
Abstract
The optimal mean arterial blood pressure for maintenance of spinal cord perfusion is not known. Our aim was to describe vasopressor usage and examine their effects in patients with spinal cord injury (SCI). We undertook a retrospective cohort study of 131 patients with SCI who received any kind of vasopressors to maintain blood pressure in the neurocritical care unit of a Level 1 trauma center (2005–2011). Vasopressor usage and complications were obtained from the medical record. Neurological outcomes were evaluated by the American Spinal Injury Association score. Dopamine was the most commonly used vasopressor (48.0%), followed by phenylephrine (45.0%), norepinephrine (5.0%), epinephrine (1.5%), and vasopressin (0.5%). Logistic regression analysis demonstrated that complications (e.g., ventricular tachycardia, troponin elevation, atrial fibrillation, heart rate >130 or <50, etc.) due to vasopressors were independently associated with the overall usages of dopamine (odds ratio [OR] 8.97; p<0.001) and phenylephrine (OR, 5.92; p=0.004), age ≥60 years old (OR, 5.16; p=0.013), and complete SCI (OR, 3.23; p=0.028). There was no difference in neurological improvement with either dopamine (OR, 1.16; p=0.788) or phenylephrine (OR 0.96; p=0.940). Incomplete SCI (OR, 2.64; p=0.019) and surgery <24 h after SCI (OR, 4.25; p=0.025) were independently associated with improved outcome. In summary, vasopressors are associated with increased complications in SCI patients. Further prospective studies are required in order to determine the potential benefits and risks of blood pressure management in patients with SCI.
Introduction
S
In 2008 the Consortium for Spinal Cord Medicine introduced their 10th clinical practice guideline: Early Acute Management in Adults with SCI. 10 This document was followed by the American Association of Neurological Surgeons (AANS) 2013 SCI treatment guideline that recommended raising the mean arterial blood pressure (MAP) between 85 and 90 mm Hg for the first seven days following acute SCI. 11 This recommendation ended with the statement, “The issue of whether or not blood pressure augmentation has an impact on outcome following human SCI is important and deserves further study. If augmentation of MAP is determined to be of potential benefit, the most appropriate threshold levels of MAP and the length of therapy need definition.” 5,11
The choice of vasopressors to meet MAP guidelines remains an active research question. Recently, there has been an increased interest in examining effectiveness and complications of vasopressors in septic and cardiogenic shock. Both a 2010 study 12 and a 2012 meta-analysis 13 by De Backer and colleagues found that the incidence of arrhythmias was significantly higher with dopamine than norepinephrine and was associated with an increased risk of death.Both of these studies varied from SCI MAP guidelines in that a much lower MAP target of 70 mm Hg was chosen. In patients with SCI, guidelines/reviews recommend that the vasopressor choice depends on the level of the SCI, with only injuries above T6 requiring a vasopressor with both alpha and beta effects such as dopamine. 9
Our primary objectives were to 1) identify demographic and clinical findings in consecutive patients with SCI admitted to the San Francisco General Hospital (SFGH), intensive care unit (ICU), 2) characterize the vasopressors effectiveness and complications, and 3) design a potential vasopressor strategy that could reduce the rate of side effects among patients in SCI.
Methods
Study design, setting, and participants
We performed an observational retrospective cohort study in order to evaluate the effects of vasopressors on all consecutive patients with SCI admitted to SFGH Level 1 Trauma Center from January 2005 to December 2011 using a Department of Neurosurgery database and cross referencing trauma logs, and searchable terms using electronic medical records (San Francisco, CA). The database is continuously updated with births, deaths, marriages, name changes, patient movements, and trauma incidence from the regional trauma registries. In this cohort study, we retrospectively identified patients with a principal diagnosis of SCI (code 953–957) according to the International Classification of Diseases (ICD), 9th Revision, Clinical Modification, from codes designating discharge diagnoses. To be eligible, patients had to 1) be age ≥18 years, 2) have SCI with neurological deficit requiring admission to ICU, and 3) have vasopressors given for a minimum of 24 h. We excluded children 17 years and younger and patients who did not received any vasopressors. A secondary analysis was performed excluding patients with evidence of hemorrhagic shock. These patients were excluded if they received >3 units of packed red blood cells in the first 24 h after injury or had injuries consistent with ongoing bleeding (e.g., hemothorax, liver laceration, and vascular injury). Research procedures were approved by the University of California, San Francisco institutional review board, exempting the study from individual patient's consent.
Variables
Age, gender, medical diagnoses prior to injury, SCI etiology, Glasgow Coma Scale, level of SCI, completeness/incompleteness of injury based on the American Spinal Injury Association (ASIA) score, ASIA score throughout admission and at discharge, Injury Severity Score (ISS), vital signs, surgical decompression timing, 14 –16 vasopressor types, and complications. Complications were defined as follows: tachycardia (heart rate >130), bradycardia (heart rate <50), new atrial fibrillation, ventricular tachycardia, elevated troponin, electrocardiogram (EKG) ST changes consistent with ischemia, acidosis (pH <7.0), atrial flutter, and skin necrosis. Change in ASIA score during hospitalization was chosen based on multiple studies where early ASIA improvement was predictive of long term neurological outcome. 17,18 To minimize selection bias, the authors responsible for chart review were blinded to the patient's neurological outcome. In addition, a separate blinded investigator evaluated only computerized vital signs and ICU nursing notes to determine hourly heart rates, cardiac rhythms, MAPs, vasopressor types and doses, changes in vasopressors, EKG reports, and troponin levels.
Statistical method
The University of California San Francisco Clinical and Translational Science Institute study statistician was blinded to treatment assignments. Descriptive statistics were used to detail the study cohort and patients who received dopamine versus phenylephrine. For univariate analyses, data are presented as medians with interquartile ranges (IQR) for non-parametric distribution, and as percentage for binary variables. To compare patient level characteristics of vasopressors, Mann-Whitney U and Kruskal-Wallis tests were performed with a Dunn post-hoc test used for continuous variables. The Pearson chi square and Fisher exact test were used to analyze categorical variables. To further analyze the relationship between patients-specific variables and SCI interventions, two outcomes were measured: vasopressor's complications and neurological improvement based on ASIA scores as discharge status. Multivariate logistic analysis was performed in order to calculate odds ratio (OR) and 95% confidence interval (CI) after controlling simultaneously for potential confounders: gender, older age (≥60), complete SCI (ASIA category A), severe injury (ISS ≥15), vasopressors types, and acute surgery (<24 h after SCI) on outcome. All statistical analyses were performed by Predictive Analytics Soft Ware (PASW) statistic 18 for Mac (SPSS Inc., Chicago, IA). All reported p values are two-sided and have not been adjusted for multiple testing.
Results
Descriptive data
Medical records from 221 patients were reviewed. Our mechanisms of SCI may vary from other level 1 trauma centers given the lower amount of high mechanism blunt trauma from motor vehicle collisions but with a higher rate of falls than other institutions (Table 1). A total of 131 patients who received vasopressors were subsequently identified as meeting the study inclusion criteria. One hundred thirteen patients did not demonstrate evidence of added hemorrhagic shock. Eighty-nine patients were excluded because they did not receive any vasopressors and usually had mild injuries allowing discharge within a few days. One patient was also excluded because of his age (≤17).
Vasopressor usage
For the first line of treatment, the majority (95.4%; n=125) received a single vasopressor, and six patients (4.6%) received multidrug therapy. We found that the predominant first choice of vasopressor was dopamine in 60.3% of patients (n=79) patients; the alternative treatment was phenylephrine in 33.6% of patients (n=44). This was most likely a result of dopamine being recommended as the initial agent on the SCI order sheet (Fig. 1). Characteristics of each group were not significantly different, except for a lower ISS in the dopamine groups than phenylephrine (Table 2).
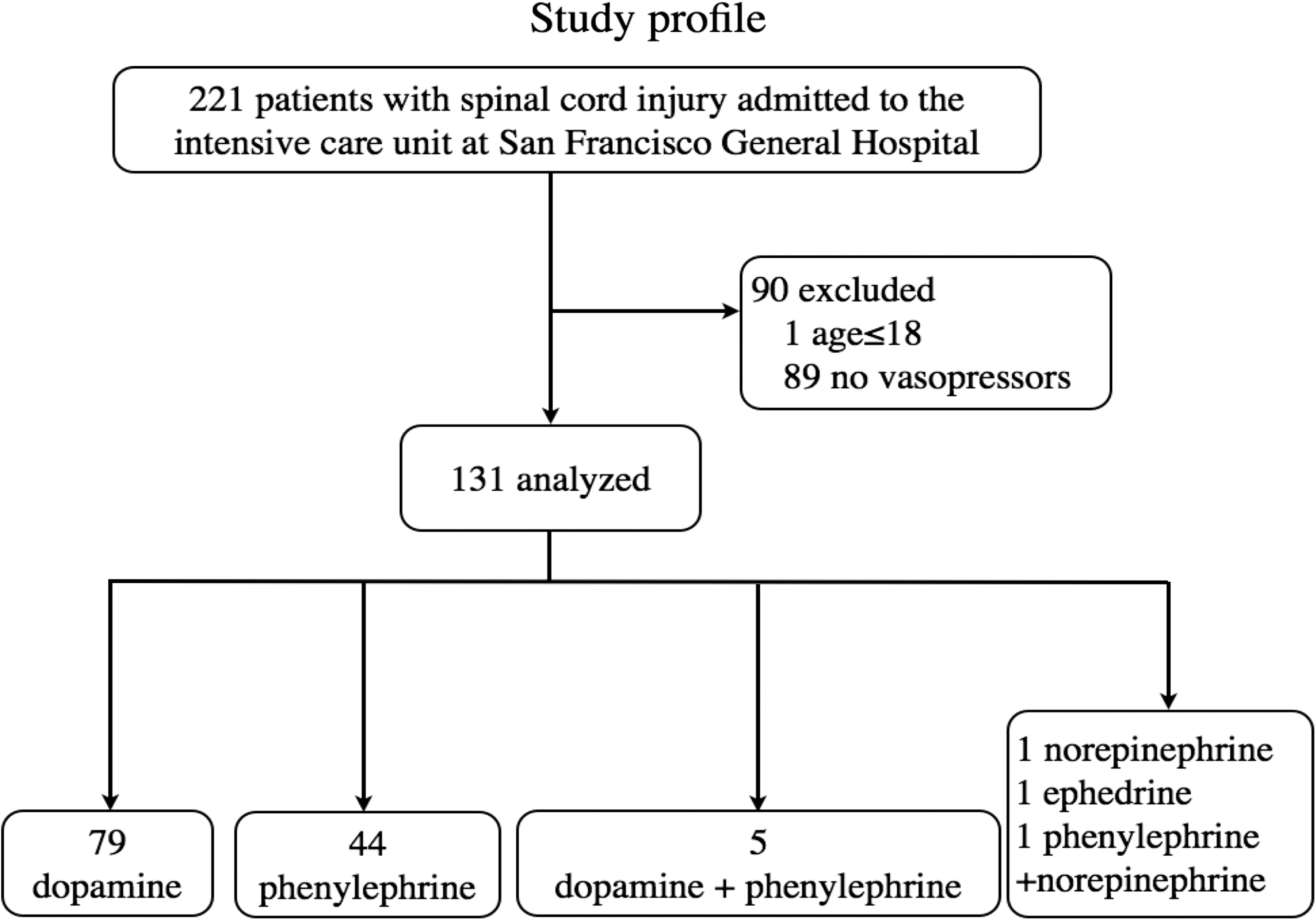
Study profile and derivation of final sample.
=continuous variables reported as median (interquartile range); categorical data reported as n (%); b=significant difference between dopamine and phenylephrine groups only
GCS, Glasgow Coma Scale; ISS, Injury Severity Score; SCI, spinal cord injury; ASIA, American Spinal Injury Association classification.
The rate of first vasopressor complications was 69% (n=85). When adverse events occurred during treatment with the first choice of any vasopressor, patients were usually switched to a second choice. The initial choice of dopamine was changed 69.1% (38/55) while phenylephrine was changed to a different vasopressor 56.7% (17/30; Fig. 2). Many patients had vasopressors changed again after the second pressor caused further complications. The most commonly used vasopressor was dopamine (48.0%), followed by phenylephrine (45.0%), norepinephrine (5.0%), epinephrine (1.5%), and vasopressin (0.5%). Overall, despite the recommendation of 168 h (seven days) of MAP elevation, our patients received only 120 h (5 days; median IQR, 54 h) of MAP goals before they were relaxed to a lower level. In addition, MAP goals were not successfully attained during 28 h (median IQR, 30 h) of the 120 h.
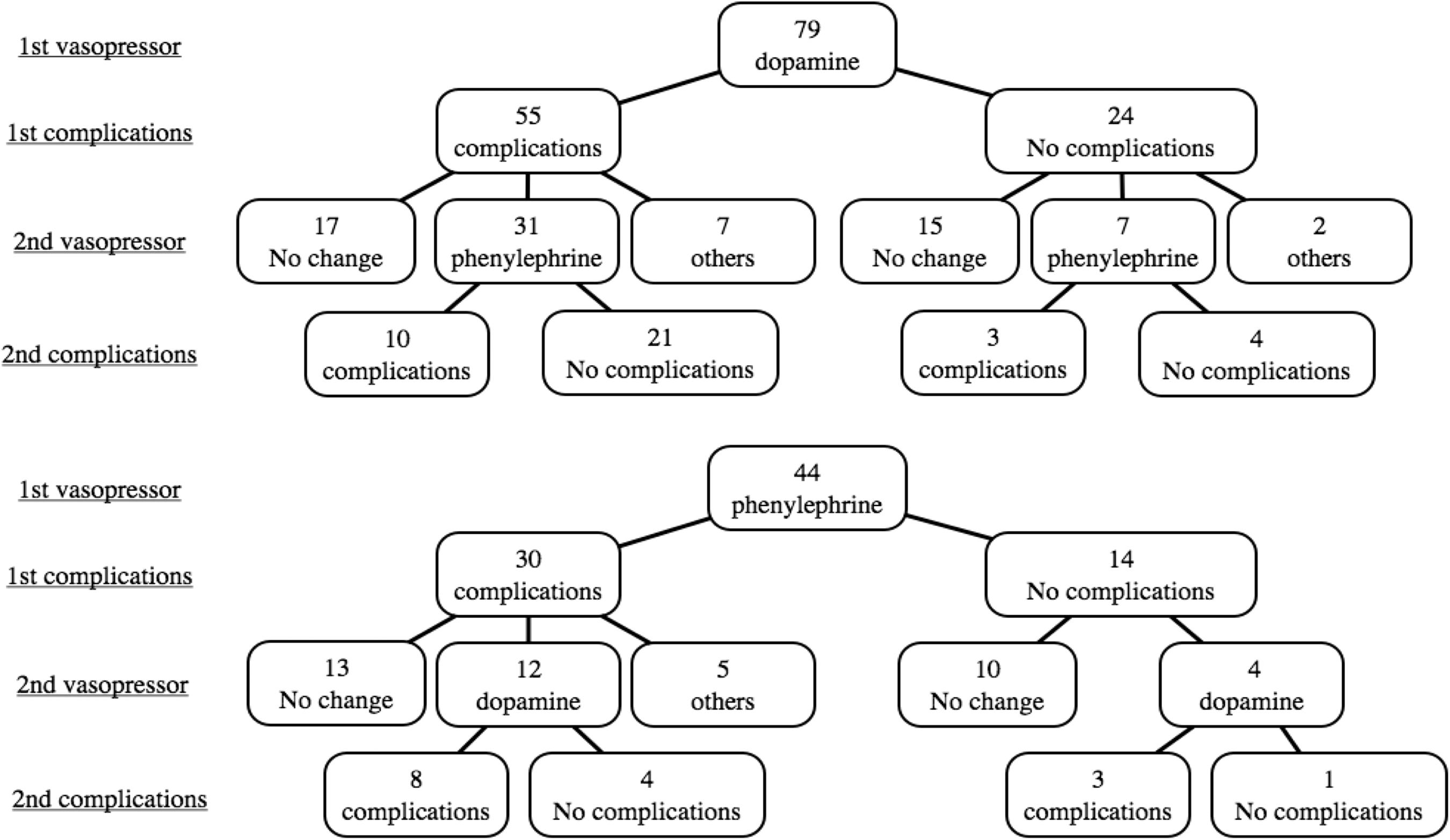
Choice of first vasopressor with number of patients requiring change of vasopressor after complications.
Adverse events
Dopamine caused significantly more complications (69.2% [74/107]), compared with the phenylephrine group (46.5% [47/101]; OR with dopamine, 2.58; 95% confidence interval, 1.56 to 4.54; p=0.0012). Overall, 74.0% of the patients (97/131) who received any type of vasopressor experienced a complication; the most common type of complication was tachycardia (41.2% [54/131]), followed by bradycardia (24.4% [32/131]), atrial fibrillation (12.2% [16/131]), ventricular tachycardia (10.7% [14/131]), elevated troponin/st changes (6.1% [8/131]), acidosis (3.1% [4/131]), atrial flutter (0.78% [1/131]), and skin necrosis (0.78% [1/131]). As expected, dopamine resulted in more tachycardia (dopamine, 35.5% [38/107] vs. phenylephrine, 15.8% [16/101]; OR with dopamine, 2.93; 95% CI, 1.51–5.69; p=0.0012; Fig. 3A) while phenylephrine caused bradycardia (phenylephrine, 20.8% [21/101] vs. dopamine, 10.3% [11/107]; OR with phenylephrine, 2.29; 95% CI, 1.04 to 5.04; p=0.036; Fig. 3B). Dopamine also was associated with significantly more serious complications such as ventricular tachycardia, ECG ST segment elevation, or elevated troponins (dopamine, 10.3% [11/107] vs. phenylephrine, 3.0% [3/101]; OR with dopamine, 3.74; 95% CI, 1.01 to 13.8; p=0.036; Fig. 3C). Atrial fibrillation also was significantly higher in the dopamine group (dopamine, 14.0% [15/107] vs. phenylephrine, 0% [2/101]; OR with dopamine, 8.07; 95% CI, 1.80 to 36.3; p=0.0015; Fig. 3D). Phenylephrine was associated with metabolic acidosis (phenylephrine, 4.0% [4/101] vs. dopamine, 0.0% [0/107]; OR with phenylephrine, 9.92; 95% CI, 0.53 to 186.8; p=0.038; Fig. 3E).
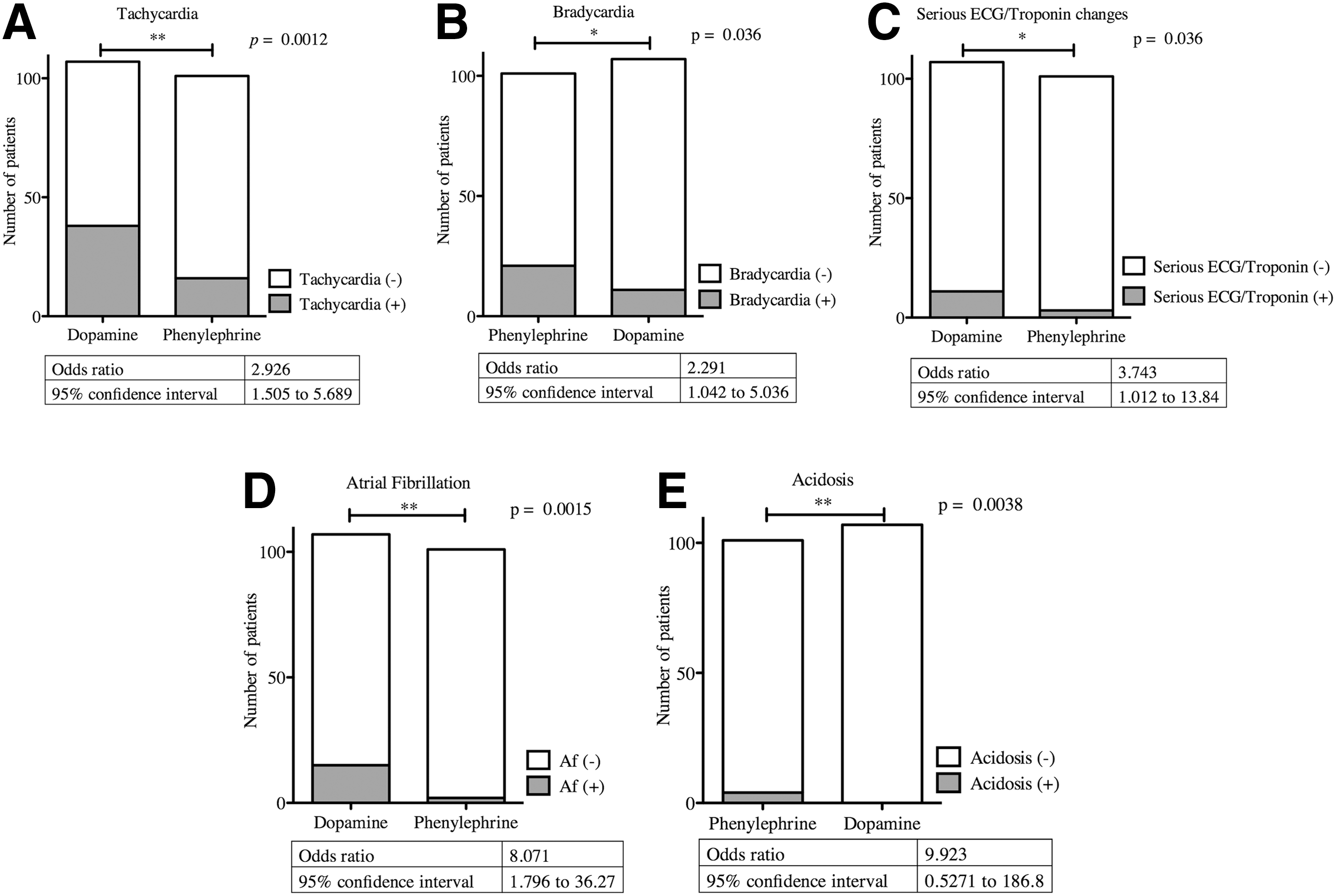
Complication type per vasopressor.
Given the guideline recommendations of using phenylephrine only below T6, we evaluated the choice of vasopressor based on the level of injury. A total of 76.3% of patients (n=100) had an SCI at or above T6, and 23.7% (n=31) had an SCI below T6. Phenylephrine was initially chosen in conflict with the guidelines in 29.0% of injuries (29/100) at or above T6. In contrast, dopamine, with both alpha and beta effects, was initially chosen in 45.2% (14/31) of SCI below T6 despite the guidelines recommending phenylephrine. 10 Of note, inappropriate use of dopamine below T6 had significantly more complications, compared with that of inappropriate phenylephrine use at or above T6 (dopamine, 78.9% [15/19] vs. phenylephrine, 45.2% [33/73]; OR with dopamine, 4.56; 95% CI, 1.38 to 15.3; p=0.0015). The maximum dose of dopamine did not significantly predict the occurrence of complications (with vs. without complications, respectively: median dose [IQR], 10.0 [4.63] vs. 10.0 [4.88] μg/ml; p=0.61). Phenylephrine maximum dose was associated with complications, mainly bradycardia (100.0 [80.0] vs. 80.0 [68.8]; p=0.048).
Age was shown to play an important role in the likelihood of vasopressor complications. Dopamine caused significantly more complications in the ≥60 age group (≥60 age group (83.9% [26/31] vs. ≤59 53.9% [41/76]; OR with dopamine, 4.44; 95% CI, 1.54 to 12.8; p=0.0073), but there were no statistical differences with phenylephrine (p=0.66; Fig. 4). Although phenylephrine did not have an increased rate of complications in elderly patients, its overall rate of bradycardia was significantly higher when given to patients with cervical SCI at or above C4 (at or above C4, 33.3% [10/30] vs. below C4, 15.5% [11/71]); OR with at or above C4, 2.73; 95% CI, 1.01 to 7.38; p=0.001).

Dopamine versus phenylephrine complication rate as a function of age (≥60 years old versus≤59 years old age). **p<0.01
Multivariate analysis
In multivariate analysis, older age (≥60 years), both dopamine and phenylephrine usage, and complete SCI were associated with a significant increase in complications (Table 3). Multivariate analysis of early ASIA outcome data also revealed that neither dopamine nor phenylephrine improved outcome significantly, compared with acute surgery (<24 h after SCI) or initial presence of incomplete injury (Table 4). In an added multivariate analysis of 113 patients without evidence of additional hemorrhagic shock, we found vasopressor complication factors to be similar (Table 5). ASIA outcome data was also similar except for the acute surgery group, which demonstrated a trend towards improvement (Table 6).
p<0.05; ** p<0.01; *** p<0.001; R2=0.20 (Cox & Snell), 0.30 (Nagelkerke), Model χ2=28.29
CI, confidence interval; OR, odds ratio; B, B coefficient; SE, standard error; SCI, spinal cord injury; ISS, Injury Severity Score.
p<0.05, R2=0.12 (Cox & Snell), 0.16 (Nagelkerke), Model χ2=15.08
ASIA, CI, confidence interval; OR, odds ratio; B, B coefficient; SE, standard error; SCI, spinal cord injury; ASIA, American Spinal Injury Association classification; ISS, Injury Severity Score.
p<0.05; ** p<0.01; R2=0.22 (Cox & Snell), 0.33 (Nagelkerke), Model χ2=25.98
CI, confidence interval; OR, odds ratio; B, B coefficient; SE, standard error; SCI, spinal cord injury; ISS, Injury Severity Score.
R2=0.08 (Cox & Snell), 0.11 (Nagelkerke), Model χ2=8.44
ASIA, American Spinal Injury Association classification; CI, confidence interval; OR, odds ratio; B, B coefficient; SE, standard error; ISS, Injury Severity Score; SCI, spinal cord injury.
Discussion
We have examined the use of vasopressors to meet MAP goal guidelines as recommended by the Consortium for Spinal Cord Medicine and the AANS. 10,11 We have shown a significant number of complications requiring vasopressors to be changed in the ICU during the first five to seven days post-injury. In addition, we demonstrate a higher complication rate from dopamine in line with many recent studies suggesting higher arrhythmia rates in septic and other forms of shock. 12,13
Dopamine was significantly associated with complications even when used according to MAP goal guidelines. In addition, dopamine was associated with the most serious complications (ventricular tachycardia/EKG ST segment elevation/elevated troponins) and had an 84% complication rate when used in patients older than 60. Complications from dopamine have been recently shown in septic shock 13 and cardiogenic shock. 12 In a meta-analysis comprising 2768 septic shock patients, dopamine administration was associated with an increase in incidence of arrhythmic events and greater mortality, compared with norepinephrine. In a subgroup of cardiogenic shock patients, dopamine also was associated with an increased mortality. As a result, several national organizations now recommend norepinephrine as first line vasopressor treatment for shock.
Generalizability
The loss of sympatho-excitatory descending input from the supraspinal structures results in a condition known as neurogenic shock. 19,20 The choice of vasopressor according to SCI level is also addressed in the Consortium guidelines. 10 The cervical and upper thoracic injuries through T6 warrant a vasopressor with inotropic, chronotropic, and vasoconstrictive properties. This suggests either dopamine or norepinephrine as first choices. Although dobutamine was used in one past study, 21 it is primarily inotropic and has limited use in SCI due to vasodilation and potential reflex bradycardia. 22 Epinephrine has both alpha and beta effects but may cause arrhythmias and thus may not be a suitable choice. According to the Consortium for Spinal Cord Medicine, a pure vasoconstrictor, such as phenylephrine, is appropriate for low thoracic and lumbar lesions where hypotension is mainly the result of peripheral vasodilation. 10 Our study demonstrated that a significant number of patients received phenylephrine at or above T6 and dopamine below T6 in conflict with the guidelines, most likely due to the pre-guideline patients and physician comfort with dopamine. Dopamine used below T6 caused significantly more complications than inappropriate use of phenylephrine. Also, the incidence of cardiovascular abnormalities following acute SCI is reported to be very common, particularly after cervical injuries. 23 –28 Our data revealed that high cervical SCI (at or above C4) was strongly related to bradycardia after phenylephrine. This complication appeared to be a direct drug effect as patients were only included if they developed heart rates <50 bpm after phenylephrine was started and excluded if already bradycardic.
It is difficult to measure the effectiveness of one vasopressor over another. Despite the recommendation of 168 h (seven days) of treatment, our patients received 120 h (5 days; median IQR, 54 h) of MAP goals before they were relaxed to a lower level. In addition MAP goals were not even attained during 28 h (median IQR, 30 h), demonstrating the difficulty of maintaining MAP goals using vasopressors in trauma and SCI patients. There has been one recent study evaluating the effectiveness of different vasopressors in TBI. 29 Phenylephrine was chosen more frequently than norepinephrine or dopamine. Phenylephrine also was associated with a higher MAP than dopamine and a higher cerebral perfusion pressure than norepinephrine during the 3 h after the start of treatment. The only complication evaluated was heart rate where bradycardia was highest in patients who received phenylephrine. Tachycardia was elevated in the dopamine group followed by norepinephrine and phenylephrine groups. Clinically, MAP guidelines differ in TBI with the goal of maintaining a cerebral perfusion pressure between 50 and 70 mm Hg; thus, it is difficult to compare these TBI studies to our SCI group. 29
There is considerable disagreement within the neurocritical care community as to whether MAP goals should be recommended. The SCI MAP guidelines were primarily based on two studies from 1993 and 1997 respectively. Levi and colleagues in 1993 used dobutamine or dopamine with fluids in 50 cervical acute SCI patients to obtain a MAP of 85 mm Hg for five to seven days. 21 Of note, there was no comparison group or control and some patients received early surgery. The study was designed to evaluate pulmonary vascular resistance and systemic vascular resistance in complete quadriplegia with the data demonstrating a higher sensitivity of the pulmonary vascular bed to the loss of central sympathetic control in complete SCI.
In 1997, Vale and colleagues used dopamine followed by norepinephrine in 70 patients to obtain a target MAP of 90 mm Hg. The study also did not have a control group as it was considered a “pilot study.” 8 All patients had a swan ganz line and were initially resuscitated with fluids and blood prior to vasopressors. There was no comment on vasopressor complications requiring changes. The authors commented that they “arbitrarily selected the MAP of 85 mm Hg as the target even though it is considered high normal compared with non-injured males 15 to 30 years. A duration of seven days was chosen based on data from studies which indicate maximum cord edema and spinal cord vascular congestion occur between three and five days after spinal cord injury.” 30 Summarizing both studies the Consortium guidelines state: “The appropriate resuscitation end point and optimal mean arterial blood pressure for maintenance of spinal cord perfusion are not known. Further study is needed to define ideal MAP and the potential role for elevation of MAP with fluids or pharmacologic treatment.” 10 We attempted to further refine our findings to exclude added hemorrhagic shock patients and found similar complication and outcome results. Our current study highlights the need for further discussion regarding the difficulties and complications in attaining these incompletely studied MAP targets.
Although the current study was retrospectively performed by a single institute, according to the multivariate analysis, neurological improvements were significantly associated with early surgical timing (<24 h after SCI) as with other prospective studies. 14 This finding was reduced to a trend when mixed hemorrhagic shock patients were removed. In our initial cohort, 98 out of 131 patients with SCI underwent surgery, and acute stage surgery (<24 h after SCI) was performed in 27.5% (n=27), which is similar to other studies. 15,16 It has been stated that the 24-h cutoff must be the most feasible time window during which surgical decompression had the promise to obtain a neuroprotective effect. 14 Given our findings, surgical timing should be included in any further prospective trials evaluating vasopressor choices and MAP targets.
Limitations
Some limitations of the study include the small overall number of patients that received vasopressors in each group, which might reflect selection bias. This study also does not specifically address whether MAP guidelines are effective in improving outcome. Although we did gather discharge outcomes for all patients, we do not have long-term post-injury ASIA scores given the large number of discharge/rehabilitation facilities involved and the lack of one year standardized testing. We did not have a meaningful number of patients with ephedrine as either a first or second choice vasopressor and thus cannot comment on the effectiveness of this vasopressor.
Conclusions
In summary, vasopressor use for MAP goals in spinal cord injured patients results in a concerning complication rate requiring multiple vasopressor changes. Dopamine has significantly higher complication rates than other vasopressors and a concerning rate of serious arrhythmias and ischemia. Older patients and those with more severe injuries are especially at risk. Given the continuing questions regarding this therapy, additional vasopressors such as norepinephrine should be studied with different MAP goals to evaluate neurological improvement and avoid preventable complications.
Author Disclosure Statement
No competing financial interests exist.