
Abstract
An increasing number of preclinical investigations have suggested that the degree of expression of the matrix metalloproteinase (MMP) family of endopeptidases may explain some of the variability in neurological damage after traumatic brain injury (TBI). As cytokines are a prominent stimulus for MMP expression in animals, we conducted a prospective multimodal monitoring study and determined their association with temporal MMP expression after severe TBI in eight critically ill adults. High cutoff, cerebral microdialysis (n=8); external ventricular drainage (n=3); and arterial and jugular venous bulb catheters were used to measure the concentration of nine cytokines and eight MMPs in microdialysate, cerebrospinal fluid (CSF), and plasma over 6 days. Severe TBI was associated with a robust central inflammatory response, which was largely similar between microdialysate and CSF. At all time points after injury, this response was predominated by the pro-inflammatory cytokines interleukin-6 (IL-6) and IL-8. Use of univariate generalized estimating equations suggested that the concentration of several MMPs varied with cytokine levels in microdialysate. The largest of these changes included increases in microdialysate concentrations of MMP-8 and MMP-9 with increases in the levels of IL-1α and -2 and IL-1α and -2 and TNF-α, respectively. In contrast, the microdialysate level of MMP-7 decreased with increases in microdialysate concentrations of IL-1β, -2, and -6. These findings support the observations of animal studies that cross-talk exists between the neuroinflammatory and MMP responses after acute brain injury. Further study is needed to determine whether this link between cerebral inflammation and MMP expression may have clinical relevance to the care of patients with TBI.
Introduction
I
Upregulation of the matrix metalloproteinase (MMP) family of endopeptidases may be an important pathway associated with secondary brain injury after TBI. 12 –18 Increased expression and activity of the proteases MMP-2 and -9 after TBI in animals have been shown to contribute to blood–brain barrier degradation, cerebral edema, neuronal death, and the associated severity of neurological deficits. 12 –14,17,18 In contrast, more delayed expression of MMP-3 after experimental brain injury has been associated with brain repair in some studies, including removal of central nervous system (CNS) debris and reorganization of synaptic environments. 19 As MMPs therefore appear to have a dual role after TBI, any consideration of an attempt to develop drugs to interrupt their destructive effects, or enhance their role in injury resolution, must be done with a thorough understanding of their temporal expression profile and molecular regulation.
Cerebral cytokines have previously been shown in animal investigations to constitute a prominent stimulus for the expression of MMPs and their release into the brain. 20 –22 CNS-derived immune cells, neurons, and microglia secrete a host of cytokines after TBI, and several of these cytokines, including interleukin-1β (IL-1β) and tumor necrosis factor-α (TNF-α), have been shown in vitro and in vivo to increase the transcription and/or activity of MMP-3 and -9. 21 –25 By influencing the production of MMPs, cytokines may indirectly be responsible for some of the destruction or dysfunction of the blood–brain barrier that frequently occurs during CNS inflammation. 21,23 –25 It is also possible that these inflammatory mediators could orchestrate or modulate the dual MMP response that occurs after TBI.
To better understand the MMP response and its regulation after severe TBI in humans, we conducted the Proteomics of Severe TBI study. We reported the first part of this study in an accompanying article (page 00), which described the temporal course of MMP production after severe TBI and its relationship with several surrogate and clinical outcomes. 26 In this second part, we sought to characterize the temporal cytokine response in microdialysate, cerebrospinal fluid (CSF), and jugular bulb and arterial plasma after severe brain trauma and its association with the MMP response. We also sought to explore whether an association exists between the cerebral inflammatory response and other non-MMP microdialysate measures, cerebral physiology, and various surrogate and clinical outcomes.
Patients and Methods
This study was approved by the Conjoint Health Research Ethics Board (CHREB) at the University of Calgary and is registered online (
Patients
Consecutive mechanically ventilated adults admitted to the Foothills Medical Centre (Calgary, Alberta, Canada) intensive care unit (ICU) between July 1, 2007 and September 31, 2010 were prospectively screened for study eligibility. Eligibility criteria included: (1) age ≥18 years, (2) severe TBI (defined as a post-resuscitation Glasgow Coma Scale [GCS] score ≤8 27 ), (3) requirement for invasive intracranial pressure (ICP) monitoring, 28 and (4) life expectancy >72 h. Exclusion criteria included severe TBI that had occurred >12 h before eligibility screening.
Patient management and multimodal monitoring, including cerebral microdialysis
Study patient clinical care was coordinated by fellowship-trained intensivists or neurointensivists according to recommendations from the Brain Trauma Foundation. 29 Treatment often included placement of peripheral arterial and jugular venous bulb catheters. Within 24 h of ICU admission, patients also had a CT-visible, gold-tipped cerebral microdialysis catheter with a nominal weight cutoff of 100 kDa (CMA-71, CMA Microdialysis, Stockholm, Sweden) inserted. In accordance with present recommendations for microdialysis in neurocritical care, probes were implanted into non-injured brain parenchyma on CT through a right frontal burr hole whenever safe and feasible. 30
After CT confirmation of correct cerebral microdialysis catheter tip placement, the catheter probe was connected to a CMA 103 perfusion pump (CMA Microdialysis). Perfusion fluid (CMA Microdialysis) was then passed through the catheter at 0.3 μL/min. Obtained microdialysate sample vials were immediately analyzed in 1 h intervals at the bedside to determine levels of glucose, lactate, pyruvate, and glycerol using the CMA 600 (CMA Microdialysis) enzyme photometric analyzer. Microdialysate was pooled every 6 h and then aliquoted and stored at −80°C until cytokine and MMP analyses could be performed.
Clinical and physiologic data collection
We collected data on patient age, sex, height, weight, injury mechanism, study entry and post-resuscitation GCS, pupillary light reactivity at Emergency Department presentation, and co-morbid conditions. CT head findings were reviewed to grade TBI severity using the Marshall score. 31,32 Data on mean arterial pressure (MAP), ICP, cerebral perfusion pressure (CPP), body and brain temperature, and arterial (SaO2) and jugular venous oxygen saturation were also recorded at least hourly until discontinuation of the microdialysis probe. Neurological outcome was assessed at hospital discharge by one of the investigators using the Glasgow Outcome Scale (GOS) score. 33
Blood and CSF collection and processing and analytical methods
We used the validated Luminex® assay from R&D Systems (Minneapolis, MN) to quantify the concentrations of IL-1α, -1β, -2, -4, -5, -6, -8, -10 and TNF-α as well as MMP-1, -2, -3, -7, -8, -9, -12, and -13 according to manufacturer's instructions. 34 As beads from the Luminex® multiplexing kit bind to both the active and inactive forms of the MMP proteins, this assay measures overall MMP levels. Briefly, undiluted microdialysate or CSF and diluted plasma or serum were thawed quickly at 37°C, centrifuged at 20800 g at 4°C for 10-min, and then stored on ice. A total of 25 μL of sample were then distributed to their appropriate wells. The plate was then incubated, in the dark, for 2 h at room temperature on a plate shaker set at 500-rotations-per-minute (rpm). Wells were subsequently washed three times with 100 μL of wash buffer and then 25 μL of diluted biotin antibody cocktail was added to each well. Thereafter, the plate was incubated, in the dark, for 1 h at room temperature on a plate shaker set at 500 rpm. Wells were subsequently washed three times with 100 μL of wash buffer, and then 25 μL of diluted Streptavidin-PE was added to each well and the plate was incubated for 30 min at room temperature on a plate shaker set at 500 rpm. Wells were then washed three times with 100 μL of wash buffer. Subsequently, 75 μL of wash buffer was added to each well, and the plate was read using the Luminex® 200 apparatus (Applied Cytometry Systems, UK). The data were analyzed with StarStation V.2.3 (Applied Cytometry Systems, UK).
Statistical analyses
Normally and non-normally distributed data were described using means (with standard deviations [SD]) and medians (with interquartile ranges [IQR]) as appropriate. The association between cytokine concentrations, averaged 6 h physiologic data, and MMP concentrations (as well as various outcomes) was examined by fitting univariate population-averaged panel-data models using generalized estimating equations with an exchangeable within-group correlation structure. 35 These models constitute a valid method for accounting for correlated data when the nature of the correlation structure is unknown, and use all of the observed data points to estimate the expected mean change in cerebral cytokine concentrations per each one unit increase in the value of a specified predictor variable. 35 They were first fit using measured or ordinal predictor variables, and then were refit after dichotomizing these predictor variables at several commonly used clinical cutpoints, including a CPP<50, GOS>2, ICP>20, lactate/pyruvate ratio >40, or a brain tissue oxygen tension (PbtO2) <15 or 20.
We considered two-sided p values<0.05 to be statistical significant. As the analysis was entirely exploratory, calculated p values were not corrected for multiple statistical tests. Stata version 12.0 (Stata Corporation, College Station, TX) was used for all analyses.
Results
Patient demographics, clinical course, and outcomes
Although 10 patients were enrolled in the study, two were subsequently excluded. The first patient died before any microdialysate samples could be collected, while all of the microdialysate samples were contaminated by erythrocytes in the second patient because the catheter membrane fractured after insertion. All eight included patients had their microdialysis catheter tip placed into radiographically uninjured brain tissue in the right frontal lobe.
The baseline characteristics and clinical outcomes of the eight enrolled patients are presented in Table 1. Most patients were males (87.5%) and their mean age was 43.3 (SD, 16.4) years. The most common head CT-identified abnormalities included subarachnoid hemorrhage (50%), subdural hematoma (50%), and/or cerebral contusion(s) (37.5%). The only enrolled female patient developed refractory intracranial hypertension secondary to diffuse cerebral edema and needed a bifrontal decompressive craniectomy approximately 70 h after study enrollment. Her results are also described alone. At the time of operation, the cerebral microdialysis, but not the external ventricular drainage, catheter was replaced.
SD, standard deviation; IQR, interquartile range; CT, computed tomography.
The Marshall score is a categorization scheme for diffuse head injury based on initial CT head findings that considers the status of the peri-mesencephalic cisterns, degree of midline shift, and presence of surgical intracranial masses.
Temporal cytokine response in microdialysate, CSF, and plasma after severe TBI
Severe TBI was associated with a robust inflammatory response (Figs. 1 –3). At all time points after TBI, this response was predominated by the pro-inflammatory cytokines IL-6 and -8 in microdialysate and CSF. While the concentration of IL-6 and -8 were high in both fluids after severe brain trauma and then gradually declined with time, IL-8 increased in concentration again between 84 and 156 h after injury in both microdialysate and CSF. Although levels of IL-1β, IL-1α, and TNF-α were significantly less than that of IL-6 and -8, they were nonetheless elevated in both microdialysate and CSF early after TBI. While levels of IL-5 were measured in microdialysate and CSF, levels of this cytokine approximated the lower detection limit in all samples, and therefore data on its temporal response could not be confidently presented.
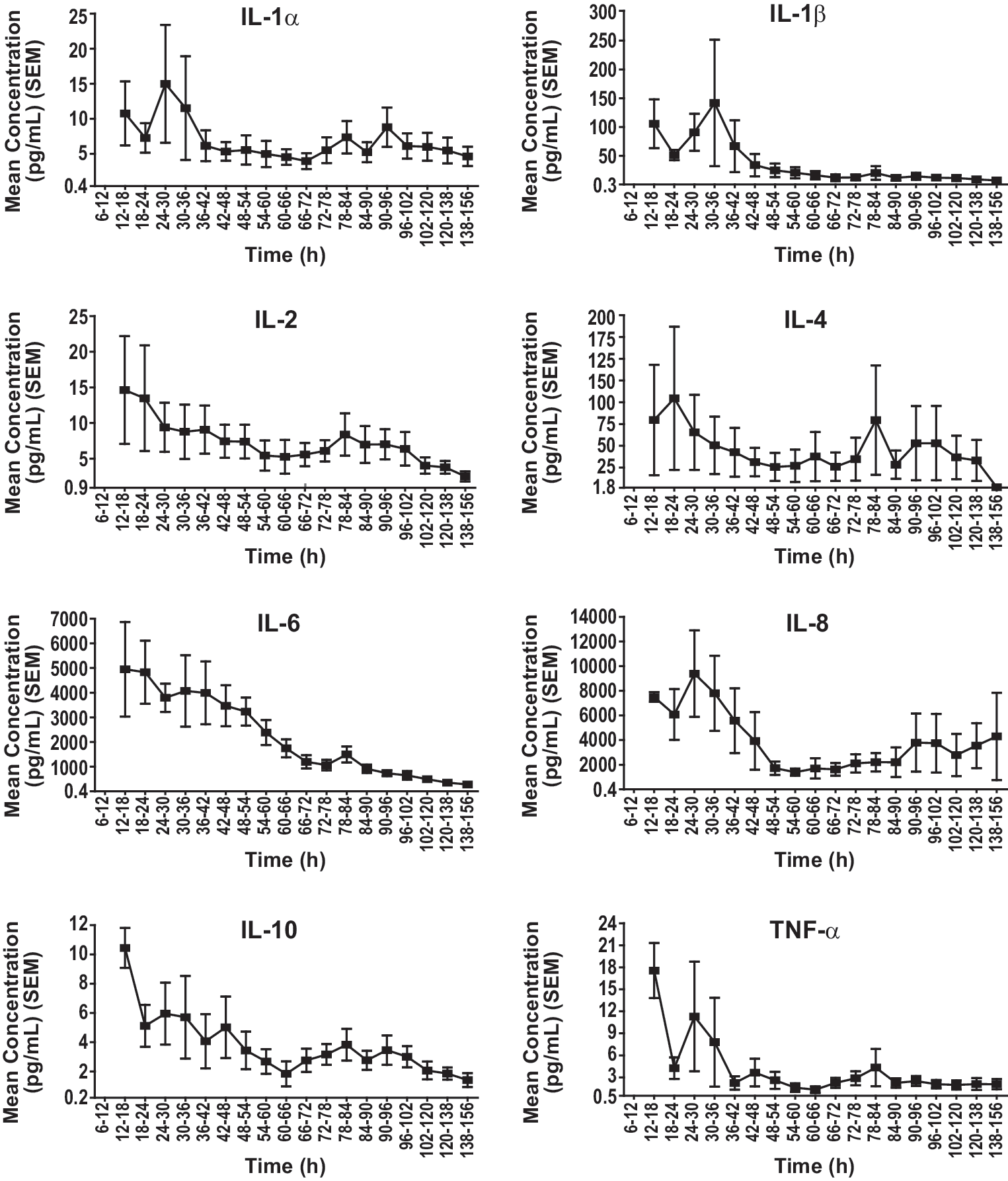
Temporal cerebral cytokine response in microdialysate for the eight enrolled patients. IL, interleukin; SEM, standard error of the mean; TNF, tumor necrosis factor.

Relationship between the cerebral cytokine response in microdialysate and cerebrospinal fluid for the three patients fitted with microdialysis and external ventricular drainage catheters. IL, interleukin; SEM, standard error of the mean; TNF, tumor necrosis factor; CSF, cerebrospinal fluid.
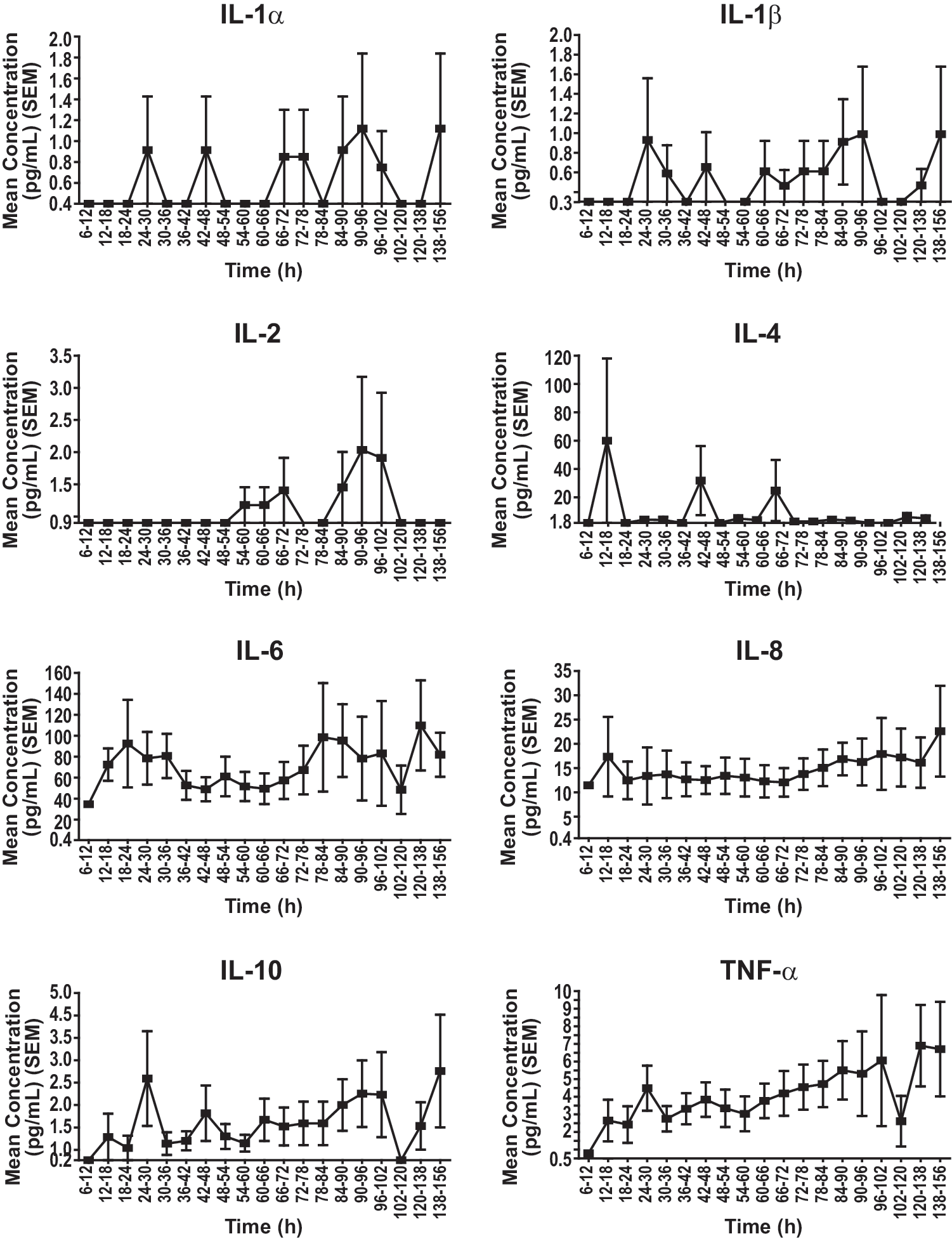
Temporal cerebral cytokine response in plasma for the eight enrolled patients. IL, interleukin; SEM, standard error of the mean; TNF, tumor necrosis factor.
The levels of most cytokines were similar between microdialysate and CSF among the three patients also fitted with external ventricular drainage catheters. While slight differences appeared to be present in the concentration of IL-2 and -10 and TNF-α across these two fluids between 6 and 72 h (Fig. 2), these differences were explained by the inclusion of the discrepant CSF mediator data afforded by the patient in whom refractory intracranial hypertension developed. After removing her data from the CSF drainage cohort, the temporal cytokine concentration profile in microdialysate and CSF appeared nearly identical at all time points (data not shown).
As microdialysate and CSF cytokine levels were significantly greater than those observed in jugular bulb and arterial plasma, the neuroinflammatory response appeared mostly limited to the CNS (Fig. 3 vs. Fig. 2). Further, no difference in cytokine concentrations or temporal cytokine expression was observed between jugular bulb and arterial plasma (data not shown). IL-6 and -8 were again the predominant cytokines measured in plasma after severe TBI, with concentrations of IL-1α, -1β, -2, and -4 being near the detection limit of the assay, and those of IL-5 falling below this limit. In contrast to the concentration-time pattern observed in microdialysate and CSF, however, levels of both IL-6 and -8 were initially low in plasma and then slightly increased (rather than decreased) with time.
Association between cerebral cytokines and clinical or surrogate outcomes or findings
Using generalizing estimating equations, we failed to observe an association between the mean microdialysate concentration of any cerebral cytokine and mortality, GOS at hospital discharge, or length of hospital stay. However, the mean microdialysate level of IL-4 increased with length of ICU stay ([4.53 pg/mL]/d; 95% confidence interval [CI], 2.53 to 6.53). Associations between post-resuscitation GCS score and the mean microdialysate concentration of IL-2 (p<0.001), -4 (p<0.001), and -6 (p=0.014) and TNF-α (p=0.002) were also observed. Moreover, the mean microdialysate concentrations of IL-1β and -4 were 3.7 fold (39.19 pg/mL [95% CI, 1.22 to 77.17]) and 13.7 fold (38.46 pg/mL [95% CI, 0.40 to 76.51]) higher, respectively, among those with a bilateral absence of pupillary light reactivity at presentation compared with those with unilateral or no pupillary light abnormalities. Finally, the mean microdialysate concentration of TNF-α was 2.1 fold (2.68 pg/mL [95% CI, 0.0020 to 5.37]) higher among those with unilateral or bilateral absence of pupillary light reactivity at presentation compared with those with no pupillary light abnormalities.
The mean microdialysate concentration of several cytokines also varied with selected surrogate measures. The mean microdialysate concentration of IL-2 decreased with increasing ICP ([−0.32 pg/mL]/mm Hg; 95% CI, −0.0032 to −0.64) while the mean microdialysate concentration of IL-6 ([−27.69 pg/mL]/mmHg; 95% CI, −2.62 to −52.76) and −8 ([−55.51 pg/mL]/mm Hg; 95% CI, −23.12 to −87.90) decreased with increasing CPP. Moreover, the mean microdialysate concentration of TNF-α was 2.8 fold (5.94 [95% CI, 3.45 to 8.44] pg/mL) higher among patients with an ICP>20 versus ≤20 while the mean microdialysate concentration of IL-8 was 3.5 fold (6149.03 [95% CI, 2714.54 to 9583.52] pg/mL) higher among those with a CPP<50 versus ≥50. Although microdialysate cytokine concentrations did not vary with PbtO2 when examined on a continuous basis, the mean microdialysate levels of IL-6, -8, and -10 and TNF-α were higher among those with a PbtO2<15 versus ≥15 (Table 2). Moreover, the mean microdialysate concentration of several cytokines varied with microdialysate glucose, lactate/pyruvate ratio, and a lactate/pyruvate ratio >40 versus ≤40 (Table 2).
The coefficient can be interpreted as the mean change in cytokine concentration per unit increase in the variable of interest.
IL, interleukin; TNF, tumor necrosis factor.
Correlation between the MMP and cytokine responses after severe TBI
Significant changes in the mean microdialysate concentrations of MMP-1, -7, -8, and -9 occurred with changes in the mean microdialysate concentrations of several cytokines (Table 3). The mean microdialysate concentration of MMP-1 significantly increased with IL-2 and -10 and TNF-α whereas the mean microdialysate concentrations of MMP-8 and -9 increased with all measured cytokines except IL-8 and -10, respectively. Moreover, the mean microdialysate concentration of MMP-7 significantly decreased with increases in the microdialysate concentrations of IL-1β, -2, and -6. The largest of these changes included increases in the mean microdialysate concentrations of MMP-8 and -9 with increases in the levels of IL-1α and -2 as well as IL-1α and -2 and TNF-α, respectively.
The coefficient can be interpreted as the mean change in cytokine concentration per unit increase in the variable of interest.
IL, interleukin; TNF, tumor necrosis factor.
Association between cytokine and MMP responses before and after decompressive craniectomy
Data on the combined temporal cytokine and MMP response in microdialysate from the one patient in whom diffuse cerebral edema and refractory intracranial hypertension developed are shown in Figure 4. Interestingly, compared with the entire study cohort, this patient had a suppressed expression of MMP-8 and the pro-inflammatory cytokines IL-6 and -8, as well as an increased expression MMP-9 and the anti-inflammatory cytokines IL-2 and -4, before the development of refractory intracranial hypertension. Moreover, concentrations of IL-1α, -1β, -2, and -8 and MMP-8 and -9 were initially relatively high in this patient. After decompressive craniectomy, there was a rapid and dramatic spike in the concentrations of IL-1α, -1β, -2, -4, -6, and -8 and TNF-α as well as MMP-8 and -9 in microdialysate. Interestingly, concentrations of IL-1β, -4, and -8 in microdialysate appeared to spike before the observed increase in MMP-8 and -9 in this patient. The post-decompression MMP-9 microdialysate spike also preceded the observed increase in MMP-8 levels.

Temporal cerebral cytokine and matrix metalloproteinase response in the one patient in whom refractory intracranial hypertension developed before and after decompressive craniectomy. IL, interleukin; TNF, tumor necrosis factor; MMP, matrix metalloproteinase.
Discussion
The primary goal of the second part of this prospective multimodal monitoring study was to understand the relationship between the temporal cytokine and MMP responses after severe TBI in humans. We observed that severe TBI was associated with a robust central inflammatory response predominated by levels of the pro-inflammatory cytokines IL-6 and −8. Interestingly, although based on only three patients, levels of most cytokines were similar between microdialysate and CSF among patients also fitted with external ventricular drainage catheters. Further, the mean concentration of various cytokines varied with several clinical and surrogate outcomes and with levels of MMP-1, -7, -8, and -9. These findings support the observations in animal studies that the neuroinflammatory response may have clinical importance and cross-talk may exist between the cerebral inflammatory and MMP responses after brain injury.
In this study, a unique temporal pattern of cerebral extracellular cytokine production was observed. IL-6 and -8 were elevated in microdialysate after severe TBI and the initiation of cerebral microdialysis. This observation was to be expected because IL-6 has previously been shown to be significantly elevated in these fluids after TBI 36 –39 and likely has pro-inflammatory and neuroprotective roles in the setting of acute brain injury. 22 Moreover, IL-8 is a well-established chemoattractant that has also been shown to be expressed in high concentrations in microdialysate and CSF after TBI. 39 –41 Its expression and activity has been linked with recruitment and infiltration of blood-borne neutrophils into the CNS and increased blood–brain barrier permeability. 22,42 Further, although microdialysate levels of IL-1α and -1β and TNF-α were substantially lower than those of IL-6 and -8 in this study, each of these cytokines were nonetheless elevated compared with plasma. In agreement with the findings of others, levels of TNF-α appeared to already be declining at the initiation of microdialysis, possibly supporting the suggestion that this cytokine may have an early role in coordinating the neuroinflammatory response. 22,38
We found the extracellular brain concentration of several cytokines to be associated with several clinical and surrogate outcomes, including length of ICU stay, GCS and CT Marshall scores, pupillary abnormalities, ICP, CPP, and microdialysate glucose, PbtO2, and lactate/pyruvate ratio. Although associations between cytokines and outcomes have also variably been reported by others, suggesting that the level of expression of some cerebral cytokines after TBI may have clinical relevance, these results should be interpreted cautiously because they were unadjusted for age, GCS scores, and other factors. 22 Moreover, while generalized estimating equations are a valid statistical method of examining correlated data, which calculate a panel-averaged result rather than a true mean, many uncorrected statistical tests were conducted. Although this was done because our intent was for these analyses to be exploratory, we cannot exclude the possibility of a type I error for one or more of our findings.
Most importantly, in support of accumulating preclinical data suggesting that the expression or release of MMPs may be regulated by cerebral cytokine production, 20,21 we observed that the microdialysate concentration of many of the measured cytokines significantly correlated with levels of MMP-1, -7, -8, and -9. The largest of these changes included increases in the mean microdialysate concentrations of MMP-8 and -9 with increases in the levels of IL-1α and -2 as well as IL-1α and -2 and TNF-α, respectively. The above associations are largely in agreement with the finding that stimulation of cultured astrocytes or microglia with the pro-inflammatory cytokines IL-1α or -1β and TNF-α induce expression and/or increase levels of MMP-2, -3, and/or -9. 21,43 –47 Moreover, direct injection of TNF-α into rat brain leads to elevated expression and activity of MMP-3 and -9. 21,24 Because neurons under cellular stress or undergoing apoptosis after injury release MMP-3, which triggers microglial activation and release of IL-1β and -6 as well as TNF-α, 15,15,21,48 MMPs may also be capable of modulating the ongoing inflammatory response rather than simply inducing it.
If our preliminary findings are confirmed by future studies, the association between the cerebral inflammatory and MMP response may afford a novel opportunity for development of neuroprotective agents that modulate MMP expression and/or activity. 49 In animal models of brain and spinal cord injury, MMP inhibitors reduce cerebral edema and/or neural tissue damage. 50 –52 Activation of the extracellular regulated kinase-mitogen activated protein kinase (MAPK) pathway, which is upregulated after TBI, has previously been shown to increase expression of MMP-9, suggesting that this may be the upstream pathway responsible for MMP-9 activation after brain trauma. 13 Interestingly, IL-6 is also capable of activating the MAPK pathway in cultured human neuronal cells, 49,53 and inhibition of this pathway reduces expression of MMP-9 by TNF-α in vascular cell cultures. 13,54,55 Whether this pathway is principally responsible for MMP upregulation in humans after severe TBI needs further study.
Conclusion
This prospective cohort study found that severe TBI was associated with a robust central cytokine response predominated by the pro-inflammatory cytokines IL-6 and -8. Importantly, concentrations of several cytokines were significantly associated with clinical and surrogate outcomes and with levels of MMP-1, -7, -8, and -9. Therefore, the cerebral inflammatory response to severe TBI may have clinical importance and influence or be influenced by the production of MMPs. These findings support those of animal investigations that MMP expression and activation may be an additional mechanism whereby CNS inflammation could be harmful after brain injury. Further study is needed to determine whether this link between cerebral inflammation and MMP expression may have clinical relevance to the care of patients with TBI.
Footnotes
Acknowledgments
This work was supported by grants from Alberta Innovates–Health Solutions (formally the Alberta Heritage Foundation for Medical Research [awarded to Dr. Zygun]), the Canadian Intensive Care Foundation (awarded to Dr. Zygun), and the Snyder Chair for Translational Research in Critical Care Medicine (awarded to Dr. Kubes). Dr. Roberts is supported by an Alberta Innovates–Health Solutions Clinician Fellowship Award and funding from the Clinician Investigator and Surgeon Scientist Programs at the University of Calgary. Dr. Jenne is funded by an Alberta Innovates–Health Solutions Postdoctoral Fellowship Award.
This work was presented at the 10th Annual Neurocritical Care Society Meeting in Denver, CO, on October 4 to 7, 2012.
Author Disclosure Statement
No competing financial interests exist.