the assessment of spinothalamic function (i.e., using laser-evoked potentials or contact heat evoked potentials), which reveals marked difference between dermatomes (again these differences between dermatomes are also not adequately reflected by the clinical testing of PP sensation). 29,30
Improving readouts of sensory plasticity
The aims of increasing the sensitivity of testing epicritic sensation after SCI are twofold: 1) to identify changes within dermatomes, that is, high resolution of segmental changes, and 2) to provide insight into specific pathways that for the epicritic sensation are characterized by their high level of myelination. Therefore, applying such measures in an interventional study can address if segmental changes occur that are beyond spontaneous or regular findings (both beneficial and detrimental). In addition, such measures might be useful if interventions are considered to improve the myelination (i.e., concept of re-myelination) of damaged spinal fibers, where the recovery of A-β fibers depend on high level of myelination and might reveal superior recovery than less or unmyelinated sensory fibers (such as C fibers). 31,32 Therefore, in clinical trials, an improved resolution of sensory function by combined LT and SWM/EPT testing could be meaningful in revealing subtle changes that, for a proof of mechanism, might be critical for entering a next phase in which these effects can be amplified by adjusting the intervention.
Conclusion
There is limited agreement on sensory testing, specifically in incompletely affected dermatomes, among testing of LT, SWM, and EPT. This difference is likely attributable to the measurement limitations of each testing, and that they individually respond to the differently affected sensory modalities within the epicritic sensation. 28 The results show that SWM and EPT testing can add complementary resolution to LT testing at 6 months after C-SCI by detecting and quantifying differences in sensory thresholds above, at, and below the LT level of injury. The ability of combined sensory testing to gain insights beyond LT warrants consideration in the protocol design of interventional studies in which the sensitivity to indicate even subtle differences is of value both in the stratification of patients and the potential (not shown here) to reveal an improved responsiveness in sensory testing.
Footnotes
Acknowledgments
We thank the individuals with SCI participating in this study and the contribution of the staff at the Balgrist University Hospital Zurich and Swiss Paraplegic Centre Nottwil. We thank Dr. Jörg Krebs, Clinical Trial Unit, Swiss Paraplegic Centre Nottwil, and Dr John Kramer, Balgrist University Hospital Zurich for critical review of and editorial assistance with the manuscript.
Author Disclosure Statement
No competing financial interests exist.