
Abstract
Age has been identified as an independent risk factor for poor outcome following head injury in the elderly, and postulated reasons for this include nature, nurture, and variations in management. Do elderly head injuries do worse because of a self-fulfilling prophecy of poorer management? The aim of this study was to review the management of patients with cerebral contusions according to age to identify any trends. We retrospectively reviewed prospectively collected national data on cerebral contusion admissions between March 14, 1988, and May 4, 2012, to UK hospitals held in the Trauma Audit and Research Network database. Patients were included in the study if they had cerebral contusion(s) with an abbreviated injury score (AIS) of 3 or more; no other head injury with a AIS score of 4 or more, or no injury in any other body region with AIS score of 3 or more, and known outcome data. In total, 4387 patients met the inclusion criteria. Mortality was found to increase with increasing age (p<0.001). However, time from admission to CT head imaging (p=0.003) and the likelihood of not being transferred to a center with acute neurosurgical care facilities (p<0.001) increased with increasing age, too. Further, there was a significant trend for the most senior grade of doctor to review more younger patients and for only the most junior grade of doctor to review more older patients (both, p<0.001). To conclude, our data suggest differences in management practice may contribute to the observed differences in mortality between younger and older patients suffering brain contusions.
Introduction
The aim of this study was to review national data on patients of all ages presenting with brain contusions to ascertain differences in management and mortality.
Methods
We undertook a retrospective review of prospectively collected national data on cerebral contusions from the Trauma Audit and Research Network (TARN;
The criteria for inclusion in this study were individuals who met all four conditions, as follows: • Cerebral contusion with abbreviated injury score (AIS) of 3–5 • No other head injury with an AIS score of 4–5 • No injury in any other body region with AIS score of 3–5 • Outcome data is known (within thirty days of admission to hospital)
The AIS is an anatomically based coding system widely used for grading the severity of traumatic injuries. Data were collected on mortality rates and whether subjects were treated at a specialist neurocenter or non-neurocenter; a neurocenter was defined as a hospital with acute neurosurgical care facilities. For those subjects who were direct admissions to the center that submitted the TARN data, we also collected data on the median time from presentation to computed tomography (CT) of the head and the grade of the most senior doctor reviewing that patient. Subjects were grouped into age deciles for the purposes of comparison.
Statistical analyses were performed using SPSS 19.0 (SPSS Inc., Chicago, IL). We used two statistical tests for trend analysis: the linear trend test in the logit scale and the Jonckheere's trend test. The linear trend test was used to analyze the risk of mortality by age, as mortality (the dependent variable) is binary (i.e., one is either dead or alive); the data were converted into logit to overcome the use of percentage mortality data in a linear regression analysis (i.e., for percentage, p, we converted as follows: log[p/(100-p)]). For the other trend tests not involving a binary dependent variable—namely admission rates to a neurocenter, time to head CT, and seniority of doctor reviewing a patient—Jonckheere's trend test was used. While the Kruskal-Wallis test also can be used when analyzing non-parametric data in an independent samples (between-groups) design such as ours, the Jonckheere's trend test was chosen as it has more statistical power when the populations from which the data are drawn are ordered a priori (i.e., in our dataset, according to age). Chi square analysis was also employed to look at mortality differences between neurocenter and non-neurocenter admissions.
Results
Baseline characteristics
In total, 4387 subjects were included in our study, and 3171 (72.3%) of these were direct admissions to the center that submitted the TARN data (as opposed to referrals from another unit). There were 3281 (75%) males in our cohort overall. The largest age band was 20 to 29 years (19.3%, n=845; Table 1). Our cohort included 578 (13.2%) subjects who were 70 years or older. The most common presenting Glasgow Coma Scale score was 15 (n=1166, 27%; Figure 1), and this did not differ significantly between age groups or gender. Of all the patients, 59.6% (n=2614) were admitted to a neurocenter (Table 1), with the remainder admitted to a non-neurocenter. Table 2 illustrates the proportion of subjects transferred to another center for ongoing care according to age. As shown by Figure 2 and Table 1, there was a trend for younger patients to be admitted to neurocenters, and older patients to be admitted to non-neurocenters (Jonckheere's trend test; p<0.001).
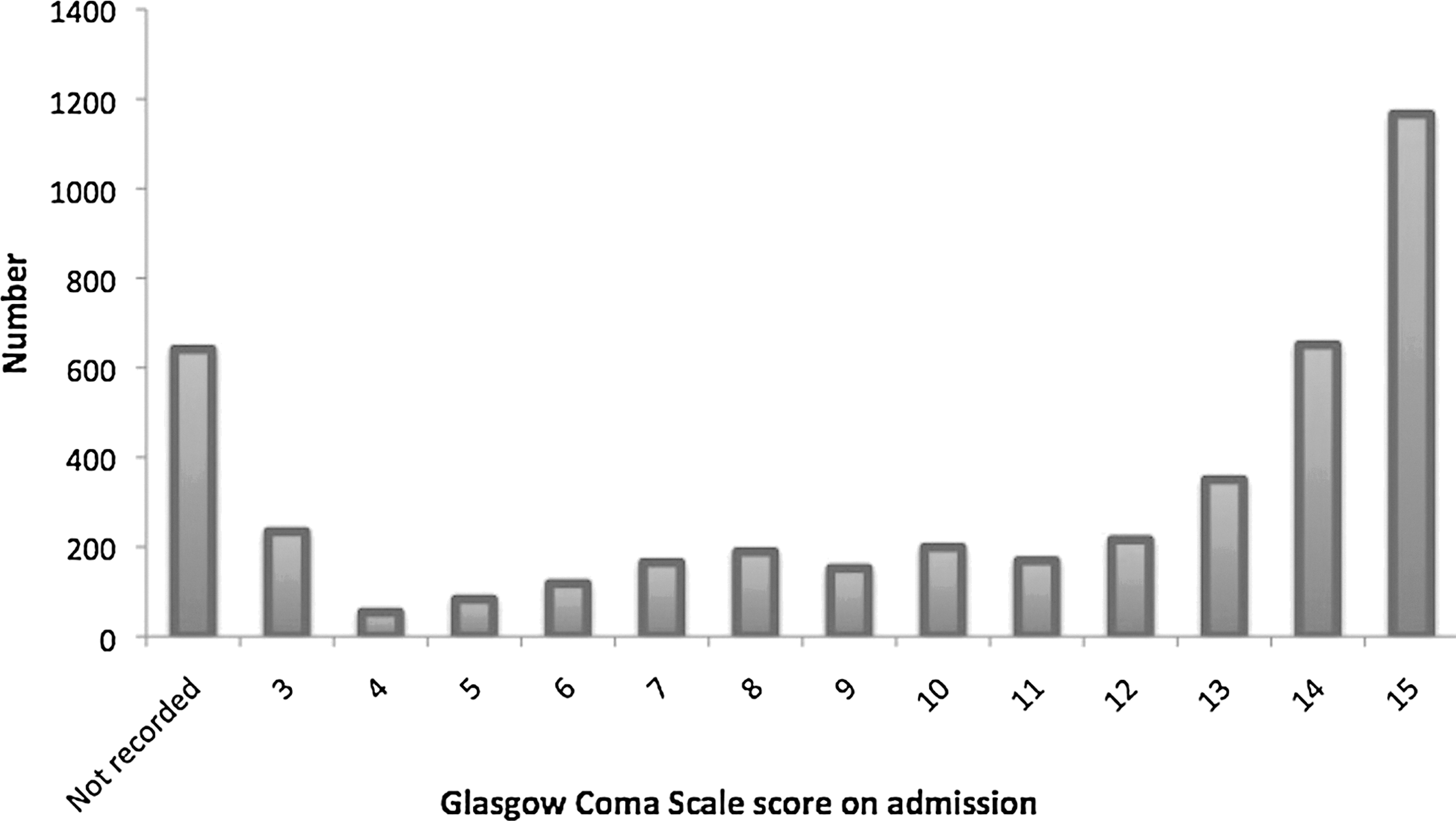
Graph illustrating the presenting Glasgow Coma Scale scores in our cohort.
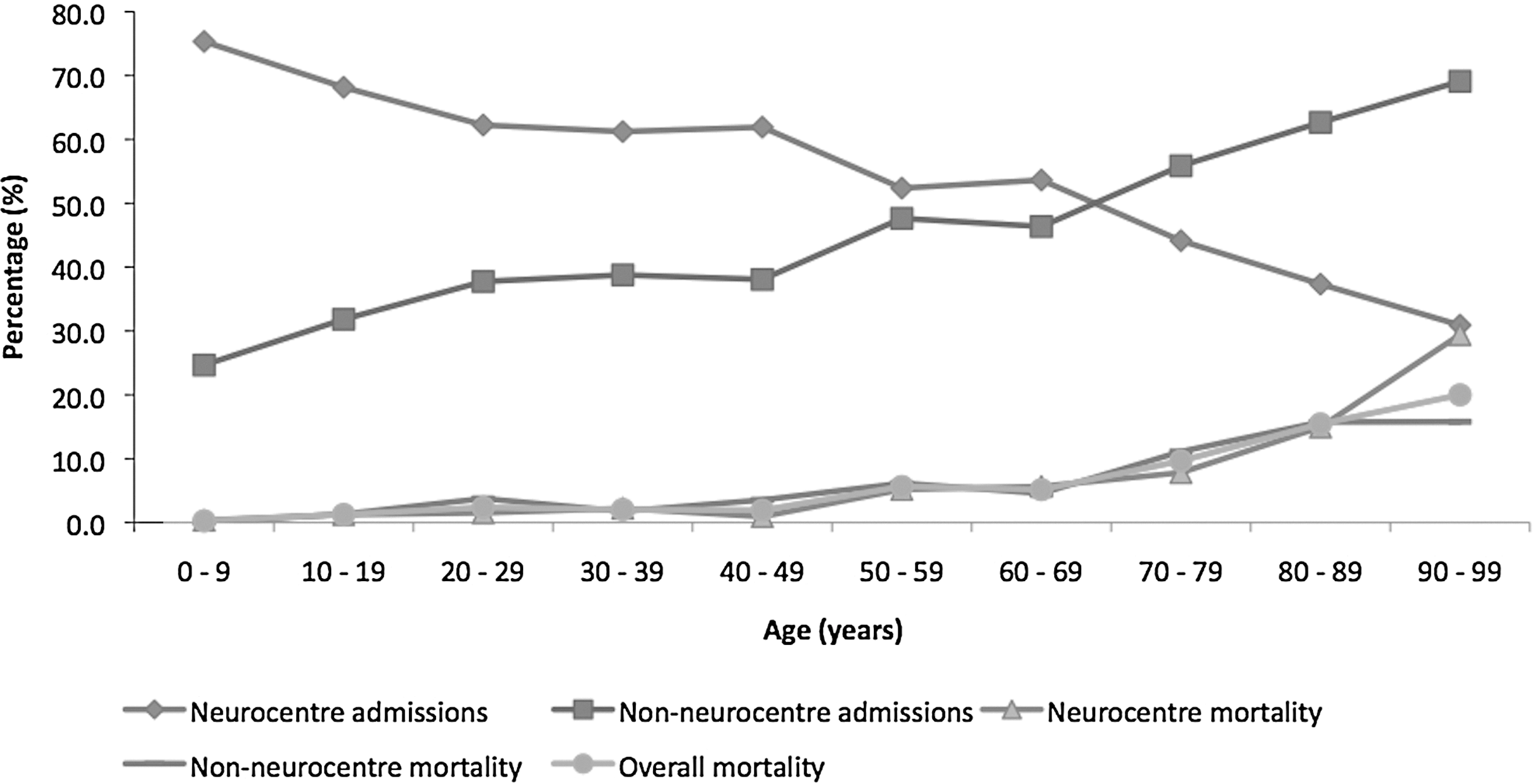
Graph illustrating the number of patients with cerebral contusions admitted to a neurocenter and non-neurocenter, and associated mortality, according to age.
Mortality
Of the 4387 patients, 169 (3.9%) died within thirty days of hospital admission. The mortality rate increased with increasing age, so that the mortality rate in the 0–9 years group was 0.3%, compared with 20.0% in those aged 90–99 (Fig. 2 and Fig. 3; linear trend test in logit scale; p<0.001). Of those admitted to the neurocenter, the average mortality rate was 2.9%, compared with 5.2% in those admitted to a non-neurocenter. When looking specifically at neurocenter and non-neurocenter admissions, there was an overall significant difference in mortality between the two groups (Chi square value=5.59; degrees of freedom=1; p<0.001).
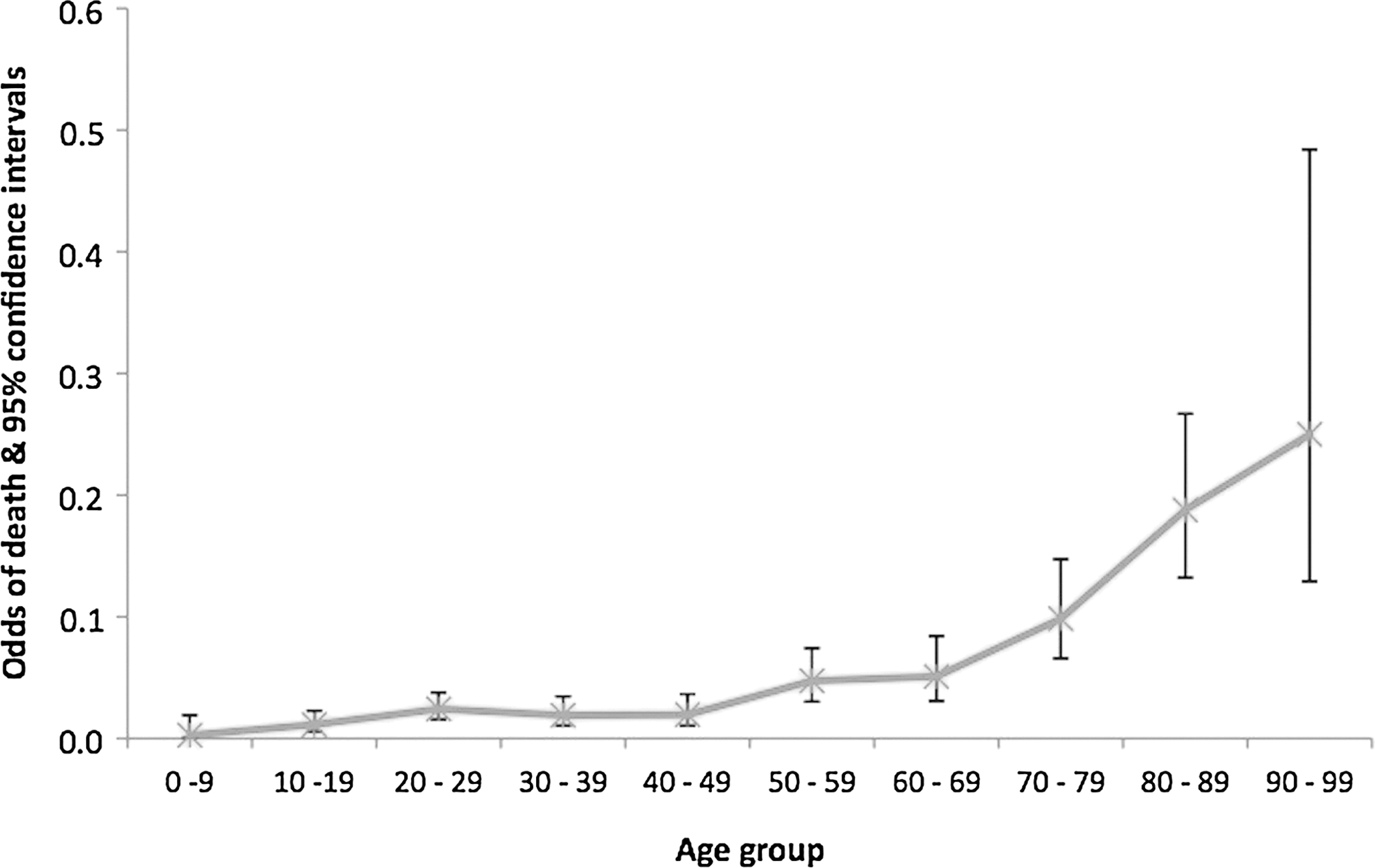
Graph demonstrating the odds of death and 95% confidence intervals, according to age.
CT
All of our subjects underwent CT imaging of the head. Of those patients who were direct admissions to the center where TARN data originated (n=3171), the median time from presentation to CT head imaging was 1.47 hours (Table 3). There was a general trend for increasing median time from presentation to CT head imaging with increasing age, being just over one hour (1.08 hours) in those aged 0–9 years, compared with more than two hours (2.27 hours) in those aged 90–99 years (Fig. 4; Jonckheere's trend test; p=0.003).

Graph illustrating the median time from admission to computed tomography scan of the head in patients with cerebral contusions, according to age.
Seniority of clinician assessing patient
The grade of the most senior clinician who assessed each patient is shown in Table 4. A consultant is a senior physician who has completed specialist training (equivalent to an attending physician). An associate specialist ranks below the consultant grade but is a permanent position with a similar role but reduced responsibilities. The terminology used to denote differing grades of doctors in training in the UK has changed over the past few years. A specialty trainee (or registrar in the old nomenclature) is a doctor training in a specific field (such as emergency medicine) and is equivalent to a resident. A foundation trainee is typically a doctor in his or her first two years of postgraduate medical training (a first-year foundation trainee can be considered the equivalent of an intern in US nomenclature). A house officer is the old term used to denote the initial postgraduate training level that existed before foundation training in the UK.
The main findings include a significant decrease in the proportion of patients assessed by a consultant with increasing age; 91 of 204 (44.6%) patients aged 0–9 years were assessed by a consultant, compared with only eight of 54 (14.8%) aged 90–99 years (Jonckheere's trend test; p<0.001). In addition, the proportion of patients assessed by a foundation trainee/house officer as the most senior doctor increased with increasing age, from 18 of 204 (8.8%) patients aged 0–9 years to 12 of 54 (22.2%) patients aged 90–99 years (Jonckheere's trend test; <0.001).
Discussion
Our data confirm that increasing age is associated with higher mortality following cerebral contusions. This is in keeping with pioneering studies from the late 1970s that demonstrated severe head injury outcomes in the elderly were poor. 5,6,16 Significant advances in patient care, especially in the trauma setting, have probably contributed to the reduction in mortality observed since then, 4 but many studies still report outcomes as poor in the elderly. 7,8,17 –19 In fact, age has been shown to be an independent risk factor for mortality following severe head injury, 5,9 –12 and increased mortality from head injury increases from as early as the age of 30. 20 Unfortunately, many of these studies have not stratified data according to underlying pathology, 21 important since the prognosis following chronic subdural hematoma is significantly better than for severe contusions, for example. Another criticism of these studies is their retrospective nature, making it difficult to ascertain whether the observed outcomes are truly a result of age-related factors, or “therapeutic nihilism in the elderly.” 22
Why should elderly patients have a worse outcome following brain injury? First, older patients have a higher propensity to develop intracranial bleeding, 5, 23,24 especially if on medication such as clopidogrel. 25 Further, experimental studies have shown that the aging brain is more susceptible to the deleterious effects of ischemia, 26 which is a common pathophysiological mechanism underlying several forms of traumatic brain injury. Elderly patients also often have comorbidities such as diabetes, ischemic heart disease, and chronic obstructive pulmonary disease that may negatively impact outcome following trauma, 23,27 although others disagree. 28,29 Pre-morbid use of statins appears to improve mortality and morbidity in individuals 65 years or older without cardiovascular comorbidities suffering head injury, 30 although further studies are required to validate this.
Our data suggest different management practices in the elderly may contribute to the mortality rates observed, with time from admission to CT head imaging and the likelihood of not being transferred to a neurocenter (i.e., somewhere with acute neurosurgical care facilities) increasing with increasing age. In addition, the seniority of doctor assessing a patient was found to decrease with increasing age. Indeed, previous studies have described age bias in the acceptance of head injury patients referred to neurosurgical centers against the elderly, 31,32 and such “ageism” may contribute to poor outcomes in the elderly. 32
Although our study design prevents further analysis as to the decisions that governed transfer to neurocenters, there were overall significant differences in mortality rates observed between those patients admitted to neurocenters and those not. While not every patient with head injury, elderly or otherwise, requires transfer to a neurocenter, we need a better understanding of the issues guiding the decisions made. A 2005 paper based on TARN data from 1989–2003 also found significantly higher mortality rates among those with severe head injury who were treated in a non-neurosurgical center, compared with those who were treated in a neurosurgical center. 33
Some studies have shown elderly patients with head injury fare better than most studies would suggest, 34 and in those with moderate head injury, increasing age may not be a risk factor for unfavorable outcome at all. 35 One may expect the cerebral atrophy observed in aged brains to permit a greater volume of extra-axial blood prior to an increased intracranial pressure. A large prospective study of traumatic brain injury patients found that although older patients required more inpatient rehabilitation and had more functional impairments than their younger counterparts, they continued to recover and improve in the months following discharge. 36 Elderly patients also respond to aggressive resuscitation and intensive care. 23,27 Although the mortality rate for cerebral contusions with an AIS >3 in our study clearly increases with age, even in the 90–99 years age group the mortality rate means that 80% of patients remained alive.
Major strengths of this study include the large numbers of patients included from a national dataset, and the relative homogeneity of the data resulting from our inclusion criteria as described in the methods. The limitations of our study include its retrospective nature and lack of long-term follow-up data.
In conclusion, our data suggest that the increased mortality seen in older patients with cerebral contusions may be related to the fact they have significant delays in CT and transfer times and see more junior doctors. It is possible that the retrospective studies performed to date demonstrating poorer outcomes following head injury in the elderly are influencing current practice, to the extent that delays and suboptimal management contributes to poor outcomes and thus creates a self-fulfilling prophecy. A prospective study with long-term data comparing outcomes in younger and older patients is needed, studying the different forms of brain injury resulting from trauma, and addressing discrepancies in management between younger and older groups. Further understanding of pathophysiological differences between younger and older patients suffering head injury may help further improve patient care for this vulnerable group.
Author Disclosure Statement
No competing financial interests exist.