
Abstract
Spinal cord injury (SCI) is a devastating condition affecting young, healthy individuals worldwide. Existing agents have inadequate therapeutic efficacy, and some are associated with side effects. Our objective is to summarize and critically assess the neurological recovery and antioxidant effects of curcumin for treatment of SCI in rat models. PubMed, Embase, and Chinese databases were searched from their inception date to February 2014. Two reviewers independently selected animal studies that evaluated neurological recovery and antioxidant effects of curcumin, compared to placebo, in rats with SCI, extracted data, and assessed the methodological quality. A pair-wise analysis and a network meta-analysis were performed. Eight studies with adequate randomization were selected and included in the systematic review. Two studies had a higher methodological quality. Overall, curcumin appears to significantly improve neurological function, as assessed using the Basso, Beattie, Bresnahan (BBB) locomotor rating scale (four studies, n=132; pooled mean difference [MD]=3.09; 95% confidence interval [CI], 3.40–4.45; p=0.04), in a random-effects model and decrease malondialdehyde (MDA) using a fixed-effects model (four studies, n=56; pooled MD=−1.00; 95% CI=−1.59 to −0.42; p=0.00008). Effect size, assessed using the BBB scale, increased gradually with increasing curcumin dosage. The difference between low- and high-dose curcumin using the BBB scale was statistically significant. Neurological recovery and antioxidant effects of curcumin were observed in rats with SCI despite poor study methodological quality.
Introduction
S
Curcumin [1,7-bis(4-hydroxy-3-methoxyphenyl)-1,6-heptadiene-3,5-dione] is a major yellow pigment in turmeric, which is the ground rhizome of Curcuma longa Linn. 10 Turmeric has been used for various medicinal purposes in both Indian (Ayurvedic) and Chinese medicine for thousands of years. 11 Curcumin has been investigated for many uses, such as treatment of inflammation, as an antioxidant, for its anti-protein-aggregate activities, inhibition of nitric oxide, radical scavenging, and for its antitumor, -allergy, and -dementia effects. 12 Because of its pluripotency, oral safety, long history of use, and inexpensive cost, curcumin has the potential to prevent multiple neurological conditions that have less than optimal current therapies. 13 Curcumin can potentially reduce damage resulting from SCI. 9 Curcumin can benefit neuronal survival in SCI by down-regulating glial fibrillary acidic protein (GFAP) expression, 12 protecting the spinal cord tissues against oxidative stress (OS), 9 decreasing the level of tissue malondialdehyde (MDA), increasing tissue glutathione (GSH) peroxidase (GPx), superoxide dismutase (SOD), and catalase (CAT) activity, 10 and through anti-inflammatory effects. 14
The aim of this study is therefore to investigate neurological recovery and antioxidant effects of curcumin for SCI in rat models.
Methods
Study selection
A systematic literature search was conducted using PubMed, Embase, CNKI (including China Doctor/Master Dissertation Full Text Database and China Proceedings Conference Full Text Database), VIP, Wan Fang, and Chinese BioMedical (CBM) databases from their inception dates to February 2014. Key words included “spinal cord diseases,” “spinal cord injury,” “curcumin,” and “curcuma.” Details of the PubMed databases search strategy, as an example, are in Appendix 1. All searches were limited to studies on animals. Reference lists from the articles that were included were also searched to identify additional studies. No language restriction was used.
Two reviewers (M.Y. and L.Y.) selected the studies independently by screening the abstracts and full texts according to the eligibility criteria. Disagreements were resolved by consensus with a third author (X.J.C.). Searches were limited to animal studies using laboratory rats.
Eligibility criteria
Types of studies
Controlled studies assessing the in vivo administration of curcumin to rats with SCI were searched. All clinical case reports and solely in vitro studies were excluded. No language, publication date, or publication status restrictions were imposed.
Types of participants
Laboratory rats of any age, gender, or strain exposed to traumatic SCI induced by contusion or compression were included. Nontraumatic local or global ischemia, photochemical reaction, traumatic root avulsion, or dorsal root entry zone models, and genetically modified models were excluded. Laceration/transection SCI models were excluded because this model does not represent the typical crush injury mechanism in humans and has limited rostrocaudal secondary damage spread. 15
Types of intervention
Any type of curcumin intervention that was compared to placebo control was included. Dosage, formulation, route of administration, and curcumin administration time were not limited. Placebo control included DMSO (dimethyl sulfoxide), physiological saline, or no treatment.
Type of outcome measure
Functional evaluation
Function was evaluated and was recorded weekly using the Basso, Beattie, Bresnahan (BBB) locomotor rating scale and the inclined plane test for hindlimb motor function. If functional evaluations were performed at different times, the test on 7 days after injury was included.
The BBB Locomotor Rating Scale
The BBB scale assessment was performed 7 days after injury for all experimental animals. Behavioral assessment was measured using the BBB scale, 15 which is a well-documented, widely used ordinal (i.e., nonlinear) scale with discrete values ranging from 0 (no observable hindlimb movement) to 21 (coordinated gait, consistent toe clearance, predominant paw position is parallel throughout stance, consistent trunk stability, and tail is consistently up).
The inclined plane test
The inclined plane test was applied to rats 7 days after trauma. It was developed by Rivlin and Tator 16 and used to evaluate the maximum slope on which rats can maintain themselves for 5 sec on the inclined plane.
Biochemical analysis
MDA and SOD levels were the most frequently used indicators of lipid peroxidation (LPO). In this study, oxidative injury in the spinal cord during SCI was determined by measuring MDA concentration because it is the end product of LPO. If the MDA and SOD were performed at different times, the tests that were performed 1 day after trauma were included, and different measurement units and testing methods of MDA and SOD were ignored.
MDA
MDA is the breakdown product of major chain reactions leading to oxidation of polyunsaturated fatty acids and thus serves as a reliable marker of OS-mediated LPO. 17
SOD
SOD levels provide information about the antioxidant capacity of the organism. 18 Although it is difficult to limit the primary injury, there is increasing evidence that the impact of the secondary injury can be reduced using pharmacological strategies. 19 –22 Antioxidant treatments decrease SCI-induced damage by reducing OS.
Data extraction
Two authors (M.Y. and J.W.) independently extracted the details from studies that were included in the meta-analysis using a predefined form. Details included first author's name, publication year, animal strain, animal age (as reported in the study), gender, number of animals in each group, method used to induce SCI, SCI level, curcumin usage, dosage, and administration time, and measured outcomes. For each comparison, data were collected for mean outcome, standard deviation (SD), and number of animals per group. In studies with multiple intervention arms, only data from the SCI and curcumin groups were considered in this analysis. If one group of animals was assessed in more than one neurological domain (e.g., motor and sensory scores) or if both the neurological score and infarct size were measured, data were combined using a meta-analysis (see below) for an overall estimate of effect magnitude and standard error.
If any data were not indicated in the text, but only shown in graphs, data were estimated using GetData Graph Digitizer 2.24. A third reviewer (X.J.C.) resolved any disagreements between the two reviewers.
Assessment of the risk of bias in individual studies
To our knowledge, there is no established valid and reliable tool to assess the methodological quality or bias in animal studies. Therefore, we used the STAIR (the initial Stroke Therapy Academic Industry Roundtable) to assess the reporting quality and study design of the studies. 23 The STAIR was updated by the STAIR group in 2009, 24 according to the Recommendations for Ensuring Good Scientific Inquiry for America. The STAIR list includes the following: 1) Sample-size calculation; 2) inclusion and exclusion criteria; 3) randomization; 4) allocation concealment; 5) reporting of animals excluded from analysis; 6) blinded assessment of outcome; and 7) reporting potential conflicts of interest and study funding.
Two authors (M.Y. and Y.L.S.) assessed the risk of bias in individual studies. Bias was assessed as a low or high risk of bias, and “unclear” indicated that the risk of bias was not clear.
Statistical analyses
Data were pooled if outcomes were reported by at least three studies. We analyzed four treatment outcomes separately (BBB scale, inclined plane test, MDA level, and SOD level). First, we performed pair-wise meta-analyses for studies that directly compared a curcumin group and a control group. Then, we performed network meta-analyses to compare different dosages of curcumin (curcumin high dose was over 100 mg/kg, medium dose was 100 mg/kg, and low dose was less than 100 mg/kg), as applicable for each study.
For each measurement outcome of interest, pair-wise and network random-effects meta-analyses were performed to determine the pooled relative effect of each intervention relative to the other effects, and the mean differences (MDs) of the postintervention values from the different interventions were determined. We adopted the postintervention values in meta-analyses based on the baseline values being comparable between curcumin and the control group, as indicated by a Cochrane review. 25
Pair-wise meta-analyses
For pair-wise meta-analyses, data were analyzed using the REVIEW MANAGER 5.1.2 software (provided by the Cochrane Collaboration). We compared the final results from the studies to assess differences between the intervention and control groups. Cochrane's I 2 was used to assess heterogeneity. Heterogeneity was assumed if the p value was less than 0.10 using the chi-square (χ2) test. If the I 2 value was above 50%, the result was considered to have a high level of heterogeneity. 25 Clinically and statistically homogeneous studies were pooled using the fixed-effects model. 25 Clinically homogeneous and statistically heterogeneous studies were pooled using the random-effects model. 25 When studies used different instruments to measure the same thing, a standardized mean difference (SMD) was used in the meta-analyses to combine continuous data. 25
Network meta-analyses
We used the network meta-analysis methods to explore the appropriate curcumin dosage using Lumley's indirect comparisons; this model uses as covariates the basic parameters (a set of comparisons sufficient to generate all possible comparisons by the consistency equations) and assumes that heterogeneity is independent of the comparison being made. 26 Network meta-analyses were conducted using R software (version 3.0.1; R Language and Environment for Statistical Computing) with the nlme package that included the lme function, which is available free online. See the online documentation for the specific parameter usage in the “nlme” package. 27 We used the random-effects model, rather than the fixed-effects model, because it is the most appropriate and conservative analysis to account for differences among trials.
Results
Selection of studies
The process followed for article selection is shown in Figure 1. A total of 112 publications were identified using our search strategy. After full-text screening of the 11 publications, eight met the inclusion criteria. Of the three publications excluded at the full-text level, two did not report an outcome that met the inclusion criteria 28,29 and the other publication mixed curcumin with other treatments. 30 Two 31,32 of eight studies were published in Chinese whereas the rest were in English.

Summary of the literature identification and selection process.
Characteristics of the studies included in the meta-analysis
Characteristics of the studies that assessed the effect of SCI in rat models are shown in Table 1.
CUR, curcumin; SD, Sprague-Dawley; H&E, hematoxylin and eosin; TUNEL, terminal deoxynucleotidyl transferase dUTP nick end labeling; Nrf2, nuclear factor erythroid 2; γ-GCS, gamma-glutamylcysteine synthetase; i.v., intravenous N/A, not available.
Sprague-Dawley (50%) and Wistar (50%) rats were used in the studies; female rats were used in four studies and males were used in the other four. No studies used both female and male rats. Median sample size for all eight studies was 34 rats (range, 12–40). The main composition of the background diet was not reported in the included studies.
All of the eight studies used a traumatic SCI model in rats. Injuries were generated using a weight-drop impactor in five studies and by drill compression in the remaining three. All studies reported induction of SCI in the thoracic region with spinal cord levels T7–T11, and four of the SCI injuries were between T9 and T10. No study investigated a cervical or lumbar SCI model.
Sources of curcumin employed were not clear, whereas five studies reported that their curcumin were purchased from Sigma-Aldrich, which was claimed that the curcumin were from Curcuma longa (turmeric). Curcumin was administrated intraperitoneally (i.p.), except in one study where it was administered orally (p.o.). 9 Curcumin dose ranged from 30 to 300 mg/kg. Curcumin was dissolved in DMSO solution in most of the studies, 12,14,31 –34 whereas the remaining two studies did not report these details. The positive control medication was MP 9,31 or methylprednisolone sodium succinate (MPSS). 10,33 Half of the studies administered the compounds shortly after the trauma, three studies 10,31,33 treated SCI instantly after the trauma, whereas one other study administered treatment within 30 min after contusion. 14 In three studies, curcumin was administered i.p. (40 mg/kg) once-daily beginning 1 day before hemisection surgery and continuing for 6 days thereafter. 12,32,34 Another patient with traumatic SCI received oral curcumin 200 mg/kg/day 9 for 7 days after injury. Epidural injection appears to be a viable way to administer curcumin to animals to improve the pharmacokinetics of the compound's poor bioavailability. 14
Almost all of the studies reported the outcomes of functional evaluation and biochemical analysis, and some of the studies also reported histological evaluation. 10,12,14,32,33 Duration of evaluation ranged from 24 h to 7 days.
Risk of bias within studies
We describe the risk of bias reported for each publication included in this meta-analysis (Table 2).
Overall, the methodological quality of the studies was not high. Two of eight (20%) of the studies were considered to be high quality. None of the studies utilized here described a sample-size calculation or inclusion and exclusion criteria. All studies except one reported randomization, 14 whereas only one study reported allocation concealment. Blinded assessment of the outcome was used in four studies, 10,14,31,33 and four studies reported animals that were excluded from the analysis. 10,14,31,32 Three studies reported potential conflicts of interest and study funding. 12,14,31
Neurological recovery effect of curcumin
Four studies (n=132) reported a neurological recovery effect on the seventh day. All of the four studies measured neurological recovery using the BBB scale and one study also used the inclined plane test to evaluate effect of curcumin on neurological recovery.
The BBB scale significantly increased after curcumin (four studies, n=132; pooled MD=3.09; 95% confidence interval [CI], 0.11–6.07; p=0.04; Fig. 2) in a random-effects model because of the high heterogeneity.
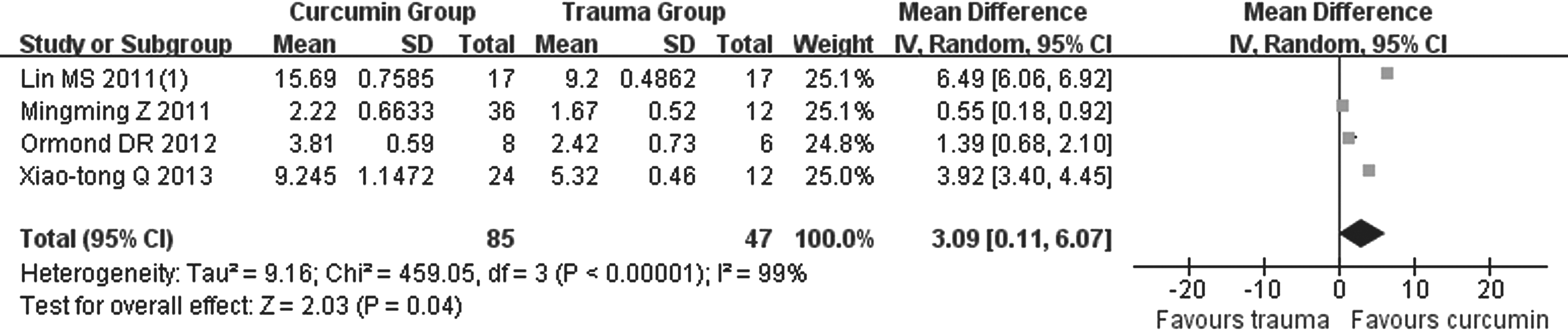
Basso, Beattie, Bresnahan scale meta-analysis using data on the seventh day after spinal cord injury. SD, standard deviation; CI, confidence interval.
Only one study 31 reported inclined plane test results, so the results could not be pooled. The study reported that 7 days after injury, the mean inclined plane test results had increased, and the curcumin treatment group and MP treatment group showed significantly higher values than the injury-alone group (p<0.05). Hindlimb motor function recovery in the high-dose curcumin group was better than that in the group that received MP therapy.
According to the network meta-analysis results, effect size increased gradually with increasing dose of curcumin. Moreover, the difference between the BBB scale results obtained with low- and high-dose curcumin were significantly different. There was a clear dose-response relationship between BBB scale results and curcumin dose (Fig. 3).
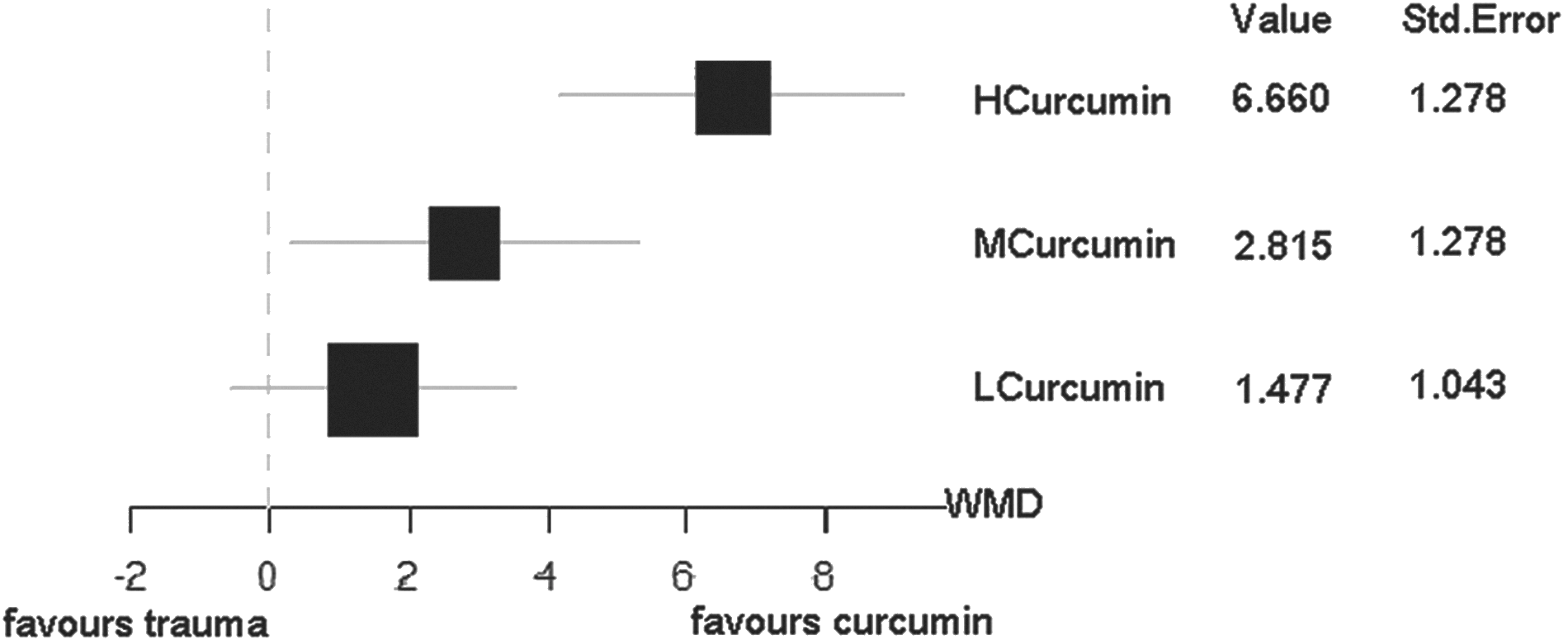
Basso, Beattie, Bresnahan scale network meta-analysis using data from 1 week after spinal cord injury. HCurcumin, high-dose curcumin; MCurcumin, medium-dose curcumin; LCurcumin, low-dose curcumin; WMD, weight mean difference.
Antioxidant effects of curcumin
Four studies (n=56) reported antioxidant effects after 24 h, four studies (n=56) measured MDA levels and two (n=32) also reported SOD levels. 9,10
MDA levels were significantly reduced after curcumin administration, using a fixed-effects model (four studies, n=56; pooled MD=−1.00; 95% CI, −1.59 to −0.42; p=0.00008; Fig. 4). Only two dosages of curcumin were used, so a network meta-analysis was not performed.

Malondialdehyde meta-analysis 24 h after spinal cord injury. SD, standard deviation; CI, confidence interval.
Only two studies reported SOD levels, and this amount was too small to be pooled. One study 9 reported that the SOD level in the curcumin group was higher than in the control group (p<0.001) and the MP group (p<0.012). Another study 10 found that the SOD activity in the curcumin group was significantly different from the trauma group, but was not significantly different from the control group (p<0.05 and p>0.05, respectively).
Discussion
Summary of evidence
This is the first systematic review to summarize the pre-clinical evidence on the use of curcumin and its potential to improve neurological recovery and affect antioxidant levels after SCI. We performed a systematic literature search that included English and Chinese databases to ensure the comprehensiveness of the studies that were evaluated. Two reviewers independently selected the studies, assessed methodological quality, and extracted data to avoid any bias.
This review extracted data from eight studies that compared curcumin to placebo control. The overall methodological quality of all the selected studies was low; there were two of eight studies (20%) considered to be of high quality. Two studies only reached the criterion of randomization. Treatment with curcumin led to a substantial and highly significant 3.09-point improvement using the BBB scale, compared to placebo control, on the seventh day after injury. There was a dose-response relationship between the BBB scale and curcumin. Only one study reported inclined plane test results 7 days after injury, and the mean inclined plane results increased, especially in the curcumin treatment group.
MDA was significantly reduced by curcumin after 24 h, and only two dose levels of curcumin were used. As a result, network meta-analysis was not performed. Only two studies reported SOD level; whereas one study reported that SOD level in the curcumin group was higher than in the control group, the other found that SOD activity in the curcumin group was significantly different from the trauma group.
The possible mechanism for the effect of curcumin in spinal cord injury
After a spinal cord trauma, the primary lesion is increased as a result of a series of autodestructive mechanisms, which result in secondary lesions. The secondary lesions result in a gradual degeneration of spinal cord parenchyma, leading to chronic neurodegeneration. 35 One of the major mechanisms after traumatic injury is free radical attacks on the cellular membrane, 36 which has long been established and plays a critical role in the pathophysiology of SCI. 37 –39 Measurement of MDA and SOD provides information about the organism's antioxidant capacity. 17,18 Antioxidant treatments decrease damage that results from SCI by reducing OS. 39 This study on OS showed that curcumin possesses significant antioxidant activity by increasing SOD level and reducing MDA level, which is an index of LPO that reflects oxidative status. Curcumin is one of the most potent and specific antioxidants for hydroxyl radicals, and it acts as a potent scavenger of free radicals.
Although other possible mechanisms about neuroprotection could be a result of the antiapoptotic effect, the prevention of neuronal damage, astrogliosis, and glial scar formation. 12,34,40 For example, curcumin may down-regulate nuclear factor kappa B, which is associated with glial scar formation and GFAP expression, which is related to astrocyte activation. 12,41 NeuN (feminizing locus on X-3, forkhead box 3, or hexaribonucleotide binding protein-3), a neuron-specific marker, revealed remarkable neuronal loss in the vehicle group after hemisection, whereas curcumin significantly protected neurons after SCI. 34
Considering these functions of curcumin, it was investigated as a potential neuronal protector following SCI. Curcumin is readily available, inexpensive, and has proven to be nontoxic even when administered at high doses. 42
The strenghts and limitations of this review
As with any meta-analysis, our study shares the limitations of the original studies. Although we searched English and Chinese databases, and included a manual search for relevant articles including gray literature that did not publish and conference proceedings, we still cannot be certain that all relevant studies were found. Moreover, selective publishing and reporting are other major causes of bias that must be considered. 43 In addition, even these estimates may be overinflated given the evidence for publication bias. No mechanism exists to publish negative results, especially in animal studies.
Results were analyzed on trial-level data, and therefore we could not assess whether all baseline characteristics were balanced among groups. There were different animal models and species used in the studies, and a simple pooled approach was not the most appropriate method, especially with only a few studies. In addition, several journals have space constraints, so the study authors may have omitted important details from their reports or key information may have been deleted during the publication process. The high heterogeneity among studies was clear not only on a statistical level, but also on actual significance. The wide variety of curcumin doses, different treatment initiation times, different routes of administration, varied methodological quality of studies, and even different sources and purity of curcumin could also bring confounding factors. However, because of the small sample of studies, a subgroup analysis of those factors may lead to misunderstanding. More studies of curcumin for SCI are needed.
The BBB scale was the most common method used to assess neurological recovery effects after SCI. Although it was validated and reliable, it relies on observation and interpretation and is thus susceptible to bias. Therefore, it should never be used unless the assessors are blinded to the treatment groups.
We are also aware that a meta-analysis, especially a shoddy one, has little clinical significance and value. A meta-analysis is a statistical analysis of the results of independent studies, which generally aims to produce a single estimate of a treatment effect. When used appropriately, it is a powerful tool in pooling data from small, yet similar, studies. The use of meta-analysis on heterogeneous studies is truly like comparing apples to oranges.
Some studies that used the wrong dosing regimen or did not include a careful dose-response analysis would also lead to confusion. However, before a dose-response analysis, the exact effect of curcumin should be clear, which was the main discovery of our meta-analysis. There was no such well-designed dose-response study about curcumin for SCI thus far, and the existing evidence could not reveal the accurate dose-response relationship about curcumin. However, our network meta-analysis had proved that a future dose-response study about curcumin for SCI would be meaningful. Future studies of pharmacological neuroprotective agents need to have a logical pharmacological design that includes dose response, determination of optimum dosing regimen that covers the duration of the target mechanism, and that it is determined whether the agent has a clinically relevant therapeutic window.
The status of methodological quality assessment for animal studies
To our knowledge, there is no established valid and reliable tool to assess the methodological quality or bias of animal studies, so the methodological quality assessments of each systematic review is not the same. The main tools used included the STAIR list, the CAMARADES (Collaborative Approach to Meta Analysis and Review of Animal Data from Experimental Stroke) checklist, and the Cochrane tool. The STAIR list includes criteria, such as sample-size calculation, randomization, and allocation concealment, that have been previously published.
24
Although it was a recommendation for pre-clinical studies of proposed acute stroke therapies, the updated seven items from the Recommendations for Ensuring Good Scientific Inquiry could be considered to be a standard for the methodological quality of animal studies for other models. The CAMARADES checklist included the criteria of peer-reviewed publication, statement of temperature control, random allocation to treatment or control, blinded induction of ischemia, blinded assessment of outcome, use of anesthetic without significant intrinsic neuroprotective activity, appropriate animal models (aged, diabetic, or hypertensive), sample-size calculation, compliance with animal welfare regulations, and a statement of potential conflicts of interest.
44
The free checklist can be obtained from the official website (
There were 12 systematic reviews on SCI in animals. 7,46 –55 Only 5 of these 12 were concerned with the methodological quality of the included trials. 46,47,49,51,53
One study 49 used a methodological quality assessment checklist that included four items from other reviews. 56 –58 Study quality was assessed using a checklist of nine items adapted from good laboratory practice guidelines for in vivo stroke modeling 59 and the CAMARADES quality checklist 44 in two studies. 46,47 Another study 53 used published literature 60 to develop a 13-item checklist to assess the quality of reporting and study design. In the remaining study, 51 two reviewers independently determined the adequacy of randomization and concealment of allocation, blinding of study personnel and outcome assessors, and registered sample-size estimations or power calculations. This shows that methodological quality was not sufficiently taken into consideration in the animal systematic reviews.
We adopted the STAIR list in our review because we considered the STAIR list to be an appropriate methodological quality assessment tool. These three checklists reached a consensus that sample-size calculation, randomization, allocation concealment, and blinded outcome assessment were important. These items are necessary to minimize bias in future studies. Compared with the other two tools, the STAIR list was more concise, and the basic criteria that focused on high quality were included in the list, such as sample-size calculation, randomization, allocation concealment, and blinded outcome assessment. The CAMARADES, however, required details of housing and husbandry, temperature control, and compliance with animal welfare regulations, which were more suitable for guiding authors preparing manuscripts for publication rather than for methodological assessment. However, the criterion of peer-reviewed publication in CAMARADES was also important for animal studies, which was different for clinical trials that are published based on peer review to guarantee the quality of the studies regarding the various kinds of animal study sources. The ITT concept should be more important in clinical trials, rather than animal studies, so the Cochrane tool was also abandoned in our review.
Future thoughts regarding animal studies
Animal studies are a necessary early step toward developing and evaluating an intervention for trials in humans. A reporting standard for animal studies is also needed, which is similar the Consolidated Standards of Reporting Trials (CONSORT) statement for clinical trials, to ensure substantial improvements are made in the reporting of data from animal studies. The National Center for the Replacement, Refinement and Reduction of Animals in Research (NC3R) refined the Guidelines of Animals in Research: Reporting In Vivo Experiments (ARRIV),
61
which was based on the CONSORT statement, and referred to the characteristics of animal tests.
62
It consists of 20 items describing the minimum information that all scientific publications reporting on research using animals should include, such as the number and specific characteristics of the animals used (including species, strain, sex, and genetic background), details of housing and husbandry, and the experimental and statistical methods (including details of methods used to reduce bias, such as randomization and blinding). This free checklist can be obtained from the official website (
Systematic reviews have been shown to be important for translating the findings from animal studies to human trials. 57,67,68 In clinical trials, systematic reviews and meta-analyses have made important contributions to our understanding of the sources of bias, and the quality of clinical trials has improved as a result. We believe that the same approach can be used to increase our understanding of sources of bias in animal experiments, which will lead to improvements in study quality. Whatever the merits of animal experiments, for many diseases, including stroke, the benefits observed in animal models have been lost in translation. It is important to determine the reasons for this discrepancy, and all available tools including systematic reviews should be used.
Conclusions
Curcumin was shown to improve neurological recovery and antioxidant effects in SCI in rat models, despite the poor methodological quality of the studies. The mechanism of curcumin action in SCI may be related to its antioxidant effect, including free radical scavenging, or neurological protective function. A dose-response relationship was found between the BBB scale and curcumin. However, a public methodological quality assessment checklist for the animal studies is needed and the STAIR list may be a used for this function. The widespread application of reporting guidelines also needs to be handled in the same way as the CONSORT statement is for clinical trials.
Footnotes
Acknowledgments
This is a Special Project of Traditional Chinese Medicine supported by Ministry of Finance of People's Republic of China (201107004), the National Basic Research Program of China (973 Program, 2010CB530400), the Program for Changjiang Scholars and Innovative Research Team in University (IRT1270) and Longhua Medical Team Project (LYTD-13), National Natural Science Foundation of China (81373666), Municipal Hospitals Cutting-edge Technologies Emerging Joint Project (SHDC12013113), Municipal Science and Technology Commission of Shanghai- TCM key project (14401970400).
Author Disclosure Statement
No competing financial interests exist.
Appendix 1. Search Strategy of PubMed
((“spinal cord injuries”[MeSH Terms] OR (“spinal”[All Fields] AND “cord”[All Fields] AND “injuries”[All Fields]) OR “spinal cord injuries”[All Fields] OR (“spinal”[All Fields] AND “cord”[All Fields] AND “injury”[All Fields]) OR “spinal cord injury”[All Fields]) OR ((“spinal cord”[MeSH Terms] OR (“spinal”[All Fields] AND “cord”[All Fields]) OR “spinal cord”[All Fields]) OR (((“neck”[MeSH Terms] OR “neck”[All Fields] OR “cervical”[All Fields]) AND (“spinal cord diseases”[MeSH Terms] OR (“spinal”[All Fields] AND “cord”[All Fields] AND “diseases”[All Fields]) OR “spinal cord diseases”[All Fields] OR “myelopathy”[All Fields] OR “bone marrow diseases”[MeSH Terms] OR (“bone”[All Fields] AND “marrow”[All Fields] AND “diseases”[All Fields]) OR “bone marrow diseases”[All Fields])) OR (((((“spondylosis”[MeSH Terms] OR “spondylosis”[All Fields] OR (“cervical”[All Fields] AND “spondylosis”[All Fields]) OR “cervical spondylosis”[All Fields]) AND (“spinal cord diseases”[MeSH Terms] OR (“spinal”[All Fields] AND “cord”[All Fields] AND “diseases”[All Fields]) OR “spinal cord diseases”[All Fields] OR “myelopathy”[All Fields] OR “bone marrow diseases”[MeSH Terms] OR (“bone”[All Fields] AND “marrow”[All Fields] AND “diseases”[All Fields]) OR “bone marrow diseases”[All Fields])) OR ((“neck”[MeSH Terms] OR “neck”[All Fields] OR “cervical”[All Fields]) AND spondylomyelopathy[All Fields])) OR (multilevel[All Fields] AND (“neck”[MeSH Terms] OR “neck”[All Fields] OR “cervical”[All Fields]) AND spondylotic[All Fields] AND (“spinal cord diseases”[MeSH Terms] OR (“spinal”[All Fields] AND “cord”[All Fields] AND “diseases”[All Fields]) OR “spinal cord diseases”[All Fields] OR “myelopathy”[All Fields] OR “bone marrow diseases”[MeSH Terms] OR (“bone”[All Fields] AND “marrow”[All Fields] AND “diseases”[All Fields]) OR “bone marrow diseases”[All Fields]))) OR ((“neck”[MeSH Terms] OR “neck”[All Fields] OR “cervical”[All Fields]) AND spondylotic[All Fields] AND (“spinal cord diseases”[MeSH Terms] OR (“spinal”[All Fields] AND “cord”[All Fields] AND “diseases”[All Fields]) OR “spinal cord diseases”[All Fields] OR “myelopathy”[All Fields] OR “bone marrow diseases”[MeSH Terms] OR (“bone”[All Fields] AND “marrow”[All Fields] AND “diseases”[All Fields]) OR “bone marrow diseases”[All Fields])))))) AND (((((((((Natural[All Fields] AND Yellow[All Fields]) OR ((((“curcumin”[MeSH Terms] OR “curcumin”[All Fields]) OR curcuminoids[All Fields]) OR (“demethoxycurcumin”[Supplementary Concept] OR “demethoxycurcumin”[All Fields])) OR (“bis(4-hydroxycinnamoyl)methane”[Supplementary Concept] OR “bis(4-hydroxycinnamoyl)methane”[All Fields] OR “bisdemethoxycurcumin”[All Fields]))) OR (“curcuma”[MeSH Terms] OR “curcuma”[All Fields] OR (“indian”[All Fields] AND “saffron”[All Fields]) OR “indian saffron”[All Fields])) OR ((“curcumin”[MeSH Terms] OR “curcumin”[All Fields] OR “tumeric”[All Fields] OR “curcuma”[MeSH Terms] OR “curcuma”[All Fields]) AND yellow[All Fields])) OR (yellow[All Fields] AND (“ginger”[MeSH Terms] OR “ginger”[All Fields]))) OR (yellow[All Fields] AND (“plant roots”[MeSH Terms] OR (“plant”[All Fields] AND “roots”[All Fields]) OR “plant roots”[All Fields] OR “root”[All Fields]))) OR (merita[All Fields] AND (“earth (planet)”[MeSH Terms] OR (“earth”[All Fields] AND “(planet)”[All Fields]) OR “earth (planet)”[All Fields] OR “earth”[All Fields]))) OR (“curcumin”[MeSH Terms] OR “curcumin”[All Fields] OR “diferuloylmethane”[All Fields])) OR (“curcuma”[MeSH Terms] OR “curcuma”[All Fields]))