
Abstract
The measurement of ocular nerve sheath diameter (ONSD) via ocular ultrasound scanning is a recent non-invasive method for intracranial pressure (ICP) assessment. Few clinical studies have assessed ONSD variations during osmotherapy for the treatment of sustained increased ICP episodes. The aim of our study was to determine the rate of ONSD variation after mannitol administration for increased ICP episodes. We consecutively included in a prospective, observational study, the patients who had severe acute brain injury and monitored with an invasive ICP monitor. For each episode of sustained elevated ICP, the ONSD was measured in the right and left eye with a 7.5-MHz echography probe, and the mean value was reported. Simultaneously, ICP and cerebral perfusion pressure (CPP) were recorded. All measurements were performed just before and 20 minutes following a 20% mannitol infusion. Data were expressed as medians and interquartile ranges. Thirteen patients were included and analysed (traumatic brain injury, n=10; subarachnoid haemorrhage, n=3). The median value of the mannitol dose infused was 0.54 g/kg (0.49–0.80 g/kg). In all cases, the ONSD was greater than 5.8 mm before osmotherapy. The ONSD significantly decreased after mannitol infusion from 6.3 (6.1–6.7) to 5. mm (5.5–6.3) (p=0.0007). Concomitantly, the intracranial pressure decreased from 35 (32–41) to 25 (22–29) mmHg (p=0.001) and the CPP increased from 47 (50–60) to 66 (59–69) mmHg (p=0.003). The variations of ONSD appear to be an interesting parameter to evaluate the efficacy of osmotherapy for elevated ICP episodes in patients with acute brain injury.
Introduction
E
Methods
This prospective observational study was performed in the surgical intensive care unit of a university hospital from December 2009 to December 2011. The study received institutional approval from the local research and ethics committee (Avis no.: 09–14, Rennes, France) and complied with human research protocols. Given the observational nature of the study, according to French law, the committee waived the requirement for informed consent from patients and relatives.
Patient selection criteria
Adult patients (≥18 years of age) who had severe traumatic brain injuries (TBIs) or subarachnoid hemorrhage (SAH) with a Glasgow Coma Scale ?GCS score of ≤8, an ICP monitor in place, and a sustained elevated ICP, defined as greater than 25 mm Hg for at least 10 min, were included. If an external ventricular drainage was in place, we checked that it was optimal. Exclusion criteria were as follows: patients with baseline ocular pathology; patients who had previously undergone eye surgery; and patients who had undergone cranial decompression surgery for refractory hypertension after the initial brain injury workup.
The following data were recorded upon inclusion: age, gender, and severity of illness at admission, as assessed by the Simplified Acute Physiologic Score (SAPS II) and GCS. Type and doses of sedative agents or thiopental administered before the beginning of the study were recorded using the Richmond Agitation Sedation Scale (RASS) and the Behavioral Pain Scale (BPS). 11,12
Investigated variables
ICP was measured continuously through an intraparenchymal catheter (Neuromonitor-Microsensor kit™; Codman, Châtenay-Malabry, France) or an external ventricular drainage system (EDS3™; Codman, Raynham, MA) inserted by a neurosurgeon. Briefly, as described previously, 13 –15 ONSD measurements were performed with a 7.5-MHz ultrasound (US) probe in a supine 30-degree bed position. Virtually, the probe was gently placed on the upper eyelid, without pressure, in the linear horizontal orientation (50-mm depth) for both the right and left optic nerve sheaths in the horizontal plane. Placement of the probe was adjusted to give a suitable angle for displaying entry of the optic nerve into the globe. The ONSD was measured 3 mm longitudinally from the location of the retina in each eye with the two-dimensional mode, using an electronic caliper and an axis perpendicular to the optic nerve. The mean value of the right and left ONSD was used in the analysis. Transcranial Doppler measurements were performed with a 2-MHz US probe (Vivid-i; General Electric, GE Healthcare, Chalfont St. Giles, UK). Transcranial Doppler imaging was used to measure the systolic, end-diastolic, and mean arterial velocities (Vs, Vd, and Vm, respectively) at the M2 segment of the right and left middle cerebral arteries (MCAs), and the pulsatility index (PI) was automatically provided by the computer as: PI=(Vs – Vd)/Vm. All patients had an arterial catheter (Seldicath 4F 38874 13; Plastimed Laboratory, Saint-Leu-La-Forêt, France) that enabled the measurement of mean arterial pressure (MAP) and the calculated cerebral perfusion pressure (CPP) as MAP – ICP.
Experimental protocol
After inclusion criteria were verified, baseline measurements were recorded, including MAP, ICP, right and left ONSD, systolic, end-diastolic, and mean arterial velocities of the right and left MCAs, and the PI. The ONSD and transcranial Doppler measurements were then performed. Osmotherapy with 20% mannitol was performed, at a dose of 0.5–1.0 g/kg, through a dedicated venous line over 20 min. Twenty minutes after the end of the mannitol infusion, the same measurements as those obtained at baseline were performed. No adjustments of sedative agents or thiopental were allowed during the entire period of the study. All ONSD and transcranial Doppler measurements were performed by the same investigator (Y.L.), who has 6 years of experience in ONSD USG practice.
Statistical analysis
All analyses were performed using R software (version 2.11.1; 2010; The R Foundation for Statistical Computing, Vienna, Austria). The simple linear regression technique and Spearman's correlation coefficients were used to analyze correlations between ONSD and ICP before and after mannitol infusion. Comparisons of ONSD and ICP measurements were performed using paired Student's t-tests, and non-normally distributed data were compared using Wilcoxon's test. Variables are expressed as the mean and standard deviation or median and interquartile range (IQR) in the case of a significant non-normality of the distribution of continuous variables. For all analyses, a p value<0.05 was considered significant.
Results
During the study period, we screened 93 patients with severe TBI and 25 with SAH. Among these patients, 28 experienced an elevation in ICP requiring mannitol osmotherapy (TBI, n=23; SAH, n=5). Seventeen patients met the inclusion criteria, but 4 could not be included because of investigator or US scanner unavailability. Ultimately, 13 patients were included and analyzed (TBI, n=10; SAH, n=3). ICP was monitored by an external ventricular drainage system in all SAH patients and by an intraparenchymatous catheter in all TBI patients.
Baseline characteristics are reported in Table 1. ONSD was measured in all patients, but transcranial Doppler measurements were only obtained in 12 patients (1 patient lacked a temporal acoustic window). At the time of measurement, the RASS score was –5 and the BPS score was 3 for all patients. The sedative agents infused were midazolam, at a median dose of 0.59 μg/kg/min–1 (IQR, 0–0.88), and fentanyl, at a median dose of 0.12 μg/kg/min–1 (IQR, 0.09–0.14). In 3 patients, thiopental was continuously infused at a median dose of 0.042 mg/kg/min–1 (range, 0.025–0.063). The median dose of mannitol administered was 0.54 g/kg (IQR, 0.49–0.80).
Data are expressed as the median (interquartile range).
SAPS II, Simplified Acute Physiologic Score; GCS, Glasgow Coma Scale.
There was a significant correlation between ICP and ONSD measurements before and after mannitol infusion (r 2=0.54; p<0.002; Fig. 1). Individual data and median (IQR) values of ICP, ONSD, and CPP before and after osmotherapy are displayed in Table 2 and Figure 2. After mannitol infusion, ICP and ONSD significantly decreased and CPP significantly increased (Table 2). In 1 patient (no. 12), ICP did not decrease after mannitol infusion (Table 2). Transcranial Doppler PI significantly decreased after osmotherapy from median (IQR) values of 1.57 (1.47–1.90) to 1.39 (1.15–1.70; p=0.008) and from 1.49 (1.38–2.04) to 1.45 (1.21–1.65; p=0.017) in the right and left MCA, respectively.
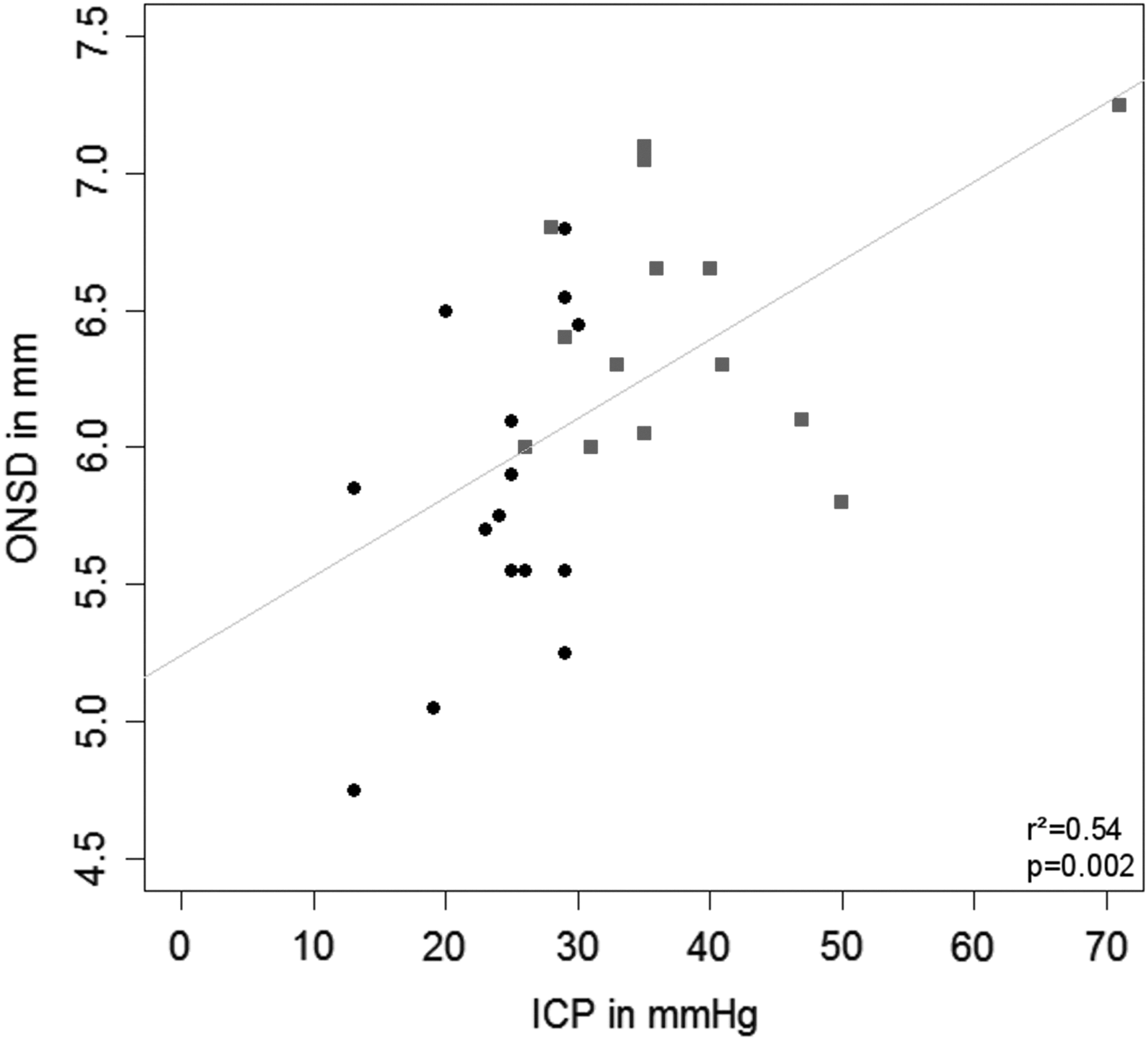
Correlation between intracranial pressure (ICP) and optic nerve sheath diameter (ONSD), including values obtained before and after mannitol infusion. Black-filled squares, baseline values; black-filled circles, values after mannitol infusion.
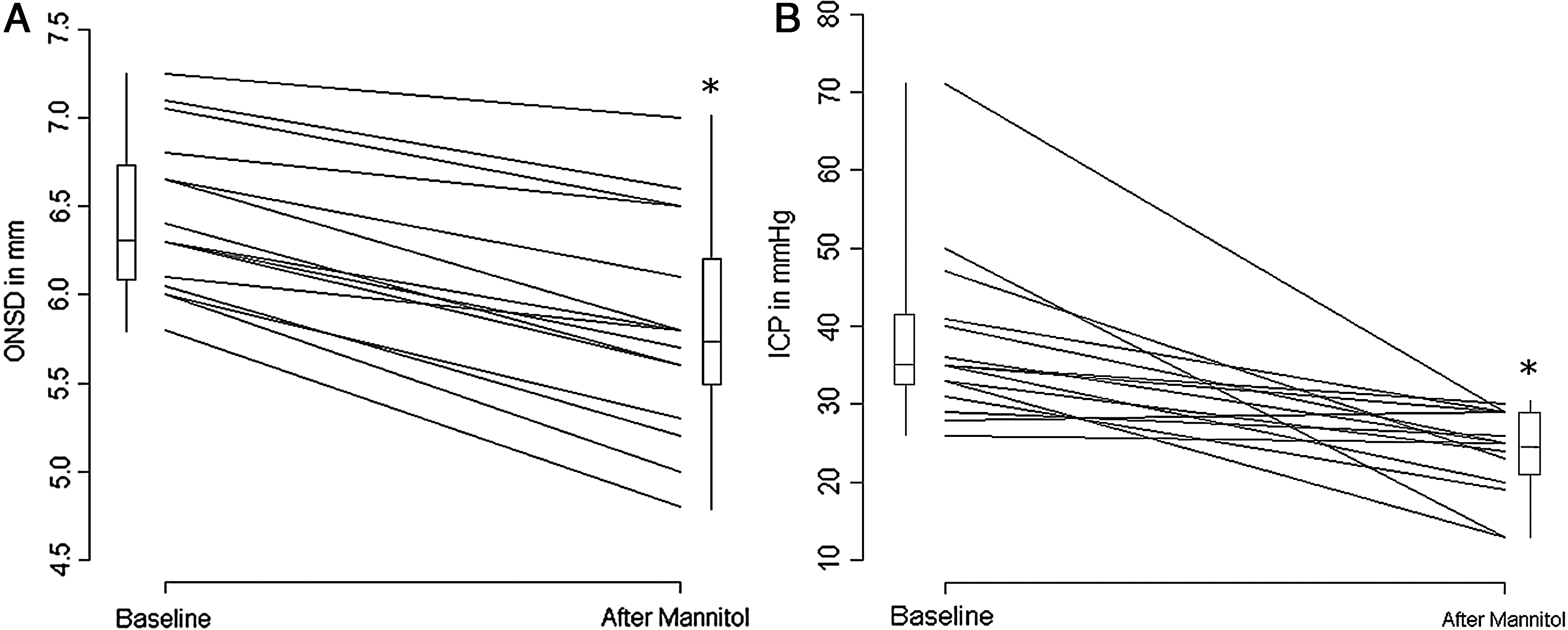
Individual variations and box plots of (A) optic nerve sheath diameter (ONSD) and (B) intracranial pressure (ICP) before and after mannitol infusion. *p<0.05 versus baseline value.
ICP after versus before osmotherapy (p=0.001).
ONSD after versus before osmotherapy (p=0.0007).
CPP after versus before osmotherapy (p=0.003).
ICP, intracranial pressure; ONSD, optic nerve sheath diameter; CPP, cerebral perfusion pressure; TBI, traumatic brain injury; SAH, subarachnoid hemorrhage; IQR, interquartile range.
Discussion
Our results showed that in patients suffering from severe TBIs or aneurysmal subarachnoid hemorrhage who had a sustained increase in ICP, a significantly reduced ONSD after mannitol infusion was associated with a concomitant decrease in ICP.
ONSD measurement techniques have already been described and validated for detection of elevated ICP. 7,14 –16 Indeed, studies on ONSD measurement have shown a good correlation between ICP measurements with intraparenchymatous fiber and USG findings in static conditions. 8,10 A threshold of 5.8 mm for ONSD was proposed to distinguish ICP of more than 20 mm Hg. 17,18 Geeraerts and colleagues have assessed ICP correlation between ICP and ONSD variations when measures were realized at ICP fiber insertion and 24 h later. The correlation was good (r 2=0.74; p<0.0001), but ONSD cannot be considered as a surrogate for invasive ICP monitoring. 9,10 No study has specifically focused on ONSD variations in clinical situations requiring osmotherapy for elevated ICP. With regard to dynamic conditions in patients with cerebrospinal fluid (CSF) absorption disorders, Hansen and Helmke evaluated ONSD response to changing CSF pressures with intrathecal infusion tests and reported that ONSD increased when the ICP threshold was between 15 and 30 mm Hg; however, they also noticed that this response did not continue when ICP exceeded 30 mm Hg. 19 In our study, we attempted to assess the reliability and correlation of ICP shifts after osmotherapy with ONSD changes. First, before mannitol infusion, our ONSD measurements corresponded to previous reports. 8,9,20,21 Only 1 patient could be suspected to have been incorrectly assessed because of an observed ONSD value of 7.2 mm, which is slightly higher than that normally observed during episodes of elevated ICP. 17,22 When the delta of ONSD according to baseline ICP level was considered, no correlation was found (r 2=0.13; p=0.64). Considering the patient with the value at 70 mm Hg ICP as an outlier, if we exclude it, the new correlation coefficient between ICP and ONSD was not significantly different (r 2=0.52 vs. r 2=0.54). Second, all osmotherapy challenges that induced an ICP decrease were associated with a simultaneous ONSD decrease. Similarly, transcranial Doppler measurements of the PI showed a decrease in these values after osmotherapy, in accord with previous studies. 23 Notably, the variation of ONSD after osmotherapy seemed less important when ICP was high (70 mm Hg), compared with ICP levels of approximately 30 mm Hg. Despite the small size of our study, one explanation for this observation could be the existence of radially oriented trabeculations between the optic nerve pia mater and its sheath that limit the expansion of the optic nerve sheath, as described in previous reports. 7,15,24 Recently, Hansen and colleagues have reported on the nonlinear restoration of ONSD after ICP normalization similar to a hysteresis relation, 25 which could account for special elastic properties of surrounding perineural structure. In our study, ONSD measurements were performed in the anterior section of the optic nerve, as previously described, 26 which is the most distensible region of the optic nerve. Indeed, in the anterior section of the bulbous portion of the optic nerve, these trabeculations are sparse, compared with those in the posterior sections. For high ICP values, ONSD enlargement is maximal, except in the case of hydrocephalus. This latter situation results in obstruction of CSF circulation and can underestimate ONSD change, whereas ICP variations are important. In the present study, none of the patients had hydrocephalus consecutive to external ventricular drainage clotting. In the case of ICP decreases as a result of osmotherapy, ONSD did not immediately return to baseline possibly because of a gradient between the bulbous region of the optic nerve and the craniospinal subarachnoid space sustained by the poorly distensible posterior section of the optic nerve, where trabeculations are predominant, 14,24 thereby delaying CSF pressure equilibration. Moreover, in cases of severe ONSD dilation, we cannot exclude the role of dural nerve sheath hemorrhage and/or edema, because venous retinochoroidal communication is hampered by mechanical compression. 27 Finally, the recent study of Rajajee and colleagues underscores the possible role of delayed reversal of optic nerve sheath distension and the decrease of specificity in ONSD measurements when ICP is acutely fluctuating between high and normal values. 28 This property should make for caution in the interpretation of ONSD variations.
Conclusion
ONSD sonography is a useful and user-friendly, noninvasive tool to detect ICP elevation, and ONSD is well correlated with ICP. Under dynamic conditions, this correlation remains valid even after osmotherapy with mannitol. Accordingly, ONSD sonography may be useful for monitoring efficacy of osmotherapy challenges during episodes of elevated ICP, particularly in the emergency room when invasive ICP monitoring is unavailable. However, careful interpretation of ONSD in the upper limit of values seems to be needed because no or little variation of ONSD after mannitol infusion can be associated with ICP reduction.
Footnotes
Acknowledgment
The preliminary results have been presented, in part, at the 24th annual congress of European Society of Intensive Care Medicine (ESICM), October 1–5, 2011, in Berlin, Germany.
Author Disclosure Statement
No competing financial interests exist.