
Abstract
Patients with traumatic extracranial cerebrovascular injury (TCVI) comprise about 1% of all blunt trauma admissions according to numerous single-center studies. However, previous studies have used aggressive screening protocols; these studies may not reflect common practice and the overall incidence of TCVI. The annual incidence of the diagnosis of TCVI from 2003 to 2010 was estimated using the Nationwide Inpatient Sample (NIS). For comparison, a systematic review of previous studies of the incidence of the diagnosis of TCVI was conducted. The estimated total number of admissions with TCVI ranged from 1283 to 2652; these admissions represented 0.46–0.95% of all blunt trauma admissions. There was a significant increase in the incidence of TCVI during the study period. A total of 49 studies of TCVI reported incidences of diagnosis ranging from 0.03% to 4.8%. In conclusion, the annual nationwide incidence of the diagnosis of TCVI is increasing. Although NIS incidences of the diagnosis of TCVI are at the low end of the range of previous reports, the increasing incidence in the NIS data likely reflects increasing use of aggressive screening protocols.
Introduction
B
The purpose of this study was to determine the incidence of the diagnosis of TCVI in the United States, using the Nationwide Inpatient Sample (NIS) for the years 2003–2010. The NIS is the largest all-payer hospital inpatient database in the United States. It contains data from a 20% stratified sample of nonfederal United States hospitals, representing ∼8,000,000 hospital admissions each year. For comparison, a review of other relevant studies of the incidence of the diagnosis of TCVI was also undertaken.
Methods
Data source
The Nationwide Inpatient Sample (NIS) databases for the years 2003 through 2010 were used to produce estimates of national traumatic extracranial vascular diagnoses in the United States. NIS is the largest all-payer inpatient database developed as part of Healthcare Cost and Utilization Project (HCUP) by the Agency for Health Care Research and Quality (ARHQ). This project was approved by the Institutional Review Board.
Study population
Extracranial blunt TCVI was defined as a hospital admission with at least one extracranial vascular diagnosis (EVD) and a documented external cause of non-penetrating injury (ECOI) in the NIS database. International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnosis codes used to identify EVDs with or without prior history of trauma are listed in Table 1. These codes were used to scan through the 15 diagnosis positions in each year database for EVD. Although it is possible to have more than one EVD per patient, only one diagnosis event was considered in the analysis. To identify the trauma cases, we searched the NIS databases using HCUP Clinical Classification Software (CCS) for ICD-9-CM E codes (Table 2). The CCS E codes collapse ICD-9-CM codes for external cause of injury into smaller clinically meaningful categories. Of the four positions for ECOI, only the first listed external cause of injury was employed in the identification and classification of the trauma cases. The incidence of TCVI was calculated by dividing the frequencies of TCVI by all selected injuries.
Statistical analysis
The NIS databases were analyzed using SAS 9.2 statistical software (SAS Institute, Cary, NC) for the 8 year study period. National estimates of the diagnosis of TEVD in the United States were obtained by PROC SURVEYMEANS and PROC SURVEYFREQ procedures in the SAS statistical package. These procedures take into consideration the weighting, clustering, and stratification involved in the NIS sampling technique. Changes in incidence rates over time were assessed with a Cochran–Armitage trend test.
Literature review
The PubMed database was searched up to December, 2013. The following text words were used:
Results
NIS data
Total estimated numbers of blunt trauma admissions and blunt trauma admissions with TCVI are listed in Table 3 and graphed in Figure 1. Although the number of admissions for blunt trauma did not change markedly, hospitalizations for TCVI increased significantly from 1308 in 2003 to 2652 in 2010 (97.3%, p<0.001). The incidence rate rose from 0.46% in 2003 to 0.95% in 2010. Of the mechanisms of injury, motor vehicle traffic (MVT) was the most common, responsible for 59.3–74.7% of TCVI admissions (Table 1). The next most common mechanisms were falls from any height (8.6–15.5%), motorcycle crashes (6.5–15.3%), pedestrians being struck (4.2–8.8%), and assault with an object (1.9–4.9%). Relatively uncommon were bicycle accidents (1.1–3.5%) and assault with a vehicle (0–0.4%).
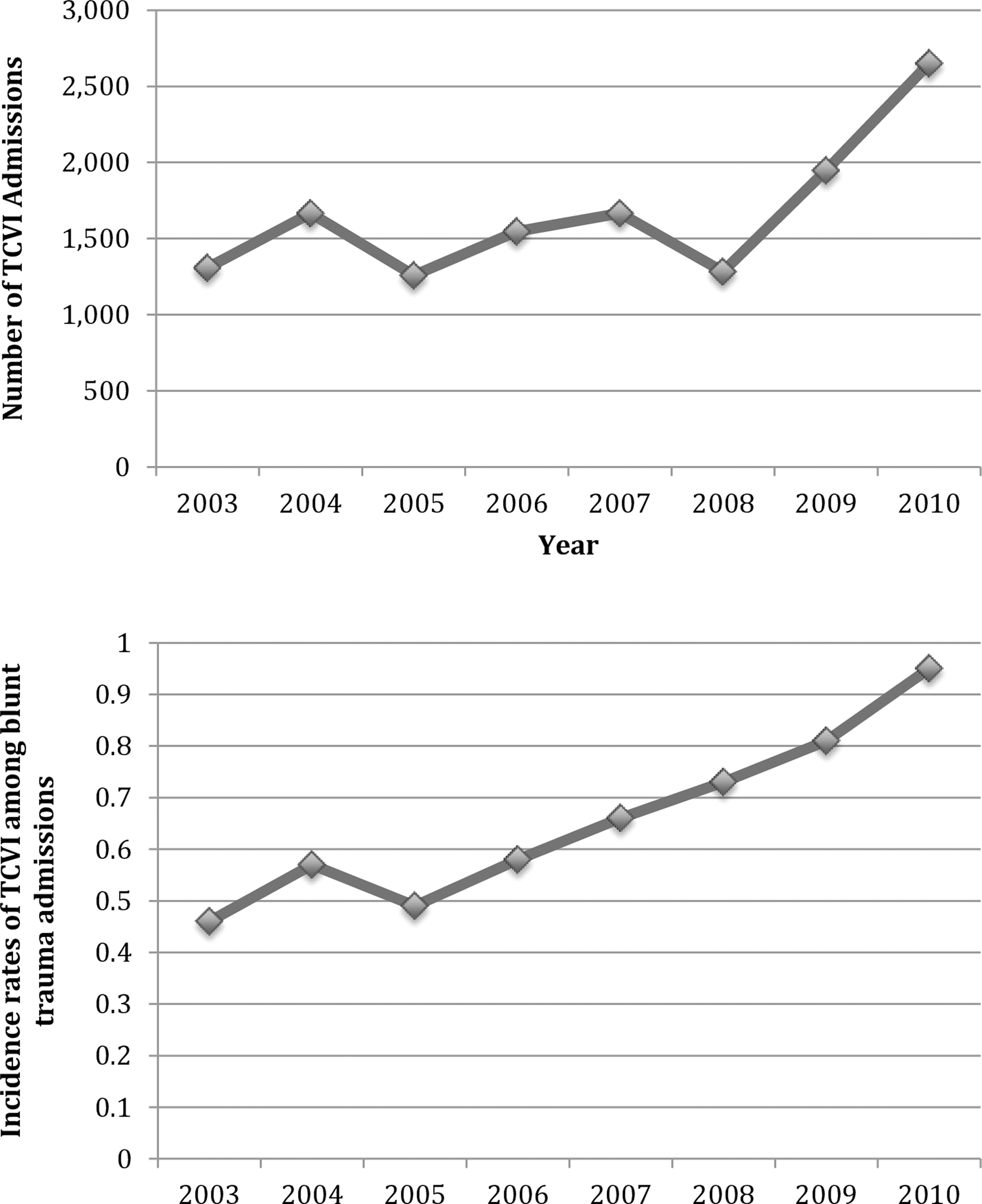
Numbers and incidences of traumatic cerebrovascular injury admissions among blunt trauma admissions.
Cochran-Armitage Trend test comparing blunt injuries with and without TCVI.
Healthcare Cost and Utilization Project (HCUP) privacy protection policy prohibits reporting of data on groups of patients ≤10 in number.
NR, not reported.
Other studies reporting on the incidence of TCVI
A search of the literature produced 49 relevant studies, from 1990 to 2013 (Table 4). A total of 27 studies reported on the incidence of both carotid artery and vertebral artery injuries, 1,3 –6,8,11 –13,15,16,18 –33 17 reported on carotid injuries only, 10, 34 –49 and 5 reported on vertebral artery injuries only. 50 –54 Some of these reports were from the same center during the same period, and, therefore, some of the samples may have overlapped. For the studies including both carotid and vertebral artery injuries, the incidences of TCVI diagnoses among all blunt trauma admissions ranged from 0.03% to 4.8%. No trend in incidences was observed over the time period of the studies. The most common causes of injury were motor vehicle crashes and other forms of road trauma (50–89%). Other common causes of injury were falls (6–18%) and assault (2–21%). Male gender (57–79%) was more common than female gender in most studies. Most patients were in the fourth or fifth decade of life. Only three studies including both carotid and vertebral artery injuries included data on ethnicity; all four found that that Caucasians were the most common ethnic group. One study found Hispanics to be the next most common ethnic group, 25 whereas the other two found African Americans to be the second most common ethnic group. 5,30
CTA, computed tomographic angiography; MVC, motor vehicle crash; MCC. motorcycle crash.
Discussion
This study found that the total annual estimated number of hospital admissions with TCVI as a diagnosis ranged from 1308 to 2652 during the years 2003–2010. The population of the United States was estimated to be 308,745,538 in 2010; 55 with 2652 estimated TCVI admissions in that year, the incidence of TCVI for 2010 was 0.86 per 100,000 population. For comparison, the incidence of hospitalization for traumatic brain injury is ∼79.0 per 100,000 population. 56
This study found an overall incidence of the diagnosis of TCVI among all blunt trauma admissions of 0.46–0.95%. These results are at the lower end of the range of reported incidences of carotid and vertebral artery TCVI in the other studies found in the literature review, which ranged from 0.03% to 4.8%. There are several possible explanations for this. First, most of the centers in the other studies employed comprehensive screening protocols with CTA. That is, all blunt trauma patients with risk factors for TCVI, such as cervical spine fractures and severe brain injuries, had neck CTAs to investigate for TCVI. Many of the centers included in the NIS database likely did not use CTA screening protocols during the study period. Second, most of the other studies were from level I trauma centers, and these centers are likely to manage a higher concentration of patients with polytrauma and associated TCVI than many centers included in the NIS. Third, a number of other studies reported TCVI diagnosed only with CTA and not confirmed with cerebral angiography, which is still considered to be the gold standard for imaging of the carotid and vertebral arteries. The accuracy of CTA in this setting is limited and varies according to study. The false positive rate of CTA for screening for TCVI has been found to be as high as 37%. 3 Therefore, because the other studies may have included some false positive CTA results, the resulting TCVI incidences in the other studies may have been higher than the true incidences. A fourth possibility is that the total numbers of blunt trauma admissions in this study were overestimated, leading to underestimation of TCVI incidences. However, the total numbers of blunt trauma admissions found in this study are comparable to estimates of total annual national admissions for trauma reported in other studies, including the NIS 57 and the National Electronic Injury Surveillance System All Injury Program (NEISS-AIP). 58
This study found a significant increase in the incidence the diagnosis of TCVI over time. Another study, using the National Trauma Database, also found a significant increase in the diagnosis of blunt traumatic vertebral artery injuries over time, from 2001 to 2005. 53 This is likely because of the increasing use of CTA screening protocols, as well as more sensitive later generation 16- and 64-detector CT scanners.
The results of this study regarding gender, age, ethnicity, and cause of injury are similar to the findings in the other studies. This observation provides some degree of confirmation that the patient data set in the present study matches the patients detailed in other reports of TCVI.
There are several limitations to the present study. First, the retrospective design of this study carries the potential for selection bias and error. We attempted to indirectly confirm the validity of the incidence data in the present study by comparing the results with those of other studies found in the literature review. The similarities between the present findings and other published studies suggest that the patients in these studies were similar. Second, the NIS, being a very large database, is likely to contain some amount of coding error and variability in coding. For example, the diagnosis of TCVI is likely to be underreported in centers without CTA screening protocols, and the NIS database is limited to 15 diagnoses per admission; patients with polytrauma may have>15 diagnoses.
Conclusion
Data from the NIS about the number of patients with TCVI admitted to hospitals in the United States on an annual basis is within the range of incidences of the diagnosis of TCVI among trauma patients reported by individual and small groups of centers. The fact that the NIS incidences lie toward the lower end of the range of previously reported incidences is likely because of the relatively comprehensive screening protocols used by the centers that have published their data. The NIS incidences have risen over time, and this is likely attributable to more widespread use of screening of trauma patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.