
Abstract
Childhood traumatic brain injury (CTBI) is one of the most common causes of impairment in children and adolescents, with psychosocial difficulties found to be the most persisting. Given that the transition into adolescence and adulthood can be a stressful period, it is likely that young people who have sustained a CTBI will be more vulnerable to developing psychosocial problems. To date, most research has focused on psychosocial development up to five years following a CTBI and it is unclear how survivors develop in the long-term as young adults. The aim of this research was to track the long-term psychosocial outcomes of children with CTBI and compare them with healthy controls over a period of 16 years. Seventy-five participants with a CTBI and 29 control participants were followed up at five time-points over a period of 16 years. To measure psychosocial functioning (social skills, internalizing, and externalizing symptoms), questionnaires were completed by the primary caregiver acutely (pre-injury baseline), then six months, five years, 10 years, and 16 years post-injury. No significant group differences were found regarding the developmental trajectory of social skills, or internalizing and externalizing symptoms between the CTBI and control groups. The severe CTBI group demonstrated a trend of lower social skills, while the mild CTBI group showed a trend of higher internalizing and externalizing skills at six months, five years, and ten years post-CTBI event, compared with other groups. The mild CTBI group scored in the borderline range for externalizing symptoms six months post-CTBI; however, all other mean scores were within the normal range. Over a period of 16 years, young adults with CTBI showed similar developmental trajectories regarding psychosocial outcomes, compared with healthy controls. This study confirmed previous literature that CTBI is associated with increased levels of psychosocial problems.
Introduction
C
The transition from childhood to adolescence to adulthood can be stressful, and the rates of developing psychological and social impairments are higher during these developmental periods. 5 –8 For children and adolescents with a TBI, these transitions are particularly challenging, and the rates of new psychological and social impairments in this group have been reported to be elevated in association with physical and cognitive difficulties. 9
Beauchamp and Anderson 10 –12 argue that intact social skills rely on normal maturation of the brain and the development of cognition and behavior within a supportive environment. Internal and external influences related to the child and their environment, the child's brain development and integrity, and their current (cognitive) abilities (attention, communication, executive function, social cognition) interact and define the behavioral and neural base for social and psychological well-being. Max 12 has extended this model, adding a “permeable layer” of behavioral and psychiatric symptoms to broaden its application to psychopathology. Combining these two approaches provides a comprehensive model for psychosocial recovery after childhood brain insult (Fig. 1).
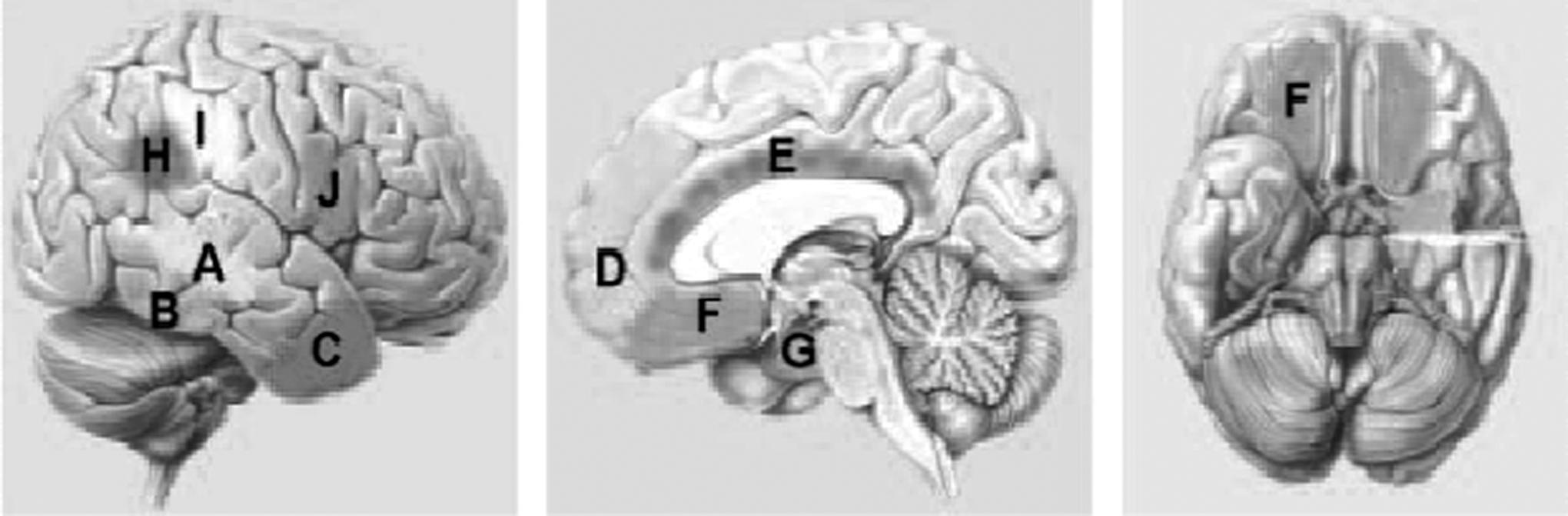
Brain regions contribution to the social network:
For the purpose of this study, and taking into account the above conceptual frameworks, 10,11 psychosocial outcomes have been divided into social skills and psychological symptoms. Social skills are defined as “the ability to think about the social world and to contemplate ways and means of navigating the social environment,” 13 while psychological symptoms refer to those attributed internally (towards the self; depressive, anxious, withdrawn) and externally (towards the outside, such as other people or the environment; aggression, rule-breaking behavior). 14
Existing research has shown that following CTBI, children and adolescents demonstrate greater social and psychological impairments than peers, 15 –20 including lower self-esteem, fewer friendships, and more maladaptive, aggressive, and antisocial behavior, with poorer emotional and behavioral regulation. Further, when facing a social problem, children with CTBI tend to respond more aggressively, using avoidant or irrelevant solutions, compared with typically-developing children. 21 –24 Over time, these symptoms and behaviors can become more severe and may lead to secondary psychiatric disorders. 25,26 In addition, adolescents with CTBI have a 49% risk of developing any kind of psychiatric disorder, such as depression, 27 anxiety, 28 attention-deficit/hyperactivity disorder (ADHD), 29,30 conduct disorder, 31 and manic or hypomanic episodes, 32 compared with a risk of 13% for children and adolescents without CTBI. 26
In the TBI field, psychosocial well-being has received greater consideration over the last decade, and it has become apparent that children and adolescents with a CTBI are at higher risk of developing social and psychological impairments. To date, however, most research in the psychosocial domain is retrospective and cross-sectional or has investigated short-term outcomes up to five years, with few prospective longitudinal studies. Further, little is known about the long-term developmental trajectories of psychosocial functioning in this population. This study aimed to extend current research by investigating long-term developmental trajectories of social and psychological function and the influence of severity post-CTBI. We report on data collected from the acute stage to 16 years post-injury. It was expected that young people with more severe CTBI would demonstrate poorer social outcomes and more internalizing and externalizing behavior symptoms, while typically developing controls would show stable development of these skills over time.
Methods
Participants
The participants in this prospective, longitudinal study were recruited between 1993 and 1997 and were identified from consecutive acute admissions to the neurosurgical ward at the Royal Children's Hospital in Melbourne, Australia. 33,34 The children were included if they were aged from 1 year to 7 years and 11 months at time of injury with evidence of CTBI, including altered consciousness and sufficient information to determine injury severity in medical records. The children also were required to be able to complete the study protocol and speak English. Children with a non-accidental, penetrating, or previous TBI, or pre-existing diagnosis of neurological, developmental disorder, or mental health problems, (e.g., ADHD or autism spectrum disorders) were excluded. Initially, 109 children were approached; seven children were excluded due to having pre-existing neurological disorders (n=2), previous head injury (n=1), or an inflicted head injury (n=4). One child had sustained such a severe injury that he was not able to complete the study protocol. Another five families decided not to participate due to time or travel issues, leaving an original sample of 96 participants with CTBI at the acute time-point. These families were followed up at six months, five years, 10 years, and 16 years post-injury.
A control group of 35 healthy children was recruited concurrently via preschools and childcare centers within the communities of the children with CTBI to match for age, gender, socio-economic status (SES), and pre-injury characteristics. These children were followed up at the same time-points as the children with CTBI. Children were included in the control group if they were between the ages of 1 year to 7 years and 11 months, able to complete the protocol, able to speak English, and had no previous TBI or pre-existing diagnosis of neurological, developmental disorder, or mental health problems.
Due to attrition, there were some missing data for questionnaire variables at most of the time-points. Twenty-one families with children who sustained a CTBI and six families from the control group who consented to 16 years of follow-up did not complete any of the time-points. Therefore, 75 children in the CTBI group and 29 children in the control group were included in the analyses. Characteristics of both the included and excluded participants in the group with CTBI and the control group are displayed in Table 1.
p<0.05 - with a lower score representing better SES.
SES. socio-economic status.
Measures
Demographic and injury related information
Details of the participants' medical and developmental history, parent occupation, and family constellation at time of injury were collected during the acute phase for the CTBI group. Injury information (Glasgow Coma Scale [GCS] score, length of coma, neurological signs, and surgical interventions) were collected from the medical records. The severity groups were determined by combining the following information: mild TBI (n=9)—GCS score on admission of 13–15, no evidence of mass lesion on computed tomography (CT)/magnetic resonance imaging (MRI) scans, and no neurologic deficits; moderate TBI (n=19)—GCS score on admission of 9–12, and/or mass lesion or other evidence of specific injury on CT/MRI, and/or neurological impairment; and severe TBI (n=8)—GCS score on admission of 3–8, and mass lesion or other evidence of specific injury on CT/MRI, and/or neurological impairment.
Environment
Two questionnaires were used to measure environmental factors. To assess proximal factors (family function), the Family Functioning Questionnaire 35 at time of injury was used to measure family functioning. This questionnaire consists of 30 items rated on a 6-point scale (1=totally agree to 6=totally disagree). From these 30 items, three factors were derived: conflict, intimacy, and parenting style. A higher score on the scales represents poorer functioning. To assess distal factors (socio-economic status [SES]), Daniel's Scale of Occupational Prestige 36 was used at the time of injury to rate the parent's occupation on a 7-point scale, with a lower score representing higher SES
Intervention and medication use
Information on intervention and medication use, previously and ongoing, was obtained via a demographic questionnaire capturing both parents and the participants ratings at the 16-year time-point. Parent and participant ratings were combined as parents provided more accurate ratings regarding medication usage during the participant's childhood; however, the young adult was more reliable as an adult source of usage.
Primary outcomes
Outcomes were assessed at five time-points. During the acute time-point, parents rated their child's pre-injury psychosocial functioning (baseline). At the later time-points, ratings reflected the child's current functioning. Due to age differences across the duration of the study, the questionnaires used for children during the acute, six months post-injury, and five years post-injury follow-ups differed from those completed at the 10- and 16-year follow-up. Table 2 shows which measures were used at each time-point to assess social adjustment, and internalizing and externalizing symptoms.
VABS, Vineland Adaptive Behavior Scale; ABAS, Adaptive Behavior Assessment System; PIC-R, Personality Inventory for Children-revised, BASC; Behavior Assessment Scale for Children; ABCL, Adult Behavior CheckList.
Social outcomes
To measure social skills, the Vineland Adaptive Behavior Scale (VABS) 37 and the Adaptive Behavior Assessment System, second edition (ABAS-II) 38 were used. Both questionnaires measure adaptive behavior via parent report. The VABS and ABAS have a correlation of 0.78. 38 Both measures compute a ‘social domain (mean=100, SD=15), which was used to compare social outcomes between the group with CTBI and controls at the different time-points. Higher scores reflect better social function, with a score of 85 and below indicating impairments in social functioning.
Psychological outcomes
Internalizing and externalizing symptoms were measured using the Personality Inventory for Children—Revised (PIC-R), 39 the Behavior Assessment Scale for Children (BASC), 40 and the Adult Behavior Checklist (ABCL). 41 The PIC-R, BASC, and ABCL all include an internalizing and an externalizing domain. For the PIC-R, these scales are derived internalizing/somatic symptoms and undisciplined/poor self-control, and measure equivalent constructs of the internalizing and externalizing scales to the BASC and ABCL. All three questionnaires employ T-scores, with a mean score of 50 and standard deviation of 10 for these domains. A score between 60–64 was considered borderline and a score above 65 was considered to fall within the clinical range for the overall internalizing and externalizing scales. 39 –41 Higher scores represent more behavioral dysfunction. The PIC-R and BASC have a correlation between 0.12–0.56, and the BASC and CBCL (child version of ABCL) have a correlation between 0.31–0.92. 39 –41
Procedure
This study was approved by The RCH Human Research Ethics Committee. During the acute stage of this study, participants were recruited from The Royal Children's Hospital following admission for a CTBI, and the control participants were recruited via advertising at preschools and childcare centers. The families were re-invited to participate six months, five years, 10 years, and 16 years post-injury. During these time-points, the primary caregiver completed questionnaires and the child was assessed on their neurocognitive abilities. Once the children entered adolescence and young adulthood, they also completed some self-report questionnaires. For this study, the questionnaires completed by parents measuring psychosocial functioning were analyzed.
Statistical analyses
The analyses were conducted using SPSS (version 20). 42 To compare the participating and non-participating groups with and without CTBI, and to compare the participating group with and without CTBI for confounding influences, an independent t-test and chi-square were conducted.
Due to the attrition and missing data, a linear mixed model 43 was used to investigate the differences in the trajectory of social skills, internalizing symptoms and externalizing symptoms between the group who sustained a CTBI and the typically developing control group. To model the trajectory of outcomes, an unconditional growth curve model with an unstructured covariance matrix was employed. Preliminary analysis (Table 3) showed that the two groups differed on pre-injury SES. For this reason SES was employed as a covariate in the linear mixed model.
p<0.05, with a lower score representing better SES.
Use of medication and utilization of interventions were only included if they were related to psychosocial problems; including psychostimulants, antidepressants, antipsychotic for medication and psychologist, occupational therapy, speech therapy, cognitive remedial, social work as interventions.
M, mean; SD, standard deviation; SES, socio-economic status.
Results
Current sample
A comparison of the demographic characteristics of the participants with CTBI and the control group (Table 3) showed no group differences for gender, age or pre-injury adaptive, family functioning, medication use and utilization of interventions. For the severity groups, the time since injury did not differ significantly. The groups did differ in pre-injury SES, with the control and mild CTBI groups having a higher SES than the moderate and severe CTBI groups. Therefore, SES was used as a covariate in further analyses.
Psychosocial trajectory
Figures 2, 3, and 4 show the developmental trajectories of social skills, internalizing symptoms, and externalizing symptoms across the acute, six month, five year, 10 year, and 16 year time-points post-injury.
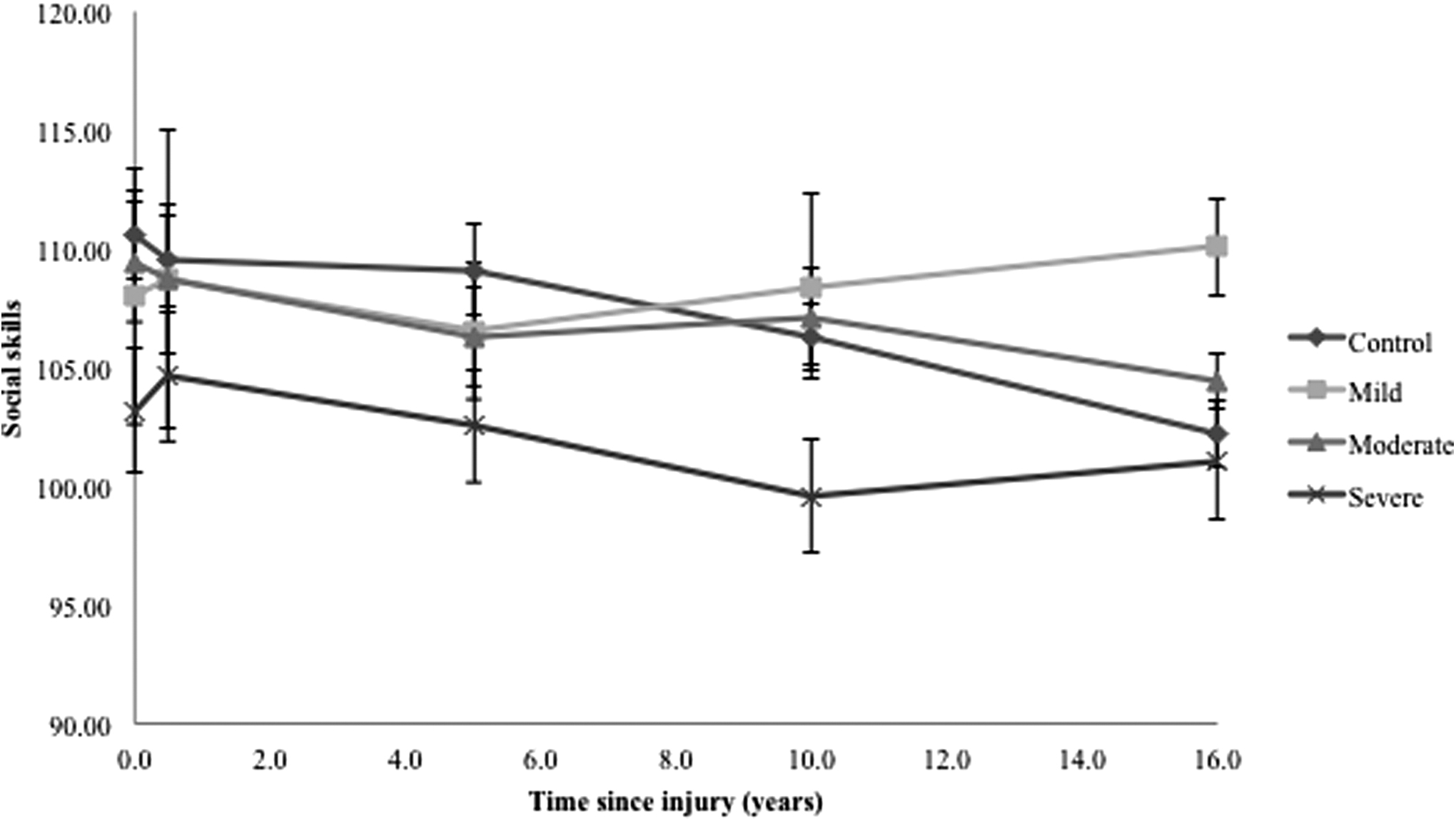
Social developmental trajectory of the group with childhood traumatic brain injury (TBI) and controls. A higher score indicates increased problems.
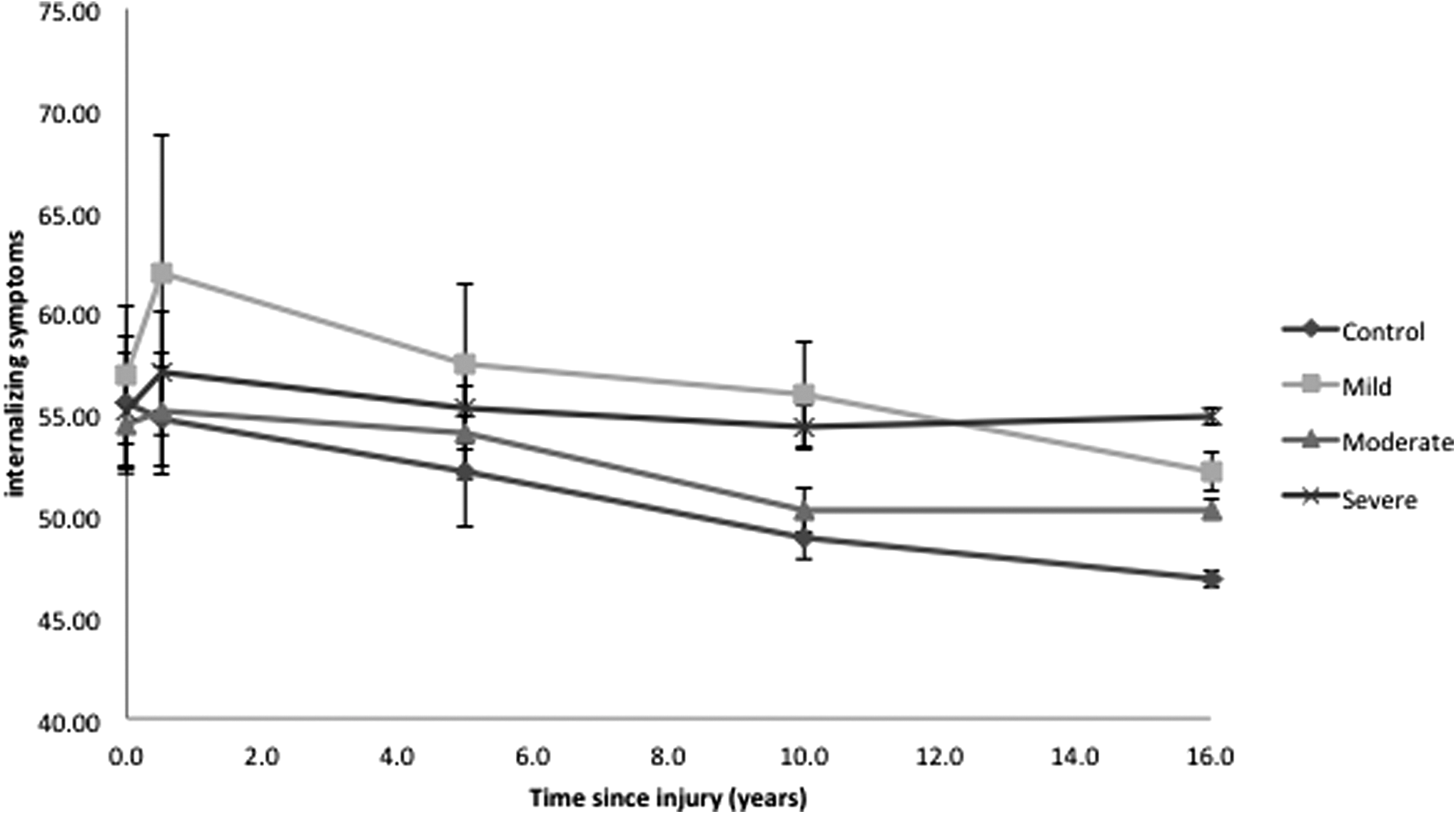
Internalizing developmental trajectory of the group with childhood traumatic brain injury (TBI) and controls. A higher score indicates increased problems.
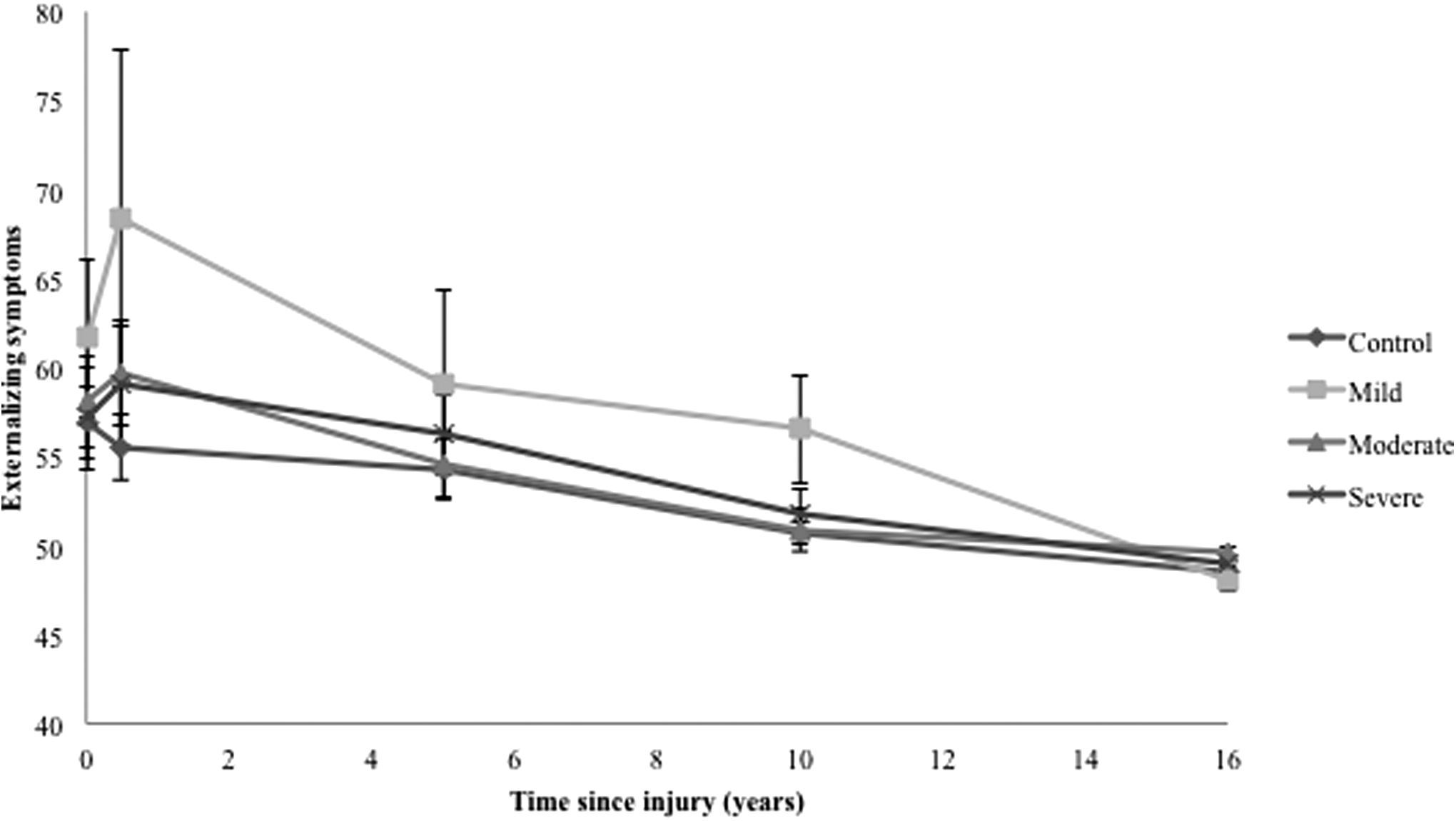
Externalizing developmental trajectory of the group with childhood traumatic brain injury (TBI) and controls. A higher score indicates increased problems.
Figure 2 shows that the severe group demonstrated lower levels of social skill development, compared with the mild, moderate, and control groups. Nevertheless, these group differences were not found to be significant (F [3, 80.04]=0.58; p=0.629). No significant main effect of time (F[1, 56.69]=2.14; p=0.149) and no interaction effect (F[3, 54.78]=0.51; p=0.675) was found.
Figure 3 shows the developmental trajectory of the internalizing symptoms. Pre-injury, all groups reported a similar level of internalizing symptoms; however, the mild group showed a marked increase at six months. No significant group effect was found (F[3,106.16]=0.18; p=0.910) but there was a significant time effect, with higher internalizing symptoms in the CTBI groups at the six-month time-point and a decrease after six months (F[1, 381]=4.23; p=0.040). The interaction effect of the groups x time differences was not significant (F[3, 374.82]=0.67; p=0.574).
Figure 4 shows that the mild group reported higher levels of externalizing symptoms, compared with the other groups, especially six months post-injury. A time effect was detected for the development of externalizing symptoms (F[1, 248.50]=14.44; p<0.001) with the highest scores of externalizing symptoms for the CTBI groups at the 6-month time-point and a decrease after 6 months. No interaction effect was present (F[1, 30.33]=0.09; p=0.77), the group differences were not significant (F(3, 100.11)=0.52; p=.671), and SES effects were non-significant (F[1, 62.26]=0.16; p=0.690).
Discussion
The current study aimed to investigate the developmental trajectory of psychosocial outcomes for survivors of CTBI from the time of injury into adulthood.
As hypothesized, the young adult survivors with more severe CTBI showed a trend of lower levels of social skills development. The mild CTBI group showed higher levels of internalizing and externalizing symptoms between six months and 10 years post-injury. Despite the time effect for internalizing and externalizing symptoms being significant, these levels do not differ significantly, compared with the other groups over time. Further, SES did not systematically influence the results. Of particular importance, mean levels of social skills, and internalizing and externalizing symptoms for all the severity and the control groups fell within the average range.
Social skills
As expected, the severe CTBI group did seem to report somewhat lower levels of social skills, compared with the other groups. Interestingly, there were no distinct trajectory pattern differences between groups. All the groups were reported as having average to high average social skills. It may be that the participants that do decide to be involved in research are more willing to help others, and may therefore demonstrate better social skills. Further, the severe group had a lower baseline level of social skills, compared with the other groups. Confirming existing research, 44 there is a relationship between lower social skills and more severe CTBI, however, this relationship might be directional. As this effect was not significant, this relationship is only speculative.
Internalizing behavior symptoms
Survivors of mild CTBI group displayed more internalizing symptoms than other groups, although all the groups had similar psychosocial trajectories over the 16-year period. This trajectory of internalizing symptoms in the mild CTBI group is noteworthy, and possibly reflects the stress experienced by adolescents associated with the physical, biological and interpersonal changes during this developmental stage, 5 –8 on top of their existing difficulties. The elevated levels of internalizing symptoms continuing into adulthood may indicate that this stress extends following the transition into adulthood, when young people become increasingly independent and move from school to work.
Externalizing behavior symptoms
While there was no significant group difference or interaction effect for externalizing symptoms, there was a main effect of time, with the same pattern as described for internalizing symptoms. The CTBI groups had an increase of symptoms from pre-injury to six months post-injury, followed by a decrease of symptoms, while the control group had a gradual decrease over time at all time-points. The increase may reflect the acute period of adjustment or post-traumatic stress symptoms. All scores fell within the normal range; however, the mild CTBI group did score in the borderline range at the six-month post-injury time-point. This may indicate that they have an increased risk of developing more severe symptoms or disorders if they are not identified and addressed early.
Overall, there was no significant difference between the groups on levels of social skills, internalizing symptoms and externalizing symptoms over a period of 16 years. The elevated internalizing and externalizing symptoms in the mild CTBI group six months following their injury is congruent with existing research that up to two years following their injury, children with CTBI were at risk of developing internalizing (e.g., depression, anxiety) and externalizing (aggressive behavior and conduct) disorders. 45,46 However, in the current study, these differences were not found in the long-term. This might suggest that following a CTBI, the majority of the children do catch up on their psychosocial development. Further, all groups have been followed up intensively, and were provided with detailed reports of their performance and referral to additional intervention or support if needed. Therefore, it may be suggested that our participants (across all groups) did receive early intervention that may have reduced or prevented symptoms.
Limitations
Sample
As this is a prospective, longitudinal study, attrition and sample bias are potential risks. Some participants and their families declined participation due to work commitments, travel distance, or current life events; however, analysis of participating and non-participating families indicated no systematic differences, with the exception that the non-participant group had lower SES. Further, we used a linear mixed model, in which it is possible to predict the expected value of the missing data; however, this still may have influenced the levels of psychosocial outcomes.
Measures
A further challenge for child longitudinal studies is the lack of measures relevant across childhood into adulthood. We specifically chose measures with robust psychometric properties and correlations, but regardless, the use of different measures for social skills, internalizing, and externalizing symptoms at each time-point should be considered when interpreting findings. Further, the source of information—proxy-report completed by the parent—also may affect the level of reported social skills and internalizing and externalizing symptoms. In younger children, it may be argued that parents have the greatest opportunity to observe their child's psychosocial functioning; however, during adolescence and early adulthood, as young people become more independent and relationships with friends become more prominent, parents are possibly less knowledgeable about the young person's psychosocial status.
Nevertheless, Green and colleagues 47 reported that during adolescence there is a fair-to-excellent agreement on psychosocial functioning between the adolescent with a CTBI and their parent. In contrast, Rosema and colleagues 48 showed that during the transition into adulthood, the young adult with CTBI did agree with parent report on the more observable behaviors, such as drug and alcohol use, social and communication skills, however, they did not concur on levels of internalizing symptoms such as anxious/depressed symptoms, withdrawal and thought problems.
Clinical implications and future research
While the groups with CTBI and the control group did not generally differ in their pattern of psychosocial development, survivors of mild CTBI showed a trend for higher levels of internalizing and externalizing symptoms, while survivors of severe CTBI showed a trend for decreased social skills, compared with the other groups. Consistent with previous research, 1 –4 individuals with CTBI had an increased risk of developing psychosocial symptoms and disorders, such as loneliness, depression, anxiety, and rule-breaking behavior, associated with decreased social participation and quality of life. It is important that following CTBI, children and adolescents are more regularly monitored so increased levels of psychosocial symptoms can be detected early, and intervention can be implemented to prevent these individuals from developing more severe symptoms and disorders. Future research investigated risk and protective factors may be helpful in monitoring and preventing these symptoms.
Conclusion
In the current study, young adult survivors of all CTBI severities demonstrated developmental trajectories largely in line with the normal expectations for social and psychological function. The mild CTBI group had higher levels of internalizing and externalizing symptoms at the six months post-injury time-point, compared with the other groups, with an “at risk” level for externalizing symptoms. However, during the transition into young adulthood, the mild CTIB group caught up in their psychological development. Further, the severe CTBI group showed lower levels with regard to their social skills trajectory, from the baseline into the transition of young adulthood. Even though the symptom levels fell within the normal range as a group, it is important to monitor individuals appropriately to prevent them from developing more severe symptoms or disorders.
Footnotes
Acknowledgments
This study was supported by the Victorian Neurotrauma Initiative (VNI), a National Health and Medical Research Council (NHMRC) Fellowship (to V.A.), a NHMRC Career Development Award (to C.C.), and the Victorian Government Operational Infrastructure Scheme.
Author Disclosure Statement
No competing financial interests exist.