
Abstract
In this report, we applied diffusion tensor imaging (DTI) methods in 36 patients with uncomplicated mild traumatic brain injury (mTBI) and a comparison group of 37 participants with orthopedic injury. Our aim was to characterize regional and global macro- and microstructural attributes of white matter (WM), gray matter (GM), in addition to volume and diffusivity of cerebrospinal fluid (CSF) to identify and differentiate patterns of acute and short-term recovery. Given that previous DTI reports on mTBI in adults using a region-of-interest approach implicated the corona radiata (CR), corpus callosum, and hippocampus, we analyzed and quantified DTI metrics of these regions using atlas-based methods. The normalized volume percentages of global CSF, GM, and WM were not different between the mTBI and orthopedic comparison (OC) groups at either the baseline or follow-up time points or between the baseline and follow-up time points within the OC group (p>0.17; uncorrected for multiple comparisons). The DTI metrics did not differ between groups at either occasion. However, an increase was noted on follow-up in the OC group in the global mean diffusivity of GM (uncorrected p=0.003) and WM (uncorrected p=0.02), indicating a decrease in diffusivity at the 3-month postinjury, as compared to the baseline scan. An analysis of the DTI data collected longitudinally in the CR show insignificant changes in the OC group (p>0.08; N=37). CR radial diffusivity was found to be elevated in the between-group comparison at baseline (mTBI1 vs. OC1), but did not differ in the within-group comparison (mTBI1 vs. mTBI2; N=19), suggesting the possible resolution of edema. Our analysis of the cross-sectional and follow-up data, which is uncorrected for multiple comparisons, demonstrates dissociation between volumetric (macrostructural) and tissue integrity (microstructural) attributes and shows the potential utility of DTI to capture transient edema in the CR.
Introduction
Mild traumatic brain injury (mTBI) is a major public health concern in both civilian and military populations. 1 –4 Identifying early neuroimaging markers that relate to cognitive and behavioral changes associated with mTBI is an important application of noninvasive quantitative magnetic resonance imaging (qMRI) modalities. 5 –7 Macrostructural attributes, provided through qMRI modalities, include global and regional tissue volumes and cortical thickness. 8,9 Microstructural attributes include magnetization transfer ratio, relaxation time, anisotropy, and diffusivity and may reflect subtle alterations in the microenvironment as a result of changes in water content and tissue integrity. 4,7 Diffusion tensor imaging (DTI) offers sensitive markers of tissue microstructural integrity that could be used to model the biophysical sequelae in mTBI for diagnosis and prognosis. 10 –24 For example, reduction in mean diffusivity (MD) in acute mTBI has been hypothesized to relate to cytotoxic edema, 20 whereas increased MD without concomitant changes in diffusion anisotropy (e.g., fractional anisotropy; FA) may be indicative of vasogenic edema, which could resolve with time. 16,25 –29 A steady decrease in white matter (WM) diffusion anisotropy commensurate with an increase in diffusivities may indicate Wallerian degeneration as a result of diffuse axonal injury or axonal transection. 11 Identification of early injury hallmarks using in vivo qMRI data clearly requires longitudinal, multi-modal data of high quality along with a robust analysis method.
The causes and effects of mTBI are heterogeneous and vary based on multiple injury-related factors, such as type of injury, injury severity, postinjury interval, and location, 1,3 as well as potential individual factors, which may affect vulnerability to injury or recovery (e.g., age at injury, gender, genetic factors, presence of premorbid mood, or other disorders). The application of DTI to mTBI has resulted in somewhat inconsistent results, as highlighted in recent meta-analyses and reviews. 22 –24 For example, whereas several studies reported reduced FA and elevated MD in WM regions in patients with mTBI in acute and chronic stages, 11 –18 others have reported an increased FA and decreased MD in both acute and subacute stages. 19 –21
Other potential sources contributing to discrepancies in the literature to date may involve the degree to which the comparison group is comparable on demographic factors, such as age, gender, and other important demographic factors, including socioeconomic status (SES) or education, as well as the extent to which cognitive and psychological effects of traumatic injury were assessed. Finally, few studies have utilized a longitudinal design that incorporates longitudinal data to assess progression of injury or potential recovery resulting from tissue repair and resolution of edema, which may be crucial in resolving apparent discrepancies in the published literature.
In this study, we applied DTI methods in patients with uncomplicated, nonblast, closed-head mTBI and a comparison group of patients with orthopedic injury. Subjects were enrolled within 24 h and evaluated at 3 months postinjury with MRI at both points to characterize global and regional macro- and microstructural attributes of WM and gray matter (GM), in addition to volume and MD of cerebrospinal fluid (CSF) to identify and differentiate patterns of recovery. 8,9 Given that several previous DTI reports on mTBI in adults using a region-of-interest (ROI) approach implicated the left anterior corona radiata (CR), 15 we analyzed this entire zone using atlas-based methods. In addition, we included the corpus callosum (CC) and hippocampus because these regions are commonly implicated in TBI. 9,16,30
The main aims of this work were to 1) present data quality measures to assure scanner stability and reliability in this longitudinal study, 2) analyze both cross-sectional and longitudinal data using DTI to identify regions that are most vulnerable in this cohort, and 3) attempt to relate the findings to previous work.
Methods
The project reported on here is part of a larger study of mTBI, supported by the Department of Defense (DoD), where a consecutive series of patients have been prospectively recruited in the Houston area's two level 1 trauma centers. At the time of this report, subject enrollment was approximately 30% complete. The definition of mTBI used in this study followed the guidelines of the DoD 31 and the American Congress of Rehabilitation Medicine. 32 This work was approved by the institutional review boards at participating institutions and is compliant with the Health Insurance Portability and Accountability Act. Written informed consent was obtained from each participant before enrollment and study procedures.
Inclusion criteria for both groups included age 18–50 years, injury occurring within the preceding 24 h, and no requirement for hospitalization for the injury for which the participant was enrolled. For participants with mTBI, inclusion criteria also required the presence of a head injury (documented in medical records and/or verified by witnesses), Glasgow Coma Scale (GCS) 33 score of 13–15, alteration or loss of consciousness (LOC) <30 min, post-traumatic amnesia <24 h, and a negative head computed tomography (CT) scan. Inclusion criteria for the orthopedic injury comparison (OC) group included an Abbreviated Injury Severity (AIS) score <3 on an extremity or pelvis injury, with no head injury present. Exclusion criteria for both groups included AIS >3 for any body part, history of significant pre-existing disease (e.g., psychotic disorder, bipolar disorder, post-traumatic stress disorder diagnosed by a psychiatrist or psychologist, or past treatment for alcohol dependence or substance abuse), blood-alcohol level >80 mg/dL at the time of consent, documentation of intoxication, left-handedness, or contraindications for MRI (including claustrophobia and pregnancy). We also utilized the Socioeconomic Composite Index (SCI), 34 which includes the following three components: 1) occupational prestige; 2) annual income; and 3) years of education. A z-score transformation is derived for each of these three components based upon the distribution of the combined groups. The z-score of each of these components is then transformed into a single z-score (see Table 1).
Group Average Values and Comparisons Between Global and Regional DTI Metrics
Numbers in bold type represent p values≤0.05.
Administered only at the baseline interview.
DTI, diffusion tensor imaging; SCI, Socioeconomic Composite Index34; OC1, orthopedically injured comparison group at baseline (<24 h); OC2, orthopedically injured comparison group at 3-month follow-up; mTBI1, mild traumatic brain injury group at baseline (<24 h); mTBI2, mild traumatic brain injury group at 3-month follow-up; ICV, intracranial volume (wbGM+wbWM+wbCSF) in milliliters (mL=cm*cm*cm); wb, whole brain (cerebrum+cerebellum); FA, fractional anisotropy (×1000); MD, mean diffusivity (×106 mm2 sec–1); LV, lateral ventricles; GM, gray matter; WM, white matter; CSF, cerebrospinal fluid; SD, standard deviation; N/A, not applicable.
For this report, we included 36 patients with mTBI (mTBI1; 13 females; 29.0±8.4 years; age range, 18.1–49.7) imaged at 21.2±11.6 h postinjury. Of these, 17 reported no LOC and 19 reported an LOC of 1–10 min. Nineteen of these mTBI patients (4 females; ages, 19.6–49.7) were imaged at both baseline and 3 months (mTBI2; 98±16 days; median, 91). In addition, the orthopedic comparison group of 37 patients (OC; 10 females; 29.4±9.2 years; age range, 20.3–50.4) recruited from emergency departments without head injuries were imaged at baseline (OC1; 25.3±13.5 h postinjury) and 3 months (OC2; 93±14 days).
Magnetic resonance imaging data acquisition
We acquired whole-brain data acquired between June 2010 and September 2012 on a single Philips 3.0 T Intera system with a dual quasar gradient system with maximum gradient amplitude of 80 mT/m, maximum slew rate of 200 mT/m/ms, and an eight-channel SENSE compatible head coil (Philips Medical Systems, Best, the Netherlands). The MRI protocol included high-resolution anatomical T1-weighted (T1w) and fluid-attenuated inversion recovery, along with gradient echo and susceptibility-weighted imaging, to ensure the absence of micro bleeds or incidental pathology. 6,7
Below, we only include basic details on DTI data acquisition.
Diffusion tensor imaging data acquisition
Diffusion-weighted data were acquired using a single-shot spin echo diffusion sensitized echo-planar imaging (EPI) sequence with 32 diffusion gradient orientations, diffusion sensitization of b=1000 sec/mm–2, diffusion gradient pulse duration and separation [δ, Δ]=[26.8, 13.2] ms, and repetition and echo times of 8000 and 55 ms, respectively. EPI image distortion artifacts were reduced by using a SENSE acceleration factor or k-space under sampling R value of two. Slice thickness was 3 mm with 44 axial slices covering the whole brain (foramen magnum to vertex), field of view was 256×256 mm2, and an image matrix of 256×256, with a total scan time of ∼5.8 min. The number of non-diffusion-weighted or b∼0 images was nine, and this provided high signal-to-noise ratio (SNR0=40:60) and high contrast between tissue types.
Diffusion tensor imaging data processing
DWI data were corrected for geometric distortions resulting from eddy currents using the b0 images and was used for removal of nonbrain tissue using the brain extraction tool, BET (
Whole-brain tissue and cerebrospinal fluid segmentation and quantification
Whole-brain CSF (wbCSF) was segmented into ventricular (vCSF) and nonventricular or sulcal CSF (sCSF). 8 Whole-brain GM and WM were segmented using a DTI-based approach. 36 The approach provided volume and corresponding DTI metrics, such as FA, radial diffusivity (RD), axial diffusivity (AD), and MD (MD=[AD+2*RD]/3).
Regional cerebrospinal fluid, gray matter, and white matter segmentation using diffusion tensor imaging
DTI scalar maps were used to facilitate regional tissue segmentation and parcellation, using statistical parametric mapping (SPM) unified and multi-modal segmentation
37
implemented in SPM (
As a representative of deep noncallosal tissue, we focused on the anterior, posterior, and superior segments of the CR (ACR, SCR, and PCR) bilaterally. Regional and global volumes were normalized to the intracranial volume (ICV) obtained from each subject. The ICV was obtained by summing the total GM (cerebral and cerebellar), WM, and CSF (ventricular and sulcal) volumes. 8,36,39,40
Data quality assurance
To assure scanner stability, we acquired water phantom data and analyzed it as described elsewhere. 43,44 We also obtained histogram distributions of regional DTI metrics to assure normality. 45
Statistical analysis
Group comparisons (e.g., mTBI vs. orthopedic comparison) were conducted using unpaired t-tests. Longitudinal data were compared using paired t-tests. Correlations of regional attributes (ICV-normalized volumes, FA, and MD) with age were computed using Pearson's correlation coefficient and comparisons between slopes used the z-Fisher transform. 46 In this study, there are four groups (OC at baseline [OC1], OC at 3 months [OC2], mTBI at baseline [mTBI1], and mTBI at 3 months [mTBI2]), many brain regions (∼200 parcellated GM, WM, and CSF), and five qMRI metrics (ICV-normalized volume, FA, MD, RD, and AD), and hence an estimate of the needed statistical significance would be ∼0.05/(200*5*10) to account for the number of possible tests. In this preliminary analysis, we did not adjust for the number of multiple comparisons (significance, p≤0.05). All computations and statistical analyses were conducted using MATLAB (The Mathworks Inc, Natick, MA).
Results
Demographics and clinical variables
The mTBI and OC cohorts were comparable in gender and age (p=0.85) as well as SES, as measured by the SCI (p=0.51; Table 1).
Water phantom quality analysis
To assure scanner stability with time, we analyzed the DTI collected on a spherical water phantom almost monthly over 4 years (47 time points). The phantom was kept in the scanner room and temperature was ∼18–20°C, controlled by room air conditioning. A central ROI of 21×21 voxels at the scanner isocenter with a volume ∼3.5 mL was automatically placed to quantify the mean and standard deviation (SD) of regional FA (Fig. 1A) and mean diffusivity (Fig. 1B). As shown in Figure 1, there were no clear systematic drifts with time in either average FA (p=0.25) or MD (p=0.16). Average regional FA over 4 years was small ∼0.015±0.002, whereas average diffusivity was approximately 1.88±0.16 (×10–3) mm2 sec–1.

Scatter plot showing (
Magnetic resonance imaging brain data quality
A representative example of the fusion of T1w and DTI on 1 subject is presented in Figure 2A. Figure 2B demonstrates the spatial normalization of each participant's DTI scalar and principal eigenvector map in the MNI space, and Figure 1C illustrates a number of regions used in subsequent analyses. To assure data reliability for quantitative analyses, data on mTBI and OC participants were plotted as a function of age for multiple regions. Sulcal and ventricular CSF volumes or wbCSF volume were normalized by the total ICV obtained from participants in each group at each time point (r=0.36; p=0.03; Fig. 3A). Frontal cortical GM decreased with age (r<−0.40; p<0.01; Fig. 3B,C) and MD increased with age (Fig. 3D) at comparable rates in both groups (p>0.80).

(

Scatter plots of age versus global metrics on selected groups. (
Global macro- and microstructural magnetic resonance imaging group comparisons
Normalized volume percentages of global CSF, GM, and WM were not different between mTBI and OC groups at either the baseline or follow-up time point or between the baseline and follow-up time points within the OC group (p>0.17; Tables 1 and 2). DTI metrics did not differ between groups at either occasion. However, an increase was noted on follow-up in the OC group in global MD of GM (p=0.003) and WM (p=0.02), indicating a decrease in diffusivity at the 3-month postinjury, as compared to the baseline, scan. Microstructural changes in MD in brain parenchyma were tested regionally on the CC genu (gCC) and splenium (sCC), ACR, PCR, and SCR (Fig. 3C) as well as hippocampus DTI as representative of deep WM and GM, respectively.
Group Average Values and Paired t-Test Comparisons Between Global and Regional DTI Metrics in the Baseline and Follow-up mTBI Group
Numbers in bold type represent p values≤0.05.
mTBI1, mild traumatic brain injury group at baseline (<24 h); mTBI2, mild traumatic brain injury group at 3-month follow-up; ICV, intracranial volume (wbGM+wbWM+wbCSF); wb, whole brain (cerebrum+cerebellum); FA, fractional anisotropy (×1000); MD, mean diffusivity (×106 mm2 sec–1);
LV, lateral ventricles; GM, gray matter; WM, white matter; CSF, cerebrospinal fluid.
Regional microstructural magnetic resonance imaging group comparisons
Figure 4A shows the spatial heterogeneity of CC FA in gCC and sCC of the CC for the within-group comparisons (e.g., OC1 vs. OC2 and mTBI1 vs. mTBI2). Note the expected trend in FA, where FA in the splenium is greater than that in the genu. 13,16,21 As an example, Figure 4B shows the expected decrease in FA with increased age in the gCC for the within-group comparison for the orthopedically injured patients, with the difference (OC1>OC2; p=0.02). Figure 4C,D shows the variation of MD with age in the left hippocampus. There were no differences between OC1 and mTBI (p=0.80). Changes are detected using paired t-test comparisons between OC1 versus OC2 (p=0.001) and between mTBI1 and mTBI2 (p=0.01; uncorrected).

(
An analysis of the CR is presented in Figure 5. Radial diffusivity of the six regions of the CR was comparable in the within-group analysis for the OC group (p>0.08; Fig. 5A). Radial diffusivity was found to be elevated in the between-group comparison at baseline (mTBI1 vs. OC1; Fig. 5B,C), but did not differ in the within-group comparison (mTBI1 vs. mTBI2; Fig. 5D), suggesting the possible resolution of edema.
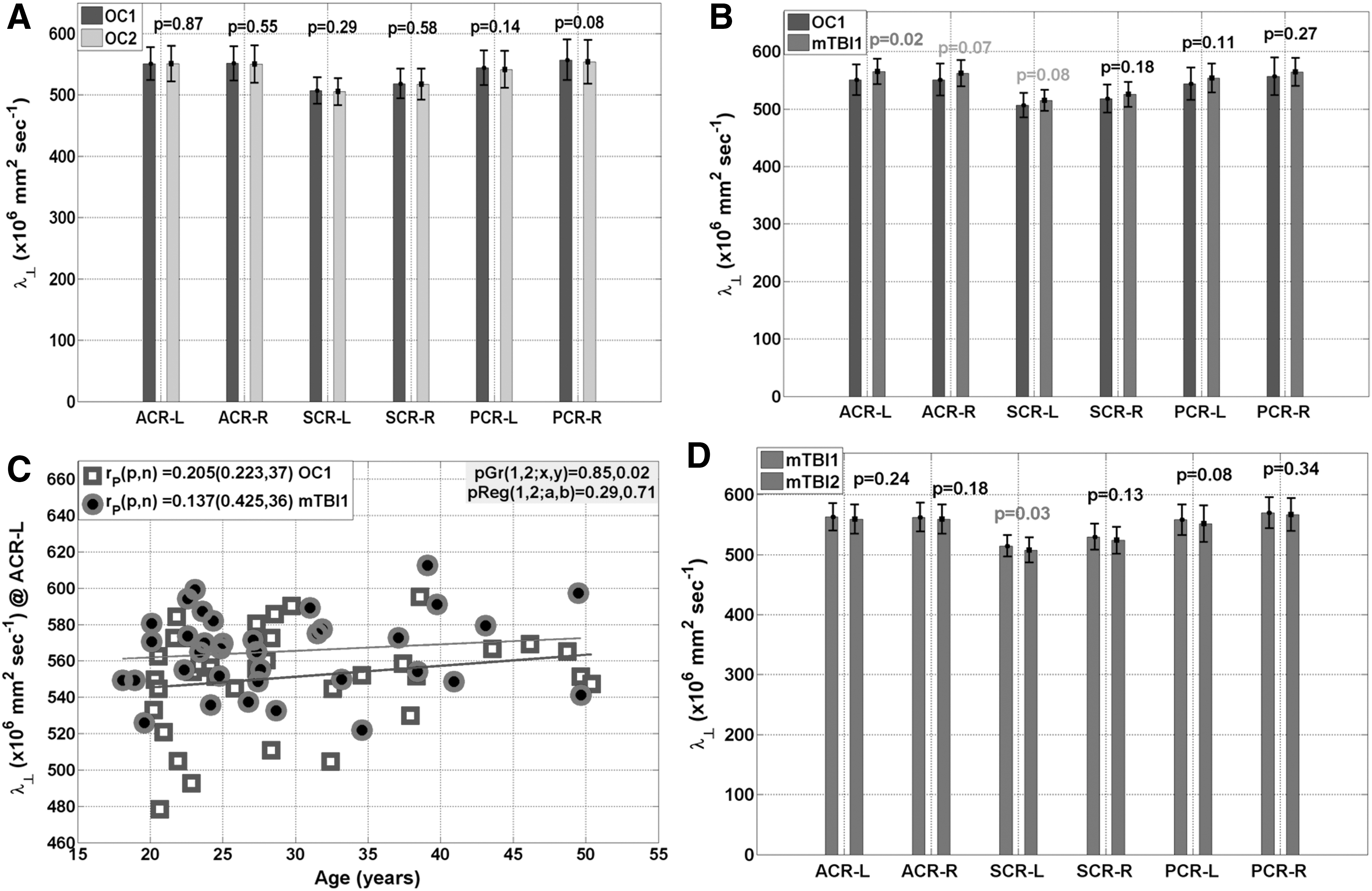
Group comparisons of the average radial diffusivity in the bilateral components of the corona radiata (ACR, SCR, and PCR) between (
Discussion
In this study, we analyzed the water phantom data to assure scanner stability. We also analyzed brain data collected from two cohorts comparable in age (∼20–50 years) and gender imaged at two different time points to identify patterns of acute (∼24 h postinjury) and short-term (∼90 days postinjury) DTI characteristics and volumetry. The measured water phantom FA nonzero values were small and reflect SNR-related overestimation bias, 43,44,45,47 whereas the measured water diffusivity values reflect accurate estimation, as reported in the literature, at comparable temperatures. 44,48 Water phantom diffusivity measurements showed small fluctuations within tolerable experimental errors mainly as a result of room temperature fluctuations and scanner table vibrations, as reported by others. 44,49 Global and regional changes in WM, GM, and CSF volumes were not different between controls and mTBI. An important aspect of this work is that almost all mTBI patients included were characterized by a GCS=15 and had negative head CT; additionally, the study included an orthopedically injured comparison group that was exposed to a traumatic experience, without head injury, to account for systemic and psychological responses to the stress of a physical injury and predisposing risk factors.
In data collected for this study to date, we did not find evidence for longitudinal change in either the mTBI or the OC comparison group in volumetric measures, suggesting that these measures may not be sensitive to subtle changes in the milder end of the spectrum of mTBI, at least at a group level.
The measured whole-brain and regional values for CSF, WM, and GM and expected age-related change resulting from normal late development and early aging in controls are consistent with published in vivo MRI 50,51 and postmortem 52 trends for volume. However, further study of changes within subsets of patients with mTBI (e.g., those with findings on CT or MRI, those with greater injury severity, as measured by GCS score, duration of LOC or post-traumatic amnesia, those with certain symptoms or persistent symptoms, and so on) is warranted.
Consistent with a previous report, 3 subtle changes in WM microstructure were detected in CR radial diffusivity and hippocampus MD, suggesting that these regions may be more vulnerable and may be used as early injury neuroimaging markers.
The short-term trends observed in the mTBI cohort (N=19; baseline vs. 3 months) indicate a pattern of normalization or recovery, as evidenced by a decrease in both AD and RD without a change in FA, which could be indicative of possible resolution of transient edema 25 –29 as a result of mTBI, as has been reported by others. 16,17,21
It is well documented that DTI variables are region 53 and age dependent 54,55 ; hence, interpretation of the DTI results requires caution because the effects of injury on subsequent development is yet undetermined, even in the age range represented by our sample. However, our between-group analyses at baseline indicated that both mTBI and OC groups showed comparable and expected change over time on regional and global metrics. Moreover, our measurements of the lateral ventricular CSF diffusivity indicated consistency and stability of the data in both mTBI and OC cohorts, as has been reported previously. 56
A complete account of the biophysical contributors to in vivo DTI brain measurement is not currently available. 53,57 Reduction in FA in WM commensurate with an increase in RD may indicate the presence of demyelination, whereas injury to the axonal cytoskelectal structure without axonal transaction may be marked by a reduction in FA, along with increased AD. DTI could not reliably distinguish such mechanisms without additional serial and histological data. 57,58 We observed decreased diffusivities over time without a change in FA, which is indicative of the resolution of edema 25 –29 by 3 months postinjury.
Study limitations
Analysis of the data at only two time points (acute baseline and short-term follow-up) is a limitation of this study. We also did not analyze the potential interplay of regional and global qMRI metrics with cognitive, emotional, and behavioral measures. This study also utilized a group of patients with mTBI on the mildest end of the injury spectrum, according to conventional measure of injury severity (e.g., GCS, imaging, length of LOC, and post-traumatic amnesia) post groups, and did not include a healthy noninjured group. We also analyzed several regions and did not account for multiple comparisons resulting from the preliminary nature of this analysis in the context of an ongoing, active study. Because of scan-time considerations, we have not acquired additional MRI data, such as diffusion measurements with multiple b-factors, 59 water content maps, 29 and regional cerebral blood perfusion, 60 to help model and assign more specifically the biophysical contributors to the measured DTI-based findings.
In conclusion, despite these limitations, we have presented preliminary evidence of changes over time after injury that suggest some form of recovery or repair that is common between the mTBI and OC groups. The study of long-term or chronic effects of mTBI on brain structure and function is warranted.
Footnotes
Acknowledgments
This study was funded by the Dunn Research Fund (to K.M.H) and awards from the Congressionally Directed Medical Research Program of the Department of Defense (W81XWH-08-2-0133, W81XWH-08-2-0135, W81XWH-08-2-0138, W81XWH-08-2-0132, W81XWH-08-2-0149, W81XWH-08-2-0142, W81XWH-08-2-0140, and W81XWH-08-2-0131).
Author Disclosure Statement
No competing financial interests exist.