
Abstract
Accumulating pre-clinical data suggests that matrix metalloproteinase (MMP) expression plays a critical role in the pathophysiology of secondary brain injury. We conducted a prospective multimodal monitoring study in order to characterize the temporal MMP response after severe traumatic brain injury (TBI) in eight critically ill humans and its relationship with outcomes. High-cutoff, cerebral microdialysis (n=8); external ventricular drainage (n=3); and arterial and jugular venous bulb catheters were used to collect microdialysate, cerebrospinal fluid, and arterial and jugular bulb blood over 6 days. Levels of MMP-8 and -9 were initially high in microdialysate and then gradually declined over time. After these MMPs decreased, a spike in the microdialysate levels of MMP-2 and -3 occurred, followed by a gradual rise in the microdialysate concentration of MMP-7. Use of generalized estimating equations suggested that MMP-8 concentration in microdialysate was associated with mortality (p=0.019) and neurological outcome at hospital discharge (p=0.013). Moreover, the mean microdialysate concentration of MMP-8 was 2.4-fold higher among those who died after severe TBI than in those who survived. Mean microdialysate levels of MMP-8 also rose with increasing intracranial pressure (ICP), whereas those of MMP-7 decreased with increasing cerebral perfusion pressure (CPP). Significant changes in the mean microdialysate concentrations of MMP-1, -2, -3, and -9 and MMP-1, -2, -3, -7, and -9 also occurred with increases in microdialysate glucose and the lactate/pyruvate ratio, respectively. These results imply that monitoring of MMPs following severe TBI in humans is feasible, and that their expression may be associated with clinical outcomes, ICP, CPP, and cerebral metabolism.
Introduction
A
Accumulating pre-clinical data suggest that modification of the brain extracellular matrix by the matrix metalloproteinase (MMP) family of zinc- or calcium-dependent endopeptidases plays a critical role in the pathophysiology of secondary brain injury after TBI. 3 –9 To date, 24 MMPs have been identified in humans, including the collagenases (MMP-1, -8, -13, and -18), gelatinases (MMP-2 and -9), and stromelysins (MMP-3, -10, and -11), of which 13 are soluble mediators. 10,11
Although the activity of most MMPs is normally negligible or low in the adult CNS, a substantial upregulation of their expression has been demonstrated in animal models of TBI, with each MMP likely exhibiting a unique temporal expression profile. 10 –12 Of the soluble MMPs, expression of MMP-2 and -9 occurs early after injury in animals. 12 These upregulated enzymes have been shown to disrupt blood–brain barrier integrity, promote vasogenic cerebral edema, and adversely affect neuronal survival. 3 –5,8,9 They are also associated with increased brain lesion volumes, cerebral edema, and neurological deficits following experimental brain trauma. 3 –5,8,9 In contrast, the more delayed expression or activity of other MMPs, such as MMP-3, may contribute to recovery after TBI by removing debris, reshaping the extracellular synpatic environment, and promoting neurogenesis. 13
As little is known about the MMP response after TBI in humans, 14,15 and because timing of MMP expression may be important for administration of neuroprotective agents, 12 we conducted the Proteomics of Severe TBI study. The primary purpose of the first part of this prospective cohort study was to characterize the temporal MMP response after severe TBI in critically ill humans using multimodal monitoring, including cerebral microdialysis and jugular venous bulb and peripheral arterial catheters. We also sought to explore the association between microdialysate MMP concentrations and cerebral physiology, clinical findings and outcomes, and standard microdialysis measures, including glucose, lactate, pyruvate, brain tissue oxygen tension (PbtO2), and the lactate/pyruvate ratio (LPR).
Methods
This study was registered online (
Patients
Consecutive mechanically ventilated adults admitted to a 30 bed, closed, medical/surgical/neurosurgical intensive care unit (ICU) at the Foothills Medical Centre (FMC) (Calgary, Alberta, Canada) between July 1, 2007 and September 31, 2010 were prospectively screened for study eligibility. The FMC is a university-affiliated, tertiary care, level 1 regional trauma center that provides trauma and neurosurgical services for southern Alberta, southwest British Columbia, and southeast Saskatchewan. Approximately 80 adults with severe TBI are admitted to the FMC ICU annually.
Eligibility criteria included: 1) age ≥18 years, 2) severe TBI (defined as a post-resuscitation Glasgow Coma Scale [GCS] score ≤8 16 ), 3) need for intracranial pressure (ICP) monitoring, 17 and 4) life expectancy >72 h (as determined by the investigators in consultation with the attending intensivist and staff trauma and neurological surgeons). Exclusion criteria included severe TBI that had occurred >12 h before study screening. Enrolment into the study occurred after written informed consent had been obtained from the legal surrogate decision maker for each patient, with regained consent being obtained from study patients after their recovery whenever possible.
Intensive care management of severe TBI
All patients were managed by fellowship-trained intensivists or neurointensivists in consultation with attending trauma and neurological surgeons, according to institutional protocols created in accordance with current recommendations from the Brain Trauma Foundation. 18 Their management often included early placement of peripheral arterial, central venous, and jugular venous bulb catheters.
Cerebral microdialysis
Within 24 h of ICU admission, all patients had a computed tomography (CT)-visible, gold-tipped cerebral microdialysis catheter with a nominal weight cutoff of 100 kDa (CMA-71, CMA Microdialysis, Stockholm, Sweden) inserted. In accordance with current guidelines for microdialysis in neurointensive care, 19 probes were implanted into brain tissue that appeared normal on CT, within the right frontal lobe whenever safe and possible.
After confirmation of correct cerebral microdialysis catheter placement with CT, the catheter probe was connected to a CMA 103 perfusion pump (CMA Microdialysis). Perfusion fluid (CMA Microdialysis) was then passed through the catheter at 0.3 μL/min. This flow rate was chosen a priori as it had been associated with a 70% microdialysate relative recovery for lactate, pyruvate, and glutamate in a previous study. 20 In 1 h intervals, obtained microdialysate sample vials were immediately analyzed at the bedside to determine concentrations of glucose, lactate, pyruvate, and glycerol using the CMA 600 (CMA Microdialysis) enzyme photometric analyzer. In order to allow for catheter stabilization, the first obtained sample was discarded to waste. Samples were refrigerated for a maximum of 24 h following bedside analyses. Microdialysate was pooled every 6 h and then aliquoted and stored at −80°C until MMP analyses could be performed.
Clinical and surrogate measures or outcomes
After study enrolment, data pertaining to age, gender, height, weight, mechanism of injury, post-resuscitation and study entry GCS, pupillary light reactivity at emergency department presentation, and comorbid conditions were collected for each patient. CT head findings were also reviewed in order to grade radiographic TBI severity using the Marshall Score. 21,22 This score is a nominal CT head categorization scheme for diffuse brain injury that considers the status of the perimesencephalic cisterns, degree of midline shift, and presence of surgical intracranial masses. In addition, physiologic data, including mean arterial pressure (MAP), ICP, CPP, body and brain temperature, and arterial and jugular venous oxygen saturation were recorded at least hourly until discontinuation of the microdialysis probe. Neurological outcome was assessed at hospital discharge by one of the investigators, by rating the patient's functional status using the five point Glasgow Outcome Scale (GOS), which ranges from dead (1) to minor/no disability (5). 23
Blood and cerebrospinal fluid (CSF) collection and processing
Blood and CSF were collected every 6 h after enrolment. Blood was collected into lithium-heparin-containing vacutainer tubes (CIE) from the patient's indwelling arterial catheter and then immediately spun at 1200g for 15 min in a swinging bucket centrifuge. The resultant plasma was then aliquoted and stored at −80°C until MMP analyses could be performed. In patients with an indwelling external ventricular drain, CSF was collected into heparin-containing vacutainer tubes (Benton Dickinson Biosciences, Oakville, ON, Canada) using sterile technique. Immediately after collection, CSF-containing tubes were stored at 4°C for a maximum of 24 h until they could be spun at 1200g for 15 min in a swinging bucket centrifuge to remove red blood cells and cellular debris. CSF was then aliquoted and stored at −80°C until MMP analyses could be performed.
MMP analyses
Quantification of the concentrations of MMP-1, -2, -3, -7, -8, -9, -12, and 13 was performed using the validated Luminex® bead-based multiplexing assay from R&D Systems (Minneapolis, MN) according to manufacturer's instructions. 24 This assay binds to both the active and inactive forms of MMP proteins, and, therefore, measures total MMP levels.
Briefly, microdialysate and plasma were thawed quickly at 37°C, centrifuged at 20,800g at 4°C for 10 min, and then stored on ice. Plasma samples were diluted as recommended by the manufacturer, whereas microdialysate and CSF samples were undiluted. A total of 25 μL of diluted plasma or undiluted microdialysate were distributed to each appropriate well. The plate was then incubated, in the dark, for 2 h at room temperature on a plate shaker set at 500 rotations per minute (rpm). Wells were first washed three times with 100 μL of wash buffer, and then 25 μL of diluted biotin antibody cocktail was added. The plate was subsequently incubated, in the dark, for 1 h at room temperature on a plate shaker set at 500 rpm. Wells were subsequently washed three times with 100 μL of wash buffer. Thereafter, 25 μL of diluted Streptavidin-PE was added to each well and the plate was incubated for 30 min at room temperature on a plate shaker set at 500 rpm. Wells were then washed three times with 100 μL of wash buffer. Subsequently, 75 μL of wash buffer was added to each well and the plate was read using a Luminex® 200 apparatus (Applied Cytometry Systems, UK). The data were analyzed with StarStation V.2.3 (Applied Cytometry Systems, UK).
Statistical analysis
As a primary objective of the study was to determine whether MMPs could be measured in microdialysate after severe TBI over time, no formal sample size calculation was possible. We aimed to enroll eight patients, as we believed this would be an adequate number to demonstrate feasibility of the proposed methodology for measuring MMPs and to describe their temporal concentration profile in microdialysate, CSF, and arterial and jugular bulb plasma. All analyses comparing MMP concentrations to clinical and surrogate outcomes were, therefore, entirely exploratory.
Means (with standard deviations [SD]) and medians (with interquartile ranges [IQR]) were used to describe normally and non-normally distributed variables, respectively. To analyze the association between pooled 6 h MMP concentrations and various other analytes, physiologic data, and clinical findings or outcomes, we developed univariate population-averaged panel-data models using generalized estimating equations. 25 These models are a variant of the generalized linear method, and may be used to model the expected mean change in the MMP concentration given an increase in the value of a chosen predictor variable. 25 Advantages of the use of these models over other comparison methods include the option to estimate the correlation structure from the data without the assumption of a pre-specified structure, 25 and their increased power for detection of differences between groups as a result of the use of the totality of data points, rather than only an arbitrary set. Although results of these models are often conveniently described as “means,” they calculate a panel-averaged result. As the nature of the correlation between variables was unknown, an exchangeable within-group correlation structure was used. 25 Terms containing ordinal measures, including GCS, GOS, and CT Marshall scores, were included in the models by expanding them into dummy variable sets using an interaction expansion command. These equations were first built using measured or ordinal indicator variables, and then were recalculated after dichotomizing select variables at several commonly used clinical cut points, including a CPP<50, GOS>2, ICP>20, LPR>40, or a PbtO2<15 or 20. Time zero for all patients was the estimated time of actual TBI.
All tests were two sided with the type I error rate set at 0.05. As the conducted analyses were exploratory, p values were not corrected for multiple statistical tests. Stata version 12.0 (Stata Corporation, College Station, TX) was used for all analyses.
Results
Patient demographics and outcomes
Although ten patients were enrolled into the study, two were subsequently excluded. The first patient died before any microdialysate samples could be collected. All of the microdialysate samples from the second patient were contaminated by red blood cells as the microdialysis catheter membrane fractured following its insertion into an area of CT hypodensity. The remaining eight patients had their microdialysis catheter tip placed into radiographically uninjured brain tissue in the right frontal lobe.
The baseline characteristics and clinical outcomes of the eight enrolled patients are presented in Table 1. Most patients were males (87.5%) and their median age was 46.0 (IQR, 30.0–57.5) years. Common CT head-identified abnormalities included subarachnoid hemorrhage (50%), subdural hematoma (50%), and/or cerebral contusion(s) (37.5%). The only female patient developed refractory intracranial hypertension secondary to diffuse cerebral edema and required a bifrontal decompressive craniectomy ∼70 h after TBI. Her results are, therefore, also described individually. Three (37.5%) patients died in the ICU after the 6 day study period. There were no complications attributed to microdialysis, including intracranial hemorrhages or infections.
The Marshall score is a categorization scheme for diffuse head injury based on initial CT head findings, which considers the status of the perimesencephalic cisterns, degree of midline shift, and presence of surgical intracranial masses.
CT, computed tomography; IQR, interquartile range; SD, standard deviation.
ICP, CPP, and brain oxygenation and metabolism after severe TBI
Figure 1 presents the ICP, CPP, PbtO2, glucose, and LPR over time for the eight patient cohort. Whereas ICP and LPR were mostly stable and CPP largely increased with time among the eight study patients, PbtO2 increased between 12 and 66 h before decreasing to approximately baseline levels. In contrast, ICP rapidly increased and CPP, PbtO2, and LPR decreased prior to decompression for the one patient who required a decompressive craniectomy. As expected, her ICP decreased and CPP and PbtO2 increased after craniectomy. Brain extracellular glucose generally decreased among all patients over time.
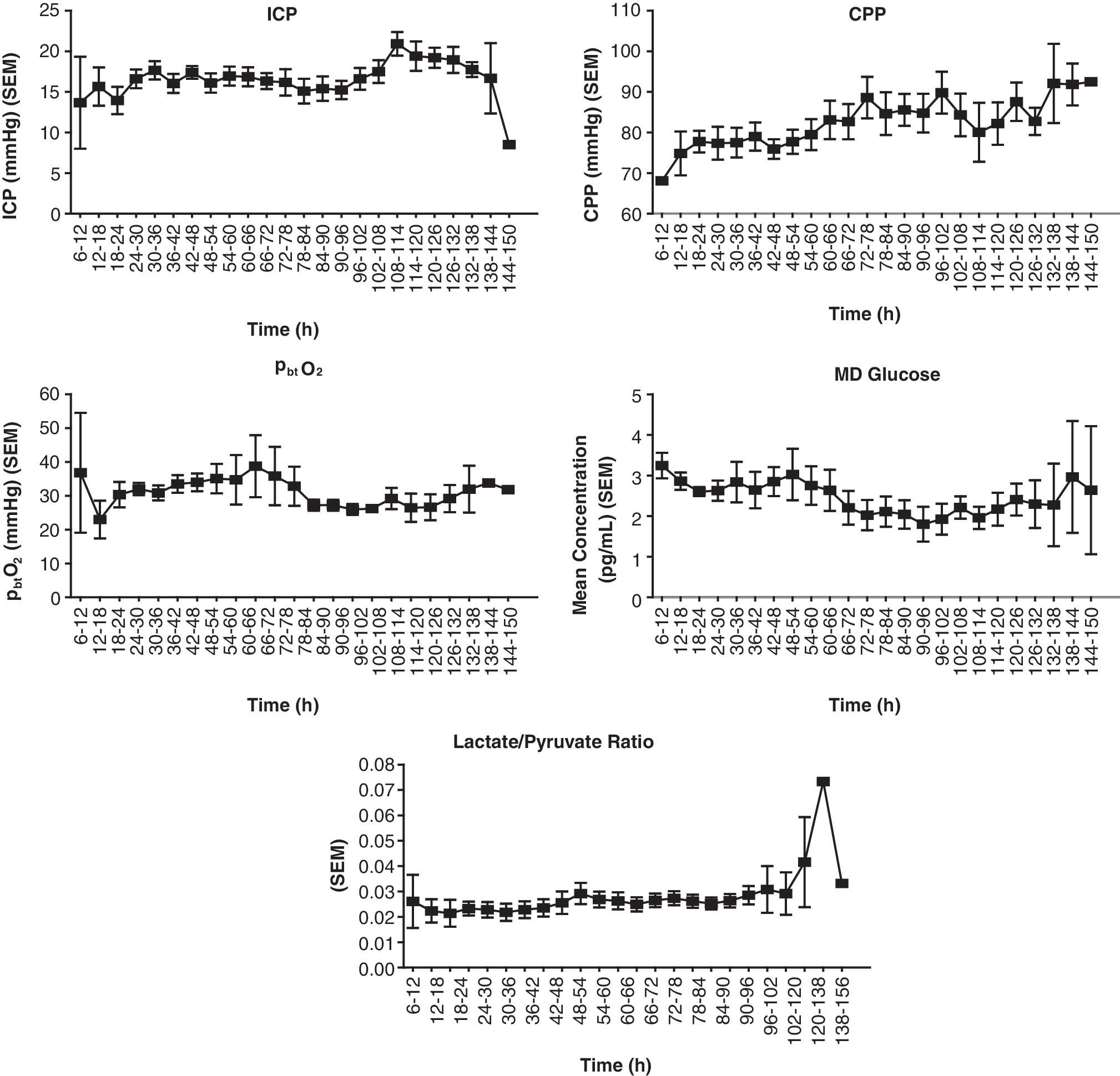
Cerebral physiology among the eight enrolled patients. CPP, cerebral perfusion pressure; ICP, intracranial pressure; MD, microdialysate; PbtO2, brain tissue oxygen tension; SEM, standard error of the mean.
Temporal MMP response in microdialysate and plasma after severe TBI
Severe TBI was associated with a markedly different MMP response in microdialysate and plasma after severe TBI, with MMP concentrations in plasma being higher than those in microdialysate (Figs. 2 and 3). As MMP concentrations were nearly identical in jugular bulb and arterial plasma over the study period (data not shown), only the arterial plasma MMP response has been presented. Further, although we measured MMP-12 and -13, these proteases were undetectable in all samples, and, therefore, data on their temporal response could not be presented.

Temporal matrix metalloproteinase response in microdialysate for the eight enrolled patients. MMP, matrix metalloproteinase; SEM, standard error of the mean.
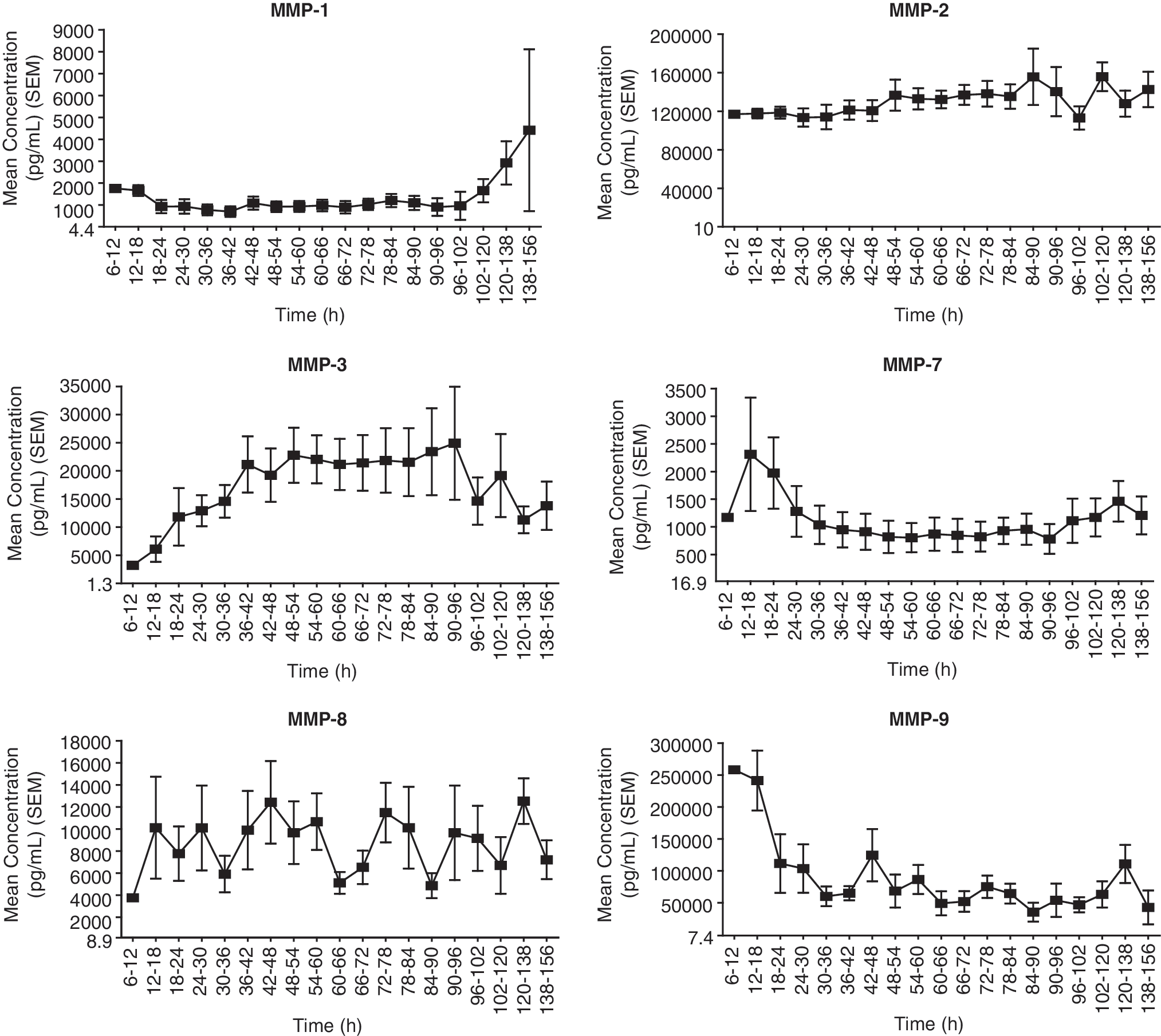
Temporal matrix metalloproteinase response in arterial plasma for the eight enrolled patients. MMP, matrix metalloproteinase; SEM, standard error of the mean.
In microdialysate, although the concentration of MMP-1 repeatedly spiked in concentration between 12 and 54 h, its levels were low, and near the assay detection limit throughout most of the latter part of the study. Although levels of MMP-1 were also low in plasma between 6 and 96 h, they increased in concentration between 96 and 156 h. MMP-2 and -3 levels peaked in microdialysate between 42 and 48 h, before declining to pre-peak low levels. MMP-2 plasma levels were high and relatively stable throughout the study. Plasma levels of MMP-3 gradually rose following severe TBI, plateaued in concentration between 36 and 96 h, and then declined. After an initial peak, plasma levels of MMP-7 declined and then were relatively stable. Although microdialysate concentrations of this MMP tracked near the assay detection limit during the earlier part of the study, they increased in concentration after 90 h. Microdialysate levels of MMP-8 and -9 were elevated in microdialysate after severe TBI and then declined with time. Whereas the plasma concentration of MMP-9 was also initially high and then progressively declined later in the study, the MMP-8 plasma level fluctuated, but appeared to slightly increase with time.
Temporal MMP response in microdialysate versus CSF after severe TBI
Among the three patients fitted with microdialysis and external ventricular drainage catheters, several potential differences in MMP temporal concentration profiles were observed between microdialysate and CSF (Fig. 4). Although the temporal concentration profile and levels of MMP-1, -8, and -9 were generally similar between these two compartments, the concentration of MMP-1 in CSF was higher between 12 and 30 h. Moreover, whereas microdialysate levels of MMP-2 and -3 were mostly low after severe TBI, their CSF levels were higher throughout the study period and displayed a different temporal profile. Levels of MMP-2 and -3 in CSF were initially high after severe TBI and then declined to lower levels between 84 and 156 h.
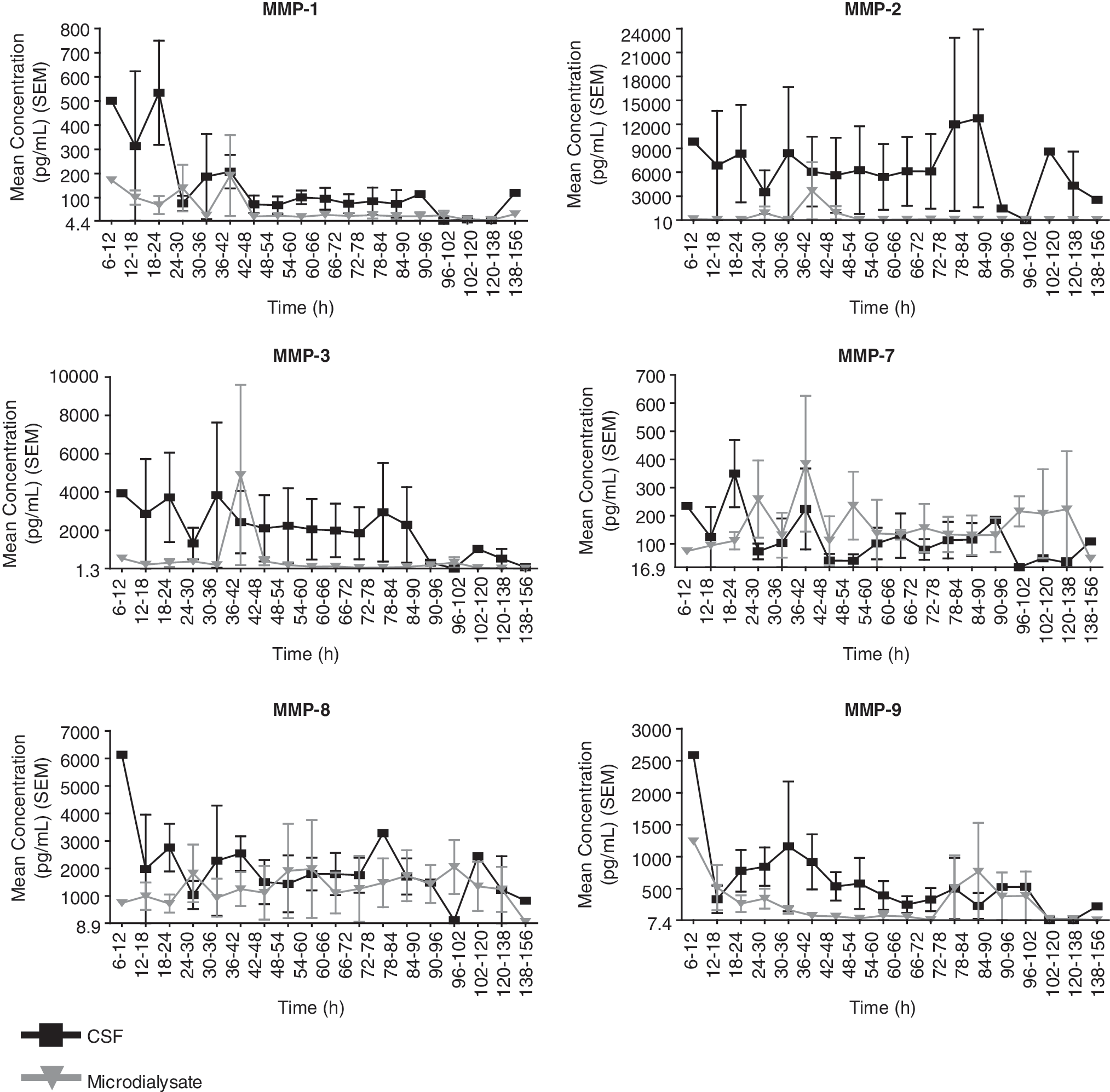
Temporal matrix metalloproteinase response in microdialysate versus cerebrospinal fluid among the three patients fitted with microdialysis and external ventricular drainage catheters (includes the patient who developed refractory intracranial hypertension). CSF, cerebrospinal fluid; MMP, matrix metalloproteinase; SEM, standard error of the mean.
Changes in the MMP response after decompressive craniectomy
The patient who developed diffuse cerebral edema and refractory intracranial hypertension demonstrated several differences in cerebral physiology and temporal MMP response as compared with the remainder of the cohort. In this patient, there was an increase in the plasma concentration of MMP-8 and -9 prior to the onset of refractory intracranial hypertension. Moreover, immediately following decompressive craniectomy, there was a rapid and large spike in the microdialysate concentration of MMP-8 and -9, which was not observed in plasma. As compared with the remainder of the cohort, MMP-3 plasma concentrations were also several-fold lower both before and after decompressive craniectomy, and MMP-3 peaked in microdialysate between 96 and 102 h.
Correlation between MMPs and cerebral physiology and clinical outcomes or findings
Exploratory analyses using generalized estimating equations suggested that the microdialysate concentration of MMP-8 was significantly associated with mortality (p=0.019) and GOS at hospital discharge (p=0.013). The mean microdialysate concentration of MMP-8 was 2.4-fold (939.48 (95% confidence interval [CI], 155.92–1723.03) pg/mL) higher among those who died after severe TBI than among those who survived. There was no association between microdialysate levels of any of the MMPs and the length of hospital or ICU stay. However, the mean microdialysate concentration of MMP-2 (p<0.001) and -7 (p=0.031) were significantly associated with post-resuscitation GCS score. The mean microdialysate level of MMP-7 was also significantly associated with CT Marshall score (p=0.0092). As compared with a Marshall score of 2 (basal cisterns present and/or midline shift ≤5 mm and/or no high- or mixed-density lesions >25 cc), the mean MMP-7 microdialysate concentration was 2.2-fold (168.08 [95% CI, 37.36–298.80] pg/mL) higher among those with a Marshall score of 5 or 6 (evacuated or unevaucated intracranial mass lesion). Moreover, the mean microdialysate level of MMP-8 increased with increasing ICP ([49.27 pg/mL]/mm Hg; 95% CI 9.03–89.51) whereas that of MMP-7 significantly decreased with increasing CPP ([-3.25 pg/mL]/mm Hg; 95% CI, -5.92 to -0.58). Finally, the mean microdialysate concentration of MMP-2 decreased with decreasing brain temperature ([-26.25 pg/mL]/°C; 95% CI, -17.41 to -35.09).
Correlation between MMPs and microdialysate measures
In addition to changes in the mean microdialysate concentrations of MMP-1, -2, -3, and -9 with increases in microdialysate glucose, the concentrations of MMP-1, -2, -3, -7, and -9 varied with the LPR (Table 2). Moreover, the mean microdialysate level of MMP-7 was 2.8-fold (312.83 [95% CI, 153.60–472.05] pg/mL) higher, whereas the mean microdialysate level of MMP-9 was 0.07-fold (184.63 [95% CI, 396.32–27.02] pg/mL) lower, among patients with a LPR>40 versus those with an LPR ≤40. Finally, although no association was found between MMPs and PbtO2 when examined on a continuous basis, there was a trend toward a 4.8-fold higher (1000.56 [95% CI, -97.37–2098.48] pg/mL) MMP-9 concentration among patients with a PbtO2<15 kPa versus those with a PbtO2 ≥15 kPa.
The coefficient and its 95% confidence interval may be interpreted as the mean change in MMP concentration per unit change in glucose or lactate/pyruvate ratio.
MMP, matrix metalloproteinase.
Discussion
Accumulating pre-clinical data suggests that matrix metalloproteinase (MMP) expression plays a critical role in the pathophysiology of secondary brain injury. 3 –5,8,9 This study is the first to report that the majority of the soluble MMPs are upregulated after severe TBI, and to simultaneously characterize each of their temporal responses in microdialysate, CSF, and jugular venous bulb and arterial plasma. Although based on only eight patients, our results suggest that the temporal MMP expression profile in the brain after severe TBI in humans may be similar to that reported by animal studies. 12 Moreover, the microdialysate concentration of select MMPs may correlate with outcomes after severe TBI, as we observed them to associate with mortality, neurological outcome, GCS, ICP, and CPP. These findings support the suggestions from animal investigations that the MMP response may have clinical relevance after acute brain injury.
We observed that different MMPs exhibited unique temporal concentration profiles in microdialysate and CSF after severe TBI in humans. 12 Although several potential differences between microdialysate and CSF were noted among the three patients simultaneously fitted with external ventricular drainage and microdialysis catheters, overall the temporal course of most MMPs was similar across these two fluids. Importantly, differences in biomarker concentrations between microdialysate and CSF have been suggested by some authors to reflect discrepancies in the function of the two main interfaces that exist between peripheral blood and structures of the CNS. 26 Although the blood–brain barrier has long been known to restrict entry of substances into the CNS, the function of the blood–CSF barrier is less well known, and some have suggested that it may serve as a route of elimination for substances from the brain. 26 –28 Moreover, as biomarkers such as MMPs are produced by cells of the CNS and secreted into the interstitial space, and then act on cell-surface receptors within the brain, microdialysate is likely the more relevant fluid for study. 26 The microdialysate concentrations of MMP-8 and -9 were observed to be relatively high after severe TBI and then to decline to lower levels by ∼ 48 h. After this decrease in the levels of MMP-8 and -9, a small spike in the microdialysate levels of MMP-2 and -3 occurred, followed by a gradual rise in the concentration of MMP-7. These findings are similar to that of another microdialysis study that observed levels of MMP-9 to be higher than MMP-2 in microdialysate, and then to gradually decline to lower concentrations over the first 48 h after TBI. 14
As MMPs have been reported to have a biphasic role following brain injury, the correct characterization of their temporal expression profile may have clinical relevance. Substrates for MMP-2 and -9 include critical components of intercellular tight junctions and the basal lamina of the blood–brain barrier. 4,12,29,30 Early expression of these MMPs has been associated with increased brain lesion volumes, cerebral edema, and/or neurological deficits following experimental brain trauma. 3,8,31,32 In contrast, MMP-3 is capable of removing proteins within the post-injury growth-inhibitory glial scar, and may contribute to remyelination, removal of CNS debris, and reshaping of the extracellular matrix following brain injury. 13 As such, this enzyme may support axonal regrowth and allow for efficient synapse reorganization and neurotransmission after TBI. 6,13,33 MMP-7 may also alter synaptic stability and reorganization, as two investigations have suggested that it may alter dendritic spine morphology after brain injury. 34,35 Therefore, based on animal data and the temporal MMP concentration profiles observed among our sample of eight patients, if an inhibitor of MMP-8 or -9 is designed or trialed in the future, this agent may have to be administered within the first 48 h, and before the microdialysate rise in MMP-3 and -7 concentration.
We observed several MMPs to be associated with clinical and surrogate findings or outcomes after severe TBI. Increased levels of MMP-8 were associated with elevated ICP, mortality, and neurological outcome among those with severe TBI. Although little data on the role of MMP-8 in TBI yet exist, several studies have shown that MMP-8 expression in experimental autoimmune encephalomyelitis (an animal model for multiple sclerosis) is associated with disease severity, 36,37 and one study reported that MMP-8-null mice exhibited significantly reduced inflammatory cell infiltrates and demyelinating lesions. 38 MMP-7 was associated with CPP and CT Marshall score, with increased levels of MMP-7 being observed among patients with intracranial mass lesions on head CT. Although the importance of these findings in the current study remains unknown, increased expression of MMP-2 and -9 has previously been demonstrated in resected contusion tissue from patients with TBI as compared with lobectomy brain tissue controls. 39
A significant association between the microdialysate concentrations of MMP-1, -2, -3, and 9 and brain glucose was also observed, suggesting that a link between extracellular matrix remodelling and brain glucose may exist following severe TBI. Hyperglycemia is common among critically ill patients with severe TBI, and very loose glucose control has been linked with worsened neurological outcomes.
40
Mechanisms whereby hyperglycemia may be harmful to the acutely injured brain include free radical formation with oxidative injury, activation of N-methyl-
Limitations
Our study has several limitations. First, as the study was exploratory, some of the associations reported herein may have represented type I errors. Second, we were unable to adjust our associations between MMPs and outcomes for known prognostic factors given that our sample included only eight patients. Therefore, based on the data reported in this study alone, it would be too early to extrapolate our findings to clinical utility. Third, although the differences in magnitude and/or temporal expression of MMPs between microdialysate and plasma could have been the result of a greater degree of production in the periphery versus the brain, these observations are limited, given that they could have been the result of a sampling error, as the microdialysis probe tip was placed into uninjured brain rather than the traumatic penumbra. Although this limitation may also explain some of the differences observed between CSF and microdialysate, probe placement was performed in accordance with current guidelines for microdialysis in neurointensive care. 19 Finally, although the significance of the measurement of total (active and inactive) versus active MMP expression is as of yet unstudied, we were only able to measure total MMP levels in this study.
Conclusion
In summary, similar to the findings of animal models of TBI, we found that different MMPs exhibited unique temporal concentration profiles in microdialysate, CSF, and blood after severe TBI. MMP-8 and -9, which have been linked with blood–brain barrier disruption, cerebral edema, neuronal death, and inflammatory cell infiltration, were expressed early after severe TBI, and remained elevated until ∼ 48 h. After their levels decreased, MMP-3 peaked in concentration in microdialysate, followed by a gradual rise in the microdialysate concentration of MMP-7. These MMPs may have a role in recovery from CNS injury. As the brain extracellular concentration of select MMPs was significantly associated with several clinical and surrogate outcomes after severe TBI, the MMP response may have clinical relevance. However, our findings should be confirmed by future investigations.
Footnotes
Acknowledgments
This work was supported by grants from Alberta Innovates – Health Solutions (formally the Alberta Heritage Foundation for Medical Research [awarded to Dr. Zygun]), the Canadian Intensive Care Foundation (awarded to Dr. Zygun), and the Snyder Chair for Translational Research in Critical Care Medicine (awarded to Dr. Kubes). Dr. Roberts is supported by an Alberta Innovates – Health Solutions Clinician Fellowship Award and funding from the Clinician Investigator and Surgeon Scientist Programs at the University of Calgary. Dr. Jenne is funded by an Alberta Innovates – Health Solutions Postdoctoral Fellowship Award.
Author Disclosure Statement
No competing financial interests exist.