
Abstract
Although the prevalence rate of chronic post-traumatic headache (CPTHA) after mild traumatic brain injury (TBI) reaches up to 95%, its mechanism is unknown, and little is known about the characteristics of the pain system in this condition. Our aim was to investigate the capabilities of two pain modulatory systems among individuals with CPTHA and study their association with CPTHA, here for the first time. Forty-six subjects participated; 16 with TBI and CPTHA, 12 with TBI without CPTHA, and 18 healthy controls. Testing included the measurement of heat-pain (HPT) and pressure-pain (PPT) thresholds in the forehead and forearm, pain adaptation to tonic noxious heat, and conditioned pain modulation (CPM).The participants completed a post-traumatic stress disorder (PTSD) questionnaire. The two TBI groups did not differ in the TBI and background characteristics. However, TBI patients with CPTHA had significantly higher HPT and lower PPT in the cranium and higher PTSD symptomatology than TBI patients without CPTHA and healthy controls. Adaptation to pain and CPM were diminished in the CPTHA group compared with the two control groups. The intensity of CPTHA correlated negatively with cranial PPT, magnitude of pain adaptation, and CPM. CPTHA intensity correlated positively with PTSD symptomatology. CPTHA appears to be characterized by cranial hyperalgesia and dysfunctional pain modulation capabilities, which are associated with CPTHA magnitude. It is concluded that damage to pain modulatory systems along with chronic cranial sensitization underlies the development of CPTHA. PTSD may reinforce CPTHA and vice versa. Clinical implications are discussed.
Introduction
C
CPTHA is the most prevalent type of pain after mild TBI, with a prevalence rate of 47–95%, compared with ∼20–38% in moderate-severe TBI. 1,2,6,7 Two recent studies examined the rate of headache longitudinally among a large cohort during the 1st year after the TBI. 8,9 The incidence at baseline was 54–44%, and the cumulative incidence of headache over 1 year was 71–91%. More than one third of the subjects reported persistent headache across the follow-up period.
Despite the high prevalence rate of CPTHA and its deteriorating impact on the quality of life of individuals with TBI. 10,11 Studies on the characteristics and pathophysiology of CPTHA are surprisingly scarce. Consequently, the mechanism of CPTHA, and hence its treatment, remains as yet unclear. In a previous study, our group conducted systematic quantitative somatosensory testing among individuals with chronic TBI with and without CPTHA, and healthy controls. 12 Individuals with CPTHA exhibited thermal hypoesthesia and hypoalgesia in the head (painful region) and hands (remote pain-free regions) compared with both control groups, but had similar mechanical sensibility, suggesting a generalized rather than local impairment of the spinothalamic system and spared dorsal column system, a sensory profile compatible with “central pain.” 13 –16 Testing also revealed mechanical hyperalgesia and allodynia in the head among individuals with CPTHA compared with controls, 12 suggesting the presence of cranial sensitization. 17 –20 We concluded that CPTHA is a complex syndrome that seems to result from a combination of injury to both central and peripheral structures, possibly leading to central pain, and chronic sensitization of intra- and extracranial nociceptors.
The central mechanism underlying CPTHA is not clear, but one such mechanism may be related to dysfunctional pain modulation capabilities that render individuals susceptible to chronic pain. An association between chronic pain and dysfunctional pain modulation was reported for various types of primary headache 21 –25 and other chronic pain conditions. 26 –28 Our aim, therefore, was to study whether CPTHA is associated with disrupted pain modulation. As a control for the TBI itself, a group of individuals with TBI but without CPTHA was included in the study, as well as healthy controls. To the best of our knowledge, such testing has never been conducted in individuals with CPTHA.
Methods
Subjects
Forty-six individuals participated in the study, which was composed of three groups: 1)16 individuals with CPTHA after TBI (13 males and 3 females, age 36.5±11 [mean±SD] years), 2) 12 individuals with TBI without headache of any kind (10 males and 2 females, age 34.1±9 years) and 3) 18 pain-free healthy individuals (14 males and 4 females, age 31.6±9 years).
Patients diagnosed with CPTHA and who met with inclusion criteria, were chosen from a computerized list of patients who had attended the Headache Unit of the Department of Neurology at Sheba Medical Center, Tel-Hashomer. Recruitment of subjects was initiated by mail explaining the aims of the study, followed by a phone call explaining the study in more detail and further verifying the inclusion criteria. The eligible patients who agreed to participate in the study were invited to a single testing session. Individuals with TBI who did not have CPTHA were recruited from the Department of Head Injury at Sheba Medical Center, Tel-Hashomer and from the Department of Psychiatry at the Tel-Aviv Sourasky Medical Center, Tel-Aviv. Both departments have units for continuous care for individuals at the chronic stage of TBI. It is of note that the state's health system recognizes the need for these patients to continue (sometimes lifelong) treatment following TBI, and patients are seen (for maintenance, support and occasional crisis intervention) on a regular basis. These individuals were first approached by their therapists who explained the aims of the study. The inclusion criteria and eligibility of those who agreed to participate were verified, and eligible individuals were invited to a single testing session. Healthy controls were recruited from among the workers of the Medical Center and Tel-Aviv University.
Inclusion criteria for all individuals with TBI (group 1 and 2) were: 1) a diagnosis of mild brain injury as determined by a clinical evaluation and CT and/or MRI scans, 2) a minimum duration of 12 months since the injury, 3) no evidence of neurological and systemic diseases (e.g. diabetes, Parkinson's disease), 4) no pre-existing headache, 5) no medication-overuse headache, 6) no evidence of cervicogenic or whiplash-related headache, 7) no prior psychiatric illnesses, 8) no current depression, 9) no somatization disorder, 10) no current involvement in litigation, and 11) no communication and/or comprehension problems as assessed by clinical examination and by the routine neuropsychological tests that were administered at the time of admission to each unit. An additional inclusion criterion for group 1 was the presence of CPTHA for >6 months. CPTHA attributed to mild brain injury was diagnosed according to the International Classification of Headache Disorders (ICHD)-23 section 5.2.2: A) Headache with no typical characteristics known, B) head trauma with the following: 1) Either no loss of consciousness or loss of consciousness for <30 minutes, 2) Glasgow coma scale score ≥13, 3) symptoms and/or signs of concussion, C) Headache develops within 7 days after head traumas, D) Headache persists for >3 months after head trauma. Clinical and imaging examinations excluded secondary disorders such as hematoma, cerebral vein thrombosis, cerebral hemorrhage, or epilepsy.
It is noteworthy that most of the subjects had headaches for >12 months; therefore, they could be considered chronic. All patients were living in households in the community, and were seen at the rehabilitation clinic on a regular (once a week/a fortnight/a month) basis.
Informed consent was obtained from all subjects according to the Declaration of Helsinki after they received full explanation of the goals and protocols of the study. Experiments were approved by the Sheba Medical Center, the Tel-Aviv Sourasky Medical Center, and the Tel-Aviv University institutional review boards.
Equipment
Thermal stimulator
Heat stimuli were delivered using a Peltier-based computerized thermal stimulator (TSA II, Medoc Ltd., Israel), with a 3×3 cm contact probe. According to the principles of the Peltier element, a passage of current through the Peltier element produces temperature changes at rates determined by an active feedback system. As soon as the target temperature is attained, probe temperature actively reverts to a preset adaptation temperature by passage of an inverse current. The adaptation (baseline) temperature was set to 35°C. The probe was attached to the testing site by means of a Velcro band.
Pressure algometer
Pressure stimuli were delivered using a hand-held pressure algometer (Somedic Sales AB, Algometer type II, Sweden). The algometer has a built-in pressure transducer, electronics recording and display unit, power supply, and subject-activated push button connected via a cable to the instrument. The principle of operation of the algometer is the exertion of a constantly increasing rate of pressure, the latter being monitored by a cursor presented on the display. The tip of the algometer that is pressed against the skin is 1 cm2. The algometer was calibrated before each measuring day.
Procedure
Subjects were invited to a single testing session lasting ∼3 h. The experiments took place in a quiet room with an ambient temperature of 22±2°C. The subjects sat in a comfortable armchair with the forearm supported on a holder. Prior to sensory testing, the subjects were interviewed with regard to demographics, the TBI, and the CPTHA, and were trained for the sensory testing before the actual testing started. The thresholds for heat-pain and pressure-pain were measured first, because their values were used in the subsequent measurements. Heat-pain threshold (HPT) in the forearm was used for the purpose of measuring pain adaptation in the forearm. HPT in the shin was measured for the purpose of determining the conditioning stimulus in the conditioned pain modulation (CPM) test. HPT was also measured in the forehead in order to study whether the results obtained in our previous study 12 on a different group of individuals with CPTHA are repeatable or coincidental. Pressure pain threshold (PPT) was measured in the forearm for the purpose of determining the test stimulus in the CPM test. PPT was also measured in the forehead in order to study whether the results obtained in our previous study 12 on a different group of individuals with CPTHA are repeatable or coincidental.
After determining the pain thresholds, the measurement of pain adaptation and CPM followed. These tests were chosen as indices of two pain modulation systems. In these tests, pain inhibition is tested while noxious stimuli are applied either inside or outside the segmental receptive fields of nociceptive neurons, respectively. The former test is related to the activation of the periqueductal gray (PAG) and nucleus raphe magnus (NRM) of the rostro ventro medulla, 29,30 whereas the latter reflects the diffuse noxious inhibitory controls (DNIC) exerted by the subnucleus reticularis dorsalis (SRD). 31,32 At the end of the testing session, subjects completed the questionnaires.
Sensory testing
Pain thresholds
HPT was measured with the thermal stimulator using the method of limits. Subjects received four successive ramps of temperature, starting from an adaptation temperature of 32°C, at a rate of 2°C/sec with an interstimulus interval of 30 sec. Subjects were asked to press a switch at the first pain sensation perceived. HPT was the averaged reading of four successive stimuli of increasing temperature. 33
PPT was measured with the pressure algometer using the modified method of limits. The tip of the pressure algometer probe was placed perpendicular over the skin. Gradual pressure was applied from a baseline intensity of 0 kPa at a rate of 30 kPa/sec, with an interstimulus interval of 15 sec. Each application was administered at a different location on the skin within a predetermined area of 3×3 cm in order to shorten the overall measurement time (for the purpose of the CPM) and in order to avoid changes in the sensitivity of the skin. Subjects were instructed to press the switch the first pain sensation perceived, thus “freezing” the display with the corresponding pressure reading and recording it. PPT was the averaged reading of three successive stimuli of increasing pressure. 34
Pain adaptation
Pain adaptation was measured by applying tonic noxious heat stimuli at an intensity of 1°C above individuals' HPT measured as descried previously. For each subject, the stimuli were administered to the volar aspect of the forearm, for 60 sec, during which time the subjects were instructed to report the intensity of their pain every 15 sec using a visual analog scale (VAS). The VAS is a plastic ruler with an inner slider that has set points where 0 indicates “no pain” and 10 indicates “the most intense pain imaginable.” Thus, readings were obtained at time 0, 15, 30, 45, and 60 sec. The amount of adaptation was calculated by subtracting the last rating from the first. The course of adaptation was analyzed to detect time trends.
CPM
CPM was measured by applying a noxious stimulus to the nondominant volar aspect of the forearm (the “test stimulus”) and evaluating its perceived intensity alone, and in the presence of another noxious stimulus applied to the lateral aspect of contralateral shin (“conditioning stimulus”). This distance between the test and conditioning stimulus was reported to produce the most intense CPM. 35 The test stimulus was PPT measured with the pressure algometer as described previously. The conditioning stimulus was noxious heat, applied with the thermal stimulator, at an intensity of 2°C above individual HPT measured as described previously for a duration of 60 sec. PPT was first measured, than, after a break of 5 min, the conditioning stimulus commenced, and after 15 sec of operation, the PPT was measured again. Both the test and conditioning stimuli terminated at 60 sec. The magnitude of CPM was calculated by subtracting the PPT measured in the presence of the conditioning stimulus from the PPT measured alone. 35
Questionnaires and additional data collection
TBI
All patients with TBI were interviewed regarding their injury, including the date and their age at the time of injury, causes and circumstances, additional injuries that incurred with the main injury, and comorbidities. Information obtained at these interviews was cross-checked with subjects' medical records.
Chronic pain
Patients with CPTHA were queried about its onset, duration, quality, location in the head, frequency, and dynamic characteristics, as well as use of medication, and alleviating and aggravating factors. In addition, these subjects rated the intensity of CPTHA on a VAS. All patients with CPTHA completed the McGill Pain Questionnaire (MPQ). 36 The MPQ provides a quantitative evaluation of the patient's pain experience with a separate measure of its sensory, affective, and cognitive dimensions. Three quantitative parameters were derived: 1) the pain rating index (PRI), based on summing the values of the words chosen by the subject from the list; 2) the number of words chosen (NWC) from that list; and 3) pain intensity (pain at its least and when it becomes worse) on a five word/number scale.
Post-Traumatic Stress Disorder (PTSD)
PTSD is an anxiety disorder that develops following exposure to a potentially life-threatening event. Because PTSD and TBI are known to coexist, and because studies show an association between PTSD and chronic pain among individuals after TBI 10,37 especially among individuals with mild TBI, 38 we measured the severity of PTSD symptomatology among the participants. The PTSD Inventory was used. 39 This is a 17 item self-report scale based on the Diagnostic and Statistical Manual for Mental Disorders, 4th ed. (DSM-IV) criteria for PTSD, which evaluates post-traumatic stress symptomatology. PTSD severity is calculated as the number of symptoms present. The inventory was used in previous studies and has good convergent validity when compared with structured clinical interviews. Internal consistency calculated was high (α=0.91).
Statistical analysis
Data were analyzed with the IBM SPSS statistics software (version 21). Average values of continuous variables are described by means (SD). Categorical variables are described by frequencies. Analyses of variance (ANOVA) with post-hoc comparisons were used to evaluate differences between the groups in the continuous variables. Chi square analyses examined group differences in categorical variables. Pearson correlation examined associations between variables. The problem of multiple comparisons was addressed with the false discovery rate (FDR) procedure. 40 p values <0.05 were considered statistically significant.
Results
Characteristics of the study groups
Tables 1 and 2 describe the characteristics of the two TBI groups (individuals with and without CPTHA, respectively). Age and sex distribution was similar in these two groups as well as in the healthy controls. The two TBI groups did not differ in the time elapsed since injury, cause of injury, neck injury, and past involvement in lawsuits regarding the TBI. Subjects in both groups reported taking medication for various conditions including sleep disorders, blood pressure, gastrointestinal (GI) problems, and attention deficit disorder, with no significant difference between the groups. Eleven patients from the CPTHA group and three from the non-CPTHA group reported taking analgesic medications. Eight patients in the CPTHA group and five in the non-CPTHA group reported taking antidepressants/anxiolytics.
MVA, motor vehicle accident; FFH, fall from height; HIT, direct hit on the head.
MVA, motor vehicle accident; FFH, fall from height; HIT, direct hit on the head; GS, gunshot wound.
Characteristics of the CPTHA
The average VAS ratings of the CPTHA over the past six months was 6.7±1.3 (range 4.5–10) and it fluctuated between a minimum intensity of 4.6±1.7 (range 2–7) to a maximum intensity of 9.8±0.5 (range 8–10) at its worst. Mean NWC and PRI calculated from the MPQ were 15.5±6 (range 6–30) and 38.2±15 (range 17–62), respectively. All subjects reported that the headache had been present since the TBI. Ten patients (62.5%) reported that pain intensity since the injury was more or less stable, and six patients (37.5%) reported that pain intensity had gradually increased with time since the injury.
Headache was reported to occur 7–3 times a week by nine patients (56.25%), at least once a week by four patients (25%) and two to three times a month by three patients (18.75%). Headache was reported to last from a few minutes up to a few hours each time. During the episode, the headache was reported to gradually increase, rising to very high intensities and then subsiding.
The location of headache varied. The most frequent painful region was the temple (10/16, 62.5% of patients) followed by the vertex region and forehead (each 8/16, 50%), back of the head and eyes (7/16, 43.75%), and occipital region (5/16, 31.25%). Six patients reported having pain in the neck concomitant with the headaches.
The quality of headache was reported as pressing and penetrating by 12/16 (75%) patients. Additional descriptions were: pulsing and throbbing (10/16, 62.5%), sharp (9/16, 56.25%), radiating (7/16, 43.75%), pricking, drilling, and piercing (each 5/16, 31.25%). Descriptors of the affective dimension were: exhausting (12/16, 75%), intolerable (10/16, 62.5%), excruciating (9/16, 56.25%), and heavy (5/16, 31.25%).
Most frequently reported aggravating factors were: loud noise (10/16, 62.5%), stress/tension (8/16, 50%), bright light (7/16, 43.75%), and physical exercise and sleeplessness (each 5/16, 31.25%). Alleviating factors reported were: medications (12/16, 75%), darkening the room (10/16, 62.5%), relaxation and rest (9/16, 56.25%), and massaging the painful regions (5/16, 31.25%).
We could classify our patients with CPTHA into three subgroups according to the clinical complaints: 7/16 appeared to have tension-type headaches, like CPTHA, which were described as bilateral pain of mild to moderate intensity, pressing and dull in quality, which was aggravated by emotional stress and tension; and 6/16 appeared to have migraine-like CPTHA that was described as unilateral pain of moderate to severe intensity, throbbing, drilling, and piercing in quality, which was aggravated by physical activity, bright light, and load noise. Three patients had mixed CPTHA. Despite the differences in the clinical symptomatology, we could not find differences among these subgroups in any of the results of the sensory tests, PTSD symptomatology, or intensity and duration of CPTHA. Therefore, the results presented subsequently refer to the entire group.
Sensory testing
Pain thresholds
Figure 1 presents HPT

Heat pain threshold of patients with chronic post-traumatic headache (CPTHA) in the forehead and forearm was higher than that of non-CPTHA individuals (1, *p<0.05, ^1, p=0.09) and healthy controls (2, **p<0.05)
With regard to PPT, ANOVA revealed a significant effect of group type on PPT in the forehead (F[2,45]=4.11, p<0.05). Post-hoc tests revealed that PPT of patients with CPTHA was significantly lower than that of non-CPTHA individuals (p<0.05) and healthy controls (p<0.01) (Fig. 1B). Group type did not affect PPT in the hands (F[2,45]=0.13, p=0.87). All groups had similar thresholds (Fig. 1B).
Pain adaptation
Figure 2 presents the time trend of perceived pain (VAS) during the application of tonic noxious heat in the forearm for the three groups. Repeated measure ANOVA revealed a significant effect of group type (F[2,30]=7.6, p<0.01) and of time (F[4,60]=58.3, p<0.0001) on the VAS ratings in the forehead. In addition, the interaction group type by time was significant (F[8,120]=3.1, p<0.05), suggesting that the time trend of VAS ratings of all the groups was not uniform. Post-hoc tests revealed that VAS ratings of patients with CPTHA were significantly higher than those of both non-CPTHA and control groups (p<0.01 each), who were not different from one another. In addition, the magnitude of adaptation, calculated as the difference of the first from the last VAS rating was significantly smaller among patients with CPTHA (0.75±1.7 VAS units) than among both the non-CPTHA and the healthy control groups (2.6±2 and 2.3±2, respectively, p<0.01 each).

Perceived pain intensity of patients with chronic post-traumatic headache (CPTHA) did not change with time, whereas that of non-CPTHA individuals and healthy controls decreased with time, indicative of pain adaptation (p<0.01, analysis of variance [ANOVA]). Values denote mean±SEM.
CPM
Figure 3 presents the magnitude of CPM calculated as the delta in kPa between PPT in the forearm alone and PPT in the presence of the conditioning stimulus applied to the leg. One way ANOVA revealed a significant effect of group type on delta CPM (F[2,45]=7.4, p<0.01); patients with CPTHA did not exhibit CPM, and their delta value (+3.5±50 kPa) was significantly smaller than that of both the non-CPTHA (-52.4±50, p<0.01) and the healthy control (-44.6±35, p<0.01) groups.
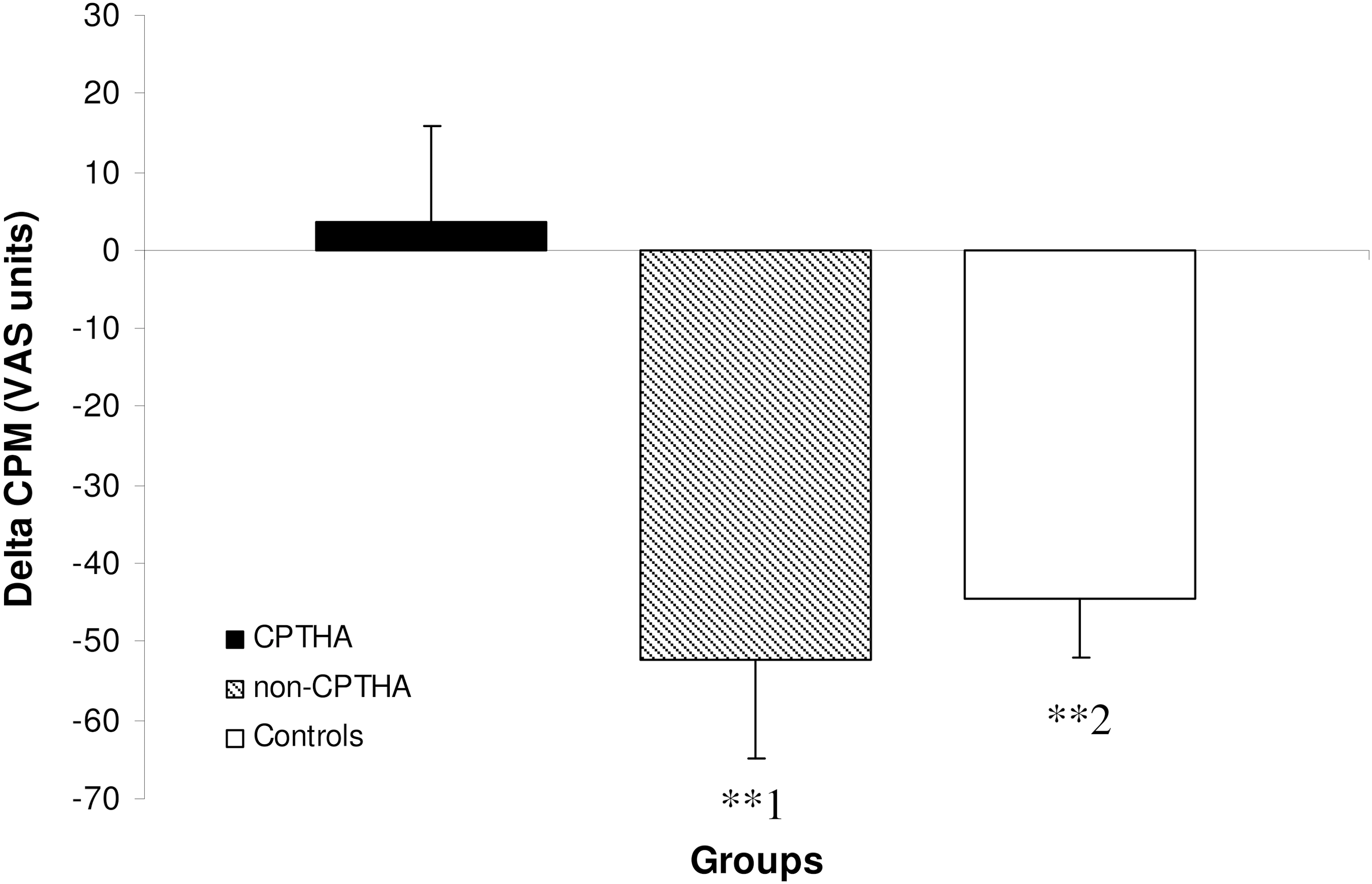
The magnitude of conditioned pain modulation (CPM) (delta in kPa of pressure pain threshold) of patients with chronic post-traumatic headache (CPTHA) was significantly smaller than that of non-CPTHA individuals (1, **p<0.01) and healthy control (2, **p<0.01) and practically absent. Values denote mean±SEM.
Correlations between CPTHA and sensory profile in the CPTHA group
As can be seen in Table 3, the intensity of CPTHA as measured with VAS and MPQ (NWC) correlated negatively with cranial PPT, pain adaptation, and CPM. Namely, the larger the intensity of CPTHA, the lower the PPT and the smaller the magnitude of pain adaptation (Fig. 4A)and CPM (Fig. 4B). The duration of CPTHA correlated positively with PPT; the longer the duration the higher the PPT (Table 3).

The intensity of chronic post-traumatic headache (CPTHA) correlated negatively with the magnitude of conditioned pain modulation (CPM) (r = −0.47, p<0.05)
p<0.05, ** p<0.01.
CPTHA, chronic post-traumatic headache; PTSD, post-traumatic stress disorder; HPT, heat pain threshold in the forehead; PPT, pressure pain threshold in the forehead; VAS, visual analog scale; NWC, number of words chosen; CPM, conditioned pain modulation.
Cranial PPT correlated negatively with pain adaptation magnitude (r = −0.69, p<0.01) but not with CPM magnitude (r =−0.11, p=0.34). HPT in the forehead did not correlate with either pain adaptation magnitude or with CPM magnitude (r=0.18, r=0.26, respectively). There was a trend toward positive correlation between CPM magnitude and adaptation magnitude (r=0.32, p=0.07), suggesting, perhaps, that in patients in whom one modulation process was dysfunctional, the other was dysfunctional too, and vice versa.
PTSD
One way ANOVA revealed a significant effect of group type on PTSD (F[1,45]=50.48, p<0.0001). The severity of PTSD symptomatology was significantly higher in the CPTHA group (56.6±10), than in either the non-CPTHA (34.4±15, p<0.001) and or the control group (22.7±6, p<0.0001).
Among the CPTHA group, the severity of PTSD correlated significantly with the magnitude of CPTHA as measured with VAS (r=0.58, p<0.01) and with HPT in the forehead (Table 3).
Discussion
Dysfunctional pain modulation
Patients with CPTHA were found to have reduced pain adaptation and diminished conditioned pain modulation (CPM). The magnitude of CPTHA correlated negatively with the magnitude of pain adaptation and CPM. These observations are reported here for the first time, and strongly suggest that CPTHA is associated with dysfunctional pain modulation capabilities.
Pain adaptation and CPM represent two different modulatory systems. Central neurons can be inhibited by nociceptive stimulation applied inside their receptive fields, triggering the PAG-rostral ventromedial medulla (RVM) exerted inhibition 29,30 or by nociceptive stimulation applied outside their segmental receptive fields, triggering the SRD exerted DNIC, 31,32 respectively. Both inhibitory loops are impaired in our patients.
Pain adaptation and CPM were not previously tested in individuals with CPTHA, but data exist on other headache types. For example, CPM was found to be reduced in individuals with tension-type, 21,22,41,42 migraine, 22,24,25 and medication overuse headache. 43 The two former are particularly relevant, because the clinical features of CPTHA resemble those of primary headaches. Lack of habituation of somatosensory evoked potentials 44 –47 and the blink reflex 48 was also found among individuals with primary headache.
The correlation found herein between the magnitude of CPTHA and the magnitude of pain adaptation and CPM does not provide causality. However, because non-CPTHA subjects and healthy controls have the same degree of pain adaptation and CPM, it would suggest that the dysfunctional pain modulation capabilities among CPTHA patients are related specifically to the CPTHA rather than to the TBI.
Cranial sensitivity to pain
Patients with CPTHA had generalized heat hypoalgesia (in the forehead and forearm) and cranial mechanical hyperalgesia. These results replicate our previous study with a different cohort, 12 but no additional comparable studies exist in this population.
Other headache populations exhibited altered pain sensitivity, albeit somewhat different than that of those with CPTHA. Individuals with tension-type headache had cranial mechanical hyperalgesia; 17,19,23,42,49 however, unlike our patients, they also had extracranial mechanical hyperalgesia 50 and normal cranial HPT. 51,52 Migraine subjects showed either normal 17 –19,53 or lower cranial PPT and HPT. 18,54 Subjects with whiplash headache showed decreased cranial and extracranial PPT. 55,56 Therefore, the sensory profile of CPTHA has some unique features.
The generalized heat hypoalgesia indicates central damage to the pain and temperature system 57 at the spinothalamic or the thalamocortical level or both, which may occur even after mild TBI. 58,59 Such damage is a key factor in the mechanism of central pain after spinal cord injury, 14,15 severe TBI 16 and stroke. 13 Such damage was also observed in our previous study on individuals with CPTHA after mild-moderate TBI, 12 suggesting that CPTHA may be a form of central pain. Aggravation of CPTHA by physical activity and stress may also support the presence of central pain; however, allodynia and hyperpathia, both common in central pain, were not common here.
Cranial mechanical hyperalgesia may result from injury to peripheral structures in the head/neck that occurs during the TBI, including blood vessels, the dura, bones, nerve fibers, and skin. The release of algogenic proinflammatory agents at the vicinity of the injured tissue propagates a chain of events leading to neurogenic inflammation and sensitization, 50,60 of which cranial mechanical hyperalgesia may be one clinical feature. Evidence for sensitization was reported in tension-type headache 19,49 and migraine, 18,60,61 concomitant with hyperalgesia. Neurogenic inflammation has been described in animal models of mild TBI, 20,62,63 rendering affected cranial nociceptors hyperexcitable and hyper-responsive to stimuli. If cervical damage also occurred during the TBI, then nociceptive input from cervical segments arriving to the trigeminal nucleus may have been a source of referred pain that contributed to mechanical hyperalgesia. 64
Possible mechanism of CPTHA
The combination of generalized thermal hypoalgesia and cranial mechanical hyperalgesia in CPTHA is not easy to explain; however, the novel results showing dysfunctional pain modulation in CPTHA may provide possible mediation. That both the PAG-RVM and SRD loops were similarly disrupted in our patients may suggest a common cause for their disruption. As mentioned, generalized thermal hypoalgesia indicates central damage to the ascending spinothalamic/thalamocortical tracts. Such damage may reduce the descending inhibitory control that is triggered by the ascending nociceptive information, 57 leading to increased neuronal hyperexcitability, as found in central pain patients. 33,65,66 Residual nociceptive neurons that are released from inhibitory control become hyperexcitable and burst spontaneously in an epileptiform manner concomitant with pain complaints in these patients. 67,68 CPTHA may thus result from lack of sufficient inhibitory control over the pain system caused by the central damage. The epileptiform and slow-wave abnormalities in individuals with TBI and chronic psychiatric, somatic, or cognitive complaints support this possibility. 69
It is of note that the reduction in pain modulation in CPTHA was measured in pain-free body regions. If the central reduction in pain modulation occurred during the TBI, one wonders why chronic pain was felt in the head and not in other body regions. This question is also relevant to other instances of chronic pain in which pain modulation is generally disrupted, but the chronic pain is localized. The answer to this question may be that chronic pain develops in the most sensitive or affected body region. In our cohort, chronic pain was localized in the head because the cranial tissues were affected during the TBI, as was evidenced by the mechanical cranial hyperalgesia. Namely, although pain modulation may be centrally disrupted after TBI, chronic pain may develop in the regions where nociceptors' sensitization was not resolved and became chronic. Reduced pain modulation may also be inherent in the individuals with CPTHA, and the damage to the pain system occurring during the TBI may render it even further incapable, leading to the emergence of CPTHA.
The negative correlation found here, between cranial hyperalgesia and pain adaptation (that was measured in intact regions remote from the head) may imply that pain modulation is more impaired when the pathological consequences of the TBI are more robust. The latter may either be directly related to the magnitude of the brain injury, or to the magnitude of the response of the nervous system to that injury. Therefore, impaired pain modulation may not necessarily be a prerequisite for the development of CPTHA, but rather a risk factor. Longitudinal studies on the dynamics of pain modulation capabilities after TBI are needed to address these possibilities.
Although we cannot determine whether the disrupted pain modulation preceded or resulted from the CPTHA, some evidence supports the former possibility. Variances in CPM are found among healthy people, suggesting that it may be inherently weak in some individuals. 70,71 Moreover, the magnitude of CPM in the pain-free state predicted postoperative pain. 72 Finally, the magnitude of CPM was found to decrease with age, when chronic pain becomes more prevalent. 73 Therefore, CPTHA could develop in patients in whom the TBI induced damage to modulatory structures or further debilitated an already weak modulatory system.
Recently, deficient pain modulation in migraine patients was found to be associated with reduced connectivity between the PAG and modulatory structures, including the orbitofrontal prefrontal cortex (OFC) and anterior cingulate. 74 Migraine patients also exhibited reduced activity in the OFC, which correlated with lifetime headache duration and longevity. 46 Since many individuals with mild TBI present damage to the frontal cortex 75 and those with PTHA present bilateral decreased levels of white matter N-acetyl aspartate (NAA) in the frontal and bilateral lobes indicative of axonal dysfunction, 76 such damage may contribute to the dysfunctional pain modulation found here, and hence the magnitude of CPTHA. Decreased level of NAA among individuals with post-concussive syndrome 77 may also support the aforementioned possibility.
It is noteworthy that chronic sensitization of cranial nociceptors may have developed regardless of whether CPTHA is a form of central pain, and it is certainly possible that both peripheral and central sensitization play an important role in propagating and sustaining CPTHA. A vicious cycle may develop wherein cranial hyperalgesia may contribute to the maintenance of CPTHA by increasing the nociceptive load onto an already sensitized nervous system. This may in turn exacerbate the pain and underlie the phonophobia and photophobia reported by some of the patients.
PTSD in CPTHA
PTSD symptomatology was increased among patients with CPTHA compared with the two control groups compatible with previous reports. 10,12,37,38 The severity of PTSD symptomatology correlated with the magnitude of CPTHA, suggesting an association albeit not causative between CPTHA and PTSD. 78,79 The high rate of headache among PTSD subjects even without related injury 78,80 further supports an association between the two.
The relationship between PTSD and CPTHA is difficult to explain. Longitudinal studies suggest that PTSD is a risk factor for chronic pain. 81,82 It has also been proposed that PTSD and chronic pain maintain and reinforce one another, or that PTSD and chronic pain develop in certain individuals because of a shared vulnerability. 83 Therefore, PTSD may affect CPTHA via increased levels of somatization, anxiety, distress, and depression, and CPTHA may obviously perpetuate emotional problems that further exacerbate the pain. 83 However, adjusting for PTSD does not eliminate the correlation between TBI and CPTHA, suggesting that each can independently contribute to CPTHA. 84
Conclusions
Patients with CPTHA present generalized heat hypoalgesia, cranial mechanical hyperalgesia, and dysfunctional pain modulation capabilities. It appears that central disruption of modulatory systems allows for CPTHA to develop after TBI. It also appears that PTSD coexists with CPTHA and can contribute to its persistence. The clinical implication of these findings would be to administer medication to individuals with CPTHA that is aimed at increasing the inhibitory tone and/or reducing excitability; for example, antidepressants and antiepileptics, as soon as possible after the TBI, and in addition, to monitor and treat any signs of PTSD.
Footnotes
Acknowledgments
The authors thank Yuval Levitan, from the Department of Head Injury at Sheba Medical Center for his help in recruitment, and Hila Gruener for her help in data collection. This work was supported by a grant from the National Association of Insurance Companies (grant number 1644063).
Author Disclosure Statement
No competing financial interests exist.