
Abstract
Delirium is a commonly reported acute care adverse event in patients with traumatic spinal cord injury (TSCI), but studies specifically investigating it in this population are lacking. The purpose of this study was to characterize the onset, risk factors, and impact of delirium in patients with TSCI. Patients discharged between 2008 and 2010 were identified from a prospective registry in an acute SCI center. Controls were matched to delirium cases based on date of discharge from acute care. Patient characteristics, risk factors, and the hospital unit (intensive care, spine step-down, spine ward) in which delirium occurred were collected retrospectively. Length of stay (LOS) was calculated and compared between cases and controls. A predictive model was built for patient characteristics and risk factors associated with delirium using logistical regression. There were 192 patients identified from the study group; 34 (17.7%) were delirium cases and 34 were selected as controls. Most delirious episodes were reported during high acuity care (76.5%). The median time interval between injury and delirium identification was 8.5 days (interquartile range=5–31). Age at injury (p<0.01) and initial motor score (p<0.05) were significantly associated with delirium. Patients with delirium had significantly greater LOS than controls (median LOS=46.9 vs. 15.3 days respectively, p<0.0001). Elderly patients who sustain a TSCI and have a low motor score on admission are at increased risk of delirium. These results could contribute to the development of a screening program to address the problem of delirium in the TSCI population.
Introduction
D
Delirium has been well documented in populations at perceived risk, particularly among nursing home residents, 3 cardiac surgical patients, 4,5 and the hospitalized elderly. 6,7 Although it is one of the most common acute care adverse events among patients with traumatic spinal cord injury (TSCI), 8 literature on the condition is lacking within this population. Patients with TSCI are uniquely susceptible to delirium because of the nature and severity of their injury and their demographic. They are often confined to an acute care hospital bed with immediate and often profoundly reduced levels of independence and mobility. Inouye and associates 6,9 have identified these predisposing factors for delirium in the geriatric medical population, because they define a patient's baseline level of susceptibility. Because of the complexity of TSCI and the number of body systems affected, injured persons must undergo numerous medical procedures that can increase their risk of experiencing delirium. According to the model, 10 these risk factors, or precipitating factors, augment a patient's likelihood of delirium developing from their baseline risk on admission.
Delirium is a highly relevant and growing concern for patients with TSCI, because the proportion of elderly persons being injured, especially by falls, has dramatically increased both because of population-based demographic shifts 11 and varying injury patterns. 12 DeVivo and Chen 13 reported that the proportion of persons more than 60 years old sustaining a TSCI rose from 4.6% in 1970 to 13.2% by 2008. This trend is likely to continue with advances in medical technologies allowing persons to live longer and fully participate in society regardless of their age. Because the elderly are more vulnerable to becoming delirious, the changing demographic of TSCI presents a crucial need for delirium awareness and screening within the acute care setting.
A greater understanding of delirium in the TSCI population would facilitate health-specific screening programs and treatment algorithms that would decrease its impact on patients' rehabilitation and the health care system. This study builds on our previous work on the incidence of adverse events such as delirium in the TSCI population. 8,14 The purpose was to describe the onset of delirium in patients with TSCI during acute hospitalization, identify predisposing patient characteristics and risk factors specific to TSCI severity and clinical management, and determine the impact on acute hospital length of stay (LOS).
Methods
Study design
Registry cohort
This study consisted of adults with acute TSCI who were discharged from the Acute Spinal Unit of a quaternary referral center between February 2008 and May 2010. Participants in the Rick Hansen Spinal Cord Injury Registry (RHSCIR) with adverse events data collected using the Spine Adverse Events Severity (SAVES) system 8 were included in the registry cohort. The RHSCIR is a prospective observational database that gathers acute admission and subsequent follow-up data on patients who provide informed consent. For patients who do not consent, a minimal dataset is collected comprising injury and hospital care information. 15 An important feature of the RHSCIR is that it is frequently updated to ensure the accuracy and comprehensiveness of the data it contains.
Delirium cases and controls
A nested case-control study design was used, whereby patients in the registry cohort who were identified as having delirium using the SAVES system formed the cases. SAVES is an instrument validated for TSCI to prospectively detect the occurrence of adverse events during acute care. Details of the SAVES have been described previously. 16 Each delirium case was matched to a patient in the registry cohort who did not experience delirium. Controls were randomly selected based on discharge date from the Acute Spine Unit to ensure that case-control pairs received comparable treatment during their hospital stay. This method allows for analysis of association between patient characteristics and risk factor variables with delirium; if case-control pairs were matched on these variables, it would not be possible to determine their association with delirium occurrence.
Data collection
Data from the hospital units where delirious episodes occurred were collected from electronic and paper records of patient charts. Details on patient characteristics, potential risk factors, and admission/discharge information of both delirium cases and controls were obtained from the RHSCIR and supplemented by patient chart abstraction. The following patient characteristics were investigated on admission: age at injury, sex, American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade, 17 initial motor score, 18 neurological level of injury, comorbidities, drug use, blood alcohol level (≥ or <2 mmol/L), education level (> or ≤high school completion), cognitive impairment, history of alcohol abuse, visual or auditory deficits, and medication use (≥or<five types used). These characteristics were selected based on clinical relevance and key literature on delirium among surgical patients and the elderly. 1,6
Potential risk factors studied were: intra-operative adverse events, infections, having spine surgery, intensive care unit (ICU) stay, time from injury to acute admission, time from injury to first surgery, dehydration, malnutrition, new disease process (such as neurogenic bowel), bladder catheterization, respiratory insufficiency, and medication regimen (> or ≤three types prescribed). Risk factors were considered as present for the delirium cases when they were documented at least 24 h before the delirious episode. Risk factors were adapted from the protocol described by Mentes 19 to assess causes of delirium.
This study was approved by the Clinical Research Ethics Board at the University of British Columbia and the Vancouver Coastal Health Research Institute.
Data analysis
Onset of delirium
Incidence of delirium was determined by tabulating the number of patients who had delirium as a percentage of the total number of patients in the registry cohort. The number of days from injury and admission to delirium onset, and the hospital unit in which the delirious episode first occurred were noted for each delirium case (i.e., ICU, step-down unit, and spine ward). The frequency of delirium in high acuity (ICU and step-down) and non-high acuity (spine ward) units was calculated based on the total number of cases. The ICU admits ventilated and acutely ill patients, while the step-down unit has hemodynamic monitoring capability without ventilator management. The spine ward as well as the step-down unit admit patients with a tracheostomy necessitating ventilator support.
Patient characteristics and risk factors
Bivariate analyses were performed to determine whether each patient characteristic and risk factor was associated with having delirium. For continuous variables (age at injury, initial motor score, time from injury to admission, and time from injury to surgery), the Mann-Whitney U test was used to assess whether there was a significant difference between delirium cases and controls. All other variables were binary and either the Chi-square or Fisher's exact tests were used to assess for significant differences between the two groups. The outcome variable delirium was dichotomized into “no delirium” or “had delirium.” Significant association was considered to be a p value <0.05, and associations having a p value<0.2 were considered to have a trend toward significance.
The patient characteristic and risk factor variables that were significantly associated with delirium or had a trend toward significance were included in a logistic regression model to characterize their relationships while adjusting for the effects of the other patient and risk factor variables.
LOS
The distribution of LOS for the delirium cases was compared with the distribution for the controls. The Mann-Whitney U test was used to determine whether there was a significant difference in LOS between the two groups.
Analyses for this study were performed using SAS® 9.2 Software.
Results
Patient population and onset of delirium
There were 192 patients with TSCI discharged from the Acute Spine Unit during the period included in the registry cohort. Thirty-four (17.7%) of these patients experienced delirium during acute care hospitalization. The median time elapsed from their injury to the first recognition of delirium was 8.5 days (interquartile range=5–31). Figure 1 illustrates the cumulative number of days from acute admission until delirium onset for all cases. Almost 70% of delirium cases were identified within 10 days of the hospital stay. Delirium occurred most frequently in high acuity care, especially in the spine step-down unit, compared with non-acuity care (76.5% vs. 23.5%, respectively). Of the seven patients who received surgery and experienced delirium in the spine ward, two were first admitted to a combination of the ICU and spine step-down unit, three went first to the ICU, and two were admitted directly to the spine ward.
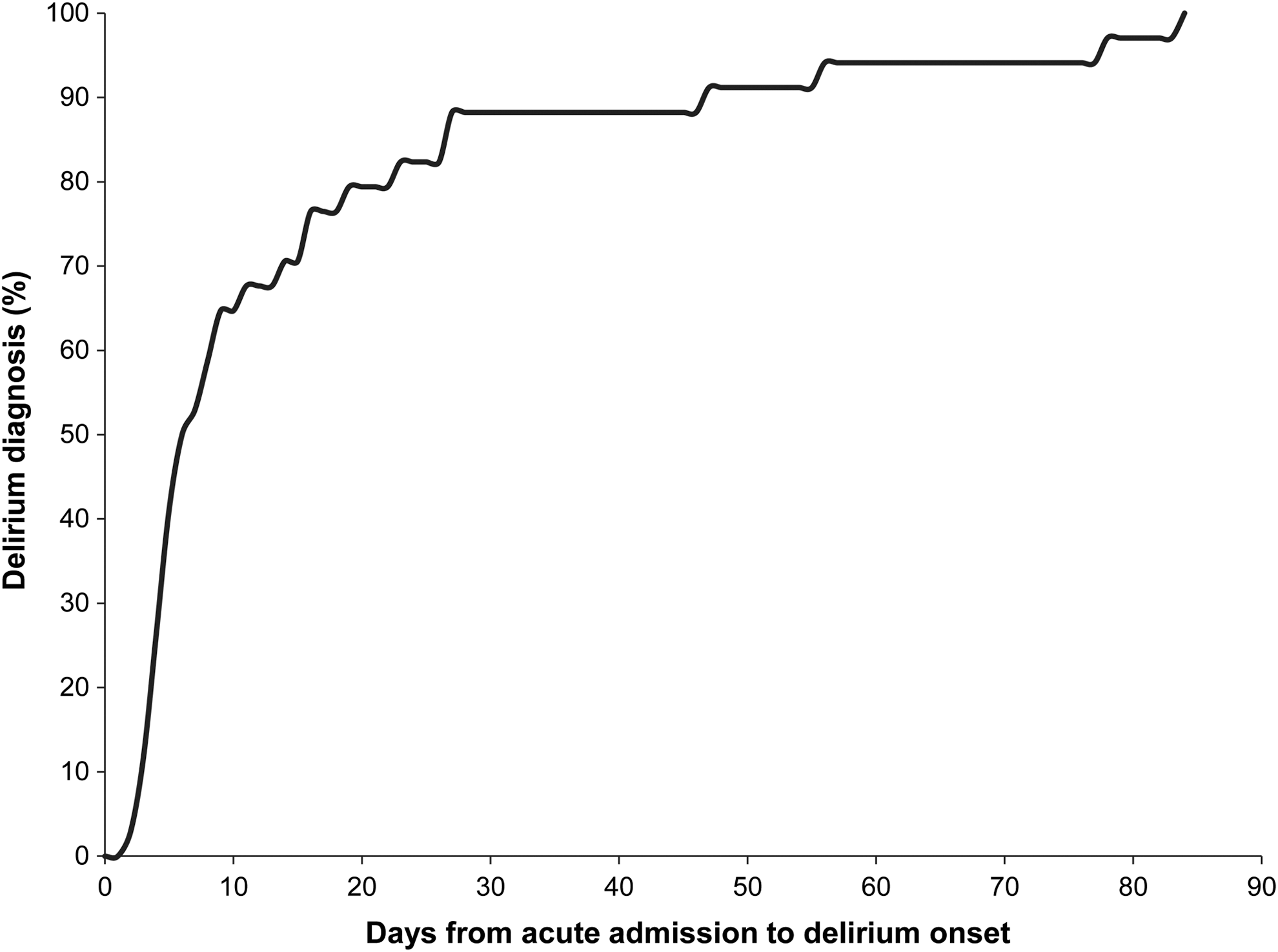
Cumulative number of days until delirium diagnosis.
Patient characteristics
Patients who experienced delirium exhibited on-admission characteristics that were different from those who did not experience delirium (Table 1). Delirium cases were significantly older (median age at injury=62 years vs. 45 years, p<0.001) and had a lower initial motor score (median score=36 vs. 55, p<0.01) than their non-delirious controls. There were significantly more patients who had at least one comorbidity in the delirium group (76.5% vs. 41.2%, p<0.01), and more patients who had a visual or auditory deficit on admission (29.4% vs. 5.9%, p<0.05). No significant differences were observed for the other patient characteristics; however, there was a trend toward a significant difference between the distribution of AIS grades in delirium cases compared with controls, as well as a trend toward significantly more cases than controls who needed five or more types of medications (p<0.2). The patient characteristics of delirium controls were compared with the other participants enrolled in RHSCIR who did not have delirium to ensure that the selected controls were representative of patients who did not experience delirium and there were no significant differences (data not shown).
p<0.2; * p<0.05; ** p<0.01; *** p<0.001.
IQR, interquartile range; AIS, American Spinal Injury Association Impairment Scale; NS, not significant.
Risk factors
Patients with delirium experienced longer intervals between their time of injury and admission to acute care and also to first surgery, but these differences were not statistically significant (Table 2). The number of intra-operative adverse events, spine surgeries, ICU stays, dehydration periods, new disease events, bladder catheterization, and respiratory insufficiency occurrences were greater among delirium cases compared with the control group, but only ICU stays and bladder catheterization had a trend toward a significant association with delirium (p<0.2). There were significantly more patients in the control group with more than three medications in their daily regimen compared with the delirium cases (97.1% vs. 76.5%, p<0.05). These associations are shown in Table 2.
p<0.2; * p<0.05.
IQR, interquartile range; NS, not significant; ICU, intensive care unit.
Logistic regression
The patient characteristics of age at injury, initial motor score, comorbidities, visual or auditory deficits, and medications used, and the risk factors of ICU stay, bladder catheterization, and medication regimen were selected for the logistic regression analysis. Table 3 shows that only older age at injury (p<0.01) and lower initial motor score (p<0.05) were significantly associated with having delirium. Specifically, with every year increase in age, a patient's odds of having delirium would increase by 4.8%, while with every 10 unit decrease in motor score, the odds of having delirium would increase by 25%.
p<0.05; ** p<0.01.
SE, standard error; OR, odds ratio; CI, confidence interval; ICU, intensive care unit.
Length of stay
Patients in whom delirium developed had a significantly longer acute LOS than those who did not have delirium (p<0.0001). The median LOS for delirium cases was 46.9 days compared with 15.3 for the control group. This difference is illustrated in Figure 2.
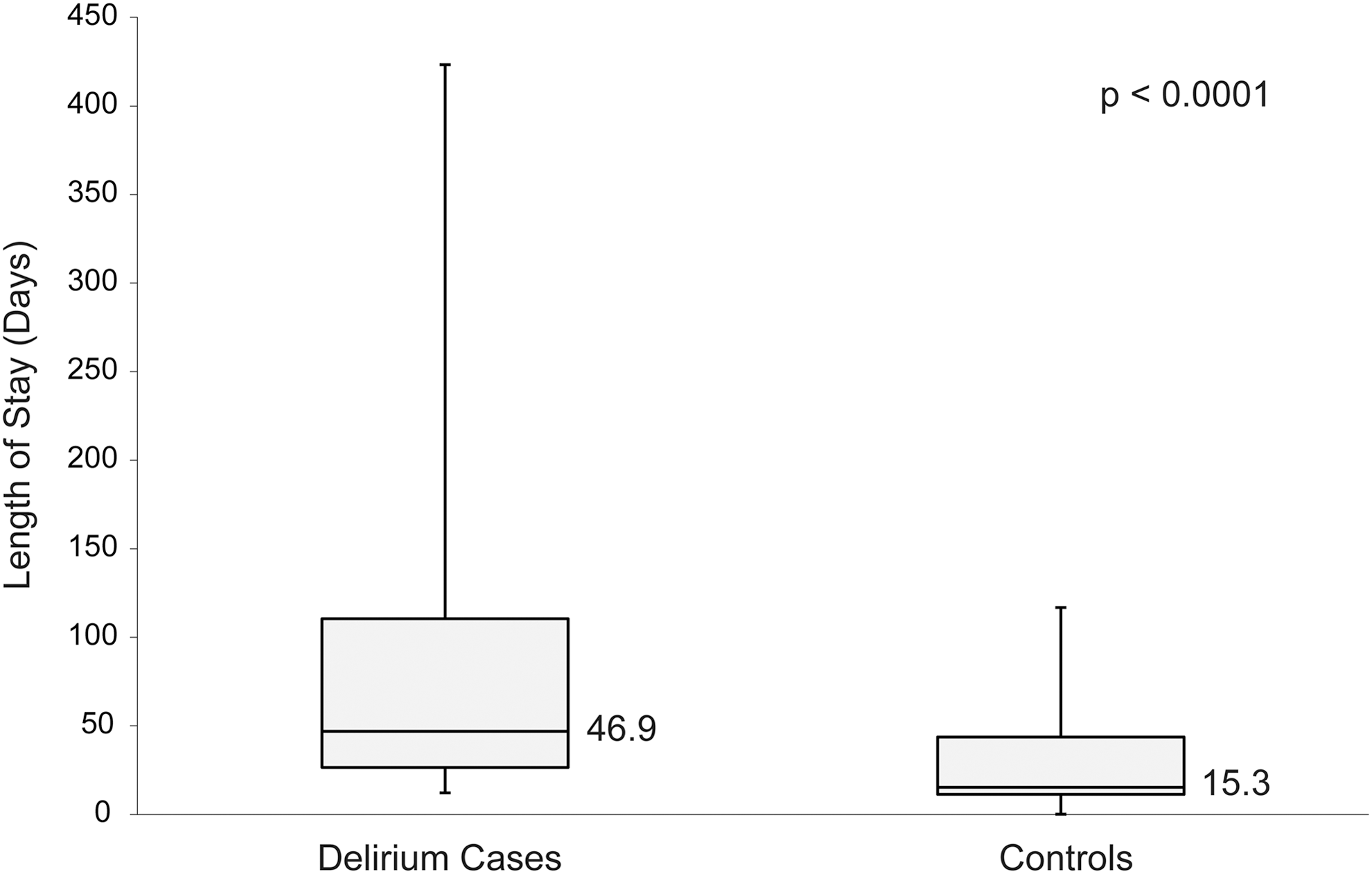
Comparison of length of stay between delirium cases and controls showing the interquartile range and median for each group.
Discussion
This nested case-control study assessed the onset of delirium, patient characteristics, risk factors, and impacts of delirium in a TSCI population. To our knowledge, it is the first to focus specifically on delirium in TSCI and adds to previous work on adverse events in elderly, trauma, and spine surgery patients. The results reveal a high incidence; nearly one-fifth of patients with TSCI experienced delirium during acute hospitalization, and it occurred most commonly in high acuity care. Compared with patients who did not have delirium, affected personss were more likely to be older and have a lower initial motor score. In addition, the acute LOS was significantly higher on average for delirious patients than non-delirious patients. These results emphasize the impact of delirium on the acute care of patients with TSCI.
The identification of risk factors for developing delirium and the timing of diagnosis support the creation of a screening and intervention program. We have shown that a screening program could potentially be implemented in high acuity care, which in our case consists of the ICU and spine step-down unit, to identify older patients who have low motor scores on hospital admission. These targeted patients could then be treated with a multi-factorial intervention regimen similar to the one described by Björkelund and associates 20 for elderly patients with hip fracture, that significantly decreased delirium with increased observation of physiological parameters and maintenance of risk factors.
The incidence described in this study was higher than studies involving elective spine surgery 21,22 or spine trauma with and without SCI 16 ; however, it is difficult to compare incidence across studies that differ in patient population and reporting methods. We followed a rigorous process for the identification of delirium cases that used the prospective SAVES method, consultation with a psychiatrist, who referred to criteria set out by the American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) 23 and the Confusion Assessment Method (CAM) 24 or CAM-ICU model. 25
We report an incidence of 17.7% in our patient population that included both patients with TSCI who undergo surgery and those who do not. Street and associates 14 found a 7% incidence of post-operative delirium in their spine trauma group while Kawaguchi and associates 21 and Lee and associates 22 reported 12.5% and 13.6% in their respective elective spine surgery populations. If we isolated only those patients who had surgery, we found a 14.1% incidence of delirium, which is still higher than the incidence reported in the literature. Our study population with TSCI has injuries that are much more severe, involving neurological deficit, whereas other articles with spine surgery and spine trauma groups include patients who have spine conditions and spine fractures without neurological deficit.
The frequent occurrence of delirium in the spine step-down unit compared with other units is expected because it is the intermediate care unit between the ICU and spine ward. Although many studies have reported delirious episodes during ICU stays, 26 the traumatic nature of the injuries to our patient population may impede the diagnosis of delirium. Patients with TSCI are often intubated and sedated in the ICU such that cognitive assessment is difficult and patients are not fully responsive. Consequently, their condition is more stable and amenable to delirium detection in the spine step-down unit.
An understanding of a patient's risk of developing delirium development involves a comprehensive approach that encompasses interpreting risk factors in context with patient characteristics. According to the multi-factorial model of delirium described by Inouye and Charpentier, 10 there is a complex interplay between a patient's initial susceptibility (depicted by their characteristics on admission) and interventions during the process of care that can augment delirium risk. Patients whose baseline risk is low—for example, who are young when first admitted to the hospital—require exposure to more serious precipitating factors or a combination of factors before delirium develops. Alternatively, elderly patients may need only a minor physical insult, such as marginally reduced blood oxygen levels, for delirium to occur.
Age at injury was an anticipated patient characteristic to be associated with delirium given the large body of literature on delirium in the geriatric population. In their review, Martins and Fernandes 27 noted that 30% of hospitalized elderly were affected by delirium, and this number was reflected in on-admission diagnoses, emergency departments, and over the course of hospitalization. In addition, Ushida and associates 28 identified that being over 70 years old was associated with developing delirium in a population receiving cervical spine surgery. Moreover, there is considerable evidence that cognition declines substantially with age, 29 which further suggests that persons who are injured later in life have a more pronounced risk of experiencing delirium.
Initial motor score was another relevant patient characteristic that was associated with delirium. According to the International Standards for Neurological and Functional Classification of Spinal Cord Injury, scores below 50 generally indicate impairment to both the upper and lower limbs. 17 Consequently, patients having greater neurological deficit and ensuing impairment would be more prone to having delirium. These findings correspond with the study by Kawaguchi and associates, 21 who reported that ambulatory status on admission was a predictor of post-operative delirium in patients receiving spine surgery. Essentially, patients who are less mobile and are physically confined to beds or wheelchairs have an increased risk of delirium.
In our investigation of factors associated with delirium occurrence, we found that administering more than three types of any medication was significantly associated with not having delirium. This finding is unusual, but may be explained in context with how the data were collected. For the control group, risk factors were regarded as being present if they were identified at any point during a patient's acute stay. On the other hand, risk factors for delirium cases were deemed present if they arose before delirium onset. Therefore, if a patient with delerium received medications after diagnosis, it would not be included as a risk factor. Consequently, the medication profile of delirium cases may have less than three types of medications because of the study method.
Our results indicate that patients who experience delirium have a considerably greater acute LOS than those who do not. This could suggest that delirium or another associated demographic (e.g., age) or injury (e.g., severity) variable increases LOS. This difference translates to increased costs incurred for the care of delirious patients, as well as a larger burden on staffing and other resources to the health care system. In their study on the costs associated with delirium, Milbrandt and coworkers 30 concluded that patients who experienced at least one delirious episode had significantly higher ICU costs and total hospital costs compared with patients who did not have delirium. In addition, increased costs appear to be related to the severity and length of delirious episodes. 30
Limitations to this study include its sample size and consequently low statistical power. Because it was intended to assess the types of patients with TSCI in whom delirium develops, however, it serves as an initial analysis in this population. Increasing the sample size may reveal additional patient characteristics and risk factors for delirium and may improve generalizability of our results.
The process of delirium identification in acute care may be biased against less serious cases that may not demonstrate the obvious symptoms of delirium. Patients who exhibit symptoms such as withdrawal and lethargy may not be recognized as potentially delirious compared with those who have hallucinations and attention deficits. Also, because this study is based at a single institution, our findings may not be applicable to other institutions where population characteristics and care protocols may vary.
Future directions from this work include increasing the sample size through larger-scale studies and the involvement of different centers so that findings can be applied across institutions. To fully make a case for the value of delirium screening in patients with TSCI, the economic benefit and the impact of delirium on patient outcomes downstream of acute care, such as rehabilitation and community reintegration, must be characterized as well. Demonstrating that early identification and early preventive intervention is effective at reducing the incidence of delirium is a necessary future avenue of research. In addition to performing an economic analysis, it would strengthen these results.
Conclusion
Elderly patients who sustain a TSCI and have a low motor score on hospital admission are at increased risk of delirium. This study provides a foundation for an early screening program that can be introduced during the acute hospitalization of patients with TSCI to potentially facilitate better patient and system outcomes. The implementation of such a program would enable early identification so appropriate treatments are received to reduce the duration and severity of delirious episodes, or identify patients who are at risk and begin preventive measures to lower delirium incidence.
Footnotes
Acknowledgments
We would like to acknowledge Lise Bélanger for clinical knowledge regarding the identification of delirium, So Eyun Park for help with the ethics application, Dr. Nader Fallah for statistical support, and the Combined Neurological and Orthopaedic Spine Program for assistance with patient data access.
Production of this article has been made possible through a financial contribution from Health Canada. The views expressed herein represent the views of the Rick Hansen Institute.
Author Disclosure Statement
Antoinette Cheung, Dr. Nancy P. Thorogood, Yun Zhong, and Dr. Vanessa K. Noonan are employees of the Rick Hansen Institute. Dr. Marcel F. Dvorak previously consulted for the Rick Hansen Institute. For Drs. John T. Street and Charles G. Fisher, no competing financial interests exist.