
Abstract
The purpose of this study was to identify the risk factors related to the hemorrhagic progression (HP) of brain contusion in patients after traumatic brain injury (TBI). Recently, many studies have reported abnormal lipid levels associated with hemorrhagic stroke. Unlike hemorrhage stroke, however, the lipid profiles in patients with TBI have not been examined. Therefore, we evaluated the risk factors of HP in patients with TBI and focused on lipid profiles. Fifty-six patients with TBI with mild to moderate injuries (Glasgow Coma Scale ≥9) who initially did not need surgical intervention were enrolled in this study. Patients underwent repeated computed tomography (CT) scans at 4 h and 24 h after injury. Magnetic resonance imaging (MRI) was performed 7 days after the initial injury. In each noncontrast CT scan, the hemorrhage volume was quantified using the ABC/2 technique. Clinical features, previous medical history, initial CT, and microbleeding on follow-up MRI were analyzed retrospectively. There were 31 (55%) patients in whom significant HP developed (volume >30%). Current smoking (p=0.034), higher initial systolic blood pressure (p=0.035), and lower triglyceride levels (p=0.039) were significantly associated with HP. Current smoking and a triglyceride (TG) level <150 mg/dL were the only statistically significant predictors of HP in the multivariate analysis (p=0.019, p=0.021, respectively). HP with TBI is common in patients who currently smoke and have lower TG levels (150 mg/dL). These patients should be monitored closely, and surgery may be considered before deterioration occurs.
Introduction
H
Recently, many studies have reported abnormal lipid levels associated with hemorrhagic stroke. Unlike hemorrhagic stroke, however, lipid profiles in patients with TBI have not been examined. Therefore, this study focused on lipid profiles in patients with traumatic cerebral contusions to identify the factors that predict HP.
Methods
Patients and protocol
This retrospective, single-center study between March 2011 and February 2013 included patients with mild to moderate (Glasgow Coma Score [GCS] ≥9) head injury with traumatic cerebral contusion hemorrhage confirmed by a CT scan for which surgical evacuation was not planned initially. The study protocol was approved by the Institutional Review Board of the College of Medicine, The Catholic University of Korea (HC14RISI0034).
All patients were admitted to the intensive care unit and treated according to the guidelines for management of TBI. According to our institutional protocol, all patients underwent a CT scan initially in the emergency department and repeated CT scans were performed at 4 h and 24 h after the initial injury. Magnetic resonance imaging (MRI), which included susceptibility-weighted imaging (SWI), was performed 7 days after the initial injury.
Inclusion and exclusion criteria
The inclusion criteria for this study were (1) a small amount of contusion hemorrhage (5∼20 mL) on an initial CT scan that did not necessitate emergency surgery; (2) a time point less than 4 h after the occurrence of head trauma; and (3) follow-up CT scans performed 4 h (mean 266±16 min) and 24 h (mean 1424±47 min) after the initial CT scan. Exclusion criteria were (1) insufficient data; (2) age <18 or >80 years; (3) unclear history of head trauma; (4) severe head injury (GCS <9); (5) the contusion was located in a deep structure, such as the diencephalon, brainstem, or cerebellum; (6) other major organ damage; or (7) known coagulopathy (Fig. 1).
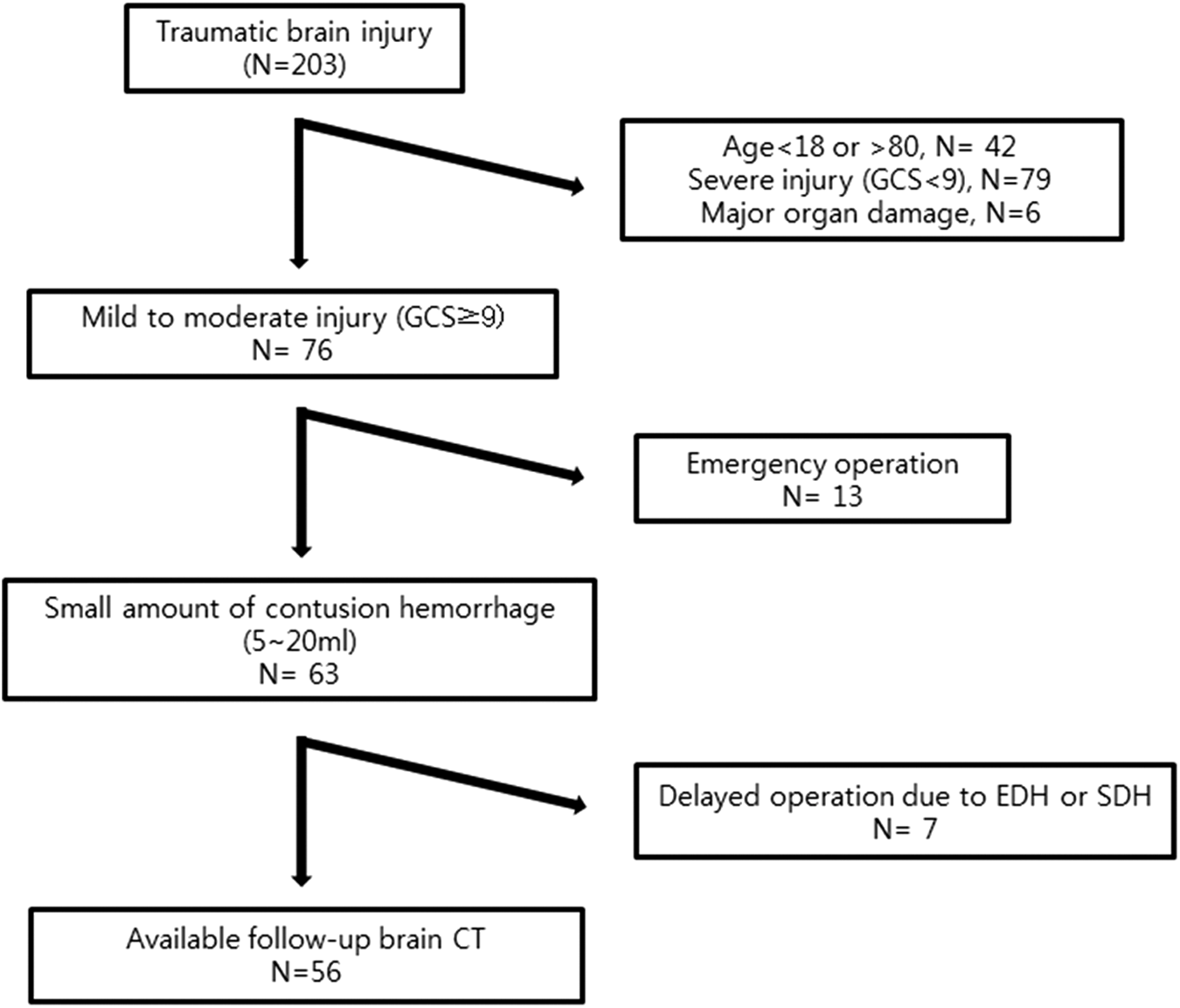
Flow diagram of traumatic brain injury with inclusion and exclusion criteria. GCS, Glasgow Coma Score; EDH, epidural hematoma; SDH, subdural hematoma; CT, computed tomography.
Data collection and radiological assessment
Medical records and radiological imaging studies were reviewed and clinical data were collected. Investigation data included the initial international normalized ratio, prothrombin time, activated partial thromboplastin time, and lipid profiles at the initial emergency department evaluation. In addition, we reviewed the characteristics of the initial and follow-up CT scans and calculated the volume of the contusion hematoma using the formula: ABC/2, where A, B, and C represent the largest dimensions of the hematoma measured at perpendicular angles to one another.
Previous research by CT scan to identify a risk factor for hemorrhage progression has used the same method. 2,4,8 –10 The calculated area of the contusions only included the volume of the frank hemorrhage without the surrounding edema. For heterogeneous multiple contusions, the largest hematoma was measured instead of the entire heterogeneous hemorrhage. An HP was defined as an enlargement of ≥30% of the hematoma size on a follow-up CT scan compared with the baseline CT image. A similar cut-off value was used in previous studies. 1,5,8
SWI was used for the radiological detection of microbleeds. The Microbleed Anatomical Rating Scale was used for the classification of microbleeds. 11 The lobar regions included the cortical and superficial subcortical white matter regions (including subcortical U fibers). The deep regions included the basal ganglia, thalamus, internal capsule, external capsule, corpus callosum, and deep and periventricular white matter. All clinical and radiological data were analyzed by the authors (H.K., 9 years of experience in neurosurgery and S.T.J, 7 years of experience in neurosurgery). Discrepancies were solved by consensus during the research period.
Statistical analysis
The patients were divided into HP and non-HP groups. Categorical variables are expressed as n (%) and continuous variables as the mean±standard deviation when the data follow a normal distribution. Categorical variables were compared with the chi-square test or Fisher exact probability test, and the medians were compared using the Student t test or the Wilcoxon rank sum test. Logistic regression was used to compute unadjusted and multivariable-adjusted odds ratios (OR) for the dichotomous outcome of the HP and non-HP groups. Odds ratios are presented with the associated 95% confidence intervals (CI). The threshold for statistical significance was set at p<0.05. All statistical analyses were performed using SPSS software version 18 (SPSS Inc., Chicago, IL).
Results
A total of 56 patients satisfied the inclusion and exclusion criteria. Of these, HP developed in 31 (55%) patients, whereas it did not in 25 (45%, non-HP). Table 1 lists the baseline clinical and demographic characteristic of both groups. Patient age and initial neurological status were similar in both groups (mean age 59.1 vs. 60.2 years, mean GCS 13.1 vs. 13, p=0.788, p=0.969). The medical histories were similar in all categories except current smoking (12% vs. 39%, p=0.034). The history of drug use (antiplatelet or anticoagulation and statin) was similar in both groups.
SBP, systolic blood pressure; DBP, diastolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; INR, international normalized ratio; TG, triglyceride.
Data are presented as median and n (%).
p value represents comparisons between the nonhemorrhage progression and hemorrhage progression groups using the Fisher exact test and the Wilcoxon rank sum test.
The odds ratio (OR) represents comparisons between the nonhemorrhage progression and hemorrhage progression groups using simple logistic regression.
Patients with HP presented with higher systolic blood pressure on admission (119.6 mm Hg vs. 134.5 mm Hg, p=0.035), and laboratory findings showed statistically significant differences (174.6 vs. 133.8, p=0.039) in triglyceride (TG) levels (Fig. 2). When groups were categorized by a systolic blood pressure (SBP) >140 mmHg and a TG level <150 mg/dL, only the TG level <150 mg/dL group showed a statistically significant difference (36% vs. 65%, OR 3.2, 95% CI 1.07–9.7, p=0.034).
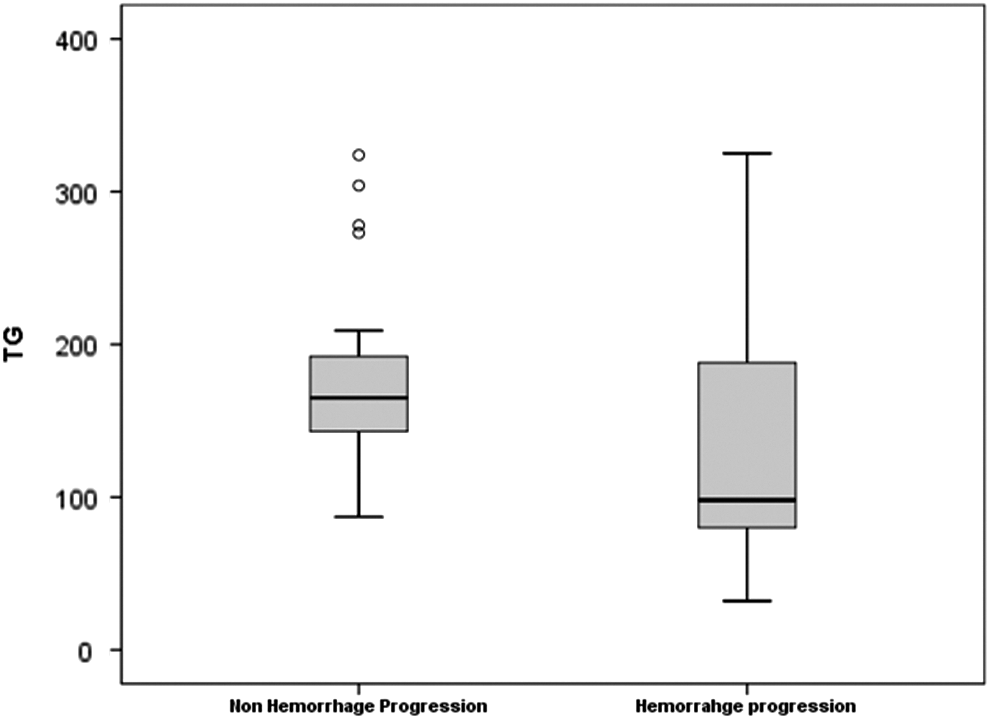
Representative box plot showing distribution of triglyceride (TG) between nonhemorrhage progression and hemorrhage progression group.
Table 2 lists the baseline CT and follow-up MRI characteristics of both groups. The initial contusion amount was not different in both groups (6.6 mL vs. 6.4 mL, p=0.841). The Hounsfield units of hematoma, frontal horn index, and midline shifting did not show any statistically significant differences. In addition, associated injuries (SDH, SAH, skull fracture, and cistern effacement) were balanced across the groups. Microbleeds detected by SWI had a tendency to be higher in the HP group, but did not show a statistically significant difference.
SAH, subarachnoid hemorrhage; SDH, subdural hematoma.
Data are presented as median and n (%).
The odds ratio (OR) represents comparisons between the non hemorrhage progression and hemorrhage progression groups using simple logistic regression.
In the multivariate analysis, two parameters significantly increased the risk of HP: current smoking history (OR 6.37, 95% CI 1.36–29.84, p=0.019) or a TG level <150 mg/dL (OR 4.43, 95% CI 1.25–15.72, p=0.021) (Table 3). The mortality rate was 3.5% (2/56), which occurred entirely in the HP group.
OR, odds ratio; TG, triglyceride.
The OR was adjusted using age and sex.
The p value represents comparisons between the nonhemorrhage progression and hemorrhage progression groups using multiple logistic regression.
Discussion
HP is a common cause of clinical deterioration and a risk factor for poor outcome in patients with TBI. Enlargement of the initial hemorrhage is variable, however, and prognostic factors for HP are numerous and unclear. Several studies have approached this issue to establish an association between risk factors and HP in traumatic cerebral contusion. Initial radiologic findings have shown several factors strongly associated with HP. Large initial hematoma size and concurrent SDH or SAH are suspected risk factors for HP. 2 Recently, the possible association of parenchymal contrast extravasation with HP was raised. 5 In addition, abnormal coagulation and coagulopathy have been associated with HP. 7,12
Although the association between blood lipids and the type of stroke (ischemic or hemorrhagic) is well known, the association between lipid profile and TBI is not clear. 13 Therefore, we focused on several factors, including lipid profiles, that influence HP to provide information on which patients need more intensive care and close observation. Our data show that approximately 55% of patients exhibit hematoma enlargement within 24 h. The prognostic factors that were independently associated with HP included current smoking and a lower TG level.
The findings from this study underscore important clinical findings regarding traumatic contusions. The first point relates to the role of smoking in hemorrhage expansion. Current cigarette smoking is known to be an independent risk factor for both ischemic and hemorrhagic stroke. 14 Mechanisms of ischemic stroke induced by smoking include atherosclerosis, thrombogenesis, and reduced cerebral blood flow as a result of arterial vasoconstriction. 15 –18 In addition, smoking may play a role in aneurysm formation, growth, and rupture. 19,20 Smoking is also a risk factor for intracerebral hemorrhage (ICH), however, and the possible mechanism is unclear.
Increased blood pressure and arterial wall damage appear to affect the intracranial hemorrhage by the rupture of small intraparenchymal arteries. 21 Therefore, current smoking predisposes vessels to fragility, and HP can more easily occur after TBI compared with nonsmokers. In addition, traumatic cerebral contusions have a penumbral zone, which is a pericontusional zone of edema with low regional cerebral blood flow similar to an acute ischemic stroke. 22,23 This lesion will induce a risk for secondary ischemic damage and changes in hemorrhage contusion. Also, smoking may accelerate secondary damage by chronic reduced cerebral blood flow similar to the mechanism of an ischemic stroke induced by smoking.
Second, our results demonstrated that abnormal lipid profiles were associated with the progression of hemorrhage contusion. Low levels of serum total cholesterol have been recognized as risk factors for ICH, and several studies show that serum total cholesterol levels are inversely related to ICH, 13,24 –26 although it is unclear how various serum lipid fractions (low-density lipoprotein-cholesterol, high-density lipoprotein-cholesterol, and TG) are associated with ICH. Some studies suggest that low TG levels play a major role in total cholesterol levels and the risk of ICH. 13,27 In our study, similar to previous studies of ICH, we showed that the HP group had a lower TG level compared with the non-HP group in patients with TBI (133.8 mg/dL vs. 193.2 mg/dL, p=0.043).
Although the mechanism of the association between TG levels and HP in TBI is unknown, there are some possible explanations. Because of cerebral blood flow and metabolism changes, studies have shown that spontaneous ICH and traumatic cerebral contusion may have common mechanisms of injury and secondary effects. 28
First, patients with microbleeds showed low TG levels in smaller studies. 29,30 In addition, an inverse association between TG levels and cerebral microbleeds (CMBs) was found in a large population-based cohort study. 31 Also in our study, the correlation between TG level and CMBs was slightly negative but not statistically significant (r=−0.095, 95%CI; −0.3–0.115, p=0.458) (Fig. 3).
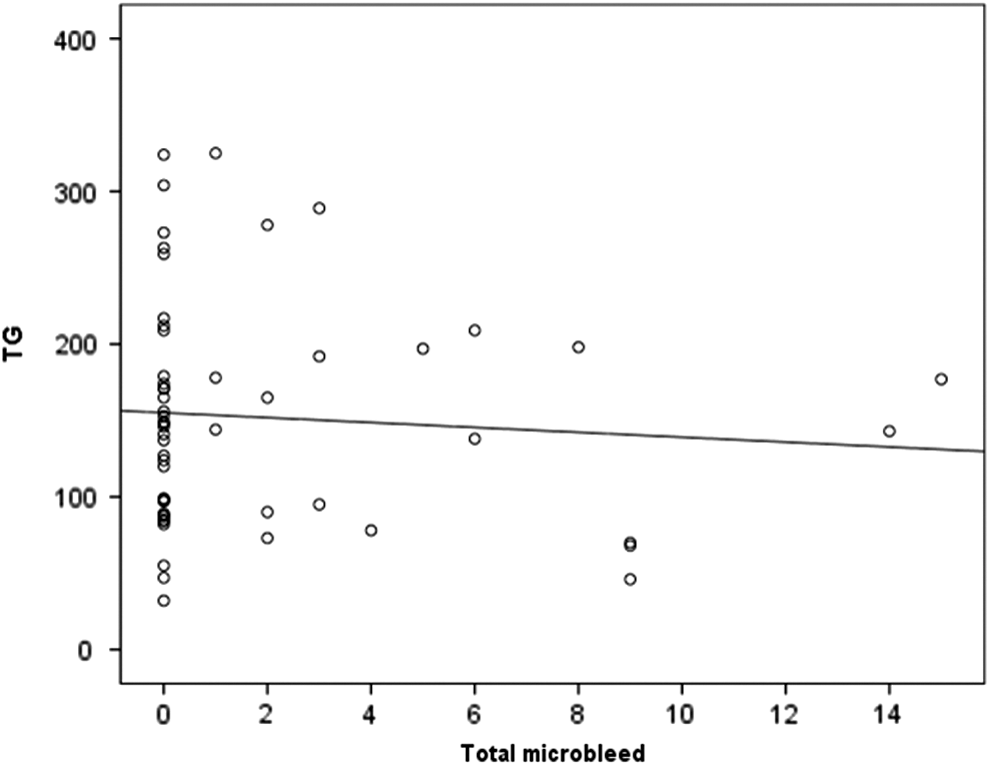
An inverse association between triglyceride (TG) level and the cerebral microbleed (r=−0.095, p=0.458)
Second, low TG levels may represent the fragility of the vascular endothelium. Because cholesterol and fatty acids are essential elements of all cell membranes, low cholesterol levels may contribute to the development of a fragile endothelium, prone to rupture by TBI. 31,32 This may contribute to the development of HP. Last, low TG levels may represent a tendency for bleeding, because TG-enriched lipoproteins are accompanied by elevations in factor VII clotting activity, plasminogen activator inhibitor, and the viscosity of blood. 33
There are several limitations of this study: (1) We used a single center and a small sample size. (2) There was a potential for errors in identifying contusion progression. Given the potential difficulties that can arise with repeated imaging from different angulations of CT scan cuts across the contusion, our data may represent a subset of all patients presenting with brain contusions. (3) We excluded patients whose clinical condition was such that the patient obviously needed immediate surgery for a significant mass effect. (4) We also excluded patients with contusions so small that the involved clinicians judged it unnecessary to repeat the CT scans. (5) Our data are limited to adults and therefore cannot be applied to children with brain contusions. (6) TG levels were not tested after 8 to 12 h of fasting because all laboratory findings were obtained from the emergency department.
Conclusion
Our study demonstrates that abnormal lipid profiles, especially lower TG levels (<150 mg/dL), and a current smoking history are significantly associated with HP in patients with TBI. So, physician awareness of the danger of HP is needed as well as more intensive observation of patients with lower TG levels and current smoking. Further investigation of the pathophysiology and a well-designed control study are needed for more conclusive results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.