
Abstract
The aim of this study was to quantify the association between diffusion tensor imaging (DTI) parameters of the cervical spinal cord and neurological disability in patients with chronic traumatic spinal cord injury (SCI). A cervical spinal cord 3T magnetic resonance imaging (MRI) with DTI sequences was performed on 28 patients with chronic traumatic SCI and 40 healthy control subjects. DTI metrics, including fractional anisotropy (FA), apparent diffusion coefficient (ADC), axial diffusivity (AD), and radial diffusivity (RD), were calculated within the normal-appearing spinal cord area at levels C2 or C3. Clinical assessment of the patients was performed according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) and the motor subscale of the Functional Independence Measure (FIM). The FA values of the patients with SCI were significantly lower than those of healthy control subjects (p<0.000001). In contrast, the ADC and RD values of these patients were significantly higher than those of control subjects (ADC p<0.0001, RD p<0.00001). In patients with SCI, the FA values were positively correlated with the motor (pr=0.56, p<0.01) and sensory (pr=0.66, p<0.001) scores of ISNCSCI and with the motor subscale of FIM (pr=0.51, p<0.01). DTI revealed spinal cord pathology, which was undetectable using conventional MRI. DTI changes in regions that were remote from the site of primary injury were most likely the result of secondary degeneration of white matter tracts. Decreased FA values were correlated with poorer motor and sensory function, as well as a lack of independence in daily living. DTI is a promising quantitative and objective tool that may be used in the clinical assessment of patients with SCI.
Introduction
Clinical examination and magnetic resonance imaging (MRI) are routinely used to evaluate the severity of SCI. Neurological examination using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) serves as the most commonly used method for the clinical definition and grading of the level and completeness of an injury. 3 Daily living activities are usually assessed using the Functional Independency Measure (FIM). 4,5 MRI findings such as hemorrhage and edema have been shown to correlate with clinical impairment in acute cervical SCI. In addition, data from both MRI and ISNCSCI have been used to predict long-term outcome after SCI. 6 –9 However, ISNCSCI is prone to some inter-rater variability, and the evaluation of children and patients with cognitive impairment is difficult because of inadequate cooperation. 10,11 Although conventional MRI can reliably depict focal injuries of the spinal cord parenchyma, the data will be mostly qualitative.
Diffusion tensor imaging (DTI) is a relatively new imaging method based on the diffusion of water molecules in tissues. Quantitative DTI parameters provide information on tissue microstructure in the nervous system. 12 The apparent diffusion coefficient (ADC) or mean diffusivity (MD) expresses the magnitude of the diffusion. Of the three directional diffusivity values (λ1, λ2, and λ3), the diffusivity along the principal axis of the diffusion tensor (λ1) is known as the axial diffusivity (AD), and the average of the second and third values (λ2, λ3) is referred to as the radial diffusivity (RD). Fractional anisotropy (FA) describes the degree of directional dependence/anisotropy of the diffusion, and it is represented as values between zero (complete isotropic diffusion) and one (complete anisotropic diffusion). 13,14
DTI has been shown to have potential for the quantification of white matter pathology of the spinal cord. This technique has been successfully applied to multiple sclerosis (MS), spondylotic myelopathy, and SCI. 15 –18 However, the patient populations used in previous studies on DTI parameters of patients with chronic SCI have been relatively small, and most of the DTI methodology was laborious to implement into clinical practice. 18 –21
The aim of this study was to quantitatively assess the state of the cervical spinal cord using DTI in patients with chronic traumatic cervical SCI, and to determine whether there are differences between DTI values with respect to the completeness of the SCI. We also investigated the correlations between DTI values and clinically relevant measures such as ISNCSCI and FIM. The association between conventional MRI findings and clinical parameters was also examined.
Methods
Study design and ethics
This study is part of the Spinal Cord Injury Series of Tampere -Retroprospective Study. The study aims to examine SCI from a multidisciplinary perspective, in a case–control manner, to enhance the clinical assessment and treatment of this specific patient group. Ethics approval for the study was obtained from the Ethical Committee of Pirkanmaa Hospital District, Finland. A written informed consent was obtained from each participant.
Subjects
All consecutive patients with a chronic traumatic cervical spine injury (n=88) who were admitted to either the ward or an outpatient clinic in Tampere University Hospital between 1989 and 2010 were contacted for participation in the study in 2011. The inclusion criteria for the patients were as follows: 1) >18 years of age, 2) resident of the hospital district, 3) clinically significant neurological findings of a traumatic cervical SCI after 24 h of monitoring in the hospital, and 4) time since injury > 1 year. The exclusion criteria were as follows: 1) known neurological illness other than SCI, 2) respiratory arrest, 3) contraindications to MRI, and 4) refusal to participate in the study. In addition, 6 patients with poor MRI image quality (e.g., artifacts from a vertebral fixation material) were excluded; the final SCI population sample consisted of 28 patients.
Patients with SCI were compared with an orthopedically injured control sample of 40 neurologically intact subjects. The control subjects were recruited from consecutive patients with ankle trauma from the Emergency Department of Tampere University Hospital. A total of 609 patients with ankle injury were screened for participation in this study. The aim was to enroll five male and five female subjects into each of following age groups: 1) 18–30, 2) 31–40, 3) 41–50, and 4) 51–60 years. The inclusion criteria were as follows: 1) age 18–60 years, 2) being a resident of the university hospital district, and 3) ankle trauma. The exclusion criteria were as follows: 1) neurological problems, 2) psychiatric problems, 3) history of traumatic brain injury (TBI), 4) former neurosurgical procedure, 5) problems with hearing or vision, 6) first language other than Finnish, 7) contraindications to MR, I and 8) refusal to participate. Of the final sample of 40 healthy subjects, 20 (50%) were male and 20 (50%) were female. The control sample was primarily collected for a mild TBI study, and, therefore, the enrollment criteria differed from the ones used with the SCI patients.
Collection of clinical data and neurological scoring
All patients with SCI were examined at an outpatient clinic in Tampere University Hospital. The collection of clinical data was performed by the first author of this study. The etiology of the SCI was classified using the International SCI Core Data Set. 22 The ISNCSCI was used to evaluate and classify the neurological consequence of SCI. 3 Completeness of the injury was defined according to the American Spinal Injury Association (ASIA) impairment scale (AIS). A single neurological level represents the most caudal level of normal sensory and motor functions. The motor score (range 0–100) consists of five manually tested key muscle forces (range 0–5, where 0=total paralysis and 5=active movement against full resistance) for both the arms and legs. To determine the sensory score (range 0–224), light touch and pinprick sensations (range 0–2, where 0=absent and 2=normal sensation) were examined over dermatomes C2 to S4/S5. However, there are sensory data missing for two of the patients. The level of disability was assessed using the motor subscale of the FIM. 4,5 The motor subscale of the FIM (range 13–91) consists of subscores for self-care, sphincter control, mobility, and locomotion. Within each subscore, two or more specific items were evaluated in a strictly defined manner in terms of independence of function. Each item ranged in value from 1 to 7 (6–7=independent=capable of performing activity without supervision or help, 3–5=modified dependent, and 1–2=completely dependent).
The medical condition of the subjects was assessed according to the International Classification of Diseases and Related Health Problems, 10th revision (ICD−10). 23 The Basic Pain Data Set was used to collect data from patients with neuropathic pain related to the SCI. 24 Information on the current medication at the time of examination was classified into 17 subgroups according to the Finnish Commercial Drug Catalog (Pharmaca Fennica), which was categorized on the basis of the World Health Organization's Anatomical Therapeutic Chemical (ATC) Classification System codes.
MRI
The MRI and DTI examinations were performed using a 3T MRI scanner (Siemens Trio, Siemens Medical Solutions, Erlangen, Germany). A 12 channel head coil and a 4 channel neck coil were used simultaneously. Sagittal T2 turbo spin echo (TSE) (TR 3500 ms, TE 108 ms, FlipAngle 160 degrees, 1 averages, field of view [FOV] 280, matrix 288×384, slice/gap 3.0/0.3 mm, echo train length [ETL] 34) and axial T2*-weighted multigradient echo combination series (TR 506 ms, TE 14 ms, FlipAngle 30 degrees, 1 average, FOV 160 mm, matrix 256×256, slice/gap 3.0/0.3 mm) were acquired. The voxel size of the T2* images was 0.6×0.6×3.0 mm. DTI data were acquired using axial multidirectional diffusion weighted echo planar imaging sequences (MDDW) (TR 4000 ms, TE 103 ms, 4 averages, FOV 152 mm, matrix 128×128, slice/gap 4.0/1.2 mm, b-factor 0 and 1000, 20 diffusion directions). The voxel size was 1.2×1.2×4.0 mm. Cardiac gating was not used. The scan time for the DTI sequence was 5 min and 50 sec.
Image analysis
An evaluation of the conventional MRI scans was performed by a neuroradiologist (A.B.). The most cranial level of the lesion was assessed, and the craniocaudal length of the main lesion was measured in millimeters.
The region of interest (ROI) measurements were performed by a physicist (U.H.) using the commercially available software Neuro3D (Siemens Healthcare, Malvern, USA). The ROIs were manually placed on axial images of the color-coded FA maps and automatically transferred onto the non-diffusion-weighted b0 images and ADC maps. Spinal cord levels were determined using the sagittal T2 anatomical images. Whole spinal cord ROIs were drawn using a freehand technique; however, for individual funicles, small circle ROIs were used. The ROIs were centered in the area of interest, taking care to avoid the border areas and cerebrospinal fluid (CSF) spaces (Fig. 1).
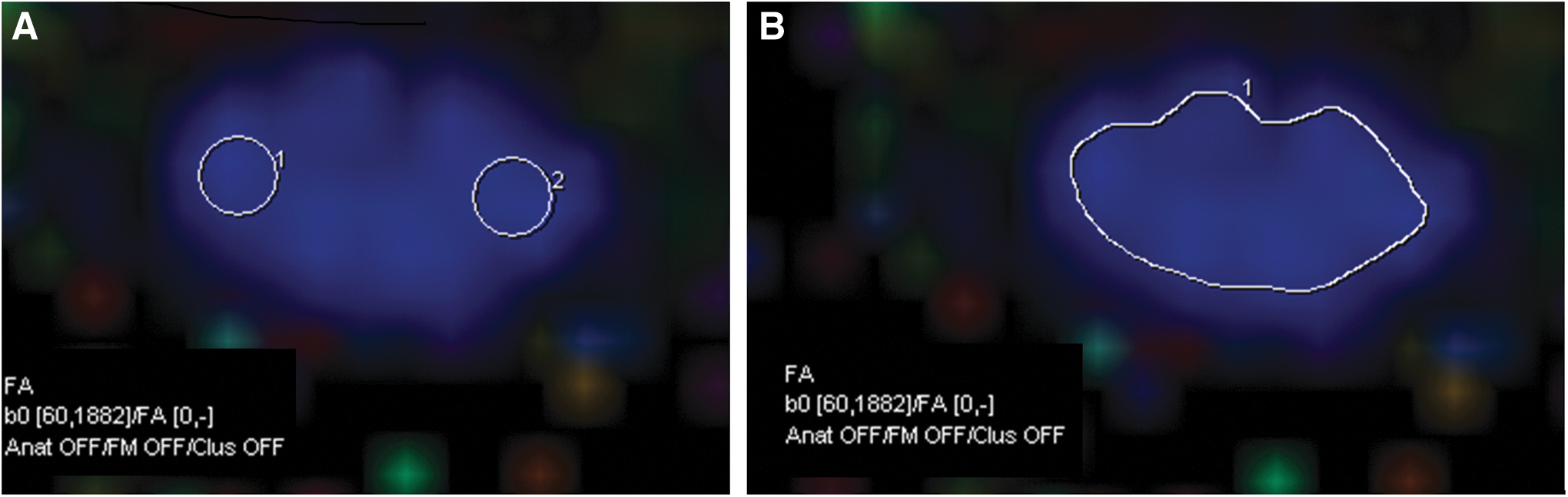
The placement of the regions of interest (ROIs) on the fractional anisotropy (FA) maps.
The mean values, standard deviations and median values of the FA and ADC were assessed for the whole cord and for the lateral funicles at cervical level C2–3 above the primary lesion and at the level of the spinal cord lesion (Figs. 2 –4). At the C2–3 level, the AD and RD were also calculated for the whole cord area. The DTI values from the left and right funiculus were averaged per level measured. At the levels of the spinal cord lesions, the gray and white matter contrast was mostly lost, which made a reliable placement of the ROI difficult. Consequently, measurements indicating “the lesion level” were made at the level just above the most cranial border of the lesion. Because of the artifacts from the vertebral fixation material, 10 of the images from the lesion level were excluded, and DTI measurements could be reliably made for 18 of the 28 patients.

Sagittal T2 images with horizontal white lines showing the measurement levels in a control subject

Axial T2* images of a control subject

Axial fractional anisotropy (FA) color maps corresponding to the same levels as in Figure 3: control subject
In the control subjects, the DTI values were measured at the C2–3, C3–4, C4–5 and C5–6 levels (Fig. 2). All of the cranial levels of the spinal cord lesions, which were observed in the conventional MRI, were situated between segments C2 and C6. Therefore, the mean DTI values among the healthy controls from the C2–3 to C5–6 levels were used as reference values for the lesion level measurements in SCI patients.
Statistical analyses
Patients with SCI were not age-matched with the control subjects; therefore, the analyses were performed using linear regression, which was adjusted for age. Correlations with the DTI values and conventional MRI findings were calculated using a partial correlation with age as a control factor. Clinical variables used in the correlations included the ISNCSCI-derived total motor score, motor subscore for the upper and lower extremities, total sensory score, single neurological level, and FIM subscores of the motor subscale. Further comparisons of the patient population were divided into two groups on the basis of the completeness of the injury; AIS A and AIS B-E. Statistical analyses were performed under the guidance of a biostatistician (M.H.). Because of multiple comparisons, the statistical significance level was established at 1%. All of the parameters were ranked prior to the analyses. The SPSS program (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) was used to perform all of the statistical analyses.
Results
Clinical findings
Clinical characteristics of the SCI patients (entire group, AIS A and AIS B-E) and control subjects are shown in Table 1. Of the patients with SCI, 17 (60.7%) patients had some chronic medical problems. The most common chronic medical problems were diseases of the circulatory system (n=9, 32.1%) and diseases of the musculoskeletal system and connective tissue (n=7, 25.0%). Twenty-four (85.7%) patients used some permanent medication; 12 (42.9%) patients used some pain medication; 11 (39.3%) patients used a prophylactic antibiotic; 9 (32.1%) patients used drugs for the cardiovascular system; and 9 (32.1%) patients used muscle relaxants. Eleven (39.3%) patients with SCI had neuropathic pain.
Missing sensory data for two patients.
ASIA, American Spinal Injury Association; AIS A, motor-sensory complete; AIS B, motor complete-sensory incomplete; AIS C-D, motor-sensory incomplete; AIS E, normal examination; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; FIM, Functional Independence Measure.
Eighteen (45.0%) of the control subjects had a diagnosed disease. Six of the patients had a disease of the circulatory system (15.0%), and four (10.0%) patients had a disease of the musculoskeletal system and connective tissue. Thirteen (32.5%) control subjects used some permanent medication. The largest group used drugs for the cardiovascular system (n=6, 15.0%). There were no control subjects who showed neuropathic pain.
Conventional MRI findings
A cervical cord operation was performed on 19 out of the 28 (67.9%) patients. A vertebral fixation material was found on 13 (46.4%) of the patients. The spinal canal was classified as narrow in 10 (35.7%) of the patients. A focal post-traumatic lesion on either the sagittal or axial T2 / T2*-weighted sequences was found in 23 (82.1%) of the patients, of which 3 patients had two separate lesions. Five (17.9%) patients demonstrated no visible spinal cord lesions. The most cranial levels of the main lesions were situated between the C2 and C6 levels. The mean length of the main lesion was 18.1 mm (SD 14.5). Spinal cord atrophy was found in 18 (64.3%) patients. On axial T2* images, six of the patients showed diffuse high signal intensity in the dorsal funicle at levels above the primary lesion (Fig. 3). In five of them, the clinical cord injury was complete (AIS A), and in one it was incomplete (AIS B). This finding probably represents secondary anterograde (Wallerian) degeneration of the ascending tracts, and was not apparent on sagittal T2 images.
None of the control subjects showed significant structural abnormalities on the conventional MRI sequences.
DTI parameters
All of the measured FA, ADC, AD, and RD values are summarized in Tables 2 and 3. The control subjects were compared with the entire group of patients with SCI, both the AIS A subgroup and the AIS B-E subgroup. Furthermore, a comparison between the AIS A and AIS B-E groups was performed. Patients with SCI demonstrated lower FA values and higher ADC values than did healthy control subjects at both the upper cervical cord and the lesion levels. In addition, the RD values were increased in patients at the upper cervical cord level.
Comparisons adjusted with age by linear regression.
p<0.01 in bold
DTI, diffusion tensor imaging; SCI, spinal cord injury; FA, fractional anisotropy; ADC, apparent diffusion coefficient; AD, axial diffusivity; RD, radial diffusivity; AIS, American Spinal Injury Association impairment scale; AIS A, motor-sensory complete; AIS B, motor complete; AIS C-D, motor-sensory incomplete; AIS E, normal.
Controls=mean of diffusion tensor parameters for healthy volunteers at C2-C3 to C5-C6 levels.
Comparisons adjusted with age by linear regression.
p<0.01 in bold.
DTI, diffusion tensor imaging; SCI, spinal cord injury; FA, fractional anisotropy; ADC, apparent diffusion coefficient; AIS, American Spinal Injury Association impairment scale; AIS A, motor-sensory complete; AIS B, motor complete; AIS C-D, motor-sensory incomplete; AIS E, normal.
Partial correlations (with age as a controlled factor) between the spinal DTI values, conventional MRI findings, and clinical findings (ISNCSCI and FIM) are shown in Table 4. Significant correlations between the DTI values and ISNCSCI and FIM scores were mostly found in the FA. The length of the spinal cord lesion correlated with the ISNCSCI scores from the MRI findings.
Two sensory scores missing (n=26/16/21 respectively).
p≤0.05, * p≤0.01in bold; ** p≤0.001 in bold and underlined.
DTI, diffusion tensor imaging; FA, fractional anisotropy; ADC, apparent diffusion coefficient; AD, axial diffusivity; RD, radial diffusivity; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; Mtot, total motor score; Mue, motor score for the upper extremities; Mle, motor score for the lower extremities; Stot, total sensory score; NL, single neurological level; FIM, Functional Independence Measure; Ftot, FIM motor subscale; Fcare, FIM self care subscore; Fspc, FIM sphincter control subscore; Fmob, FIM mobility subscore; Floc, FIM locomotion subscore.
Discussion
In our series, significant alterations in spinal DTI values appeared in both patients with complete and those with incomplete SCI compared with healthy subjects. Some of the DTI values showed a moderate to strong correlation with the clinical parameters, which assessed neurological deficits and disability after SCI. DTI revealed pathological changes in the spinal cords of patients with chronic SCI, as well as in areas where conventional MRI was normal.
In agreement with previous studies on DTI and chronic SCI, we found that the FA values of the patients with SCI were lower than those of healthy controls at both the lesion and upper cervical cord level, which was intact on conventional MRI. 18,19,21,25 In our study, the decrease in FA values was significant in both patients with complete and those with incomplete SCI compared with healthy controls. There was also a difference, although not statistically significant, in the FA values regarding the completeness of the SCI. In contrast to most previous studies, 18,19,21 we found a significant increase in ADC values in patients with SCI at both the lesion and upper cervical cord levels. Ellingson and colleagues also showed higher MD values at the lesion level in patients with SCI. However, in the area of the intact spinal cord, the MD values were reduced in patients compared with healthy individuals. 25
Although no sign of primary lesion on the conventional MRI at the C2–3 level was found in our patient population, a clinically defined single neurological level was located between C1 and C2 in five of the SCI subjects. Therefore, changes in the DTI values at the upper cervical cord level in these patients were most likely a direct result of the primary SCI. Nevertheless, the majority of the SCI patients demonstrated a single neurological level of C4 or lower. One possibility may be that the white matter tracts above the primary lesion level were also affected by secondary anterograde (Wallerian) and some retrograde degeneration. 26 In our sample, six of the most severely injured patients had diffuse high signal intensity in the dorsal funicle on T2* images, probably representing secondary degeneration. In regions of isolated fiber bundles, such as the white matter tracts in the spinal cord, white matter degeneration in the chronic phase causes an increase in the MD and RD whereas FA and AD decrease. 27 In our study, the RD was higher in the patient groups than in the controls, but the AD values were consistent. Because the AD and RD were calculated from the ROIs that covered the entire cord area, the variability in the measurements was most likely diluted by the gray matter. A study conducted by Cohen-Adad and colleagues summarized the diffusion parameters between the areas of the white matter funicles at the vertebral levels remote from the lesion and demonstrated alterations in both the AD and RD values. 21
In chronic SCI, the relationship between DTI values and some of the clinical ISNCSCI scores has been previously described. Chang and colleagues have reported that the number of abnormal FA levels in the cervical cord showed a statistically significant correlation with abnormal motor levels, but not with sensory levels. 19 Cohen-Adad and colleagues also detected a correlation between DTI parameters (FA and RD) and a combined variable consisting of the sensory and motor scores of the ISNCSCI. 21 Furthermore, in a study by Petersen and colleagues, the decrease of FA correlated with the completeness of SCI on the basis of the AIS scale. 18 In a study of pediatric SCI, the clinical findings showed a statistically stronger correlation with the DTI values compared with the upper border of the SCI on conventional MRI. 28
In our study, the FA values demonstrated a moderate to strong correlation with the motor and sensory scores of the ISNCSCI, but not with a single neurological level. There was also a moderate association between the sensory score and RD at the upper cervical cord level. These findings were consistent with earlier studies, which showed that an increase in FA and a decrease in RD were associated with a better clinical outcome. Correlations between the DTI values and FIM appeared mostly in the FA, which decreased with increasing disability. In particular, the FA was moderately associated with all of the FIM motor subscores at the upper cervical cord level. At the lesion level, a strong correlation between the FA values and motor scores of the lower extremities was found. Moreover, correlations between the FA values and FIM scores were focused on the mobility and locomotion subscores.
The upper level of the lesion determined using conventional MRI did not correlate with any of the ISNCSCI parameters, particularly the clinically determined single neurological level. The length of the lesion moderately or strongly correlated with the motor and sensory scores, indicating that the clinical state of patients was worse with a longer lesion length. The association between the length of the lesion on conventional MRI and the degree of impairment has also been previously shown in acute and subacute SCI. 8,29 In our study, the conventional MRI findings and subscales of FIM were only modestly associated with each another. However, similar findings have been reported in a study of subacute SCI, which indicated that function was better when the location of the injury was lower on the spine and when the length of the injury was shorter. 30
To the best of our knowledge, no previous studies in adults have investigated the DTI values of patients with chronic SCI using the entirety of the ISNCSCI parameters or with any instrument used to assess disability. Although the FA, ADC, and RD values in our study differed significantly between the patients and controls, the FA appeared to be the most sensitive parameter in describing the state of the spinal cord in the chronic phase of SCI. As a strength, our study population was larger than those in previous studies, and included SCI patients with variable neurological deficits and disability. The age range of the patients was broad (23–78 years), and included many elderly people.
In the present study, the placement of the ROIs was simple to put into practice. The results presented in this article also indicated that the measurements of the DTI values at the area of the intact upper spinal cord could provide clinically relevant information regarding the state of the chronic injury located below the level measured. This information could be useful in reducing the number of MRI artifacts and producing reliable DTI measures, because the measurement could be performed in regions where the vertebral fixation material and bone/soft tissue injuries did not distort the imaging data.
One weakness of our study was that the patients and control subjects were not age matched. In previous studies, the FA and ADC have been shown to decrease and increase with aging. 31 Moreover, there have also been studies that have reported no correlation between the DTI values and age. 32,33 However, the potential effect of age on DTI values was relatively small compared with the effect of the SCI. Age was also considered using statistical methods.
Overall, compared with the brain, the spinal cord is a substantially more challenging target for DTI analysis. The small size of the spinal cord, which is surrounded by vertebral bony element, as well as its physiological macroscopic motion, all present technical challenges to MRI image acquisition. 34 We chose not to use the cardiac gating technique, which would have diminished the corticospinal fluid flow-related artifacts and lengthened the acquisition time, thus increasing the number of artifacts caused by a swallowing and respiratory movement. The measurements were not strictly performed at the level of the center of the vertebral body, which could have also reduced some artifacts. 35
In the future, DTI may provide a truly quantitative and objective method for assessing spinal cord and tissue microstructure in studies of novel treatments and in clinical settings. The pattern and direction of changes in DTI values, which were measured during the acute or subacute period of SCI, differed from those in chronic SCI. In addition, associations between the clinical scores and DTI values were inconsistent. 36,37 In animal studies, it has been suggested that the DTI values at the acute phase can predict recovery after SCI. 38,39 In the long-term, prospective human studies are required to examine the changes in DTI values and clinical state with respect to time after traumatic SCI, and to determine whether the DTI values in the acute phase have a predictive value for functional outcome.
Footnotes
Acknowledgments
The authors thank our research assistant Anne Simi and our rehabilitation counselors, Raija Pettersson and Eija Väärälä, for their contribution in patient recruitment. We are grateful to the Tampere University Hospital staff of the Department of Neuroscience and Rehabilitation and the Department of Radiology for their support. This work was supported by funds from the Pirkanmaa Regional Fund of the Finnish Cultural Foundation.
Author Disclosure Statement
No competing financial interests exist.