
Abstract
This study investigated corticomotor excitability and inhibition, cognitive functioning, and fine motor dexterity in retired elite and amateur Australian football (AF) players who had sustained concussions during their playing careers. Forty male AF players who played at the elite level (n=20; mean age 49.7±5.7 years) or amateur level (n=20; mean age 48.4±6.9 years), and had sustained on average 3.2 concussions 21.9 years previously, were compared with 20 healthy age-matched male controls (mean age 47.56±6.85 years). All participants completed assessments of fine dexterity, visuomotor reaction time, spatial working memory (SWM), and associative learning (AL). Transcranial magnetic stimulation (TMS) was used to measure corticospinal excitability: stimulus-response (SR) curves and motor evoked potential (MEP) 125% of active motor threshold (aMT); and intracortical inhibition: cortical silent period (cSP), short-interval intracortical inhibition (SICI), and long-interval intracortical inhibition (LICI). Healthy participants performed better in dexterity (p=0.003), reaction (p=0.003), and movement time (p=0.037) than did both AF groups. Differences between AF groups were found in AL (p=0.027) and SWM (p=0.024). TMS measures revealed that both AF groups showed reduced cSP duration at 125% aMT (p>0.001) and differences in SR curves (p>0.001) than did healthy controls. Similarly, SICI (p=0.012) and LICI (p=0.009) were reduced in both AF groups compared with controls. Regression analyses revealed a significant contribution to differences in motor outcomes with the three measures of intracortical inhibition. The measures of inhibition differed, however, in terms of which performance measure they had a significant and unique predictive relationship with, reflecting the variety of participant concussion injuries. This study is the first to demonstrate differences in motor control and intracortical inhibition in AF players who had sustained concussions during their playing career two decades previously.
Introduction
T
Recently, sports concussion in Australian football (AF) has similarly become an area of concern and debate. 9,10 However, to date, research has been limited to data gathered from hospital admissions 11 –13 or self-reported experiences of concussion in former elite players. 14 There have been no studies investigating the neurobiological outcomes of concussion in AF, despite the Australian Football League (AFL) Medical Officers Association 15 estimating that there will be six to seven concussions per team per season.
Studies investigating manifestations of previous concussions in American football 7,16,17 have used techniques such as electroencephalography (EEG) and transcranial magnetic stimulation (TMS) to investigate the underlying neurobiology of long-term concussion. Employing EEG, these investigators demonstrated delayed and attenuated event-related potentials (P3 component) illustrating electrophysiological changes during tests for episodic memory (P3a component), and the ability to shift attentional resources to novel stimuli presented (P3b component) in athletes 2 years post-concussion, 16 as well as in long- term retired athletes who had sustained a concussion 30 years prior. 7
De Beaumont and colleagues 7,16,17 have also investigated motor cortex changes following sports concussion using TMS. In the same cohort of athletes, increases in TMS cortical silent period (cSP) duration in the motor cortex (M1) were observed in both groups of concussed athletes (2 and 30 years post), compared to non-concussed athletes. For example, the lengthened cSP found in studies by De Beaumont et al. 17 was accompanied by reduced movement velocity during performance of the rapid alternative movement task. The cSP is typically believed to index the activity of inhibitory γ-aminobutyric acid (GABA)B receptors. 18
The present study is the first to utilize such assessments, specifically TMS, cognitive tests of memory and learning, and fine dexterity, in an AF population group. Our aim was to investigate the presence of any chronic neurobiological and behavioral effects of concussion, and to ascertain whether there is a relationship between neurobiological measures, via TMS, and functional motor and cognitive outcomes. We hypothesized that there would be differences between the AF groups (combined) and the healthy control group, and between the two AF groups (elite vs. amateur). Our data are particularly novel in that they include comparisons between elite and amateur AF players and healthy age-matched controls.
Methods
Participants
Sixty male participants were recruited for the study. Table 1 illustrates participants' characteristics. Twenty participants had played professionally at the elite level (AFL), whereas 20 sub-elite players had played at amateur levels. Both groups were compared with 20 age-, education-, and gender-matched healthy participants who had never received a concussion injury. Control participants were recruited through approved advertisement and also via word of mouth. With participants self-reporting brain injury from two decades previously, we used the AFL classification, which defined a concussion as a brain injury that results in the player missing the following game. 15
Grayed boxes in table refer to control participants not reporting concussion injury.
AF, Australian football.
All participants were screened prior to testing for suitability to TMS. This included obtaining self-reports concerning current medications, implanted neuro-stimulators, screening for other neurological conditions, and musculoskeletal pain. One potential participant was excluded prior to the study because of risk of seizure following a history of epilepsy. All testing procedures (including pre-screening procedures, concussion history, current physical activity levels, neuropsychological and fine motor control testing, and TMS) were completed in one visit to the laboratory taking 60–90 min. The university human research ethics committee, conforming to the Declaration of Helsinki, approved the study.
Neuropsychological and fine motor control assessment
Participants were assessed for multiple aspects of cognitive functioning; namely, spatial working memory, associated learning, and visuomotor reaction time, using the standardized tasks from the Cambridge Neuropsychological Test Automated Battery (Cambridge Cognition, UK). During the spatial working memory task, participants were required to find tokens hidden behind colored boxes, to make sure that they remembered where tokens had been previously hidden. Associated learning assessed the participant's ability for learning novel information; participants were required to learn the locations of visual patterns on the screen. Visuomotor reaction time assessed the participant's ability to respond and move to a stimulus displayed on the computer screen. Upon seeing the stimulus appear on the screen participants were instructed to release the press-pad key and touch the stimulus on the screen as quickly as possible. The outcome measured was a reaction time (stimulus presentation to release of key pad) and movement time (release of key pad to screen touch).
Fine motor control was tested using the O'Connor Finger Dexterity test (Lafayette Instrument, USA). This well-established test, which has demonstrated good to excellent predictive validity, 20 –22 requires the manipulation and placement of three small pins into each hole. We used a modified form of the O'Connor Test by measuring the time it took to place three pins into one hole on three rows of the board (30 holes in total). 23 Because of learning effects, 22,23 participants performed the test prior to actual assessment.
TMS, M-wave, and electromyography (EMG) recordings
Using well-established methods, 24 –26 TMS was applied over the contralateral M1 with surface EMG (sEMG), using bipolar Ag-AgCl electrodes recording 500 ms responses in the first dorsal interosseous (FDI) muscle of the participant's dominant hand (PowerLab 4/35, ADInstruments, Australia).
Active and resting motor evoked potentials (MEPs) were obtained using a Magstim 200 2 stimulator (Magstim Co, UK) with a figure of eight D70 2 coil (external loop Ø105 mm). For reliability of coil placement, participants wore a snugly fitted cap (EasyCap, Germany), positioned with reference to the nasion-inion and interaural lines. The cap was marked with sites at 1 cm spacing in a latitude–longitude matrix, to ensure reliable coil position throughout the testing protocol.
At the location of the “optimal site,” where the largest MEP could be observed, the active motor threshold (aMT) was quantified, during a controlled, low-level voluntary contraction of the FDI muscle at 10% of maximal voluntary contraction (MVC). aMT was identified by delivering TMS stimuli at intensities (5% of stimulator output steps, and in 1% steps closer to threshold) from a level below the participant's threshold, until an MEP of at least 200 μV and associated silent period could be measured in at least 5 of the 10 stimuli. Resting motor threshold (rMT) determination was completed using the same protocol as aMT, but with the muscle in a relaxed state. rMT was defined as an observable MEP being at least 50 μV in 5 of the 10 stimuli. Fifteen sweeps were taken at test stimulus intensity of 125% of aMT or rMT (30 pulses in total), and stimuli were spaced between 8 and 10 sec to avoid stimulus anticipation.
Single pulse MEPs, from both active and resting conditions, were measured from the peak-to-trough difference of the waveform, and normalized as a percentage to the maximum motor response (Mmax). SP duration was taken from the onset of the MEP waveform (during active contraction of the FDI muscle) to the return of uninterrupted EMG. 18
Stimulus-response (SR) curves
SR curves for excitability and inhibition were completed using single pulse TMS of increasing intensities. 27 Ten stimuli, at random intervals between 8 and 10 sec were delivered at 90%, 110%, 130%, and 150% of aMT. A break of 30 sec was provided between each set of 10 stimuli.
SR curve mean MEP amplitudes and SP durations were quantified and plotted at each stimulus intensity. MEPs were plotted against stimulus intensity, with the data fitted using a nonlinear Boltzmann sigmoid equation (below) using Prism 5 (Graphpad software Inc., California, USA):
Where MEP is the motor evoked potential amplitude (normalized to M-wave); s represents stimulus intensity (% of stimulator output); and MEP amplitude (as a function of stimulation intensity) from Bottom (minimum MEP values, constrained to zero) to Top (maximum MEP plateau value, peak height). V50 represents the stimulus intensity at which the MEP amplitude is 50% of the MEPmax (half peak slope).
Paired-pulse measures
Both short-latency intracortical inhibition (SICI) and long-latency intracortical inhibition (LICI) were measured. SICI was measured with the FDI at rest using an interstimulus interval (ISI) of 2 ms, a conditioning stimulus of 80% rMT, and a test stimulus of 125%. 28,29 Fifteen sweeps were delivered at random intervals between 8 and 10 sec, and SICI was expressed as a ratio of the paired-pulse MEP to the single pulse resting MEP. 30
The mechanism of action of the LICI appears to resemble the cSP, with evidence that LICI may be related to the late portion of the cSP, and mediated via action of γ-aminobutyric acid (GABA), particularly GABAB receptors. 31 –34 However, pharmacological studies have suggested that the two phenomena are not identical, as they can respond differently, because of the administration of GABAB selective agonists. 35 Fifteen sweeps were delivered at random intervals between 8 and 10 sec. LICI was measured in the resting FDI at an ISI of 100 ms, with suprathreshold conditioning stimuli and test stimuli at the aforementioned test pulse. 30,36 –38
Statistical analysis
All data were screened for normal distribution using Shapiro–Wilk tests, and found to be normally distributed. Participant details (Table 1) were compared between groups using one way ANOVA or t test. All dependent variables (participant characteristics, neuropsychological test results, fine motor control, pre-stimulus EMG, MEPs, SP durations, SICI, LICI, and SR curve data) were compared, using planned comparisons to directly test the hypotheses stated. Specifically we compared the difference between the combined AF groups and the control group, and between the two AF groups. Standard regression analyses were performed between intracortical inhibition and movement data. Data are presented as mean (±SD) and α was set at p<0.05.
Results
All participants recruited completed all tests with no adverse effects. Recruited participants, footballers and healthy controls, did not report having any implanted neurostimulators, taking pain medication, or having any chronic musculoskeletal pain. Two participants in the AF group reported being on medication for unrelated (cardiovascular) conditions. As seen in Table 1, there were no statistical differences between the groups for age, height, weight, and handedness. Similarly there were no differences between the two AF groups for the number of concussions or the time since their last concussion.
Neuropsychological and fine motor control
Table 2 presents the data from the neuropsychological and fine motor control testing, respectively. Planned comparisons revealed significant differences in performance times for the O'Connor test, and the reaction time (both reaction to stimulus and movement time). The O'Connor test showed that the healthy control group performed significantly better than the combined AF groups (F 1,57=9.542; p=0.003), but no difference was observed between the amateur and elite AF groups (F 1,57=0.159; p=0.691). Reaction time (stimulus to onset) showed significant differences between the healthy control group and the combined AF groups (F 1,57=9.907; p=0.003), with no differences between the two AF groups (F 1,57=2.302; p=0.061). Movement time component (movement to target) showed significant differences between the healthy control group and the AF groups (F 1,57=5.299; p=0.037), with no differences between the two AF groups (F 1,57=2.05; p=0.086). Comparison of paired-associative learning total errors between the two football groups revealed that the elite footballers performed worse than the amateur footballers (F 1,57=5.118; p=0.027). However, no differences were observed when comparing the healthy control group with the combined football groups (F 1,57=0.404; p=0.527). Paired-associative learning for six shapes showed no significant differences between the groups (F 1,57=1.394; p=0.127). Similarly, no differences were observed for spatial working memory error between the healthy group and football groups (F 1,57=1.236; p=0.269). However, comparison within the football groups revealed that the amateur player group performed significantly worse than did the elite group (F 1,57=5.349; p=0.024).
Indicates significant difference between healthy control and combined Australian football (AF) group data (p<0.05); +Indicates significant difference between elite and amateur playing groups (p<0.05).
TMS
Planned comparisons showed no showed no significant differences between groups for mean normalised MEP amplitude (Elite: 19.7±8.25%; Amateur: 22.2±10.01%; Control: 23.9±11.71%; F 1,57=1.173; p=0.283). Mean cSP showed that the AF players displayed significantly reduced cSP duration compared with healthy controls (mean AF groups: 98.31±26.05 ms; mean Control: 136.33±16.99 ms; F 1,57=38.539; p>0.001). No differences were observed between the two AF groups (F 1,57=1.131; p=0.292). Figure 1 illustrates overlaid cSP sweeps for all participants in the Elite Group compared with typical examples in the Control group.
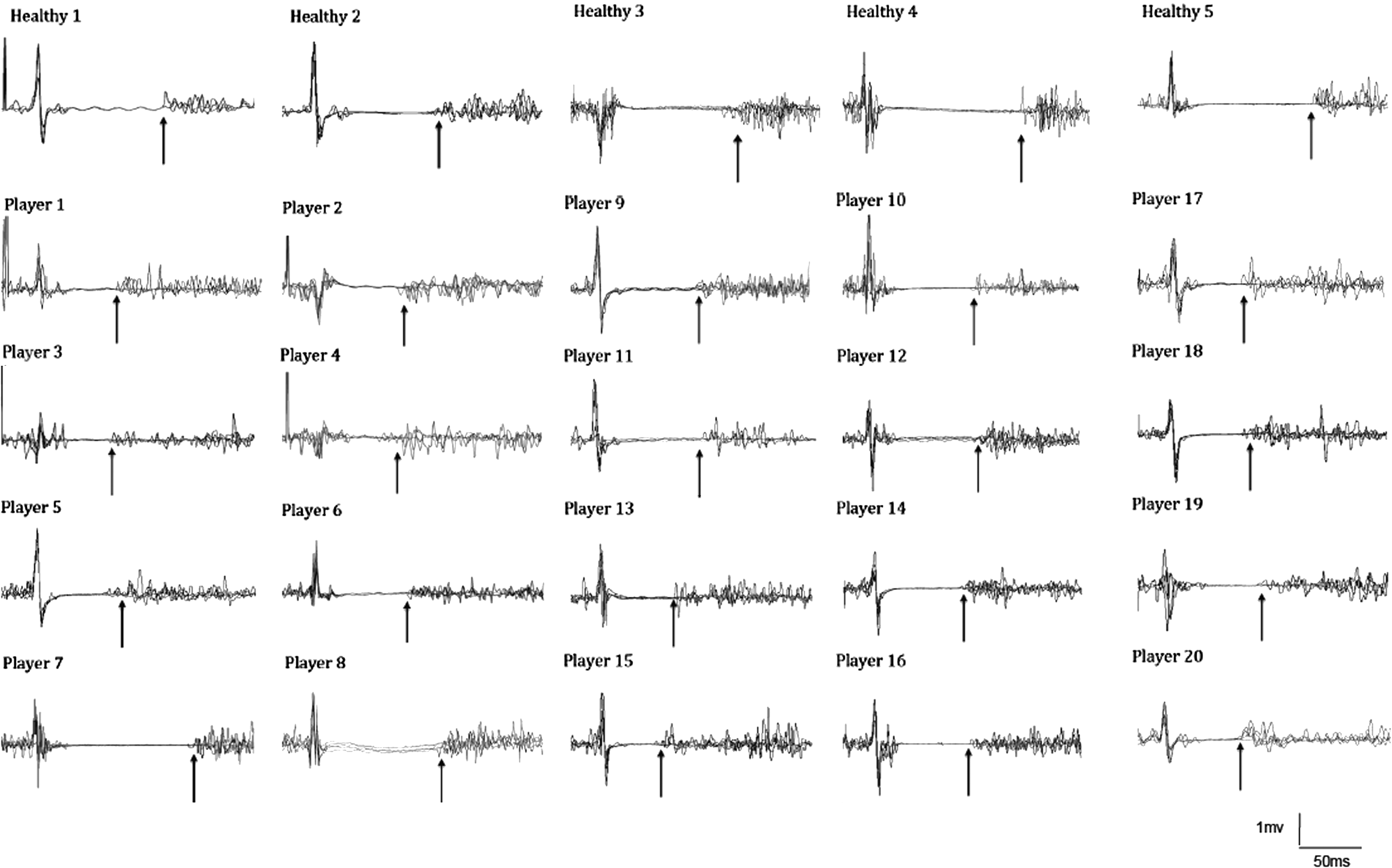
Examples of five overlaid motor evoked potential (MEP) sweeps from the 20 elite Australian football (AF) players (Players 1–20) compared with 5 overlaid sweeps from healthy age-matched controls. Arrows indicate duration of the cortical silent period (cSP) from the onset of MEP to the return of uninterrupted electromyographic (EMG) activity.
Mean SICI showed that AF players showed significant reduction in mean SICI of 12% compared with controls (AF players: 37±17% vs. Control: 25±14%; F 1,57=8.599; p=0.005), with no difference between the two AF groups (AF elite: 38±19% vs. AF amateur: 35±17%; F 1,57=1.577; p=0.253). Mean LICI showed that AF players showed significantly reduced mean LICI by 14% compared with controls (AF players: 51±19% vs. Control: 38±17%; F 1, 58=18.734; p>0.001). No differences were observed between the two AF groups (AF elite: 49±19% vs. AF amateur: 52±17%; F 1,57=0.010; p=0.918). Regression analyses were conducted to assess the capacity of movement dexterity, visuomotor reaction, and movement time to predict intracortical inhibitory measures. For cSP duration, in combination, the predictors made a significant contribution to differences in cSP, accounting for 35% of the variance in (r2 =0.352, Adj. r2 =0.317, F 3,57=10.304, p>0.001). Of the three predictors (O'Connor, reaction time, and movement time), the O'Connor (β=−0.348, t=−2.866, p=0.006) and reaction time (β=−0.369, t=−2.842, p=0.006) made significant unique contributions, accounting for 9.36% and 10.3% of the variance, respectively. Similarly, the combination of predictors made a significant contribution to differences in SICI, accounting for ∼19.5% of the variance in cSP (r2 =0.194, Adj. r2 =0.151, F 3,57=4.563, p=0.006). Of the three predictors, the O'Connor (β=−0.370, t=3.059, p=0.004) and reaction time (β=−0.339, t=−2.437, p=0.018) made unique contributions, accounting for 13.69% and 8.7% of the variance, respectively. For LICI, the combination of predictors made a significant contribution to differences accounting for 14% of the variance in LICI (r2 =0.14, Adj. r2 =0.094, F 3,57=3.082, p=0.034). Only the O'Connor made a unique contribution (β=0.253, t=2.010, p=0.049), accounting for 6.45% of the variance.
SR curves
Group mean normalized MEP and cSP duration SR Curves are shown in Figure 2a and b. No differences were observed in calculated normalized MEP curves between groups (V50: F 2,57=1.293; p=0.282; curve slope: F 2,57=1.234; p=0.299; curve top: F 2,57=0.98; p=0.381). No differences were found in calculated cSP duration for V50 (F 2,57=3.096; p=0.06) or curve slope (F 2,57=0.566; p=0.571). ANOVA revealed difference in SR curve top between groups (F 2,57=5.159; p>0.001) with planned comparisons showing a significantly higher calculated curve top in than control group than in the AF groups (F 1,58=5.306; p=0.025). No differences were observed in the calculated curve top between AF groups (F 1,38=1.847; p=0.182).
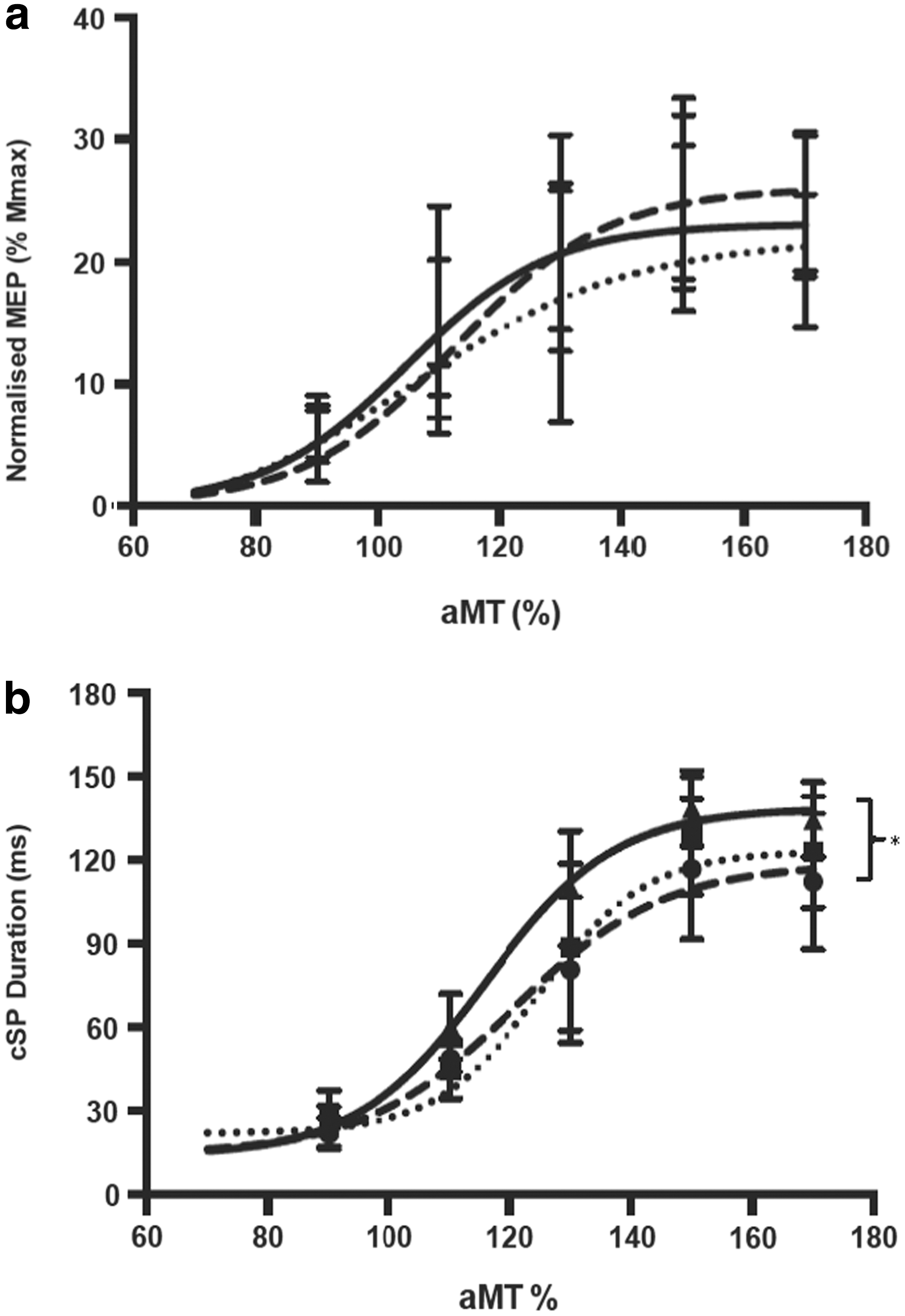
Calculated stimulus response curves for group normalized motor evoked potential (MEP)
Discussion
This study is the first to report corticomotor changes in a population of retired elite and amateur AF players who had previously reported multiple concussions. To date, studies on concussion in AF, at both the elite and amateur levels, have only presented hospital admission rates, or data on players' self-reported concussions. 11 –14,39 King et al. 14 reported that 73% of retired AF players who had played at the highest levels (AFL) recounted having had at least one concussion during their playing career. Further, more than half of these players reported having had multiple concussions. However, it is difficult to arrive at a true figure, as most concussions are not recognized and/or reported. 8,40,41 The long-term neurobiological effect of concussion in AF players, both at the elite and sub-elite levels, is unknown.
The main finding of the study was that we observed a significant reduction in the cSP duration at 125% aMT, in calculated SR curves, and reduction in SICI and LICI in both AF groups, compared with healthy age-matched controls. Changes in intracortical inhibition were associated with reductions in performance on the O'Connor test and visuomotor reaction time. The combination of predictors made a significant contribution to differences in the three measures of intracortical inhibition (cSP, SICI, and LICI). For cSP the O'Connor, reaction time and movement time each showed a significant unique contribution. For SICI, the O'Connor and reaction time made unique contributions. For LICI, only the O'Connor made a unique contribution.
Importantly, changes in corticomotor measures after sustaining a concussion more than two decades previously were not limited to the elite football group. A unique aspect of AF generally, and pertinent to the Australian sporting system, is that the competition is club based (as opposed to the college-based sports system in North America). This means that the majority of those who play AF participate at sub-elite and amateur levels. Unlike the elite levels of football (that is, professional players who compete in the AFL) many of those who play at amateur club level AF do not have immediate access to medical care during or following games. Moreover, at both levels, it is well recognized that many players do not have, or may not seek, access to long-term medical care in retirement.
Our findings in changes in cSP, SICI, and LICI are consistent with changes in GABAergic activity. However, the regression analysis suggests that the three measures of inhibition differed in terms of the performance measures with which they had significant and unique predictive relationship. This may reflect the variety of concussion injuries (such as severity and frequency) present in the participants. Moreover, as these concussions were self-reported, it is not possible to be certain of the extent of the injury received. Therefore our data, from a predictive perspective, should be viewed with some caution, and further studies should be completed with another independent sample to validate these initial findings. In spite of this, GABA receptors play an important function in neural excitability, 42,43 with SICI relating to GABAA activity, whereas cSP and LICI reflect GABAB activity. 18,44 Functionally, intracortical inhibition has been suggested to reflect and influence both motor and behavioral outcomes. For example, cSP has been shown to be longer in healthy older people than in younger people, 30 and is reduced during execution of fine movement control tasks. 26,45 However, the changes observed in cSP and paired-pulse responses in the AF players, also provide evidence of GABA involvement in response to pathology, such as concussion. As discussed in the review by Demirtas-Tatlidede et al. 46 increased GABA receptor activity occurs in response to not only acute but also chronic concussion/traumatic brain injury (TBI). This has been illustrated in previous studies following acute, 47 moderate, 16 and long-term changes in intracortical inhibition. 7
Our data, that is, changes in functional motor outcomes and intracortical inhibition, partly support previous findings in American football players who have received concussion injuries. 7,16,17 Of these three studies, only one 7 investigated a similar cohort of retired American football players who had sustained a concussion injury >30 years prior. We found, similar to the study by De Beaumont et al., 7 reduced movement performance, albeit in different motor tests. However, the present study found a decreased cSP duration and reduced SICI and LICI, whereas the investigation by De Beaumont et al. 7 found an increase in cSP. We are unsure why our findings differ, but speculate that differences may be attributed to several causes. First, there is the difference in the nature of the concussion received between the two sports. Limited studies on concussion impacts have shown that the majority of concussions (60%) in AF occurred in the temporoparietal region, 48 whereas the majority in American football (46%) were to the frontal area. 49 However, given the limited nature of both head impact data and TMS data in both football types, caution is required when interpreting the data. Second, as suggested by Demirtas-Tatlidede et al. 46 the differences probably reflect distinct aberrations following TBI. For example, lengthening in cSP has been presented by Chistyakov et al. 47 in moderate TBI at 130% aMT but not at lower stimulation intensities, whereas Bernabeu et al. 50 showed no change in cSP with severe TBI other than alterations in the MEP. De Beaumont et al. 16 demonstrated lengthened cSP correlated to the severity of the multiple concussions to those who had received a single concussion injury. Takeuchi et al. 51 showed reduced ipsilateral silent periods in TBI patients, but conversely to Chistyakov et al., 47 did not show differences in rMT. Collectively, these studies demonstrate the variability of measures following TBI that appear to be dependent upon the etiology and number of concussions, and the TMS protocols employed. We concur with Demirtas-Tatlidede et al. 46 that further investigations are required regarding intracortical inhibitory mechanisms in those who have sustained a TBI.
Several limitations to our study require acknowledgement. First, the definition of concussion, in order to recruit retired AF players, was reliant on the AFL classification of concussion, which requires a player to miss the following game. 15 Many players participating in the study at both levels of AF were not adequately assessed at the time of the concussion, as many did not have access to full-time medical personnel. Therefore, it was not possible for the retired players recruited to provide a full diagnostic report of their concussion, and we relied on self-reporting; which is not ideal. Second, we appreciate that we have used a cross-sectional design. As a result, we were not able to obtain measures of premorbid functioning in the football-playing groups. Future research should employ longitudinal designs that will inspire greater confidence regarding players' longer-term outcomes following multiple concussions. Finally, as posited by Kobayashi and Pascual-Leone, 52 TMS, which provides data on GABA-mediated pathways in the corticomotor system, can render useful information about the integrity of this pathway; however, TMS is not disease specific, and results should be interpreted in the context of other clinical data. Therefore, it would be remiss to reverse inference from a single time-point data measure in a limited sample of football players. 53 Longitudinal studies, and incorporation of other measures, for example advanced neuroimaging techniques such as GABA magnetic resonance spectroscopy, will be valuable in verifying the changes in intracortical inhibition observed in this study.
Conclusion
In conclusion, this study has shown, for the first time, that repeat concussion injuries in AF players manifest as changes in fine dexterity, visuomotor reaction time, and intracortical inhibition, quantified by TMS. Moreover, these changes were observed in both retired elite and amateur players, showing that repeated concussions have long-term outcomes regardless of the level or standard of competition that a player participates in.
Footnotes
Acknowledgments
The authors thank the reviewers for their insightful and constructive comments, and gratefully acknowledge Charlotte Davies for assistance with data collection, and Matthew Gray and Peter Jess from Smart Head Play for assistance with participant recruitment.
Author Disclosure Statement
Jerome Maller and Paul Fitzgerald are supported by NHMRC fellowships. P.B.F. has received equipment for research from Brainsway, Ltd., Cervel Neurotech, MagVenture A/S, and Medtronic Ltd., and has received funding for research from Cervel Neurotech. The other authors have nothing to disclose.