
Abstract
Sports-related concussion is a major public health problem in the United States and yet its biomechanical mechanisms remain unclear. In vitro studies demonstrate axonal elongation as a potential injury mechanism; however, current response-based injury predictors (e.g., maximum principal strain,
Introduction
S
On-field brain injury studies measuring head impact exposure (frequency, location, and kinematics of head impact) using the Head Impact Telemetry (HIT) System (Simbex, Lebanon NH) have provided important insight on head impact characteristics in contact sports. 2 –8 Kinematic measures such as peak linear and rotational acceleration alone, however, lack specificity in identifying athletes with diagnosed concussions, and no consensus has been reached on an injury tolerance threshold at the kinematics level. 2,5,6,9 In parallel, studies of neuronal and cellular responses to deformation at the microscale demonstrate that mechanical forces in the brain during traumatic brain injury (TBI) are capable of triggering both acute and chronic changes in function. 10
Injury thresholds for stretching have also been established in terms of magnitudes of axonal strain and/or strain rate required for nerve fibers, single axons, neural cell cultures, and organotypic brain slice cultures. 11 These in vivo animal and in vitro studies indicate the mechanical conditions under which functional deficits appear or cell death results in the brain, and provide a potential microstructural injury mechanism by stretching white matter (WM) axons to inform how TBI occurs at the cellular level.
To bridge the gap between on-field, kinematics-based brain injury research and the microscale studies that define tissue-level injury thresholds, computational finite element (FE) models of the human head are playing an increasingly important role in understanding how energy from an external head impact is converted into brain mechanical responses sufficient to cause injury. Several research groups have attempted to establish a concussion threshold based on model-estimated regional brain mechanical responses from analyses of reconstructed National Football League (NFL) football impacts, 12 –14 pedestrian and motorcycle accidents, 14,15 and instrumented helmets from collegiate football players. 16
Our recent work evaluating model-estimated strain and strain rate in the corpus callosum for a group of athletes with a diagnosis of concussion based on on-field head impacts measured with the HIT system also showed promise to relate regional brain responses directly to longitudinal changes in neuroimaging parameters. 17
Although in vitro investigations suggest an important axonal orientation dependency, most of these studies use isotropic variables such as the maximum principal strain (
There has been growing interest in incorporating WM microstructural orientation into injury analysis. For example, Cloots and colleagues 18 demonstrated the importance of axonal orientation and anisotropy using a two-dimensional (2D) plane strain FE model at the cellular level, and later tried to relate tissue-level mechanical loads to cellular-level brain injury through a “critical volume element” by simulating a reconstructed NFL concussion case with a three-dimensional (3D) head model. 19 Chatelin and associates 20 developed an efficient post-processing scheme to directly couple FE simulation outcome with axonal structural anisotropy determined from a diffusion tensor imaging (DTI) atlas to localize regions with potential diffuse axonal injury (DAI) and illustrated the technique by simulating two real-world head injury cases.
Kraft and coworkers 21 related strains along WM axonal bundles to cellular death for one person using a simulated head impact through a mathematical function based on in vitro injury findings to investigate the temporal evolution of damaged fiber tracts. Wright and Ramesh 22 also developed an axonal strain injury criterion by estimating nominal stretches along WM fiber directions determined from DTI, and later used it to study a reconstructed professional ice-hockey concussion case. 23 Their results indicate that the degree of WM injury predicted is highly dependent on axonal orientation. Their study, however, utilized 2D instead of 3D FE models based on MR images of a person and a co-registered WM atlas from a different person to identify potential DAI locations. In addition, no model validation was performed against relative brain-skull displacement data measured from cadaveric head impacts that are most relevant to the strain evaluations in their work.
To date, there have been no reports on the significance of WM fiber orientation in strain measures on a sizeable group of contact sports athletes with a clinical diagnosis of concussion. The objectives of this study, therefore, are (1) to evaluate strain along WM fibers (i.e., fiber strain,
Because strains are strongly model-dependent, 24 we also provide important details regarding development and validation of the Dartmouth Head Injury Model (DHIM) as well as techniques to generate geometrically accurate subject-specific head FE models in the Methods section, which are important components of this study.
Methods
This work is part of a larger effort to investigate the biomechanical basis of mild TBI (mTBI) in collegiate and high school contact sport athletes. Data from varsity athletes on the Dartmouth College football team and men's and women's ice hockey teams, and the Hanover High School football team were collected between 2007 and 2011 as reported previously. 17 All college participants provided written informed consent; high school athletes gave their assent, and written consent forms were signed by their parents/guardians. Protocol for data collection was approved by the Dartmouth College Committee for the Protection of Human Subjects.
Head impact kinematics and clinical diagnosis
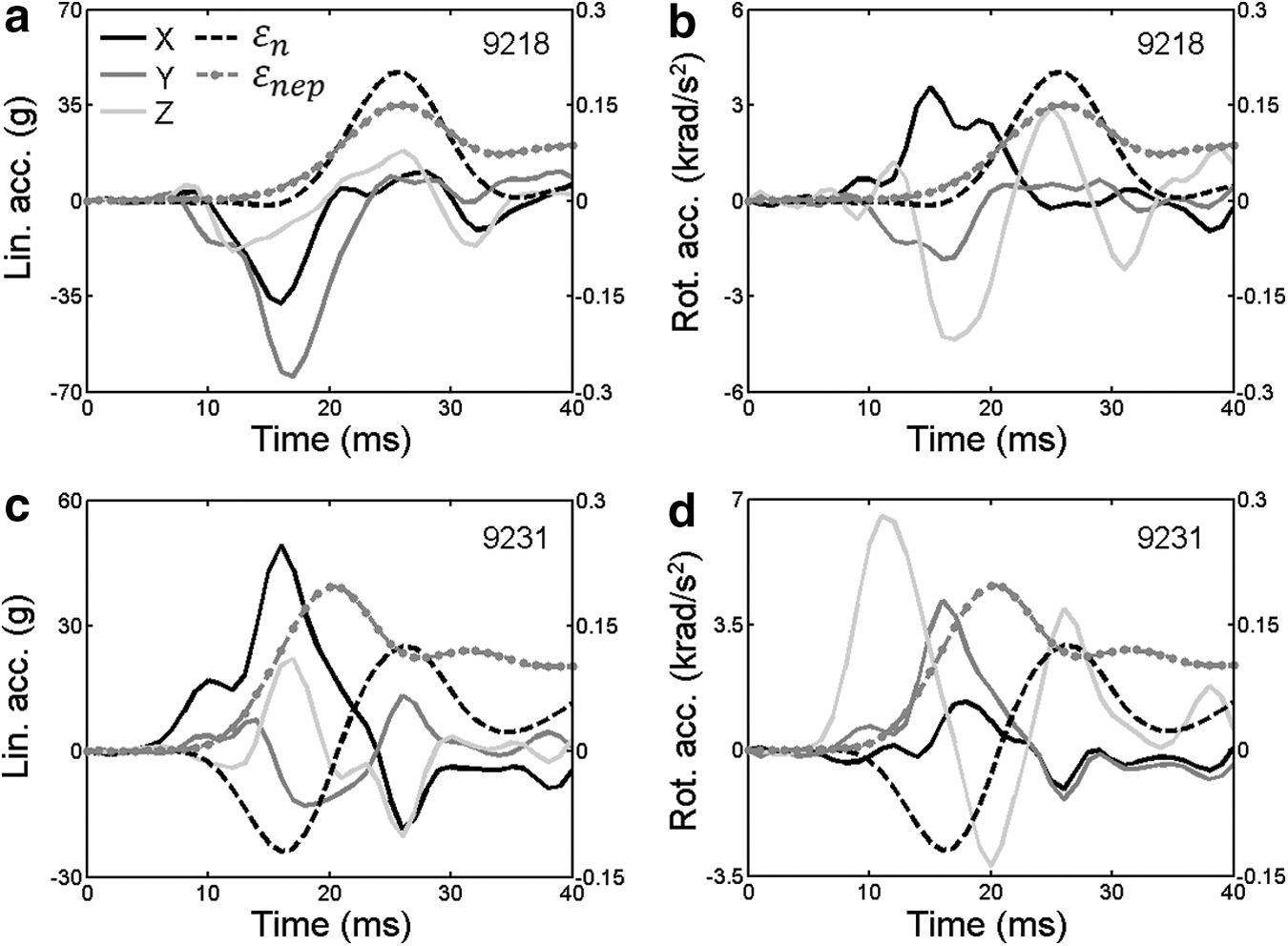
Methods for recording head impacts and associating the kinematic data with diagnosed concussions have been reported earlier.,17,25 In short, football and hockey players wore helmets instrumented with the HIT System to record in vivo accelerations after head impact (a 40 msec time-varying acceleration data recorded at 1 kHz). The details of the HIT System and its validation have been published previously. 7,26 –28 Accelerometer data recorded from each impact were extracted from the HIT System database with a custom software application (Matlab R2013a) and processed using an optimization algorithm to solve for the linear and rotational accelerations at the head center of gravity (CG). 29 The resulting accelerations were used as model inputs. For each athlete, contributions of linear and rotational accelerations at the head CG in the X, Y, and Z directions defined in the head coordinate system (Fig. 1) at the time of peak resultant magnitudes are summarized in Table 1.
(
Lin. acc., linear acceleration; rot. acc., rotational acceleration; Mag., magnitude; FT, football; CL, college; HC, ice-hockey; HS, high school.
All athletes were male except for 3871. 17
According to our previous work, 17 concussion was defined as an alteration in mental status reported or observed by the player or team's medical staff in this study. A certified athletic trainer or team physician made the diagnosis and treated all instances of concussion at their professional discretion. After concussion diagnosis, each team's medical staff provided the date and suspected time of injury as well as the approximate time of diagnosis. Anecdotal observations of the events surrounding injury (e.g., description of the impact, method of identifying the injury, and comments from coaches, trainers, teammates, or parents) were also provided. An impact recorded by the HIT System was retrospectively associated with each diagnosed concussion by cross-referencing all the information with the impact time stamp on the day of injury.
To minimize influence from any potential errors in measured impacts, each impact used for model simulation has been manually reviewed and found to be free of typical signs of elevated error (i.e., accelerometer signal noise, signal artifact from electromechanical malfunction, and rapid acceleration/deceleration indicating loss of head contact). The processed acceleration data were further verified against descriptions of general severity and location provided by sideline personnel as an additional qualitative check of accuracy. A total of 11 persons with concussion were evaluated.
Neuroimaging acquisition
For all athletes, high-resolution T1-weighted magnetic resonance imaging (MRI) and diffusion tensor imaging (DTI) were acquired in the Dartmouth Advanced Imaging Center. The brain and its anatomical regions (e.g., white matter, corpus callosum) were automatically segmented from the high-resolution MRI (1 mm×1 mm×1 mm; image dimension of 256×256×256) using FreeSurfer (Version 5.1). DTI were acquired using 46 diffusion directions (collected with b=1000 s/mm2, NEX=1) plus an additional volume without diffusion gradients (b=0) serving as an anatomical reference map. All DTI had an image dimension of 128×128×65 with a voxel resolution of 2 mm×2 mm×2 mm. Diffusion tensors, eigenvectors, and scalar diffusion parameters were computed using ExploreDTI with corrections for eddy currents and motion before fitting a tensor model. 30
DHIM
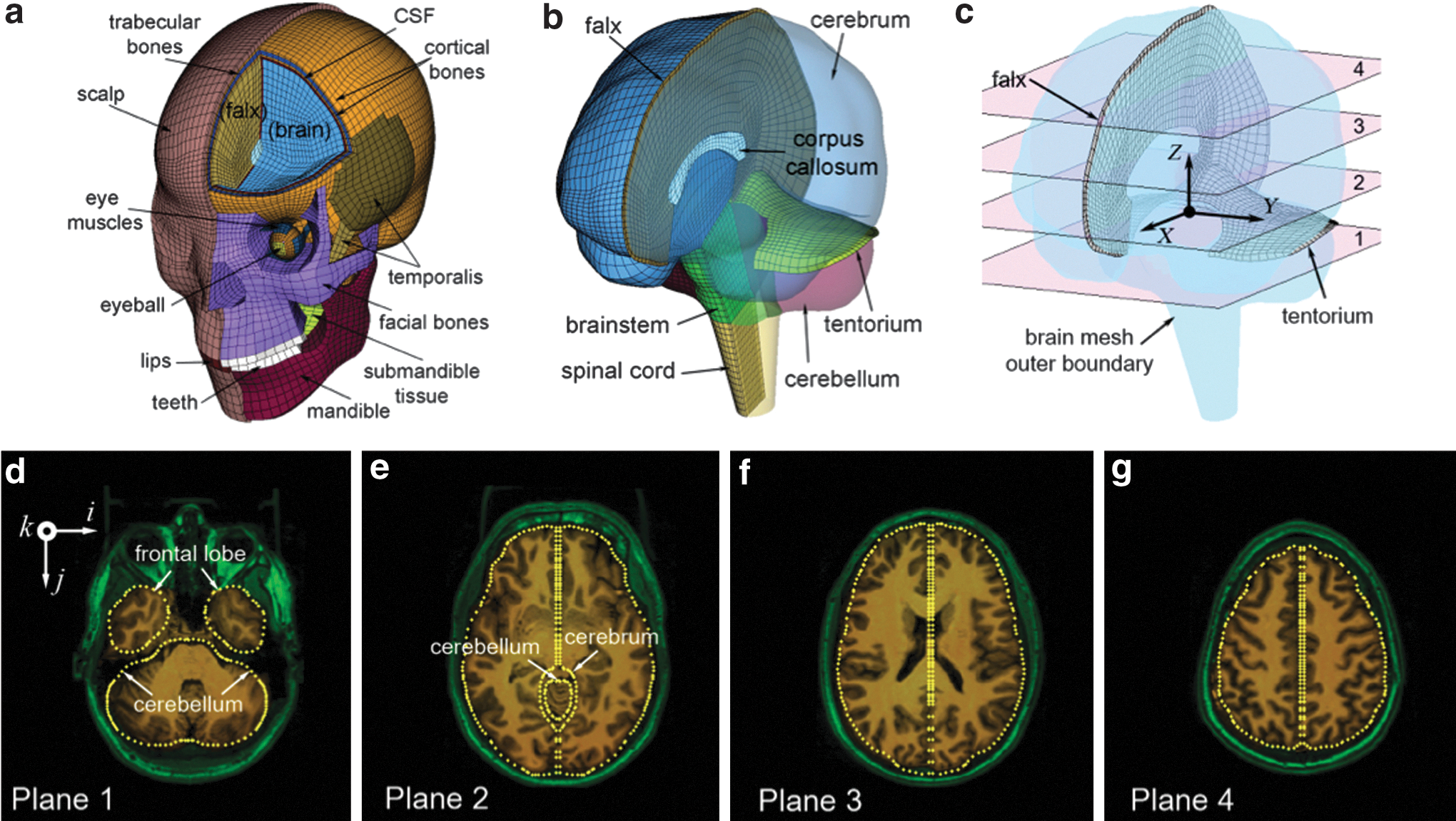
The DHIM was created based on a template high-resolution T1-weighted MRI (MRItemp) of a person selected from the group of concussed athletes whose head was positioned neutrally without tilting in the MRI. In addition to the automatically segmented brain, the falx and tentorium were manually delineated. The resulting anatomical geometries were imported into Geomagic (Geomagic, Inc., Research Triangle Park, NC) for parameterization and further into TrueGrid (version 2.3.4; XYZ Scientific Application, Inc., Livermore, CA) for meshing. Multiblocks for the cerebrum, cerebellum, brainstem, falx, and tentorium were created. The brain mesh outer surface served as a baseline to define elements for the cerebrospinal fluid (CSF) and skull using Hypermesh (Altair Engineering, Inc., Troy, MI). Membrane structures of the pia and shell structures of the dura surrounding the CSF were also generated.
To improve biofidelity in the basal region, the segmented brainstem was extended along the neural axis to include part of the spinal cord that was not captured in MRI. An elastic membrane was also included at the base to simulate the loading environment for brainstem moving through the foramen magnum. 16 In addition, scalp and face including the eyes, facial bones, and other components were created based on a template head model. 31 All solid (surface) parts were represented by hexahedral (quadrilateral) elements. A reduced integration with hourglass control was used (hourglass energy typically 5–8% of internal energy). A soft CSF layer existed between the brain surface and all of its surrounding structures to allow brain interfacial sliding through CSF deformation (nodes between all anatomical interfaces were shared). 16
The DHIM model components and associated material properties used in this study are summarized in Tables 2 and 3. In total, the model contains 101,420 nodes and 115,228 elements with a combined mass of 4.562 kg for the head, and 56,632 nodes and 55,062 elements with a combined mass of 1.579 kg for the brain (1.558 kg without the spinal cord). The average element size for the whole head and the brain is 3.2±0.94 mm and 3.3±0.79 mm, respectively.
ρ, density; E, Young modulus; υ, Poisson ratio; K, bulk modulus.
References for the material properties are also provided.
Abaqus, Dassault Systèmes, France.
Because no consensus has been reached on how best to characterize the brain material properties and experimental observations conflict on the relative stiffness of grey and white matter,
32
we have chosen to model the entire brain as a homogenous medium without incorporating the possible differences in grey and white matter material properties or material property anisotropy based on WM fibers (as opposed to the WM microstructural anisotropy for strain estimation, which is the focus of this study). An isotropic hyperelastic material model of a second order Ogden form identical to the “average model” in Kleiven
13
was chosen to simulate brain responses with the following strain energy function:
where
where gi and τi are material constants (Table 3). These material property values were derived via fitting using discrete spectrum approximation to include nonlinear elasticity. 33 The shear relaxation moduli were based on experimental values and were scaled twice based on alterations in brain tissue mechanical properties from postmortem proteolysis and preconditioning, 34,35 as described previously. 13
A summary of the mesh element qualities based on a variety of criteria is listed in Table 4, 41 suggesting a satisfactory mesh for the DHIM. The final mesh of the DHIM is shown in Figure 1 with mesh-MRI alignment to illustrate its geometrical accuracy. The average distance from the DHIM brain mesh outer boundary nodes to the brain surface segmented from MRI was 1.5±0.8 mm.
Deg, degree.
Validation of the DHIM
The DHIM was validated against relative brain-skull displacements measured in three cadaveric tests representing a frontal (C383-T1), an occipital (C755-T2), and a parietal (C393-T4) impact. 42,43 The recorded head acceleration traces were used as biomechanical input to the DHIM (scaled to match the reported head dimensions). Model-estimated relative brain-skull trajectories at selected neutral density target (NDT) locations were compared with those measured.
A correlation score (CS) based on Normalized Integral Square Error (NISE) was adopted to objectively assess the quality of model estimation. 44 The technical details have previously been published to validate the THUMS (Total Human Model for Safety). 45 Briefly, the NISE method evaluates the error measurement (EM) between a pair of time history curves in terms of phase (N-phase), amplitude (N-amp) and shape (N-shape). A corresponding CS limited to 0–100 was used to assess the level of their agreement 45 and was categorized into five classifications according to a biofidelity rating: 46
Excellent: 86≤CS≤100
Good: 65≤CS<86
Fair: 44≤CS<65
Marginal: 26≤CS<44
Unacceptable: 0≤CS<26
In addition, model responses were also compared with those from Kleiven 47 in terms of correlation coefficient for the frontal (C383-T1) and occipital (C755-T2) head impact cases.
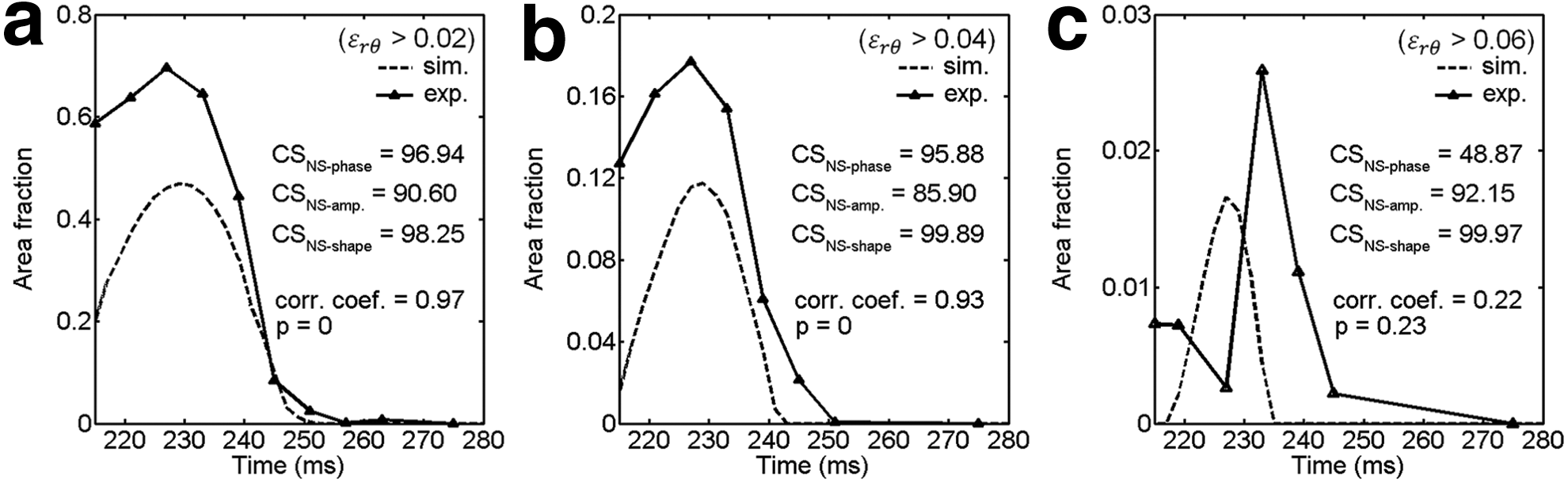
To assess the fidelity of DHIM in estimating brain strain responses in a live human (as opposed to displacement responses in cadavers), experimental data in a mild head rotational acceleration study were used for further validation. 48 A subject-specific head FE model corresponding to Subject 1 in Sabet and coworkers 48 was generated via MRI-based image registration and warping (see below) to simulate brain responses using the corresponding acceleration profile as model input. Area fractions of radial-circumferential strain above representative strain thresholds were computed, and correlation scores characterizing the level of agreement in phase, amplitude, and shape were analogously reported along with their correlation coefficients.
Subject-specific head FE models
Geometrically subject-specific FE models were necessary to relate to the corresponding neuroimaging. Because all athletes had high-resolution MRI, we used “mesh-matching” to generate subject-specific head models for the remaining athletes by warping the baseline DHIM via image registrations. 49 First, an affine registration was performed between MRItemp and each subject's own MRI (MRIsub), and the resulting transformation matrix was applied to the DHIM nodes. The affine registration accounts for translation, rotation, scaling, and shear between the two image volumes, and effectively compensates for differences in head position, orientation, and size.
To further improve the alignment, a B-spline nonrigid registration was used to provide additional deformation to apply to the transformed nodes. Because the resulting warped MRItemp will be spatially aligned with the MRIsub counterpart, the corresponding warped model will match the geometries defined in the MRIsub and can serve as a subject-specific head model.
These transformations mapped MRItemp to MRIsub in a subject's native MRI space. Because the head may be tilted during image acquisition, the image coordinates in MRIsub may be misaligned with that defined by the head anatomy (e.g., the i-axis in MRI may not be aligned with the head left-right direction; see Fig. 1 for illustrations), thereby precluding a direct application of head impact biomechanics (based on head anatomy) on the FE model. To rectify this, an additional rigid body registration was performed between MRIsub and MRItemp to transform the subject-specific head model into the DHIM space and adjust for head position and orientation.
Computation of the WM fiber strain
Abaqus/Explicit (Version 6.12) was used to simulate brain responses during head impact. The skull, scalp, and face were simplified as rigid bodies in this study because they do not influence brain mechanical responses when on-field acceleration is directly applied to the skull. 13,16 The typical run time for a 40 msec impact was ∼50 min on a multicore Linux cluster using 8 CPUs (Intel Xeon X5560, 2.80 GHz, 126 GB memory).
The
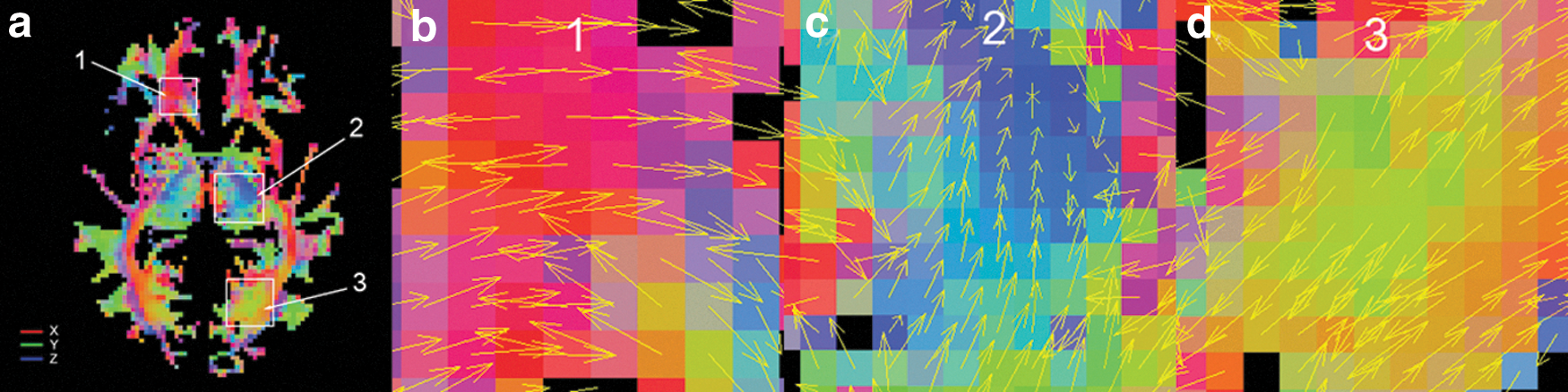
Color-coded white matter (WM) fiber orientation (
For each transformed voxel or sampling point originally in the DTI image space, a local coordinate system, xyz, was established with its origin identical to the transformed voxel location and the z-axis along the fiber orientation transformed from DTI image space into the coordinate system of the head FE model. The x- and y-axis were arbitrarily established, because they did not influence the strain component of interest. A spatial transformation from the global to the local coordinate systems,
The WM fiber strain or the stretch along the local z-axis was readily obtained:
Comparisons of
\documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\pagestyle{empty}\DeclareMathSizes {10} {9} {7} {6} \begin{document}$$\varepsilon_n$$ \end{document}
and
\documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\pagestyle{empty}\DeclareMathSizes {10} {9} {7} {6} \begin{document}$$\varepsilon_{ep}$$ \end{document}
The peak
Because regions exposed to high strains potentially indicate injury locations, it is important to compare the spatial distributions of regions with high strains determined by the two strain measures at each threshold, for which their Dice coefficient readily serves the purpose.
53
The Dice coefficient, d, is defined by the following equation for two regions, A and B:
where d ranges from 0 (no overlap) to 1 (fully overlapped, i.e., the two sets are identical).
Results
Validation of the DHIM
The CSs for the DHIM and THUMS were compared in Table 5 (except for the parietal impact, C393-T4, not reported for THUMS). Combining the frontal (C383-T1) and occipital (C755-T2) cases, the average CS was 83.37 and 85.52 for DHIM and THUMS, respectively. The average CS for DHIM was 83.74 for all three cases combined. The average correlation coefficient between DHIM-estimated responses and the measurements was 0.84 (range 0.57–0.98) and 0.73 (range 0.33–0.96) for the frontal and occipital impacts, respectively. By comparison, it was 0.63 (range 0.32–0.84) and 0.78 (range 0.31–0.97) for the two cases reported previously. 47 Model-estimated brain responses were also compared between the models and the measurements (Figs. 3 –5; results for the parietal impact only available for DHIM).

Comparison of model-estimated relative brain-skull displacements with those measured for selected neutral density target (NDT) locations (a1, a6, p1, and p6) in a frontal impact (C383-T1). DHIM, Dartmouth Head Injury Model; THUMS, Total Human Model for Safety.

Comparison of model-estimated relative brain-skull displacements with those measured for selected neutral density target (NDT) locations (a1, a5, p1, and p5) in an occipital impact (C755-T2). DHIM, Dartmouth Head Injury Model; THUMS, Total Human Model for Safety.
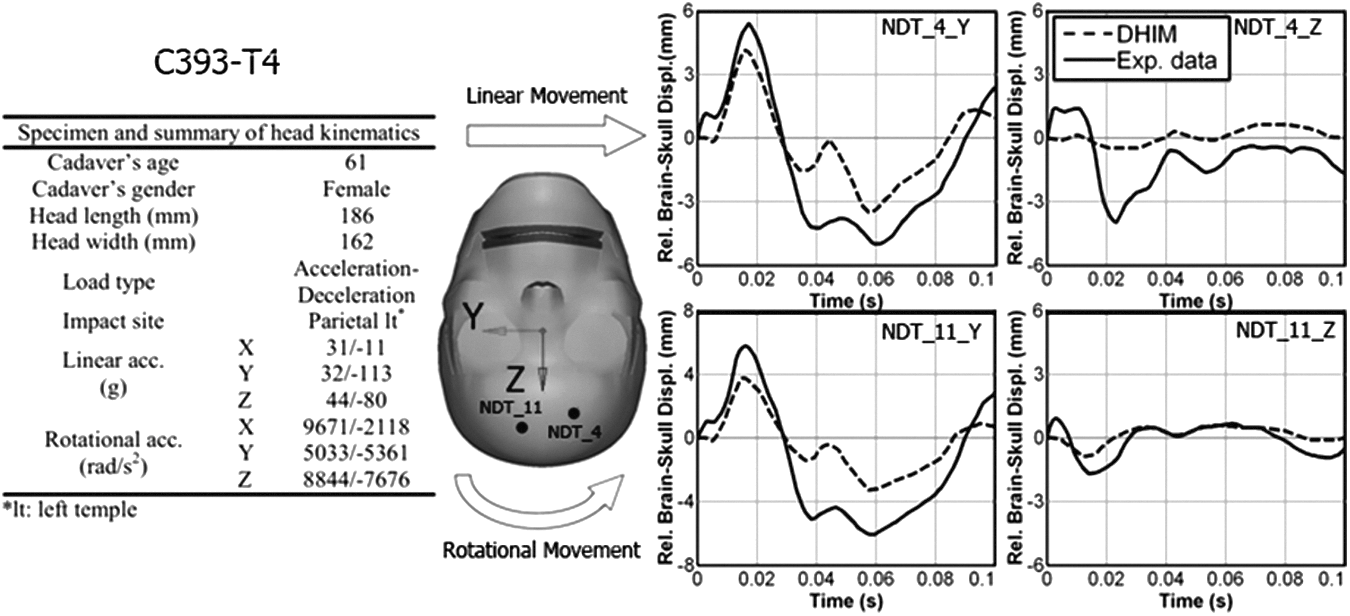
Comparison of the DHIM-estimated relative brain-skull displacements with those measured for selected neutral density target (NDT) locations (4 and 11) in a parietal impact (C394-T4). DHIM, Dartmouth Head Injury Model; THUMS, Total Human Model for Safety.
DHIM, Dartmouth Head Injury Model; THUMS, Total Human Model for Safety; NDT, neutral density target.
The area fractions of radial-circumferential strain exceeding three threshold levels obtained from the simulation were compared with the experimental counterparts on an axial plane 2 cm above the reference plane for the selected subject (Fig. 6). 48 The average CS was 89.83 and the average correlation coefficient was 0.71.
Area fractions of radial-circumferential strain (
Accuracy of subject-specific head models
Similarly, mesh accuracy for the subject-specific models was measured by the average distances from the brain mesh outer boundary nodes relative to the segmented brain surface generated from MRIsub. For all the 11 head models (including the DHIM), the average distance was 2.0±0.9 mm. Brain mesh boundary intersection points on a representative axial image plane are shown for four subjects (Fig. 7), demonstrating good alignment of brain anatomies between FE models and MRI.

Brain mesh outer boundary intersection points overlaid on a representative axial magnetic resonance imaging (MRI) for four subjects (
Comparison of
\documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\pagestyle{empty}\DeclareMathSizes {10} {9} {7} {6} \begin{document}$$\varepsilon_n^p$$ \end{document}
and
\documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\pagestyle{empty}\DeclareMathSizes {10} {9} {7} {6} \begin{document}$$\varepsilon_{ep}^p$$ \end{document}
For each subject, the

Comparisons of
The time history curves of
Spatially averaged (for the entire white matter), time-varying
For the thresholds selected, the WM volume fractions for
d, Dice coefficient.
Average values (±standard deviation) for all athletes are also shown.
Discussion
Based on 11 athletes with a clinical diagnosis of concussion, we found significant correlations between the WM volume fractions determined by the fiber strain (
These observations were similar to those previously reported that used 2D FE models to simulate one reconstructed concussion case.
23
The Dice coefficients for WM regions identified by the two strain measures ranged from 0.13 (
More importantly, the spatial distribution and extent of WM volume fraction on average based on
Apparently, accuracy in model simulation is critical. To ensure sufficient fidelity in DHIM, we have presented important details on methods to create and validate the model, to efficiently generate multiple subject-specific head models, and to incorporate WM fiber orientations derived from neuroimaging into model-estimated mechanical responses. The mesh quality of the DHIM was sufficiently high based on a variety of mesh element quality measures (Table 5), with the majority of distorted elements in the brainstem far away from the WM in the cerebrum. Its geometrical accuracy in terms of average node-to-surface distance between brain mesh outer boundary nodes and the segmented brain surface from MRI was 1.5 mm, comparable to the diagonal length of a voxel (1.73 mm).
Because the subject-specific head models were generated via “mesh-matching” that maintains the same mesh topology, nearly identical mesh element qualities were retained. The average node-to-surface distance for all subject-specific head models was 2.0 mm, slightly degraded from that of the DHIM likely because of residual errors in image registrations at the boundary. The millimeter node-to-surface error, however, was notably larger than that of our previous head model where submillimeter accuracy was obtained. 56 This was because the segmented brain surface was not directly used for block projection in this study but was parameterized to generate geometrical entities to aid the meshing instead.
Besides geometrical biofidelity, the DHIM was also successfully validated. Compared with relative brain-skull displacement data measured from three representative cadaveric head impacts (frontal, occipital, and parietal), validation of DHIM was categorized as “good” or nearly “excellent” according to CS and a fidelity rating previously adopted (average score of 83.74; cutoff CS for “excellent” validation is 86), which was comparable to the validation performance of THUMS (average score of 85.52).
On average, both DHIM and THUMS had an “excellent” validation in phase and a “good” validation in shape, while they had “good” and “excellent” validation in amplitude, respectively. Although THUMS had a slightly higher CS overall, the CS in one location was “unacceptable” (CSN-phase of 0 for NDT_a1_z in C755-T2; Table 5 and Fig. 4), which did not occur to DHIM (lowest CS of 28.12 in shape for one location in C393-T4; Table 5). In addition, validation performance of DHIM was comparable with that reported in Kleiven (2006) for two cases in terms of average correlation coefficient (0.84 and 0.73 vs. 0.63 and 0.78 for the frontal and occipital impact, respectively). 47
An overall “excellent” validation performance (average CS of 89.83; overall average correlation coefficient of 0.71, although with much higher [>0.93] and significant coefficients at the two lower threshold levels; Fig. 6) was also achieved when simulating brain strain responses in a live human brain compared with the measured counterparts in a mild head rotational acceleration experiment (∼250–300 rad/s2). 48 Validating each subject-specific model was not necessary because each model would be scaled to match the reported cadaveric or live human head dimension and would result in nearly the same response relative to the scaled DHIM, because of their identical mesh topologies, material properties and loading conditions used.
Regardless, the “good” to “excellent” validation of DHIM for a range of resultant rotational acceleration magnitudes (∼250–300 rad/s2 for a live volunteer, ∼1.9–2.3 krad/s2 for cadaveric tests C755-T2 and C383-T1, and ∼11.9 krad/s2 for C393-T4, respectively) and the high mesh quality and geometrical accuracy suggest sufficient fidelity in model simulation as well as accuracy in aligning simulation results with the corresponding neuroimaging.
While the group-wise results based on WM
Previous laboratory tests have shown that measures of impact location and peak and resultant accelerations are typically robust for a distribution of impacts across a range of conditions 7,27,28,57,58 ; however, discrepancy for each impact could be higher because of a number of environmental and individual factors (e.g., head geometry, neck response, helmet fitting, etc.) that are typically unknown or cannot be readily obtained on the field. 28 Regardless, additional precautions have been taken to minimize influence from potential errors in impact measurements, and it is unlikely that these errors would significantly affect the outcome on a group-basis in this study.
Nevertheless, because the WM volume fractions for
The WM volume fraction based on
Second, although material properties of the brain strongly influence model estimation, there is no consensus on what values to use, and there is wide variability even with respect to the grey matter vs. WM interregional relative stiffness. 32 Consequently, studies have used very different material properties of the brain (e.g., viscoelastic vs. hyperelastic 12,13,16,17,47 ; with either grey matter up to 43% stiffer than WM, 59 or WM 25% stiffer than grey matter, 60 by the same research group). While brain material properties may be age-dependent, 61 no data corresponding to the younger end of our participants (15–23 years old) exist. Because of these inconsistencies, it is perhaps difficult to assess the utility of incorporating material property anisotropy based on fibers derived from DTI, although a recent study does suggest its significance. 62 Given these considerations, we have chosen to model the brain as a homogeneous isotropic medium in this study.
Nevertheless, we have further conducted a simple parametric study to evaluate the sensitivity of the extent of WM regions exposed to high strains based on the two measures using case 3879 (selected because the WM volume fraction of 2.6% at
Finally, all athletes included in this study experienced multiple head impacts but only a single impact before the diagnosed concussion was modeled, which is a critical limitation not only for this study but also for current FE model-based brain injury studies in general that focus on single head impacts and do not consider the cumulative effects of repetitive head blows. In addition, there was a wide range of impact magnitudes (range 30.7–111.6 g and 1307–6560 rad/s2 in peak linear and rotational acceleration magnitude, respectively; Table 1) in a small sample size (although notably larger than that in previous studies evaluating WM
The unmodeled exposure to repetitive subconcussive head impacts could also be an important contributor to an athlete's clinical presentation, 8,9,63,64 which could be especially true for the athletes with very low impact severities (e.g., cases 3871 and 3911; Table 1), and will be the focus of future investigations when simulation of brain responses to longitudinal head impacts becomes feasible.
On the other hand, growing evidence indicates that athletes sustaining repetitive subconcussive impacts without a clinical diagnosis of concussion also experience measurable neurological alterations present on DTI (1–1.5% WM voxels with significant longitudinal changes) or fMRI. 8,55,64 These findings suggest that a definitive clinical diagnosis of concussion (i.e., via an instrument) may become irrelevant when region-specific responses are to be directly correlated with corresponding changes in neuroimaging. 17
Regardless of all these practical challenges, however, the consistency found between our modeling results of
There are a few other limitations to note as well. We have only evaluated strain measures to indicate the likelihood of brain injury but did not evaluate strain rate, stress, or pressure responses that have also been hypothesized to be potential injury predictors. 12,13 The representative strain thresholds were based on morphological injury and electrophysiological impairment found in an animal study, which may not directly correspond to concussive symptoms in human athletes. We did not evaluate thresholds established from other real-world injury analyses (e.g., 0.21 in the corpus callosum or 0.26 in the grey matter, or 0.19 in grey matter), 12,13 although these values were within the range evaluated, and we anticipate similar results to occur.
Given the substantial differences in
In addition, evaluating mechanical responses along prominent fiber tracts could also provide an assessment of the likelihood of DAI for functionally important neural pathways that can be directly related to specific clinical symptoms, which are not available with the voxel-based approach. These investigations will be the subjects of future publications.
Conclusion
We have evaluated and compared WM fiber strain and maximum principal strain on a group of 11 athletes with concussion in contact sports. Substantial differences exist between the two strain measures because of WM anisotropy in fiber orientation in both distribution (Dice coefficient of 0.13–0.33) and extent (∼5–10-fold differences) of WM regions estimated to be exposed to high strains using a range of axonal injury thresholds derived from an in vivo animal study. The WM regions with high fiber strains appear to be isolated and heterogeneous, and seem to occur mainly in the peripheral subcortical area and near grey matter/WM interfaces.
To ensure sufficient fidelity in model simulation, we verified that all subject-specific head FE models were geometrically accurate with a node-to-surface distance error of 1.5–2.0 mm, comparable to the diagonal length of an MRI voxel. Validation of the DHIM against relative brain-skull displacements was “good” or nearly “excellent,” which was comparable to the previously validated THUMS and that in Kleiven. 45,47
An “excellent” validation was also achieved when simulating brain strain responses in a live human volunteer. 48 With the optimal injury threshold, the average group-wise WM volume fraction exposed to high fiber strains for all subjects was 3.2±3.6%, similar to the percentage of WM voxels with significant longitudinal changes in DTI parameters for one athlete with concussion in a separate study (3.2% and 3.44% of WM voxels for FA and MD, respectively). 55
These efforts and results set the stage for future investigations as to whether incorporating WM fiber orientation in brain mechanical response variables improves the sensitivity and specificity in assessing the risk of concussion and in discriminating between injured and uninjured athletes in contact sports.
Footnotes
Acknowledgments
This work was sponsored, in part, by the NIH grant R21 NS078607 and the National Operating Committee on Standards for Athletic Equipment (NOCSAE 04-07 & SAC-1). Funding for the head impact biomechanical data collection and neuroimaging that supported this work included the NIH grants R01NS055020, R01HD048638, CDC R01/CE001254, and NOCSAE grant 04-07 & SAC-1, and are acknowledged. The authors would also like to thank Dr. Robert M. Roth in the Brain Imaging Laboratory at the Geisel School of Medicine at Dartmouth College for assistance with image segmentation in MRI, and Drs. Philip V. Bayly and Yuan Feng at Washington University in St. Louis for providing data needed for DHIM validation.
Author Disclosure Statement
Richard M. Greenwald, Jonathan G. Beckwith, and Simbex have a financial interest in the instruments (HIT System, Sideline Response System (Riddell, Inc)) that were used to collect data used in this study. The remaining authors have no financial interests associated with this study.