
Abstract
Pediatric mild traumatic brain injury (pmTBI) is the most prevalent neurological insult in children and is associated with both acute and chronic neuropsychiatric sequelae. However, little is known about underlying pathophysiology changes in gray matter diffusion and atrophy from a prospective stand-point. Fifteen semi-acute pmTBI patients and 15 well-matched healthy controls were evaluated with a clinical and neuroimaging battery, with a subset of participants returning for a second visit. Clinical measures included tests of attention, processing speed, executive function, working memory, memory, and self-reported post-concussive symptoms. Measures of diffusion (fractional anisotropy [FA]) and atrophy were also obtained for cortical and subcortical gray matter structures to characterize effects of injury as a function of time. Patients exhibited decreased scores in the domains of attention and processing speed relative to controls during the semi-acute injury stage, in conjunction with increased anisotropic diffusion in the left superior temporal gyrus and right thalamus. Evidence of increased diffusion in these regions was also present at four months post-injury, with performance on cognitive tests partially normalizing. In contrast, signs of cortical atrophy in bilateral frontal areas and other left-hemisphere cortical areas only emerged at four months post-injury for patients. Current results suggest potentially differential time-courses of recovery for neurobehavioral markers, anisotropic diffusion and atrophy following pmTBI. Importantly, these data suggest that relying on patient self-report or standard clinical assessments may underestimate the time for true injury recovery.
Introduction
T
Thus, the pathophysiology of pmTBI and the subsequent relationship to neurobehavioral sequelae remain actively debated. Diffusion tensor imaging (DTI) has emerged as a potential mechanism for non-invasively measuring traumatic injuries, with the majority of studies focusing on moderate-to-severe 6 –9 or mixed 10,11 pediatric injury cohorts at more chronic (e.g., months to years post-injury) time-points. The majority of these studies report decreased fractional anisotropy (FA) in the white matter of chronic patients. In contrast, reports of increased FA have also been observed in two other independent samples of semi-acutely injured pmTBI patients, 12 –15 although these findings have not always been replicated. 16 No studies have prospectively examined diffusion abnormalities in gray matter following semi-acute pmTBI, in spite of recent reports of abnormalities in both animal 17 –19 and adult human 20 –23 studies.
Similarly, atrophic changes in gray matter have not been investigated in the semi-acute injury phase of pmTBI or prospectively. Neuronal degeneration (atrophy) occurs in the first few months of injury and continues into the more chronic injury phase in more severe TBI, 24 –26 even in the absence of macroscopically detectable lesions. 27,28 Injury severity predicts the magnitude of both white and gray matter loss in severe pediatric TBI, with milder injuries also associated with long-term structural changes. 4,29 In adult mTBI, atrophy due to frank neuronal or neuropil loss may occur later in the course of mTBI, 22,30 may be limited to patients with lesions, 31 or may be limited to chronically symptomatic patients. 32
The current study is the first to prospectively investigate both diffusion abnormalities and atrophic changes in gray matter after pmTBI. These potentially time-dependent biomarkers of gray matter injury were investigated in a cohort of semi-acutely injured pmTBI patients and matched healthy controls (HC). All pmTBI patients were evaluated with neuropsychological testing and brain imaging within 21 d of injury, with 11 patients returning for a second visit approximately four months post-injury. We hypothesized that pmTBI patients would show evidence of increased anisotropic diffusion in gray matter regions vulnerable to injury, such as the thalamus, hippocampus, and medial and lateral frontotemporal cortices. 27,33 –35 In contrast, we predicted that there would not be any evidence of atrophy during the semi-acute or early chronic (i.e., ∼four months post-injury) phases of pmTBI. 22
Methods
Participants
Sixteen patients with pmTBI and 16 age- and education-matched HC were recruited for the current study (Table 1) from local hospital EDs. Demographic data, details about each patient's injury, inclusion and exclusion criteria, and white matter DTI data have been previously reported for this cohort and are only briefly repeated here. 14 All pmTBI were between 10 and 17 years of age and experienced a closed-head injury with an alteration in mental status. Glasgow Coma Scale score was 13–15 at the time of injury, loss of consciousness (if present) was limited to 30 min, and post-traumatic amnesia (if present) was limited to 24 h.
Effect sizes (pmTBI - HC) are Cohen's d unless denoted by Phi. Demographic data are raw scores (above the first solid line), whereas neuropsychological measures and BASC-2 measures are T-scores. * denotes significant or trend findings.
SD, standard deviation; M, male; F, female; R, right; L, left; WM, working memory; PS, processing speed; EF, executive function; WRAT, Wide Range Achievement Test; BASC-2, Behavior Assessment System for Children, Second Edition; SRP, Self-Report of Personality; PRS, Parent-Rating Scales.
Exclusion criteria for both groups included a positive history of neurological disease, psychiatric disturbance, prior closed-head injuries with more than 5 min of loss of consciousness, learning disorder, attention deficit hyperactivity disorder (ADHD), substance abuse, or alcohol abuse.
Clinical (mean days post-injury=15.33±4.58) and brain imaging (mean days post-injury=15.87±4.93) evaluations occurred within 21 d of injury and in close temporal proximity (mean day difference=0.33±1.09). Ten patients received a computed tomography scan as part of routine care, all of which were negative. Data from one patient and one control was eliminated secondary to excessive motion on diffusion scans. 36 Of the total 15 pmTBI patients included, four sustained injury from a fall, nine had a sports or activity–related injury, and two were in a motor vehicle accident. In addition, 10 of the 15 patients experienced loss of consciousness and the five that didn't had symptoms of confusion that lasted longer than 15 min.
Informed consent was obtained from participants according to institutional guidelines at the University of New Mexico.
Clinical assessment
The Wide Range Achievement Test, Fourth Edition, provided an estimate of reading ability. Behavioral and emotional issues were measured by both self-report and parent ratings from the Behavior Assessment System for Children, Second Edition. A modified version of the Rivermead Post-Concussion Scale captured previous history of head injuries and post-concussive symptoms. A battery of neuropsychological tests were administered, 37 with composite indices calculated for the domains of attention, memory, processing speed, working memory, and executive function.
Imaging protocol
High resolution T1-weighted (1×1×1 mm), T2-weighted (1.15×1.15×1.5 mm) and susceptibility weighted (1.0×0.9×1.5 mm) images were collected on a 3 Tesla Siemens scanner to investigate structural lesions. A single run of diffusion weighted images (b=800 sec/mm2; voxel size=2×2×2 mm) were acquired using a twice-refocused spin echo sequence with 30 diffusion gradients and the b=0 experiment repeated five times. Please see previous publication for further imaging details. 14
Data analyses
DTI analyses involved a mixture of AFNI, FSL, and FreeSurfer software. 14,22 Image distortions caused by eddy currents or head motion were first corrected by registering all diffusion weighted images to the first b=0 sec/mm2 image using an affine correction with mutual information as the cost function. Diffusion weighted images were anisotropically smoothed and tensors calculated using a non-linear method for tensor calculation. Final FA, axial diffusivity (AD), and radial diffusivity (RD) data were then registered to each individual's T1 volume using a 12 degree of freedom affine transformation.
The FreeSurfer reconstruction pipeline (version 5.1) was used to generate cortical thickness values and regions of interest (ROIs) based on standard labels.
38
All processing results were visually inspected as part of routine quality assurance. The FreeSurfer longitudinal pipeline was used for all cortical data when comparing visits to maximize between visit image registration and account for variable time between visits.
39
Specifically, a “symmetrized” percent change (SPC) value was derived from the rate of change of FA or thickness, created by subtracting data from the first and second visits and normalizing by the amount of time between visits, using the formula
Subcortical ROI were defined based on FreeSurfer segmentation labels 38 and multiplied by respective diffusion maps. Principal analyses examining subcortical diffusion (FA) and atrophy (normalized by estimates of total intracranial volume) were restricted to the thalami and hippocampi, and evaluated with a single multivariate analysis of variance (MANOVA) due to the moderate linear relationship that exists between structures. Secondary voxel-wise analyses were also conducted on the remainder of subcortical structures (see Supplementary Methods, online only).
Results
Quality assurance and anatomical reviews
Previously published results 14 indicated no significant group differences in head motion or image quality between the pmTBI and HC group on DTI scans. An additional test was also conducted on total frame-wise displacement, which was also not significant (p>0.10). However, given the concerns with motion on diffusion 36 and echo-planar 40 data, supplementary analyses were also conducted for any significant DTI findings using frame-wise displacement as a covariate (see Supplementary Results). A board-certified neuroradiologist who was blinded to diagnostic status did not report any trauma-related or other pathology on anatomical magnetic resonance imaging scans (T1, T2, and SWI).
Visit 1 clinical data
No significant group differences (all p's>0.10) existed for reading ability, self-reported behavioral deficits, parent-reported behavioral deficits, or history of self-reported previous mTBI (pmTBI=2/15; HC=4/15). There was a trend (t25=−1.99; p=0.06) for higher parental education for HC relative to pmTBI (data missing for three participants). All demographic and clinical data can be found in Table 1.
A MANOVA was performed to examine differences in cognition given correlational structure between domains. The multivariate effect of group was not significant (p>0.10). Uncorrected univariate tests of cognition suggested worse performance for pmTBI patients in the domains of attention (F1,28=6.34, p=0.02; Cohen's d=−0.92) and processing speed (F1,28=4.04, p=0.05; Cohen's d=−0.73), with moderate effect size also present for memory functioning (Cohen's d=−0.59). However, performance was within the normal range (T-scores) for both groups across all cognitive measures.
Visit 1 imaging data
Results of the vertex-wise analysis of FA (Fig. 1) show a cluster of increased FA for pmTBI relative to HC within the left superior temporal gyrus extending to the posterior insula (Brodmann areas [BAs] 13/22/41; Montreal Neurological Institute [MNI] coordinates =−39.5, −30.8, 10.0; 1211 mm2). Follow-up tests indicated that RD was significantly decreased for pmTBI patients relative to controls (F1,28=6.20, p=0.02), with no group-wise differences in AD (p>0.10). There was no evidence of significant group differences (corrected p>0.05) in cortical thickness for Visit 1 data.
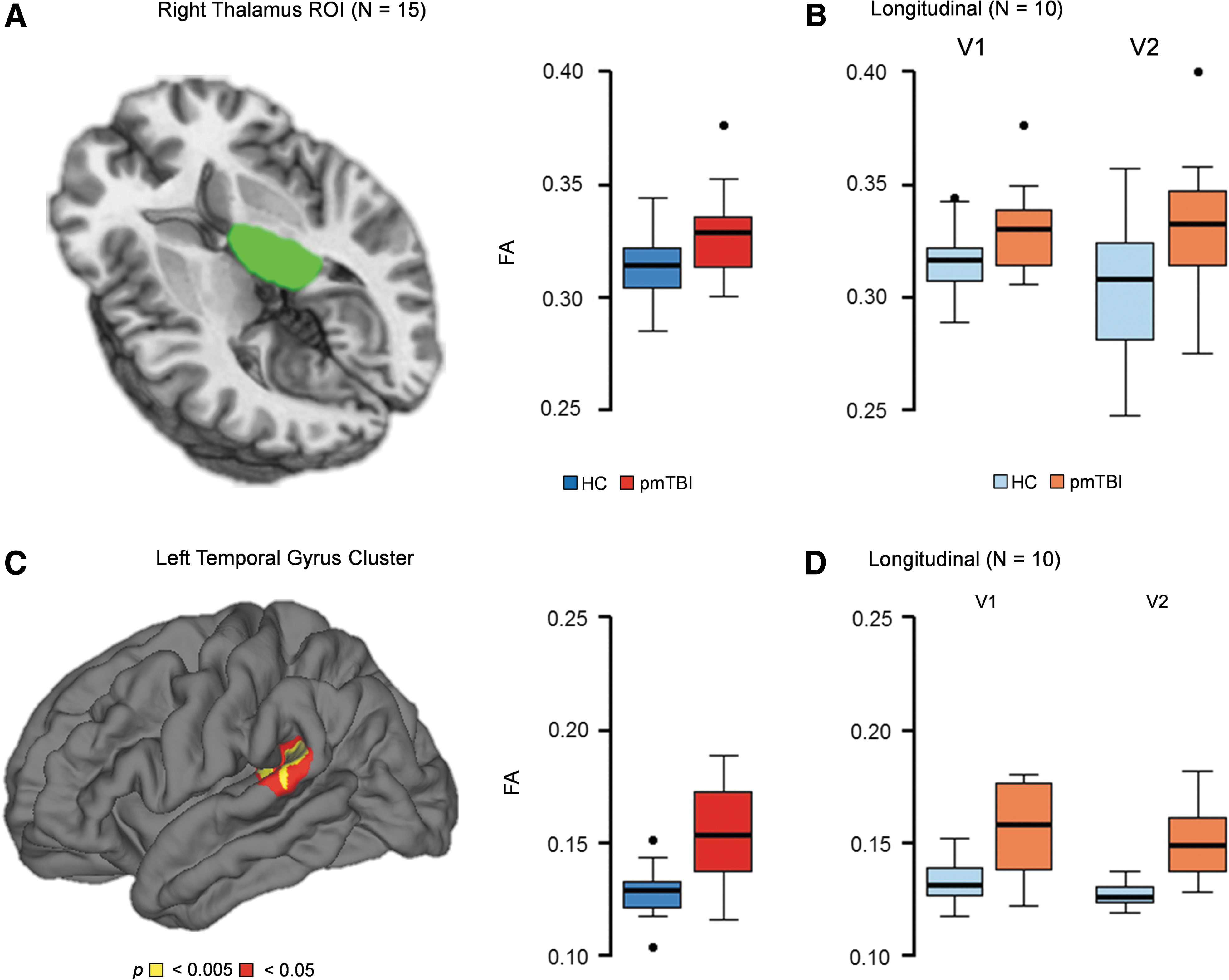
Results (Table 2) from the MANOVA examining diffusivity changes in a priori subcortical regions were not significant for the multivariate effect of group (p>0.10). However, a significant univariate effect was observed in the right thalamus (F1,28=4.94, p=0.04; Cohen's d=0.81) with pmTBI exhibiting increased FA (Fig. 1). Follow-up tests indicated that there were no significant differences in AD or RD (p>0.10). A moderate effect size was also observed within the left thalamus (Cohen's d=0.51; Table 2). There were no differences (p>0.10) in subcortical volume (hippocampi and thalami), with small effect sizes (Table 2). Supplementary analyses were also non-significant (see Supplementary Results).
Effect sizes (pmTBI - HC) are Cohen's d.
H, hemisphere; pmTBI, pediatric mild traumatic brain injury; HC, healthy controls; SD, standard deviation; L, left; R, right.
Two multiple regressions examined the relationship between cognitive deficits (attention and processing speed) and regions exhibiting significant FA abnormalities (right thalamus and left temporal cortex) across both cohorts. FA in these regions did not predict processing speed performance (p>0.10). In contrast, the overall model was significant for attentional functioning (F2,27=5.91, p=0.007), with the left temporal gyrus (t=−3.34, p=0.002) and right thalamus (t=2.42, p=0.023) both accounting for variance in the model. A significant relationship between FA and attentional measures was not present when the pmTBI group was run separately, which may have resulted from a lack of statistical power.
Visit 2 clinical data
Of the 30 participants included in Visit 1 analyses, 11/15 pmTBI and 12/15 HC returned at approximately four months (mean days post-injury=127.82±14.60 for pmTBI patients). Among returning participants, data acquisition errors occurred for one HC, and two other participants exhibited extreme motion (one pmTBI patient and one HC), leaving a final sample of 10 pmTBI and 10 HC. Changes in performance on processing speed and attention across the two visits were investigated with 2×2 (Group×Time) mixed-measures analyses of variance (ANOVAs). Results indicated a significant main effect of time for measures of attention (F1,18=7.34, p=0.01; Visit 1=54.61±3.50; Visit 2=57.48±5.18) and processing speed (F1,18=5.55, p=0.03; Visit 1=52.90±7.60; Visit 2=55.20±7.02). In addition, a significant trend was present for the main effect of group in processing speed (F1,18=3.14, p=0.09; HC=56.68±5.10; TBI=51.42±8.31). The Group×Time interaction was not significant for either cognitive domain (p>0.10). Effect sizes were reduced for both attention (Cohen's d=0.03) and memory (Cohen's d=−0.31) at Visit 2, but remained in the moderate range for processing speed (Cohen's d=−0.64).
Visit 2 imaging data
The 2×2 mixed measures ANOVAs (Group×Time) were used to evaluate significant changes in FA within the left temporal cortex and right thalamus as a function of time (Fig. 1). The main effect of group was at a trend level for the right thalamus (F1,18=3.57, p=0.075) and significant for the left temporal cluster (F1,18=16.44, p=0.001). The main effect of Time and the Group×Time interaction were not significant (p>0.10) for either region. The FreeSurfer Longitudinal pipeline was also used to examine for different rates of change in cortical FA from Visit 1 to Visit 2 between pmTBI and HC in the remainder of the brain (Group×Time interaction). Results for this analysis were not significant following correction for false positives.
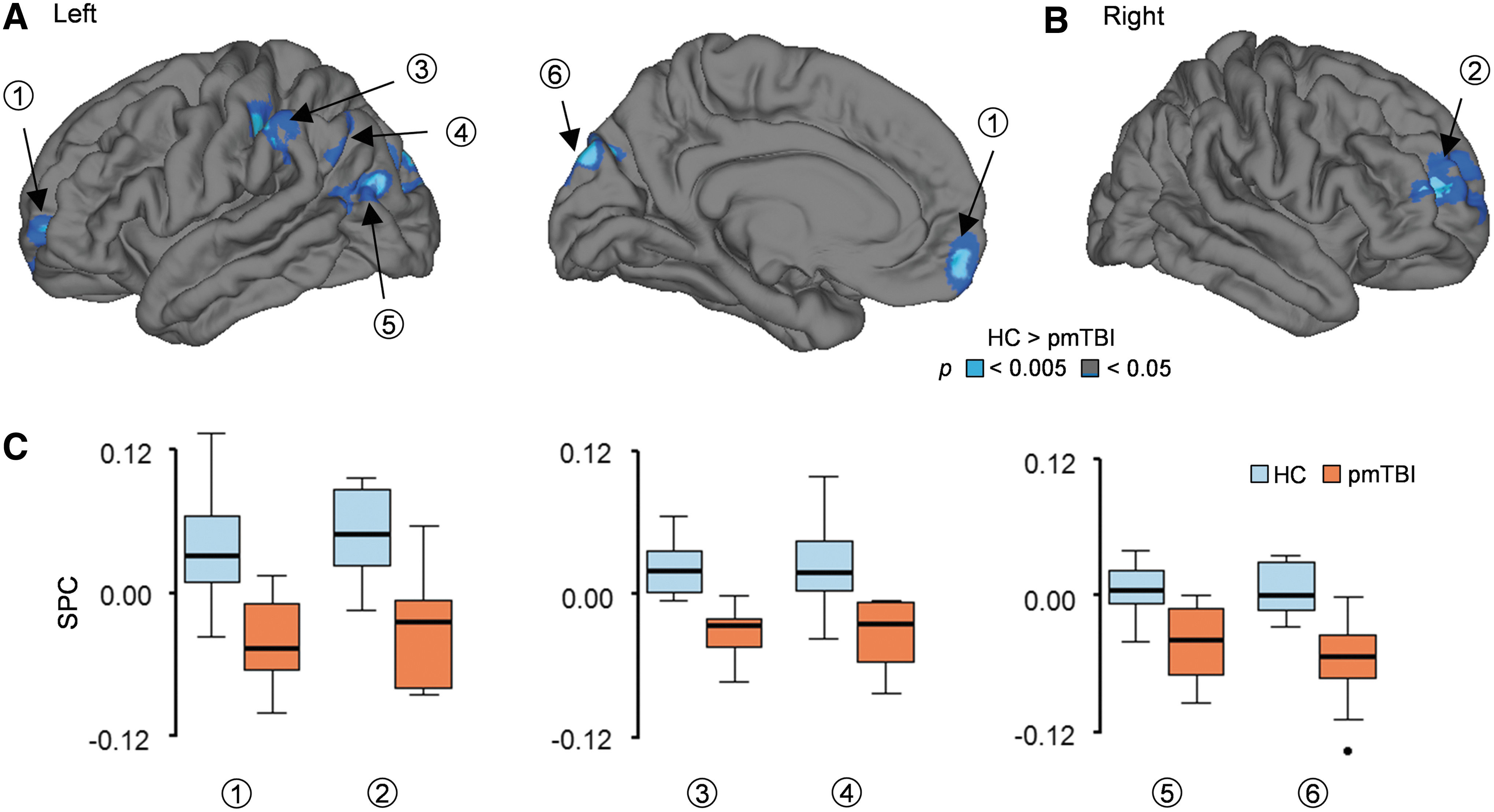
In contrast, results from an identical FreeSurfer longitudinal analysis using the cortical thickness data (Fig. 2) showed significant atrophy (change from Visit 1 to Visit 2) within the left superior and medial frontal gyrus (BAs 10,11; MNI coordinates=−7.1, 55.8, −12.8; 621.37 mm2), left middle temporal gyrus (BA 19; MNI coordinates =−41.3, −79.0, 16.9; 566.18 mm2), left postcentral gyrus extending into inferior parietal lobule (BA 40; MNI coordinates =−43.0, −28.5, 43.2; 855.11 mm2), left inferior parietal lobule (BA 7; MNI coordinates =−37.0, −63.8, 41.3; 514.70 mm2), and left cuneus and left middle occipital gyrus (BA 19; MNI coordinates =−7.4, −88.6, 30.4; 1027.24 mm2) for the pmTBI group. Significant atrophy for pmTBI patients was also observed within the right superior and middle frontal gyri (BA 10; MNI coordinates =23.9, 49.3, 15.0; 971.31 mm2).
Left
Finally, two 2×2 mixed measures ANOVAs (Group×Laterality) were conducted to assess for volume change (Visit 2 – Visit 1) for both the thalami and hippocampi. There were no significant differences in subcortical volume change as a function of group, laterality or the interaction (p>0.10).
Discussion
Although research examining gray matter changes following adult mTBI have recently been conducted, 20 –22 there have been no studies prospectively examining both diffusion abnormalities and atrophic changes in gray matter pathology after pmTBI. Current preliminary results indicate subtle cognitive deficits in the domains of attention and processing speed during the semi-acute phase of injury relative to controls, with partial (processing speed) or full (attention) recovery of function at approximately four months post-injury. Although others have reported more striking long-term neurobehavioral sequelae, 5 current results are generally consistent with previous longitudinal studies suggesting that pmTBI patients exhibit cognitive impairments (ImPACT testing) that typically normalize in the first few weeks of injury. 16
Similar to previous findings of increased FA in gray matter in adults, 22 pmTBI patients exhibited increased FA in the left temporal cortex and right thalamus relative to controls during the semi-acute injury phase, with the FA abnormalities associated with performance on attentional measures. FA remained increased within the left temporal cortex, with a trend seen for the right thalamus at approximately four months post-injury. Previous research indicates the thalamus is potentially more vulnerable to injury, 35 perhaps as a result of the accumulation of shear stresses in these regions. 41 Similarly, lateral frontotemporal cortices are also frequent injury sites as a result of the morphology of the skull. 27,29,33 Animal studies suggest that increased gray matter FA may result from the palisading of protoplasmic astrocytes and the subsequent formation of glial scars, occurring asymmetrically in the direction of the lesion. 17,19 Alternatively, increased FA and/or decreased apparent diffusion coefficient in gray matter have also been attributed to cytotoxic edema, reflecting alterations in the ratio of intracellular relative to extracellular water. 18,42,43 Future studies with increased angular resolution and multiple b-values may allow for the estimation of free intracellular versus extracellular water, 44,45 which may be helpful in differentiating cytotoxic edema versus reactive gliosis.
There was no evidence of gray matter atrophy (cortical thickness or sub-cortical volume changes) within the first few weeks of pmTBI. However, in contrast to a priori predictions, evidence of atrophy was present within bilateral frontal regions, as well as left temporal, parietal, and occipital cortex at four months post-injury. Gray matter volumes and functional connectivity have been shown to vary as a function of age, 40,46,47 and age at injury interacts with functional recovery in animal models. 48 However, a review of raw data confirmed that the reduction in cortical thickness occurred for the pmTBI cohort only over the four-month study interval and was not due to an increase for the controls. Similarly, in adult mTBI, atrophy has been reported to progress over time, possibly due to neuronal or neuropil loss later in the course of mTBI. 27,30,32 Previous reports of atrophy following pmTBI have been mixed, with one study reporting decreased hippocampal volume and increased cerebrospinal fluid 10 years post-injury. 4 In contrast, others have reported no evidence of atrophy at more than six months post-injury following complicated pmTBI. 29 Our use of a prospective design may have provided a more sensitive (i.e., within-subject) test of atrophy in frontal, temporal, and parietal regions as a direct function of injury progression relative to previous cross-sectional studies.
A particularly important topic for the field to address is the potential difference in the natural recovery courses for neurobehavioral (more rapidly resolving) and different physiological (more slowly resolving, evolving, or developing) signs of pmTBI. The current sample of pmTBI patients exhibited differential trajectories for neurobehavioral symptoms, increased anisotropic diffusion in both white 14 and gray matter, as well as atrophic changes in cortical thickness. Prospective studies in adult mTBI have shown a similar pattern of potentially faster resolution for self-reported symptomatology relative to diffusion abnormalities. 22,49 A similar process of cognitive improvement in conjunction with continuing or worsening brain pathology, potentially indicative of cerebral reorganization, is also common for more moderate to severe TBI patients. 27 In summary, similar to animal models of TBI, 50 the different signs and symptoms of pmTBI are likely to evolve differentially over time, which has important ramifications for determining when it is truly safe for a child to return to physical or cognitive activity. 51
There are several limitations to the current study. First, our relatively small sample size may have limited our ability to detect meaningful group differences (i.e., moderate effect sizes in memory and FA for left thalamus) and increased the likelihood of sampling bias. As a result, we have included effect size estimates for clinical measures and imaging measures where feasible. However, these results should be considered preliminary and require independent replication. Second, even though we did not observe significant neurobehavioral differences in returning versus not returning patients, the impact of sample attrition on longitudinal findings is unknown. Third, patients were assessed approximately 16 d post-injury, which may have compromised our ability to detect more rapidly-resolving neurobehavioral and pathological symptoms of mTBI. 52,53 Fourth, there are several factors other than trauma that can contribute to macroscopic measures of diffusion, such as head motion, 36 as well as individual differences in cognition 54 and emotional status. 55 We attempted to control for all of these factors through rigorous clinical assessment, as well as examining the effects of motion on current diffusion findings. Finally, we corrected for multiple comparisons in our imaging but not clinical data. Therefore, these results require future replication in independent samples.
In summary, pmTBI has been associated with an increased incidence of neuropsychiatric conditions, 56 delays in academic achievement, and decrease in overall quality of health. 5 Understanding the neuropathological underpinnings of these deficits is critical for both diagnostic considerations, clinical decisions about return to normal activity levels, and the development of novel psychiatric treatment strategies. Current preliminary results provide the first evidence of increased anisotropic diffusion and decreased cortical thickness as potential bio-markers of pmTBI. Importantly, our prospective design permitted the individual mapping of different timelines for these biomarkers of injury, as well as cognitive measures. The long-term consequences of a single episode of pmTBI on gray matter remain to be elucidated, as well as the potential disambiguation for single versus multiple temporally proximal pediatric brain injuries.
Footnotes
Acknowledgments
This research was supported by grants from The Mind Research Network [DOE Grant No. DE-FG02-99ER62764] to A.R.M.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.