
Abstract
The capability of quickly (as soon as possible) producing fast uncorrected and accurate isometric force impulses was examined to assess the motor efficiency of patients with moderate to severe traumatic brain injury (TBI) and good motor recovery at a clinical evaluation. Twenty male right-handed patients with moderate to severe TBI and 24 age-matched healthy male right-handed controls participated in the study. The experimental task required subjects to aim brief and uncorrected isometric force impulses to targets visually presented along with subjects' force displays. Both TBI patients and controls were able to produce force impulses whose mean peak amplitudes varied proportionally to the target load with no detectable group difference. Patients with TBI, however, were slower than controls in initiating their responses (reaction times [RTs] were longer by 125 msec) and were also slower during the execution of their motor responses, reaching the peak forces requested 23 msec later than controls (time to peak force: 35% delay). Further, their mean dF/dt (35 kg/sec) was slower than that of controls (53 kg/sec), again indicating a 34% impairment with respect to controls. Overall, patients with TBI showed accurate but delayed and slower isometric force impulses. Thus, an evaluation taking into account also response time features is more effective in picking up motor impairments than the standard clinical scales focusing on accuracy of movement only.
Introduction
A
Neurophysiological evidence indicates that patients with TBI show a deficit in their movement-related cortical potentials. Di Russo and colleagues 6 recorded flexion movements of the index finger of the left or right hand in two (alternating and repetitive) self-paced conditions in patients with TBI and healthy controls. In the patients, the motor preparation expressed by the Bereitschaftspotential (occurring about 2 sec before response in controls) was greatly reduced, and no difference between the alternating-repetitive conditions was detected (source analysis indicated the supplementary motor area [SMA] as the likely generator for this preparatory component). By contrast, only small differences were present between the two groups for the negative slope and motor potential components produced by pre-motor and motor areas and no difference for the reafferent positivity component arising from somatosensory areas.
This pattern of results indicates a selective deficit in motor preparation and a relatively spared pattern of activation during and following movement in these patients. Wiese and colleagues 7 found reduced and delayed Bereitschaftspotential during self-paced abductions of the right index finger in TBI patients with frontal cerebral damage. This pattern was associated with a reduced contribution of the (left) pre-motor cortex and an enhanced contribution of the postrolandic cortex ipsilateral to the movement. They proposed that the deficit in the Bereitschaftspotential results from deranged neuronal input from the pre-frontal cortex into the pre-SMA. Further, the enhanced motor potentials during movement execution were ascribed to the need for attentional resources to carry out movement. 7
Indeed, in analyzing responses under time constraints, it must be considered that attentional problems are a key deficit of patients with moderate/severe TBI (for reviews see 8,9 ). In particular, they show delayed reaction times (RT) to attentional laden tasks (e.g. 10 ). It is generally held that these deficits are cognitive in nature; e.g., patients with TBI show impaired RTs even after movement times are controlled for. 11 Impaired motor function, however, may contribute to the slowness of patients with TBI in RT tasks. In the study by Gray and associates, 12 patients with TBI performed relatively well on various neuropsychological tests but had slow motor speeds and RTs to simple and complex discriminations, indicating subclinical bradykinesia. Incoccia and colleagues 13 separately measured reaction and movement times in an alertness and go-no go tasks. Apart from delayed RTs, movement times were slower in patients with TBI for both tasks. Impaired movement times were also reported by Shum and coworkers 14,15 in two studies based on the Sternberg additive factor paradigm.
It has been proposed that the response slowness of patients with TBI is quite general—i.e., it similarly affects responses to a large variety of tasks if performed under time constraints. 10 Thus, van Zomeren and Brouwer 9 hypothesized this deficit to be similar to the response slowing observed in the case of normal aging. 16 In this vein, the performance of TBI patients in a variety of timely tasks is delayed by a multiplicative factor (about 1.5) with respect to that of controls. 17,18 This delay is quite similar to what is found when old persons are compared with young adults. 16,19 This is not to say that aging does not produce specific effects in selective cognitive functions (such as dual tasking or global task-shifting), but that a global factor accounts for a very large proportion of the slowing shown in the elderly. 20,21 Similar considerations can be applied to the case of TBI; a discussion of the interplay between global and specific components in the attentional deficit of patients with TBI is presented in Bashore and Ridderinkhof. 17
Recent models of RT performance segregate portions of the response because of decisional and nondecisional processes. 22,23 For example, the difference engine model 22 proposes that the overall response can be separated in two separate and independent compartments, one cognitive and one sensory-motor. It is generally thought that aging affects the cognitive but not (or minimally) the sensory-motor compartment. 16 By contrast, applying the difference engine model, 22 a recent meta-analysis has shown that the slowness of patients with TBI is because of a delay in both the cognitive and sensory-motor compartments. 24 Thus, patients with TBI show a global slowing of RTs that is similar to that of normal aging; however, unlike the effect of aging, a portion of the slowing in patients with TBI can be ascribed to the sensory-motor component of the response. 24
Overall, in spite of the relatively good prognosis for gross motor disturbances, patients with TBI show a variety of fine motor deficits that, together with other comorbidities (such as dizziness, headache, and vision problems) represent challenges to successful return to work. 2 Neurophysiological evidence points to a deficit in motor preparation and a relatively spared pattern of activation during and after movement. This planning problem interacts with the attentional deficits shown by these patients in producing the complex pattern of cognitive slowing that emerges in studies with RT paradigms.
In spite of this growing body of evidence, relatively little is known concerning the actual ability of patients to perform movements precisely and effectively because only a few studies actually carried out an in-depth analysis of the characteristics of movement. Nakamura and colleagues 25 used a motion analysis system to determine movement duration, average speed, and smoothness during reaching in the presumed-to-be-unaffected upper extremities. Patients with brain lesion had longer movement durations, were slower in average speed and had decreased smoothness during reaching. This study included both vascular and TBI patients, but no separate analyses were performed for these two groups so the association of these deficits with TBI cannot be established with certainty.
An effective paradigm to evaluate the characteristics of movement is to examine isometric force responses. Compared with limb movements, they do not depend on the complex relationships between changes in muscle force and length. In addition, they are relatively unaffected by the reflex effects of movement. One effective task requires the observer to produce a single uncorrected impulse of flexor (or extensor) force to match a previous change in the level of a visual target. 26 –28 The examination of transient force impulses minimizes the role of visual feedback in correcting the subject's response. Using this paradigm, variations of the response amplitude are obtained by the observers mainly scaling the rate of rise of force with respect to the target while maintaining constant the duration of force rise, referred to as pulse-height control. 29 –31 Ghez and associates 28 proposed that subjects use target information to scale a common trajectory waveform based on learned sensory-motor transforms to achieve the accurate matching of force.
In the present study, we used the paradigm of isometric force impulses to examine the motor efficiency of patients with moderate to severe TBI who showed good motor recovery at a clinical evaluation. In particular, we examined whether these patients are able to accurately and rapidly match force responses to a visual target. In view of previous data, 28 we focused on conditions emphasizing urgency (i.e., as soon as possible [ASAP] responses) and manipulated the predictability of target forces. We examined both time parameters (i.e., RT to start the response), as well as mean and peak speed (i.e., dF/dt) to reach target force.
Methods
Subjects
Twenty male right-handed patients with TBI (mean age 30.3 years; standard deviation [SD]: 10.8) and 24 age-matched healthy male right-handed controls (mean age 27.9 years; SD: 4.7) participated in the study. All participants signed an informed consent form conforming to the requirements of the local ethics committee.
The inclusion criteria of patients with TBI were the following: (1) moderate to severe TBI with Glasgow Coma Scale (GCS) in acute phase ≤12 with subsequent coma and post-traumatic amnesia (PTA); (2) at the least 3 months from the TBI and at the least 2 months at home; (3) males, age 18–40 years, right-handed; (4) Motricity Index (MI) score ≥85, Fugl-Meyer (FM) score >60, indicating good motor recovery for the right arm (see below); (5) neither proprioceptive deficits nor muscular tonus disorders (spasticity or dystonia) in the right arm; (6) “good recovery” at the Glasgow Outcome Scale (GOS); (7) no visual deficit at clinical evaluation; (8) no language, attention, long-term memory, executive functions deficits at clinical and daily life observations; (9) no medical drugs affecting attention, movement velocity, or planning.
Upper limb motor power was assessed by the MI arm score 32 and by the FM test. 33 The MI (score range 1–100) assesses the motor power of the upper limb. Hand grasp, elbow flexion, and shoulder abduction of the limb (or limbs) are rated. Only the right upper limb was scored here. Five of 20 patients obtained a total MI score of 92 (just a mild loss of force against resistance in one district) while 15 patients achieved the maximum score (individual data are reported in Table 1). The FM score is comprehensive of force, stability, reflex, coordination, speed, and synergies in all the arm sectors (shoulder, elbow, wrist and hand). All patients gained a score ≥62, and 6 of 20 the maximum score of 66 (see individual data in Table 1). Overall, all patients with TBI showed good motor recovery in the right dominant arm.
TfO, time from onset of TBI; GCS, Glasgow Coma Scale; PTA, post-traumatic amnesia. Lesion: R, right, SC, subcortical, L, left, F, frontal, P, parietal, T, temporal, CC, corpus callosum. Motricity Index (maximum score=100) and Fugl-Meyer (maximum score=66) tests refer to the right arm.
Individual data concerning the main characteristics of TBI are reported in Table 1. The time interval from TBI was ≤6 months in three patients with TBI, 6–12 months in three patients, 13–23 months in six patients, and ≥24 months in the last eight patients. All patients with TBI were assessed after at least a 2-month stay at home—i.e., when their neurological status had stabilized and their formal rehabilitation or training programs were finished.
Seventeen of 20 patients had severe TBI (GCS in acute phase ≤8) and 3 from moderate TBI (GCS in acute phase 9-12). Coma duration was <7 days in half of patients and between 8 and 24 days in the other half. PTA duration was ≤4 weeks only in 4 of 20 patients, but in no case ≤2 weeks (Table 1). MRI scans were available in all patients. Location examination revealed bilateral lesions in 11 of 20 patients and subcortical involvement in five patients. Focal involvements are presented in Table 1.
Neuropsychological assessment
All patients were assessed with executive function and attentional tests (individual and group results are presented in Table 2).
ST, short term; RT, reaction time; O, omissions; RS, raw score, ES, equivalent score. Loss=Global performance loss in dual task.
Cutoffs: Go/No-Go and Dual Task: T≤37; Dual Task Omissions ≥6: Matrix. Visuo-Spatial Span. Verbal Span and Wisconsin Card Sorting Test: ES=0; Trail Making Test: A: >93 sec; B >282 sec; B-A >186 sec; Dual Task: % Loss < −20%.
The performance in the Wisconsin Card Sorting Test 34 was within normal limits for all patients with TBI (for this reason, these results are not presented analytically).
As for attention functions, two tests from the computerized Testbatterie zur Aufmerksamkeitsprufung 35 were used: Go/No-Go test and divided attention test.
The Go/No-Go test measures selective attention. We used the five-stimuli version featuring two target and three nontarget stimuli. The subject has to press as quickly as possible the button on presentation of a target and not press it on presentation of nontargets. Main parameters are RTs for correct responses, number of false reactions, and number of omissions. The RTs of patients with TBI were globally good (mean=561 msec, SD=69 msec) and only in 5 of 20 cases were they slow—i.e., below the cutoff (T≤37). Performance accuracy (number of false reactions and omissions) was in the normal range for all patients.
In the divided attention test, two simultaneous tasks (one visual and one acoustic) are given. On the visual task, a series of 10×10 cm matrices are displayed on the screen, each for 2 sec. A matrix consists of a regular array of 16 dots (4×4) with 7 little “x”s superimposed randomly over them. The subject has to press a key whenever four “x”s form a square. On the acoustic task, the subject listens to a continuous series of high (2000 Hz) and low (1000 Hz) sounds (Di-Da-Di-Da, etc.) and has to detect a variation in the sequence (e.g., Di-Di or Da-Da). RTs, number of omissions, and false reactions are taken as measures of subject's performance. The RTs were globally slow (mean=561, SD=69) and in 13 of 20 cases below the cutoff (T≤37). Moreover, the number of omissions was above the cutoff (≤6) in six patients.
Further, we used a number of paper and pencil attention tests: the Attention Matrices, the Short-Term Visuo-Spatial Memory test, and the Short-Term Verbal Memory test from the battery by Spinnler and Tognoni, 36 the Trail Making Test, 37 and the Dual Task test. 38
The Attention Matrices Test assesses selective visual attention. Participants are asked to use a pencil to mark a specific number (1, 2, or 3) in a matrix of 13 lines, each line containing 10 numbers (from 0–9). Three matrices are presented. Performance is assessed by calculating the total number of correct responses made, with a cutoff of 30. Only one patient showed a performance under the cutoff (raw score [RS]≤30, equivalent score [ES]<1).
The Short-Term Visuo-Spatial Memory Test assesses the ability to recall a visuo-spatial pattern of cubes sequencing (Corsi paradigm), immediately after presentation, with a cutoff of 4. Only four patients showed a performance under the cutoff (RS≤4, ES<1). The Short-Term Verbal Span Test assesses the ability to remember an increasing number of words, with a cutoff of 3.5 words. All patients obtained a normal performance.
The Trail Making Test 38 assesses attention, speed, and mental flexibility. The test comprises two parts. The first part (A) requires the participant to draw a line linking numbers, drawn on a sheet of A4 paper, in ascending numerical order. The second part (B) requires the participant to draw a line linking numbers and letters alternately, in ascending numerical and alphabetical order (1, a, 2, b, 3, c, etc.). The participants are asked to perform the two tasks as quickly as possible. Performance is assessed by calculating the difference between time taken to perform tasks A and B, with a cutoff of 186 sec. 39 One patient with TBI was very slow both in parts A and B, and another was slow only in part A.
In the Dual Task Test, each participant performed a digit recall and a tracking task separately and then simultaneously (for instructions of administration and scoring, see
Experimental task
Apparatus
Subjects were seated in a custom-made chair with their right upper arm vertical, their elbow flexed at 90 degrees, and their forearm and hand in a padded metal restraining device mounted on a horizontal support surface at waist level. The forearm was in a neutral position of supination-pronation such that the palm faced medially. An isometric apparatus immobilized the wrist and hand and held the fingers in a comfortable semi-extended position. A custom-designed load cell system combining piezo-resistive sensor and digital temperature compensation was used (model XFL212R-Vi, FGP Sensors Inc, Ephrata, PA). The load cell, centered at the axis of rotation of the wrist, was used to record the forces developed around the wrist in the flexion-extension direction.
The signals from the load cell were amplified and, following analog to digital conversion, acquired on a personal computer, which controlled the experiments. The subject faced a 20" monitor, which displayed the time-course of the force sensor response as a continuous line. The force intensity was represented along the vertical axes and the time along the horizontal one (see black track, Fig. 1). The temporal and spatial correspondences between force display and the force produced by the subjects were highly compatible.

Example of isometric force impulse (black track) in response to predictable targets (gray track) executed by a typical patient.
Task
Subjects were requested to produce brief and uncorrected force impulses, whose peaks were to match the level required by a target visually presented along with subject force display, then to relax to resting level. The target was represented by a red square wave requiring variable intensities (1, 2, or 3 kg) and a fixed duration of 1 sec (the red track, Fig. 1). The interstimulus interval was also fixed at 2 sec. Participants were instructed to respond ASAP to target presentation.
Two conditions were used in separate blocks. In one, the target intensity was predictable (as in Fig. 1) being a fixed sequence (i.e., 1-2-3, 1-2-3). In the second condition, the target intensity was randomized and henceforth unpredictable. Each target was repeated 30 times. The experiment duration was about 30 min.
Data analysis
The following measures were taken and compared between groups and tasks: (1) RTs to targets; (2) peak of force impulse; (3) latency of peak; (4) mean rate of force change from the RT to the peak of force (mean dF/dt); (5) maximum rate of force change (dF/dt). Each set of measures was submitted to a 2×2×3 repeated measures analysis of variance (ANOVA) with group (TBI patients vs. healthy controls) as categorical factor, and task (predictable vs. unpredictable) and load (1, 2, and 3 kg) as repeated measures. For post hoc comparisons, the Tukey honestly significant difference test for unequal samples was used. The alpha level was set to 0.05.
Results
Within a couple of practice sessions, all participants were able to produce force impulses whose mean peak amplitudes matched that required by the targets, as shown in Figure 1.
The peak of the force impulse was proportional to the target load (1.85, 2.32, and 2.85 kg for the 1, 2, and 3 kg target, respectively) and did not differ between groups (F(1,42)<1). The test by load interaction was significant (F(2,84)=5.5, p<0.005): post hoc comparisons indicated that the peak force was greater (p<0.005) in the predictable condition for the 1 kg load only. The other main factors and interactions were not significant.
The time necessary to reach the peak of the force impulse (peak latency) showed a significant group effect (F(1,42)=13.0, p<0.001): peak latency of patients with TBI (64 msec) was greater than that of controls (42 msec). The load factor was significant (F(2, 84)=4.6, p<0.02): post hoc comparisons showed that, for the 1 kg load, the latency (50 msec) of peak was smaller (p<0.02) than that for the 3 kg load (57 msec). The other factors and interactions were not significant.
The maximum dF/dt varied with load (F(2,84)=20.1, p<0.0001) but did not differ between groups (F(1,42)<1). Post hoc comparisons indicated that maximum dF/dt increased as a function of the load (71.4, 90.9, and 110.1 kg/sec for the 1, 2, and 3 kg loads, respectively). All possible post hoc comparisons were significant (p<0.007). Other factors and interactions were not significant.
To further explore differences in motor programming, we focused on comparing patients' and controls' responses to unpredictable targets (Fig. 2). The ANOVA on the RT measures showed that patients' response (504 msec) was delayed (F(1,42)=17.6, p<0.0001) by about 125 msec with respect to controls (379 msec). The test by load interaction was significant (F(2,84)=4.2, p<0.02). Post hoc comparisons indicated that RTs were longer (p<0.005) in the unpredictable condition for the 3 kg load only (430 and 450 msec in the predictable and unpredictable condition, respectively). The other main factors and interactions were not significant.
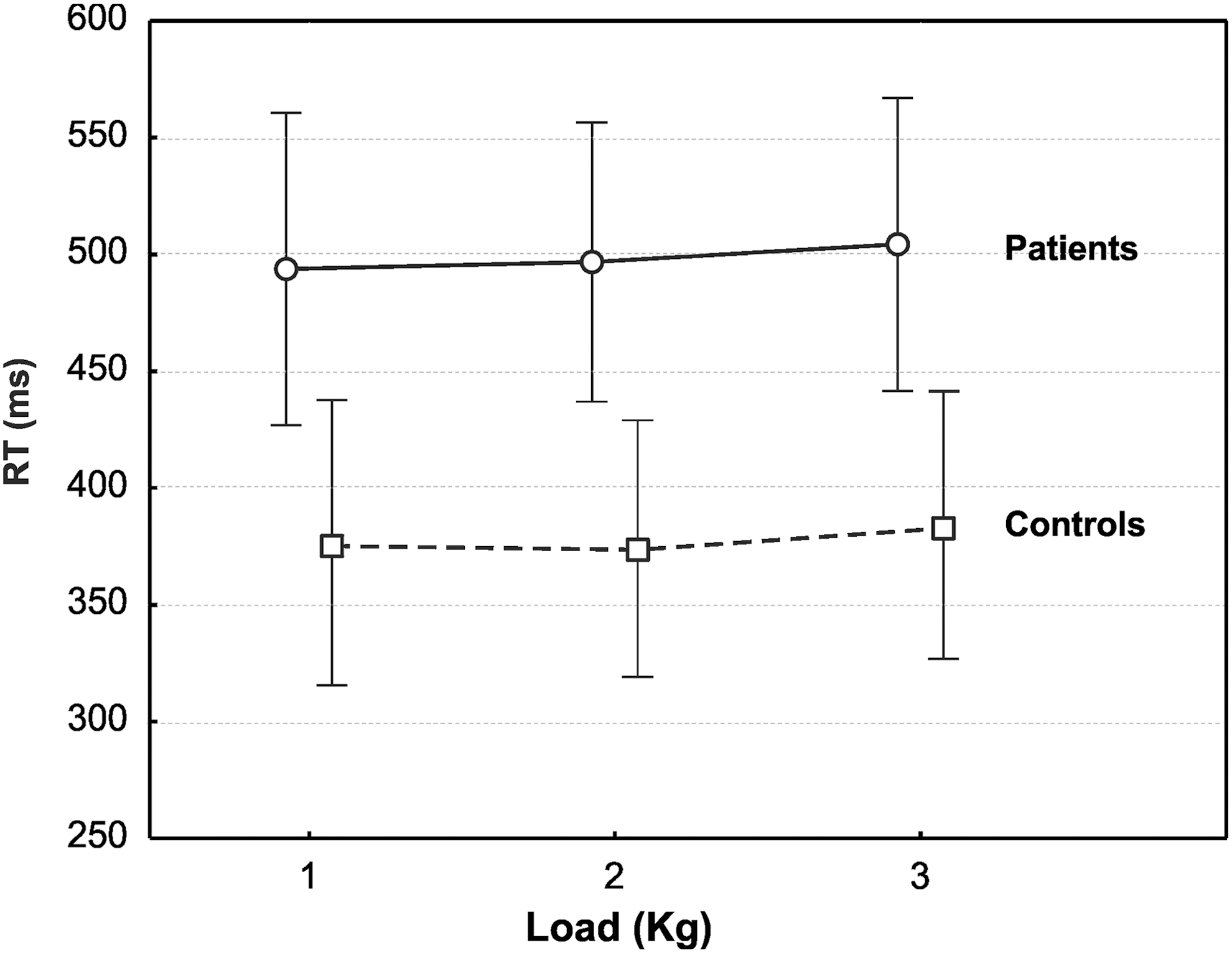
Response time as function of target load for the two groups. Vertical lines denote 0.95 confidence interval.
The ANOVA on the mean dF/dt showed significant effects of the group (F(1,42)=5.0, p<0.05) and load (F(2,84)=29.0, p<0.0001) factors. Further, the interaction between group and load was significant (F(2,84)=5.0, p<0.009; Fig. 3a), and post hoc comparisons indicated that patients' mean dF/dt was slower than controls for the 2 (p<0.05) and 3 kg loads (p<0.01). For the 2 kg load, the mean dF/dt was 35.6 and 54.2 kg/sec for patients and controls, respectively. For the 3 kg load, the mean dF/dt was 39.6 and 62.8 kg/sec for patients and controls, respectively.

(
The ANOVA on the time to peak force showed significant effects of the group (F(1,42)=12.98, p<0.0009) and load (F(2,84)=4.64, p<0.013) factors. The interaction between group and load was marginally significant (F(2,84)=2.95, p=0.058; see Fig. 3b). Others factors and interactions were not significant.
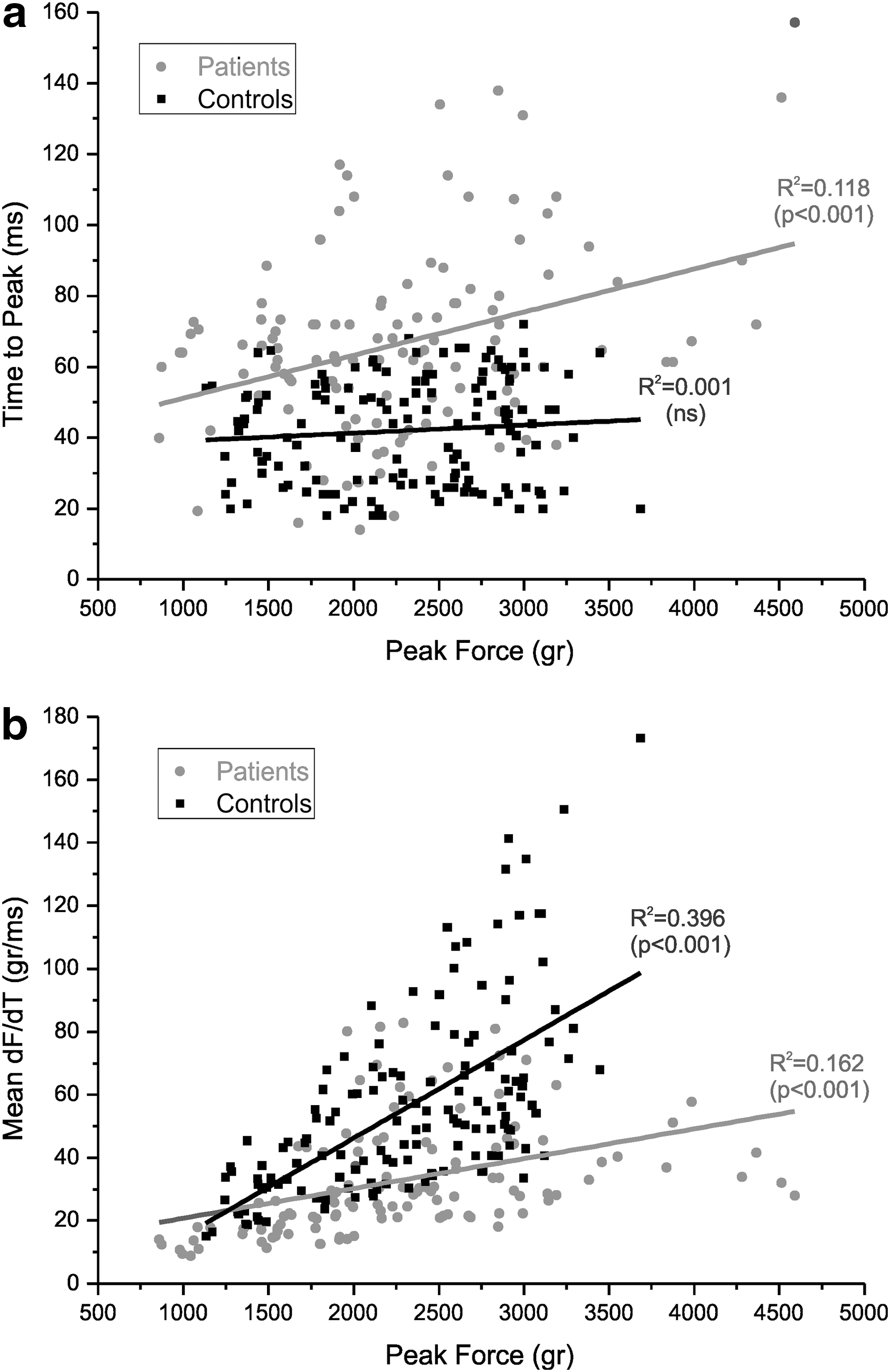
Considering the patients' and controls' dF/dt and time to peak forces differences (Fig. 3), we decided to investigate these parameters in further detail. To this purpose, we ran linear regressions of time to peak force and peak force as well as dF/dt and peak force. As shown in Figure 4a, in patients, the time to peak was positively correlated to the peak force (R2=0.118, p<0.001) while in controls, these two parameters did not correlate (R2=0.001, ns). Figure 4b shows the correlation between the mean dF/dt and the peak force. In both groups, these parameters significantly correlated (p<0.001), but the correlation was stronger in controls (R2=0.396) than patients (R2=0.162).
(
Discussion
In keeping with their relatively good motor recovery, patients with TBI were able to produce isometric force impulses to the targeted weights with a precision comparable to that of age-matched controls. Selective difficulties were also present, however.
First, their RTs were delayed by 125 msec. This finding is in line with the several observations indicating a general slowing of responding present in patients with TBI. 17,18 In the introduction, we have briefly reviewed evidence, which indicates that this delay is probably because of an impairment in both decisional and nondecisional components of the response. 24
Critical to the aims of the present study, patients with TBI were also slower during the execution of their motor response. In particular, they reached the required peak force 23 msec later than controls (corresponding to a 35% delay of responding). Further, their mean dF/dt (35 kg/sec) was slower than that of controls (53 kg/sec); again, the delay points to a 34% impairment with respect to controls. These group differences are small in absolute terms, and the performance of TBI certainly does not indicate the presence of a gross motor defect. The size of the time delay corresponds to a clinical meaningful slowing in the production of the response when compared with normal performance, however.
One could envisage that this basic delay in the production of the response may have widespread effects on the execution of complex activities requiring time-locked integration of multiple actions. In this vein, it has been reported that patients with TBI are impaired in the simultaneous rhythmical movements of hands and feet and in their agility while running in a figure-of-eight. 40 Notably, no delay was detected in the case of peak velocity (maximum dF/dt). A possible reason is the larger variability of this measure than the more stable mean dF/dt. In fact, for these two measures, the group differences were comparable, being 21 and 25 kg/sec for the mean and the maximum velocity, respectively.
The predictability parameter did not exert a detectable effect on any of the parameters considered. Previous research has shown that, in the case in which ASAP responses are required, unpredictable targets generate a constriction in the pattern of responses. 28,41 These cluster around a modal value, with overshooting of small targets and undershooting of large targets. In the present results, such restriction of the range in the responses was clearly detected, even though it was not specific of the unpredictable condition. Therefore, it appears that our predictability condition was not strong enough to induce a clear set of expectancy in our subjects. At any rate, this manipulation did not interact with groups. Therefore, it appears that the group differences in the slowness of the responses are independent of task predictability. At any rate, further research should try to examine more in depth the role of stimulus predictability.
Altogether, these results point to (1) an impaired and therefore longer motor programming time (longer RTs) and (2) an impaired capability of an effective pre-planning, even in the presence of longer programming. Normal subjects use a predominantly height-control strategy by mainly scaling dF/dt to the targets and only minimally modulating time to peak force. Instead, patients with TBI modulate more time-to-peak force and less dF/dt, mainly using a width control strategy. They are still accurate but not as fast as normal subjects are.
The strategy adopted (width control) suggests a possible degradation of the smooth and rapid coordination of movements based on feed-forward commands, typical of neurologically fully normal subjects. Such behavior appears very similar to that already observed in normal aging 42 and probably is present in children in initial stages of motor development. 43
The TBI patients' slowing in initiating and executing a motor response may have important clinical implications. First, it was detected in the chronic stage; thus, it may represent a stable sequela of TBI, although the present data do not exclude that ad hoc rehabilitative interventions may effectively compensate for the deficit (and this remains as an interesting research objective). Second, it represents a relatively isolated deficit; indeed, it was not correlated with other cognitive disorders or with PTA duration. This would call for a specific attention to such deficit in the diagnostic process.
Admittedly, the present procedures may be difficult to implement as such in a clinical setting. Thus, it would be important to develop standard tests for the evaluation of isometric force in patients with TBI. In this vein, evaluation of responses to isometric force impulses may eventually also prove relevant in the quantification of global biological and psychological damage in medico-legal assessments. Above all, subclinical motor slowing may potentially affect the general outcome in coping with several everyday life activities, particularly in the case in which these are performed under time constraints, such as driving.
Overall, patients with TBI showed accurate but delayed isometric force impulses (longer RT and longer time to peak force). This pattern is in keeping with the idea that these patients may perform flawlessly (or at least within normal limits) in standard motor scales that emphasize an accuracy evaluation of movement only. By contrast, an evaluation focusing also on response time features may be more effective in detecting their motor impairment, while motor deficits in patients with TBI may go undetected if only accuracy of the response is considered.
Footnotes
Author Disclosure Statement
No competing financial interests exist.