
Abstract
Participation in contact sports places athletes at elevated risk for repeated head injuries and is associated with negative mental health outcomes later in life. The current study identified changes observable on neuroimaging that persisted beyond the apparent resolution of acute symptoms of concussion. Sixteen young adult ice hockey players with a remote history of concussion but no subjective complaints were compared against 13 of their teammates with no history of concussion. Participants completed a detailed phenotypic assessment and a neuroimaging battery including diffusion kurtosis imaging and resting-state functional magnetic resonance imaging. Athletes with a history of concussion performed no differently from those without on phenotypic assessment, but showed significantly elevated fractional anisotropy (FA) in the left genu and anterior corona radiata relative to those without. Post hoc analyses revealed that elevated FA was associated with increased microstructural complexity perpendicular to the primary axon (radial kurtosis). Athletes with concussion history also showed significant differences in the organization of the default mode network (DMN) characterized by stronger temporal coherence in posterior DMN, decreased temporal coherence in anterior DMN, and increased functional connectivity outside the DMN. In the absence of deficits on detailed phenotypic assessment, athletes with a history of concussion displayed changes to the microstructural architecture of the cerebral white matter and to the functional connectivity of the brain at rest. Some of these changes are consistent with those previously associated with persisting deficits and complaints, but we also report novel, complementary changes that possibly represent compensatory mechanisms.
Introduction
I
CTE is believed to be caused by repeated mTBI, but it is pathologically distinct from the original injury and is not unresolved concussive symptoms. 3 Although the popular press has focused on the consequences of repeated concussions for professional athletes, approximately 40 million children and adolescents participate in organized sports 12 and sports-related injuries are a leading cause of TBI in persons aged 15 to 24 years. 13,14 Identification of the mechanisms by which concussions incurred early in life contribute to elevated risk for negative outcomes is an important public health issue. 15
Neuroimaging research into sports-related TBI (sTBI) has focused primarily on the acute post-injury period 16,17 and on characterizing the clinical and neuropathological profile of CTE. 3,18 A recent review of neuroimaging findings associated with mTBI 19 has emphasized that the focus on symptomatic groups has “effectively exclude[ed]” (p. 284) the majority of persons who incur mTBI.
In the current study, we investigated changes observable on neuroimaging associated with a history of concussion that persisted beyond the resolution of acute symptoms and may represent the mechanisms by which those athletes who experience concussion are at elevated risk for negative outcomes after another insult and in the coming decades.
Although mTBI is not usually associated with gross neurotrauma, 8,20 two novel neuroimaging methods have been shown to be sensitive to the subtle neuropathology subserving concussion: diffusion weighted magnetic resonance imaging (dMRI) and resting state functional magnetic resonance imaging (rs-fMRI). 21 –25 These measures have been correlated with symptom severity in the acute phase after injury, as well as with cognitive and mood deficits in the subacute period, suggesting they are sensitive to mechanisms of injury and recovery.
dMRI measures the diffusion of water protons, providing an index of white matter (WM) structure and integrity. 26 Fractional anisotropy (FA) measures the directionality of water motion. Persisting cognitive deficits in the chronic phase after TBI have consistently been associated with reduced FA, 19,27,28 which has been interpreted as demyelination or reduced fiber density reducing the efficiency with which water moves through tissue. Although FA can describe changes in WM efficiency, it is insensitive to the mechanisms subserving observed differences. For example, a net elevation in FA is often interpreted as evidence of greater WM integrity, but a reduction in crossing fibers would also manifest as an increase in FA in the presence of axonal destruction and reduced microstructural complexity. 29
We applied diffusion kurtosis imaging (DKI), which supplements assessment of FA with a measure of the degree to which water diffusion deviates from a Gaussian distribution. This measure has been shown to be particularly sensitive to microstructural changes in tissue. 30 Elevated kurtosis parallel to the primary axon (axial kurtosis: K a ) indicates more restricted diffusion along the direction of the primary axon and has been associated with broken and beading axons 31 and with alteration of the endoplasmic structure. 30 Elevated kurtosis perpendicular to the primary axon (radial kurtosis: K r ), however, is sensitive to myelin, increasing with development in children 32 and rat pups, 33 and decreasing with myelin breakdown. 34
rs-fMRI is used to assess functional connectivity between distributed neural networks by identifying regions at which the blood oxygen level dependent (BOLD) signal shows temporal coherence. 35 rs-fMRI describes pervasive, intrinsic neural activity without the imposition of task demands and has been shown to be sensitive to stable measures of cognitive and emotional competence. 36
Previous studies of rs-fMRI in symptomatic patients after mTBI have demonstrated alterations to the organization of the default mode network (DMN). 22 –25 DMN is a well-established network of distributed neural regions and is believed to support introspective, passive mental processes. 37 Typically, activity in DMN is anticorrelated with activity in regions subserving higher order cognitive processes, but in symptomatic patients after mTBI, stronger connections between DMN nodes and inferior parietal and medial prefrontal structures have been reported 22,24 and associated with subjective complaint. 23,25
Previous studies combining rs-fMRI and dMRI in the study of TBI have reported mixed results. In some cases, global reductions in FA in symptomatic patients have been associated with reduced intrinsic functional connectivity (iFC) generally 38 and in the DMN specifically. 39 FA reductions, however, have also been associated with increased iFC within the DMN, 40 which was interpreted as reduced network efficiency.
One previous study exploring regional measures of WM integrity and DMN organization after TBI demonstrated that, in symptomatic patients, the rate of diffusion in the splenium was correlated with the degree of coherence exhibited between an adjacent cluster in the posterior cingulate cortex (PCC) and the DMN. 41 Moreover, the degree of coherence between the PCC cluster and the DMN predicted self-reported anxiety and performance on a cognitive task.
A secondary aim of the current study was to clarify how differences in regional WM integrity and DMN organization are related, and how these metrics relate to subtle neuropsychiatric signs after the resolution of acute concussive symptoms.
We expected that, in the absence of subjective complaints, subtle deficits would be observable on objective neuropsychiatric assessment in those athletes with a remote history of concussion relative to those without. These deficits would be associated with reduced FA and corresponding changes to the microstructural integrity in these regions indexed by increased Ka or decreased Kr. We also predicted that a remote history of concussion would be associated with disruption to the functional connectivity of the brain at rest, manifested in reorganization of the DMN.
Methods
Participants
Twenty-nine males (14 to 23 years) were recruited from a selective ice hockey training camp. For those participants who reported concussion history (n = 16), incidence ranged from one to four (mean = 2.13), and all were at least 3months removed from their most recent concussion (mean = 40.6 months). All participants were deemed fit to play by team physicians, and none reported subjective complaints of post-concussion syndrome.
Phenotypic assessment
Post-concussion symptom scale (PCSS)
PCSS requires participants to indicate on a seven-point Likert scale the extent to which they are currently experiencing each of 22 symptoms, with zero indicating no current experience and six a severe symptom. PCSS was administered via the ImPACT, 42 a computerized concussion evaluation system. Two participants did not complete the ImPACT.
Youth self-report and adult self-report
Participants completed self-report measures from the Achenbach System of Empirically Based Assessment (ASEBA): the Adult Self Report 43 for those aged 18 years and older; or the Youth Self Report 44 for those under 18 years. Each battery comprises 113 behavioral statements, and participants indicate whether they believe each statement to be “Not True,” “Somewhat or Sometimes True,” or “Very True or Often True” of themselves using a 0–2 scale. These measures yield quantitative scores for broadband internalizing (INT) and externalizing (EXT) problems, with higher scores indicating more problems. Raw INT and EXT scores were used in the current study because age was included in all analyses as a covariate. 45 Two participants did not complete the ASEBA measures.
Neuroimaging measures
Image acquisition
Data were acquired at the University of Vermont MRI Center for Biomedical Imaging, which is equipped with a Philips Achieva 3 Tesla scanner. Diffusion-weighted images were acquired using a single shot, spin-echo, echo-planar image (EPI) sequence of 60 contiguous transverse slices of 2.0 mm thickness (TR = 13,000 msec, TE = 87 msec, field of view [FOV] = 240 mm, voxel size = 2 × 2 × 2 mm3). We acquired diffusion weighted b values (1000 and 2000 s/mm2) in 30 uniformly distributed, noncollinear directions and six additional images with no diffusion weighting.
rs-fMRI was acquired during a 10-min scan using a two-dimensional gradient EPI sequence of 33 slices with 4 mm thickness and 0.4 mm gap (transverse orientation, TR = 2000 msec, TE = 35 msec, flip angle = 90 degrees, FOV = 240 mm, voxel size = 3.75 × 3.75 × 4 mm3). One participant did not complete the resting-state scan. A high-resolution (1 mm isotropic) three-dimensional T1-weighted Turbo Field Echo anatomical image was acquired to facilitate spatial normalization.
Image processing
DKI
Diffusion weighted images corrected for movement artifacts and eddy-current–induced distortions using the FSL tool EDDY were passed to the diffusion kurtosis estimator (DKE). 46 DKE models tensor estimation using a linearly constrained linear least squares model, in which the constraints ensure physically and/or biologically plausible tensor estimates. Each participant's FA and kurtosis statistics were pre-processed and aligned to the FMRIB58_FA standard space image (1 mm isotropic) using nonlinear registration in FSL tool tract based spatial statistics. 47
Each participant's standard space FA, Ka, and Kr were projected onto a group-mean FA skeleton (thresholded at FA = 0.2). Voxelwise between group comparison of skeletonized FA maps was implemented in Randomise. 48 Family-wise error was maintained at p < 0.05 using threshold-free cluster enhancement, with 10,000 permutations. 49
To characterize the mechanisms subserving differences in FA, differences in kurtosis parallel to the primary axon (K a ) and perpendicular to the primary axon (K r ) were calculated for those regions at which FA differed between the groups and FA was regressed against kurtosis statistics. Age was included as a covariate in all diffusion weighted analyses.
Resting state fMRI
rs-fMRI data were preprocessed using AFNI 50 and FSL 51 in accordance with the 1000 functional connectomes pipeline 52 comprising motion correction, exclusion of nonbrain voxels, despiking, mean based intensity normalization (in 4D), and coregistration of functional and anatomical images. The time series at each voxel was prepared by band pass temporal filtering (0.01–0.1 Hz), spatial smoothing using a 6 mm FWHM Gaussian kernel, and nuisance signal regression (six motion parameters, signal from WM and cerebrospinal fluid, and the linear and quadratic trends).
Motion was accommodated by confirming that the mean framewise displacement (FD) was not statistically different between the concussed and nonconcussed groups, and including each participant's mean FD as a covariate in all group level analyses. 53 This approach has been shown to accommodate motion artifacts without the reduction in power that results from “scrubbing” frames that contain micromovements. 54 Age was included in all analyses as an additional covariate.
Intrinsic networks of functionally covarying regions were explored using independent components analysis (ICA) implemented using the group ICA for fMRI toolbox (GIFT). 55 Group ICA is achieved by initial data reduction, application of the ICA algorithm, and back-reconstruction for each individual subject. The number of independent components was estimated by the GIFT dimensionality estimation tool and further dimensionality reduction was achieved via principle components analysis at the group level to reduce the number of components to 44. The Infomax algorithm was selected for the ICA, and individual subject components were then back-reconstructed.
The spatial maps of each subject were converted to Z scores and transformed to MNI standard space with a 2 mm isotropic spatial resolution to allow group-level analysis. GIFT allows each of the resultant 44 IC to be compared with a reference DMN template to reduce the subjectivity of network classification.
The component with the highest spatial correlation with the DMN template was selected for each subject. A mask of the sample-specific DMN was created in AFNI using 3dttest++ to conduct a one-sample t test of the subjects' default mode component. The DMN mask comprised positive voxels that passed a voxelwise statistical threshold (p < 0.005) and were part of a larger cluster of at least 616 μL, maintaining family-wise error at p < 0.05.
An independent groups t test was conducted in AFNI in which the normalized correlation coefficient of each voxel with the DMN time series was compared between athletes with concussion history and those without. Within a mask defined by the sample-specific DMN, 3dClustSim was used to determine that a voxelwise threshold of p < 0.005 and a cluster size of 208 μL were required to limit the possibility of false positives to 5%.
Post-hoc exploration of the iFC of those regions showing discrepant coherence with DMN was conducted using seed-based correlation analysis. Specifically, spherical regions of interest (ROIs) of 9 mm diameter were constructed around the voxel that showed the peak difference within those two clusters at which DMN coherence discriminated those athletes with a history of concussion from those without. These ROIs were spatially transformed to each participant's native space; then the time series of the seed ROIs were regressed against the time series of all other voxels in the brain and converted to Z scores.
To allow group level analysis, registration of each participant's Z score correlation maps to a common stereotaxic space was achieved by first registering the participant's anatomical image to the Montreal Neurological Institute 152-brain template (2 mm isotropic resolution) using a 12 degrees of freedom linear affine transformation (FLIRT in FSL), refined using nonlinear registration (FNIRT), 56 and then applying the nonlinear warp parameters to the functional maps. Comparisons between the correlation maps of athletes with concussion history and those without were conducted within a whole brain mask.
The functional significance of differences observed on neuroimaging was assessed by regressing neuroimaging metrics from significant clusters against INT and EXT. To determine whether the effects observed are true for the sample as a whole or whether they represent effects unique to the injury process and may represent risk for future decompensation, additional regressions were performed for those athletes with a history of concussion in which INT, EXT, and the number of reported concussions were regressed against neuroimaging metrics. All p values reported were corrected for multiple comparisons using a modified Bonferroni procedure.
Results
Phenotypic assessment
Those participants with concussion history were older than those without (18.5 vs. 16.8 years: t27 = 2.14, p = 0.042). Univariate analysis of variance, with age as covariate, revealed the groups did not differ on the mean number of self-reported concussive symptoms (3.38 vs. 3.43, F2,24 = 0.03, ns), nor on self-reported symptoms of INT (5.33 vs. 5.50: F2,24 = 0.044, ns) and EXT (7.00 vs. 9.17: F2,24 = 0.032, ns).
Neuroimaging biomarkers associated with a history of concussion
dMRI
Voxelwise analyses revealed two clusters in the anterior WM in which FA was elevated in those athletes with a history of concussion relative to those without (Fig. 1, Table 1). Within these clusters, located in the genu of the corpus callosum and the left anterior coronal radiata (ACR), Kr was also significantly elevated in those athletes with a history of concussion relative to those without. Post hoc analyses demonstrated that, within these clusters, Kr was correlated with FA. Ka did not discriminate between those athletes with a history of concussion and those without in either of the clusters showing FA differences.

Tract-based spatial statistics analyses of group means within the white matter skeleton mask (thresholded at 0.2, green voxels) identified two clusters in which fractional anisotropy was significantly elevated in those players with a history of concussion relative to those without. From left to right, axial slices are taken from z = −11 to z = 5 at 2 mm increments. Significant clusters have been thickened using the FMRIB Software Library “tbss_fill” tool for visualization (red-yellow corresponding to low-high significance). Images are presented in the radiological view where the right hemisphere appears on the left of the image, presented in MNI152 standard space. Color image is available online at
Differences in fractional anisotropy (FA), radial kurtosis (K r) , and the correlations between these metrics within these clusters.
All p values corrected using a modified Bonferroni procedure.
Resting state fMRI
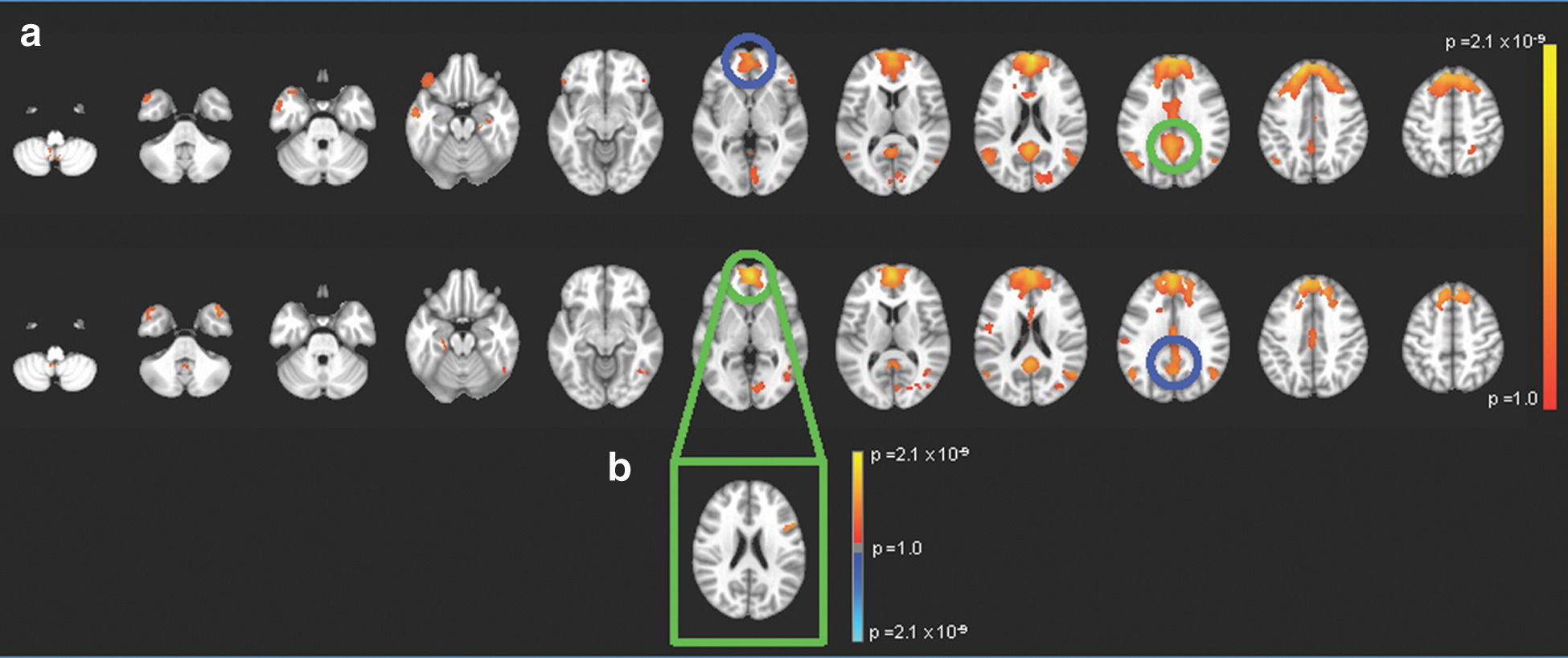
Within the sample-specific DMN mask, one cluster in anterior DMN centered on the right superior medial gyrus showed reduced temporal coherence with the DMN for athletes with concussion history relative to those without (Table 2). A second cluster in posterior DMN, centered on the left precuneus and extending in to the middle cingulate cortex, showed increased temporal coherence with the DMN for athletes with concussion history relative to those without. Figure 2 represents the mean iFC with the sample-specific DMN for those athletes with a history of concussion and those without.
Default mode network
iFC, intrinsic functional connectivity; DMN, default mode network.
All p values corrected using a modified Bonferroni procedure.
Post-hoc analyses of iFC of these regions revealed stronger temporal coherence between the medial frontal seed and a cluster outside of the DMN centered on the left inferior frontal gyrus (IFG: Fig. 2, Table 2) for those athletes with a history of concussion relative to those without.
Relating dMRI and fMRI metrics
We note the spatial correspondence between those clusters at which FA discriminated those athletes with a history of concussion from those without and the clusters in the superior medial gyrus and in the left IFG (Fig. 3) that showed discrepant functional connectivity. The strength of iFC between the DMN and the superior medial gyrus cluster was inversely correlated with K r in the genu (r25 = −0.534, p = 0.017, corrected) and with FA in the ACR (r25 = −0.492, p = 0.028, corrected).

Spatial correspondence between diffusion weighted magnetic resonance imaging and resting state functional magnetic resonance imaging metrics that discriminated those athletes with a history of concussion from those without. Warm colored clusters represent the regions at which fractional anisotropy and radial kurtosis were elevated in those athletes with a history of concussion, thickened using tbss_fill to aid visualization. The darker blue cluster represents the region centered on the superior medial gyrus that showed reduced temporal coherence with the default mode network (DMN) in those athletes with a history of concussion, and the lighter blue cluster represents the region centered on the left inferior frontal gyrus that showed stronger temporal coherence with the anterior DMN in those athletes with a history of concussion. From left to right and top to bottom, axial slices are taken at z = −9 to z = 5 in 2 mm increments. Images are presented in the radiological view where the right hemisphere appears on the left of the image. Color image is available online at
Relating neuroimaging metrics to phenotypic variables.
When assessing the full sample, no significant correlations were observed between neuroimaging and phenotypic measures. For those participants with a history of concussion, however, the temporal coherence between the precuneus cluster and the DMN was correlated with EXT (r = 0.646, p = 0.046, corrected). For those participants with a history of concussion, the correlation between EXT and Kr in the genu approached significance but did not survive the correction for multiple comparisons (r = 0.563, p = 0.108, corrected). The number of reported concussions was not associated with either DKI or rs-fMRI metrics in the ROIs.
Discussion
Phenotypic and neuroimaging biomarkers of concussion that persisted beyond the resolution of symptoms were investigated as possible signs of vulnerability to future decompensation. We observed no difference between participants with concussion history and those without on objective assessment of concussion symptoms, nor on detailed assessment of neuropsychiatric symptoms. Neuroimaging, however, revealed differences in WM integrity and in functional connectivity associated with a history of concussion.
The finding of elevated FA in the regions of the anterior WM for those athletes with a history of concussion was inconsistent with predictions and with almost all previously published research. 19,57 The participants in the current report differ in key ways from those previously studied, which may account for the unexpected results. We suggest that the relative youth of the participants in the current study and the fact that they are, on average, more than 3 years removed from their most recent injury are factors that could account for the increase in FA. The process of axon myelination, which continues through adolescence, 58 may provide an opportunity for WM repair that is not observed in studies of adult participants.
The current report also differs from previous studies of the chronic phase after TBI in studying currently asymptomatic participants. 19 In previous reports, 59 FA reductions were associated with persisting cognitive deficits, while the current study assessed athletes with no evidence of neuropsychiatric deficits. Finally, a recent review 60 argued that differences exist between sports-related TBI and TBI with nonsports etiology; of particular relevance for interpreting the results of the current study are that sports-related TBI studies include patients with lower levels of injury, and that athletes have psychological and environmental protective factors that may produce less dysfunction and more rapid recovery.
The location of the FA discrepancies is consistent with a recent meta-analysis that revealed anterior vulnerability to mTBI. 19 In the context of no subjective or objective evidence of persisting neuropsychiatric complaints, elevated FA may reflect recovery from injury. It is possible that the elevation in FA represents a destruction of crossing fibers, 29 but this suggestion is inconsistent with the observation of elevated K r , which was correlated with FA, in both clusters, suggesting increased tissue complexity.
Although speculative, an interpretation of the current findings as evidence of rehabilitation is consistent with a rat model of kurtosis dynamics in mTBI 31 that described evolution of kurtosis parameters over recovery from injury. In the acute post-injury period, K r was reduced and associated with a concomitant increase in diffusion perpendicular to the axon. In the subacute stage, K r and diffusivity statistics had normalized, suggesting that K r indexes recovery. This argument was supported by an association between normalized K r and reactive fibrous astrogliosis.
In one previous report, K r has been associated with improved cognitive performance in patients with TBI complaining of post-concussive symptoms, 61 suggesting that in the current study, elevated K r may produce a net elevation in FA, subserving the resolution of symptoms. It is biologically plausible that the WM measures reported in the current study represent a recovery mechanism, but inconsistency with previous research highlights the need for replication studies in the period after resolution of symptoms after mTBI.
rs-fMRI revealed one cluster in the superior medial gyrus that showed reduced temporal coherence with the DMN in athletes with a history of concussion, but increased iFC with the left IFG. The IFG has been implicated in higher-level cognitive processing 62 and is part of the Task Positive Network, which is typically anticorrelated with activity in the DMN. 63 Increased connectivity between the DMN and the IFG has previously been associated with memory complaints in the subacute stage after mTBI. 24 Within DMN, however, the pattern of results observed here of hyperconnectivity in the posterior DMN and hypoconnectivity in the anterior DMN is the reverse of those reported previously. 22,64
Mayer and colleagues 23 and Zhou and colleagues 25 have demonstrated that, after TBI, reduced posterior connectivity was correlated with post-concussive cognitive symptoms and increased frontal connectivity was correlated with depression, anxiety, and fatigue. 64 It is possible that in the current sample of asymptomatic athletes, reduced coherence between DMN and medial prefrontal cortex represents a mechanism that compensates for increased iFC between this node and the IFG, requiring overreliance on the posterior DMN.
The current study reports evidence of differences to both WM integrity and the functional organization of the brain in asymptomatic patients with a remote history of concussion. The degree of temporal coherence between the superior medial gyrus and the DMN was related to measures of WM integrity in the genu and the ACR. In previous reports, increased iFC between the DMN and IFG 24 has been observed in patients with cognitive complaints; we have suggested that reorganization of the DMN observed in our asymptomatic patients may reflect a compensatory mechanism supporting recovery of function. The ACR and genu have previously been implicated in the structural connectivity underlying the DMN, 65 so it is possible that changes to the microstructural integrity of the anterior WM are the mechanism by which functional reorganization occurs after mTBI.
The correlational approach that we have adopted here is limited by a priori identification of ROIs and post hoc interpretation. We suggest that in the future, data analytic techniques designed for multimodal neuroimaging assessment be applied to confirm how changes to the structure of WM tracts are related to changes to the functional organization of remote regions and across networks using a data driven method. 66,67
We have suggested that the differences observed in K r and in the organization of the DMN may represent rehabilitative or compensatory measures, but they may also represent the mechanisms by which those who have experienced a diagnosed concussion are at elevated risk of negative outcomes. Although the athletes with a history of concussion did not differ from those without on detailed neuropsychiatric assessment, they showed a relationship between externalizing symptoms and neuroimaging metrics in the ROIs that did not exist when examining the sample as a whole.
The extent to which those athletes with a history of concussion reported externalizing symptoms was correlated with the iFC of the DMN and with microstructural complexity in regions associated with a history of concussion. Externalizing symptoms include emotional and behavioral irritability, stubbornness, and lability, and are common after TBI and in CTE. 3,68
The extent to which we can determine causal relationships between the features reported here, however, is limited by the case series design. Specifically, as a cross-sectional study in which premorbid neuroimaging and neuropsychiatric profiles were not available, the current study only allowed comparison between groups. Baseline differences in DMN organization and WM integrity may confer vulnerability or resilience to athletes against the effects of mTBI, but the current study is not able to disentangle these baseline factors from injury-related factors.
The current study combined neuropsychiatric and neuroimaging assessment tailored to the pathophysiology of mTBI and applied them to currently asymptomatic athletes. We have shown that a history of concussion in asymptomatic athletes was associated with differences to the microstructural architecture of the cerebral WM and to the functional organization of the brain at rest. Some of these differences are consistent with previous reports of changes after mTBI while also suggesting novel evidence of rehabilitative processes.
The extent to which we can generalize from the current findings is limited by the homogeneity of the sample and the comparatively small sample size. As the first study to apply DKI and rs-fMRI to the period after the resolution of symptoms, the interpretation of the functional significance of these differences is necessarily post hoc. A prospective neuroimaging study in which athletes are followed from the acute post-injury period through to the resolution of symptoms would confirm the hypotheses suggested herein: that we are observing signs of residual damage tempered by signs of compensation or recovery. The ability to follow these athletes in the decades after injury would provide insight into whether the changes we observe represent vulnerability to future decompensation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.