
Abstract
Although the central nervous system has a limited capacity for regeneration after acute brain and spinal cord injuries, it can reveal extensive morphological changes. Occasionally, the formation of an extensive syrinx in the spinal cord can be observed that causes no or only limited signs of functional impairment. This condition creates a unique opportunity to evaluate the mismatch between substantial morphological changes and functional outcomes. We identified seven patients with holocord syringomyelia affecting the cervical cord following chronic traumatic thoracic/lumbar spinal cord injury (19–34 years after injury) or holocord syringomyelia of non-traumatic origin, and anatomical syrinx dimensions (length, cross-sectional area) were determined using sagittal and axial magnetic resonance imaging scans. Motor- and sensory-pathway integrity were evaluated using electrophysiological assessments (i.e., motor, dermatomal sensory, and dermatomal contact-heat [dCHEP] evoked potentials, as well as nerve conduction studies). These were specifically compared to clinical measures of upper-limb strength and grasping performance, including three-dimensional motion analysis. Despite extensive anatomical changes of the cervical cord (on average 26% reduction of residual spinal cord area and intrusion of almost the entire cervical spinal cord), a clinically relevant impairment of upper-limb motor function was absent while only subtle sensory deficits could be detected. dCHEPs revealed the highest sensitivity by disclosing impairments of spinothalamic pathways. Comparable to that of the brain, extensive anatomical changes of the spinal cord can occur with only subtle functional impairment. The time scale of slowly-emerging morphological alterations is essential to permit an enormous capacity for plasticity of the spinal cord.
Introduction
T
On a macroscopic scale, neural plasticity in terms of morphological alterations, as revealed by magnetic resonance imaging (MRI), frequently is associated with tumor or cystic formations. Interestingly, in slowly-progressing disorders such as benign brain tumors or hydrocephalus, patients can appear asymptomatic for a long time despite striking anatomical alterations. 13,14 Accordingly, in the spinal cord, the formation of a tumor or syringomyelia occasionally occurs without specific symptoms, and nonspecific symptoms such as tingling sensation, pain, and muscle weakness are reported. 15 –17
The most extensive form of syringomyelia is termed holocord syringomyelia, affecting almost the whole spinal cord in the axial plane, which can be found in association with congenital neural malformations (e.g., Arnold-Chiari) 15 or as a late sequel of spinal cord injury (SCI). 16,18 In rare cases, the etiology remains unknown and the holocord syrinx forms without apparent preceding incident. The holocord syrinx eventually may be discovered when it begins to cause symptoms or coincidentally during examination of unrelated disorders. At this stage, the syrinx may already cover a large volume of spinal cord, forcing neural tissue to the margins of the remaining space. These morphological changes not only involve adjustments within the neural tissue but also require associated adjustments of vascular and connective tissue. In the present study, clinical, electrophysiological, and kinematic measures were collected to assess the specific susceptibility of particular sensory and motor spinal tracts and to evaluate the capacity of the spinal cord to compensate for extensive morphological changes.
Methods
Subjects
Patients with a diagnosed holocord syringomyelia of the cervical spine were studied. For kinematic analyses, healthy control subjects were recruited. Additionally, MRI data of healthy age- and gender-matched subjects were drawn from our database to compare the spinal cord area. The study was approved by the ethics committee of the Canton of Zurich. Participants provided written informed consent.
Neuroimaging
Anatomical data were obtained from magnetic resonance images acquired by a 3T Magnetom Verio Scanner (Siemens Healthcare, Erlangen, Germany) with a 16-channel receive head and neck coil. The patients were scanned with a clinical MRI protocol of the cervical spine, containing the following sequences: 1) Sagittal T2-weighted turbo spin-echo sequence (repetition time, 3760 msec; echo time, 87 msec; number of slices, 20; slice thickness, 2.5 mm; matrix, 288×384; field-of-view, 220 mm×220 mm); 2) transverse T2-weighted turbo spin-echo sequence (repetition time, 3120 msec; echo time, 93, msec; number of slices, 26; slice thickness, 3 mm; matrix, 256×320; field-of-view, 160 mm×160 mm). This data was compared to T2-weighted images of healthy control subjects that were secondarily reconstructed into the transverse plane from sagittal sequences (repetition time, 3760 msec; echo time, 87 msec; number of slices, 20; slice thickness, 2.5 mm; matrix 288×384; field-of-view 220 mm×100 mm) using Jim 6.0 (Xinapse systems, Aldwincle, UK).
In patients, the extent of the holocord syrinx was evaluated by the absolute length (most rostral to most caudal vertebral segment with a syrinx in the sagittal MRI), length of syrinx (length of syrinx as percentage of total cord length between vertebral levels C0 and T12/L1), and the size of syrinx (cross-sectional syrinx area as percentage of total cord area obtained from axial anatomical MRI at the level of maximal syrinx diameter). At these levels, the cross-sectional residual spinal cord area (total spinal cord area minus syrinx area) was compared with the spinal cord cross-sectional area of age- and gender-matched healthy control subjects at the same spinal level. Spinal cord cross-sectional areas were measured using Jim 6.0. We extracted three slices from greatest syrinx diameter (bottle neck)—at level, one slice rostral and one slice caudal to that level—based on methods reported previously 19 and the cross-sectional area was calculated by an active-surface model. This procedure was repeated by a second person in order to estimate the interrater agreement, which was calculated by the intraclass correlation coefficient (ICC) according to Shrout and Fleiss. 20 In one patient, the cross-sectional syrinx area was assessed from spinal level T2 because of flow artifacts in the cervical MRI.
Neurophysiology
Neurophysiological recordings were derived from the upper extremities only, as the lower limbs were affected in those patients with preexisting SCI. The integrity of the corticospinal pathway was assessed via MEPs, elicited by a magnetic stimulator (The Magstim Company Ltd., Wales, UK) via a figure-of-eight coil placed over the motor cortex and derived from pre-activated muscles on the contralateral side of the body. If possible, the MEP was recorded from the abductor digiti minimi muscle. Only in Patient 35 was the abductor pollicis brevis taken due to a pre-existing sulcus ulnaris syndrome. To exclude peripheral nerve damage, NCS, including F-wave recordings of the ulnar nerve (median nerve in Patient 35), were performed and compared with standard values. Sensory pathways (i.e., dorsal columns and spinothalamic tract) were assessed by testing light touch (LT) and pinprick (PP) sensation and by more detailed and sensitive recordings of dSSEPs and dCHEPs, 21,22 respectively, elicited in dermatomes C4, C6, and C8. All evoked potentials (EPs) were evaluated by means of amplitude and latency, compared with standard values, and rated as abolished (no EP response), impaired (reliable response but pathological findings of latency and/or amplitude), or normal response. 23 –25
Functional outcome measures
Clinical outcome measures—such as the upper and lower extremity motor scores (UEMS, LEMS), the spinal cord independence measure III (SCIM-III), the walking index for spinal cord injury (WISCI II), 8 and the graded redefined assessment of strength, sensibility and prehension (GRASSP) 9 —were used to assess different levels of functional abilities in patients. For UEMS and LEMS, both the left and right sides were evaluated to give a total score. The SCIM-III sub-items self-care, mobility inside and mobility outside were considered for evaluation of patients' functional state during activities of daily living and divided into those that rely predominantly on upper-limb function and those that rely more on lower-limb function. Scores are indicated as percentage of maximally possible score corresponding to that of an able-bodied person. WISCI II scores are reported as percentage of maximal score (20). The four domains of GRASSP were evaluated accordingly.
Additionally, a specific reaching task was performed using the dominant arm/hand while recording kinematics in order to reveal subtle changes in upper limb movements that might not be visible to the naked eye. Because the lower limbs were affected by a traumatic injury in the SCI subjects, we only focused on upper limb motion. Kinematic data acquisition was performed at 200 Hz using a three dimensional motion capture system (Vicon Motion Systems Ltd., Oxford, UK) recording the movements of passive reflective markers placed on the scapula, the acromion, the lateral humeral epicondyle, the head of the ulna and radius, the head of the first, second, and fifth metacarpus, and the tips of each finger of the dominant hand. Subjects started from a resting position, where their hand passively lay on their lap, and were asked to reach forward towards an object the size of a walnut on a stick. They had to grasp the object, bring it to their mouth, and bite and hold it there while moving their hand back to resting position. This movement mimicked reaching for and eating a piece of food. Ten trials per person were recorded and analyzed.
For analysis, the reaching movement was split into three sub-movements: reaching, retract-to-mouth, and back-to-start. Success rate, movement speed, movement variability, and hand-path ratio (HPR) 26,27 were chosen as quantifiable readouts. Retrieval was classified as successful if all of the following conditions were met: only a one-time contact of the object while grasping (no regrasping/correction movement), the subject did not drop the object, and the object touched the mouth only once. Success rate was evaluated as percentage of successfully retrieved objects during 10 trials. Movement speed was calculated as the speed of the endpoint (marker on second metacarpus) during the reaching and retract-to-mouth sub-movements. Movement variability was calculated as the elliptic area of the endpoint in the sagittal plane where the half axes correspond to the standard deviation of the endpoint position in the horizontal and vertical axes. Reaching and retract-to-mouth sub-movements were time-normalized and variability was calculated for 10 trials at equal bins. HPR was calculated as the ratio of the direct path between start and end position and the actual path of the second metacarpal marker during the reaching and retract-to-mouth sub-movements. This readout is a measure for movement linearity of hand motion and was calculated as the mean of 10 trials.
Statistical analysis
The cross-sectional spinal cord area was compared between the two groups by a two-sample t-test. An analysis of variance (ANOVA) was used to examine differences between patients and healthy controls with regard to the kinematic data assessing movement speed and variability of the reaching movement, and HPR. Post-hoc Tukey's test was applied if ANOVA revealed significant differences. The success rate was compared between the groups using a Chi-Square test. Bonferroni correction was applied to account for multiple testing.
Results
Subjects
Seven patients (six males, one female; 45.4±8.1 years) with a diagnosed holocord syringomyelia were included in this study (Table 1). Four of the patients suffered from chronic traumatic thoracic/lumbar SCI (19 to 34 years prior to study inclusion) that affected only their lower limbs. One patient showed Chiari malformation while in two patients no associated disorder could be identified (termed idiopathic holocord syrinx). For the reaching task, we evaluated seven healthy control subjects (four males, three females; 25.1±2.6 years), while a second group of seven age- and gender-matched subjects served as controls for the evaluation of spinal cord cross-sectional area (six males, one female; 45.1±7.7 years).
Indication of the extent of the syrinx refers to the vertebral levels or intervertebral spaces. The onset of SCI refers to the incidence of the traumatic SCI prior to participation in the present study.
ID, identification; SCI, spinal cord injury; f, female; BS, brain stem; m, male; n/a, not applicable.
Neuroimaging
The ICC representing the interrater agreement for the cross-sectional spinal-cord and syrinx area measurements was 0.998. All patients showed an extensive syrinx (Table 2) in the cervical spinal cord that in mean occupied about 84% of the total cord length (Fig. 1A, 1F), and about 54% of the spinal cord cross-sectional area at the level of the largest syrinx diameter (Fig. 1B, 1D). For the whole group, the residual spinal cord area at the level of maximal syrinx diameter was significantly less (74%) in patients (59.7±12.9 mm2), compared with the corresponding spinal cord area in healthy, age-matched controls (100%, 80.2±16.8 mm2; t-test, p=0.025; Fig. 1C, 1E).
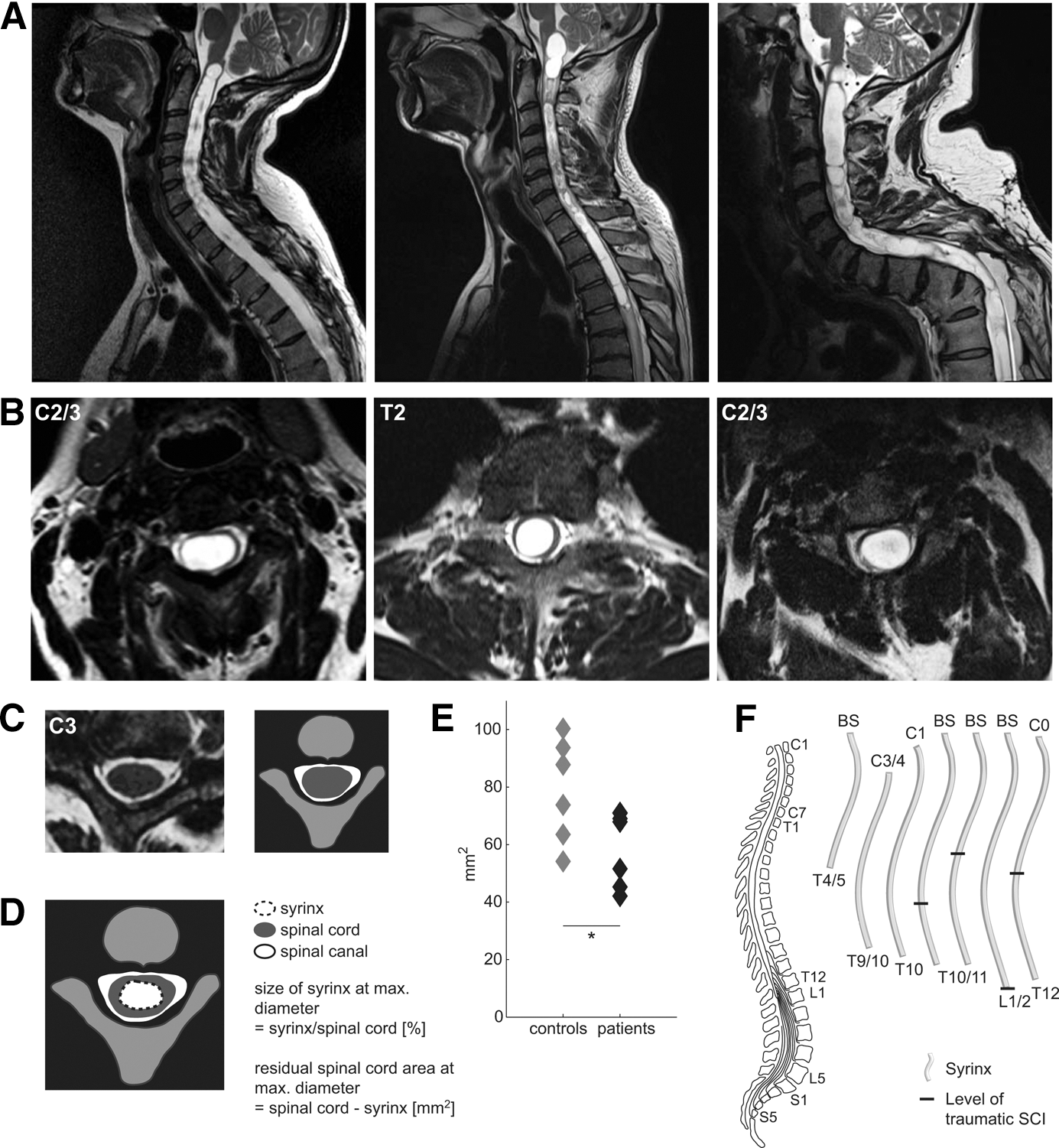
Sagittal and axial scans of the holocord syrinx. Panel
The length of syrinx refers to the extent of the syrinx in percentage of the total length of spinal cord between vertebral level C0 and the distal end of conus medullaris. The size of syrinx is described by the cross-sectional area of the syrinx in relation to the total area of the spinal cord (Fig 1B, 1D). Residual spinal cord area was assessed after subtraction of the CSF area of the syrinx from the surrounding total tissue area (outer rim of the spinal cord). Spinal-cord areas were retrieved from age- and gender-matched control subjects. On average, the residual spinal cord area in patients was 74% of control subjects (59.7 mm2/80.2 mm2), corresponding to a 26% reduction in cord area.
ID, identification.
Functional outcome measures
The mean UEMS of patients was 49.86±0.38 (99.7% of maximal value [50]), comparable to the strength domain of the GRASSP (94.9%), which showed almost normal qualitative and quantitative grasping (99.4% and 98.3%, respectively). Only the sensibility domain of the GRASSP assessed by Semmes-Weinstein monofilaments was impaired to a greater extent (71.7%). LEMS was 50 (100%) in all patients without SCI and 15.25±17.61 (30.5%) in patients with SCI (Fig. 2A). In the sub-items of the SCIM-III that predominantly depended on upper-limb function, patients attained 98.2% of maximal score. In the items that depended on lower-extremity function, patients reached 68% of maximal score, while in the WISCI II, 69% of maximal score. Patients without SCI reached 100% in the mobility categories while patients with SCI reached 77.5% in the mobility inside, 43.3% in the mobility outside SCIM sub-items and 46.3% in the WISCI II.
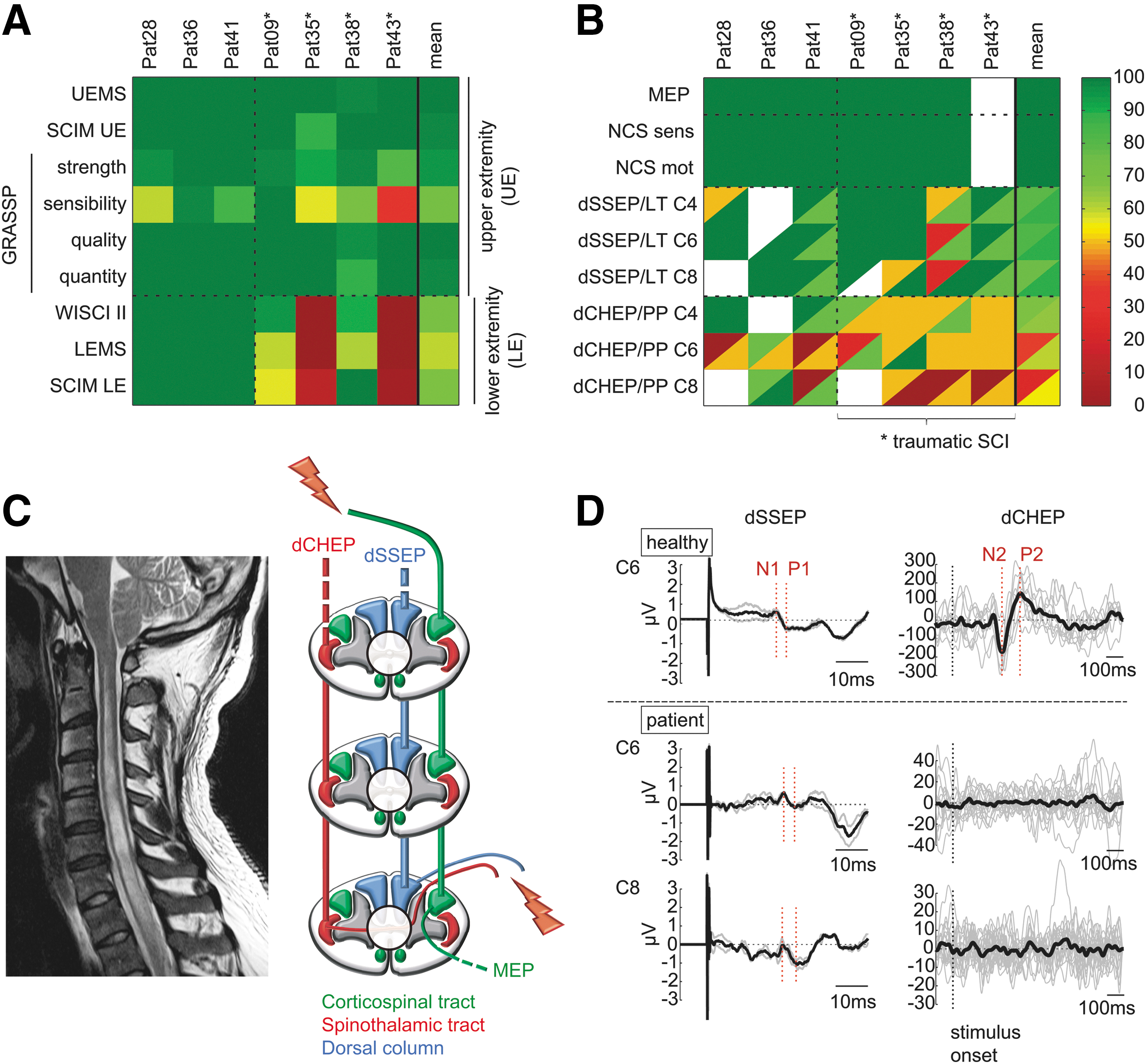
Clinical scores and electrophysiological data. Clinical scores are illustrated in
Neurophysiology
Electrophysiological data showed different sensitivities in detecting impairment (Fig. 2B) depending on the distinct pathways that were assessed (Fig. 2C), irrespective of the etiology of the holocord syrinx. The NCS yielded normal results in all patients. Likewise, all of the assessed MEPs of the upper limbs showed normal values. The assessment of sensory pathways showed distinct findings revealing differently-affected dSSEPs and dCHEPs (Fig. 2D). Four of seven patients showed normal dSSEPs from all assessed dermatomes, two patients showed at least one dermatome with normal dSSEPs, and one patient showed altered dSSEPs from every dermatome. However, there was no patient with normal dCHEPs derived from all of the measured dermatomes and three patients revealed pathological dCHEPs in all dermatomes. Clinical testing of LT and PP sensations also revealed greater impairment of PP, compared with LT sensation, when averaged across patients. LT and PP uncovered less deficits, compared with dSSEP and dCHEP recordings.
Kinematic analysis
Kinematic analysis revealed that upper-limb motor function was barely affected by the extensive holocord syrinx. Only one patient showed some deviations at performing the reaching task revealed by slightly deteriorated kinematics (Fig. 3B) when compared with healthy control (Fig. 3A). On average, patients showed upper limb movements comparable to controls (Fig. 3C). ANOVA revealed no difference in kinematic measures between groups (F=1.7; p=0.174). The movement variability (Fig. 3D) in both groups tended to be smaller during the reaching sub-movement, compared with the retract-to-mouth movement (Fig. 3E). Interestingly, healthy control subjects had a trend of greater endpoint variability than patients, though the difference was not statistically significant. The success rate was 100% in both groups. HPR did not differ between healthy controls and patients while the movement velocity tended to be higher in controls both during reaching and retract-to-mouth sub-movement, though lacking statistical significance (Fig. 3F).
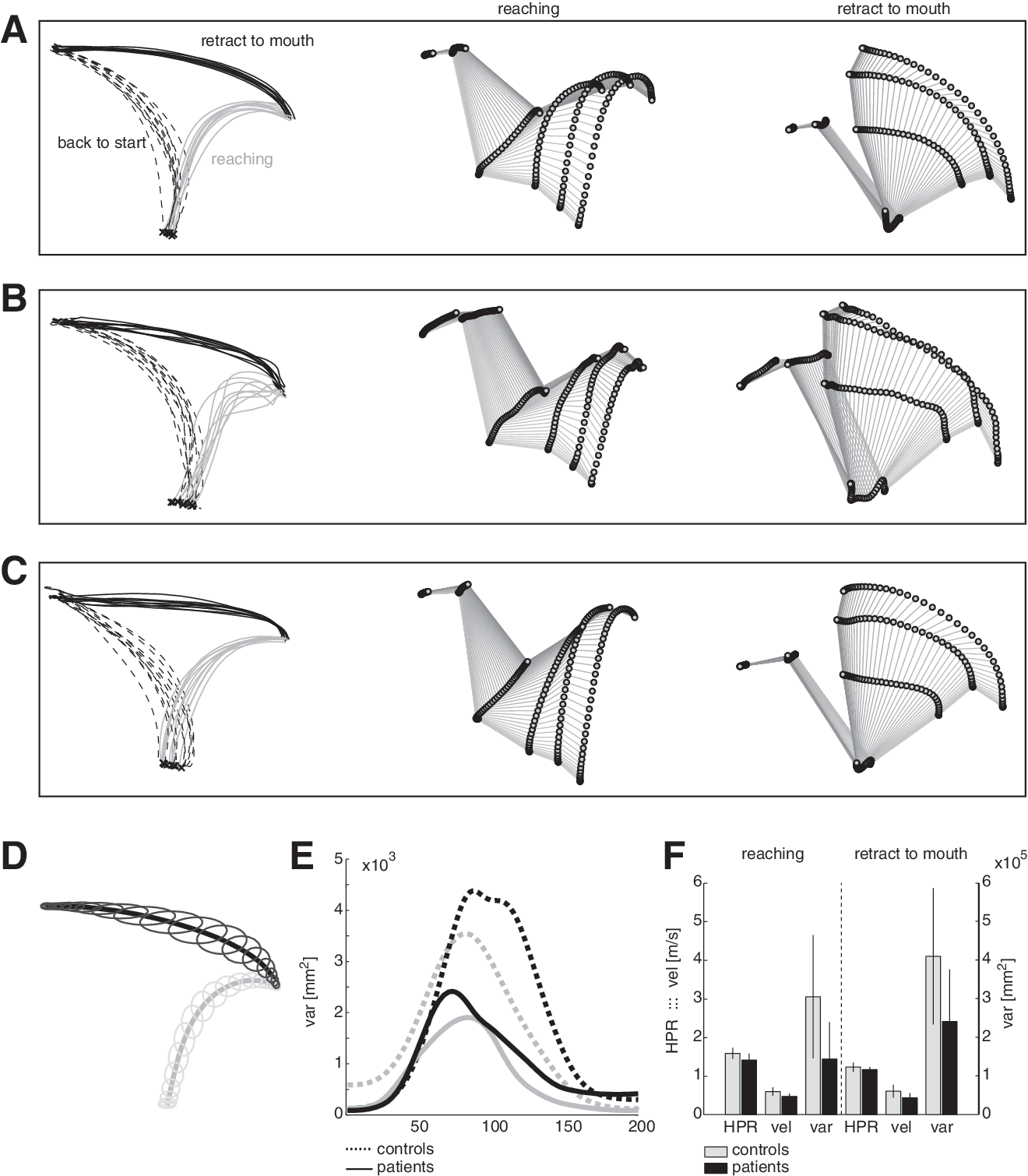
Reaching kinematics and performance.
Discussion
The present findings in patients with holocord syringomyelia show that despite extensive morphological alterations, spinal cord plasticity may still allow for normal limb movements. This impressive plasticity of the spinal cord is particularly startling considering the diminished amount of cross-sectional residual spinal cord area and major deformations of the spinal cord anatomy. While previous studies mainly focused on reporting specific symptoms for the diagnosis of a developing syringomyelia, this is the first study in holocord syringomyelia to compare the susceptibility of specific pathways in relation to extensive morphological changes and the preservation of complex upper limb movements. The findings reveal that, like the brain, the spinal cord has a high capacity to overcome large-scale morphological changes in slowly-emerging abnormalities, while the time-scale of evolution is considered critical. 13,28
Distinct manifestation of motor and sensory deficits
Clinical scores assessing upper-limb function in these patients with holocord syringomyelia revealed only minimal deficits in terms of muscle strength, and quality and success of movement, while sensation was particularly affected. In accordance with clinical motor testing, the electrophysiological assessments of motor pathways (MEP addressing corticospinal-tract conductivity, NCS evaluating α-motoneuron damage) showed unsuspicious findings. This is in contrast to findings in traumatic incomplete SCI where lesions of the cervical cord (including central cord syndrome with circumscribed lesions of the central gray matter) show altered neurophysiological recordings and lead to obvious motor impairments of the upper limbs. 22,29 –31
However, sensory assessments (clinical and electrophysiological) provided a higher sensitivity to disclose the vulnerability of specific fiber tracts. 32 Segmental sensory function assessed by dSSEPs (to examine dorsal column-medial lemniscal pathway integrity) and by dCHEPs (to show lateral spinothalamic-tract function propagating information on pain and temperature) was significantly affected, 33,34 revealing considerable impairments in dCHEPs while dSSEPs were normal in half of the patients. The reason for the differing sensitivity of EPs may lie within the anatomy of spinal tracts (i.e., lateral spinothalamic tract decussating on the spinal level of entry) affected by the centrally-located syrinx and a higher vulnerability of pain-conducting fibers (i.e., thinly myelinated Aδ- and unmyelinated C-fibers).
Upper-limb function and kinematic measures
Kinematic data confirmed the preservation of gross upper-limb motor function, and only when looking at specific parameters of arm/hand movements did a few trends became visible. The movement velocity tended to be higher in control subjects, which might be partly because of their lower mean age. Since MEP amplitudes and latencies were not impaired in patients and muscle strength was not reduced, the decrease in movement speed also may be attributed to the alteration in sensibility. During closed-loop control of targeted arm/hand movements, timely and appropriate sensory information is required for correct movement execution. Accordingly, deterioration of somatosensory information was shown to have detrimental effects on motor control in patients with proprioceptive deficits. 35,36 However, the higher variability by tendency of the endpoint trajectory during the retract-to-mouth movement in controls was rather surprising. A possible explanation may be the higher movement velocity, which leads to higher endpoint variability in target-aimed movements. 37 Generally, the movements showed great spatial inter-subject variability in terms of endpoint trajectory both in patients and controls, which is in contrast to small spatial lower-limb endpoint variability during walking. 38 The latter movement is probably dependent not only on direct corticospinal control but also on the input from subcortical brain regions and the sensory-motor integration on a spinal level.
Spinal cord plasticity
In patients with acutely (i.e., rapidly) progressing syringomyelia, associated symptoms are typically unspecific and diverse, ranging from increasing pain symptoms to changes in sensation and eventual muscle weakness, which may emerge very rapidly. 17, 39 –41 Any secondary neurological deteriorations following SCI call for further investigations. 16,18 In most studies, there was no reliable relation between clinical findings and neither diameter and length nor level of the syrinx as measured by MRI. 15,16,42,43 The present study in highly chronic and slowly-developing syringomyelia confirms this missing relation between the extent of a syrinx and clinical measures, which is probably most convincing in these presented cases with a holocord syrinx.
Interestingly, even the reduction in residual spinal cord area by as much as 26% and involvement of the whole cervical cord area was not related to the clinical conditions. Obviously, a change in cross-sectional spinal cord area is not a valuable marker for potential axonal damage but may serve as an indicator for the extent of morphological changes. The objective of this study was to reveal the discrepancies between morphological changes and neural function by taking the extreme example of holocord syrinx. Comparable discrepancies can be observed in compressive spinal disorders such as chronic calcified disc protrusions and extramedullary spinal tumors where despite massive space-occupying conditions with enormous thinning of the cord, patients also may present themselves with minor and unspecific symptoms. 44,45 A common feature of all these disorders is that they develop on a very slow time scale that likely spans over several years. In the presented four cases with post-traumatic holocord syrinx following thoracic or lumbar SCI, the mean latency between incident of SCI and inclusion into this study ranged between 19 and 34 years.
The underlying mechanisms enabling morphological plasticity while preserving complex function are not well understood. Obviously, a well-coordinated adjustment of neural and glial tissue, as well as vascular and connective tissue, is required. If and to what extent some of the underlying mechanisms may be in principle comparable to reparative changes (i.e., whether there are common elements of spinal plasticity after acute trauma and slowly-developing morphological changes) is unclear.
Limitations
This study is limited by the relatively small number of subjects with holocord syringomyelia available to us. The intention of this study was not to investigate the etiology and progression of the disorder, nor was it intended to serve as a basis on which to make decisions regarding surgical intervention. Clearly, to make a statement on how much structural changes the spinal cord may tolerate, which specific tracts may be affected, and for an exact quantification of tissue dimensions, more subjects need to be included using more sophisticated imaging techniques at higher spatial resolution, such as tractography (i.e., diffusion tensor imaging).
Conclusion
Analogous to that of the brain, extensive morphological alterations of the spinal cord may develop with only minor and unspecific clinical symptoms. While upper- and lower-limb function appeared unimpaired specific sensory assessments were most sensitive to reveal distinct alterations. In slowly-progressing disorders, spinal cord plasticity can overcome large-scale morphological changes enabling unimpaired functioning on a behavioral level.
Acknowledgments
We would like to thank M. Stüssi for assistance with kinematic data acquisition; W. Popp for performing the secondary analysis for the interrater agreement analysis; R. Sutter and the Department of Radiology at the Balgrist University Hospital for acquiring and partly processing MRI data; P. Freund and P. Grabher for providing MRI data; the Department of Neurophysiology and the Departments of Occupational and Physical Therapy at the Balgrist University Hospital for their contributions to data acquisition; and J. Steeves for his inputs concerning manuscript revisions.
This work was supported by the European Commission's Seventh Framework Program [CP-IP 258654, NEUWalk]; the Wolf Foundation, Switzerland; the Clinical Research Priority Program CRPP Neurorehab UZH.
Footnotes
Author Disclosure Statement
No competing financial interests exist.