
Abstract
Growing evidence suggests that temporally proximal acute concussions and repetitive subconcussive head injuries may lead to long-term neurological deficits. However, the underlying mechanisms of injury and their relative time-scales are not well documented in human injury models. The current study therefore investigated whether biomarkers of brain chemistry (magnetic resonance [MR] spectroscopy: N-acetylaspartate [NAA], combined glutamate and glutamine [Glx], total creatine [Cre], choline compounds [Cho], and myo-inositol [mI]) and structure (cortical thickness, white matter [WM]/subcortical volume) differed between mixed martial artists (MMA; n = 13) and matched healthy controls (HC) without a history of contact sport participation (HC; n = 14). A subset of participants (MMA = 9; HC = 10) returned for follow-up visits, with MMA (n = 3) with clinician-documented acute concussions also scanned serially. As expected, MMA self-reported a higher incidence of previous concussions and significantly more cognitive symptoms during prior concussion recovery. Fighters also exhibited reduced memory and processing speed relative to controls on neuropsychological testing coupled with cortical thinning in the left posterior cingulate gyrus and right occipital cortex at baseline assessment. Over a 1-year follow-up period, MMA experienced a significant decrease in both WM volume and NAA concentration, as well as relative thinning in the left middle and superior frontal gyri. These longitudinal changes did not correlate with self-reported metrics of injury (i.e., fight diary). In contrast, HC did not exhibit significant longitudinal changes over a 4-month follow-up period (p > 0.05). Collectively, current results provide preliminary evidence of progressive changes in brain chemistry and structure over a relatively short time period in individuals with high exposure to repetitive head hits. These findings require replication in independent samples.
Introduction
T
Proton magnetic resonance spectroscopy (1H-MRS) provides a potential measurement of brain injury within both gray matter (GM) and white (WM) matter. 12 The N-acetylaspartate (NAA) signal, often measured as the sum of NAA and the weaker and poorly resolved N-acetyl-aspartylglutamate (NAAG) signal, is frequently observed to be decreased in acutely and semi-acutely injured mTBI patients. 13 –15 A reduced ratio of NAA to total creatine (creatine and phosphocreatine; Cre) has been observed in the prefrontal GM and WM in athletes following concussion, 16 –20 with the decrease in NAA reportedly greater for first-time injuries. 17 Importantly, both cross-sectional 21 and longitudinal 16,19,20 studies have suggested that NAA increases (i.e., improves) post-injury, presumably as a function of recovery. Similar findings of decreased NAA and subsequent recovery have been observed in animal models in brain regions without axonal injury or histological evidence of cell death, 22 suggesting that 1H-MRS may be more sensitive than anatomical imaging for detecting trauma. However, not all studies have reported alterations in NAA following mTBI, 23,24 and to our knowledge few studies have examined longitudinal changes in metabolites few a function of participation in sports activities with high risk of repetitive injury.
Other work suggests that Cre, the signal from mobile choline-containing molecules (Cho), myo-inositol (mI), and the combined signal (Glx) from glutamate (Glu) and glutamine (Gln) may also be promising markers of long-term repetitive injury following mTBI. Findings from previous studies on Cre are mixed, with reports of both increased 21,25 and decreased 26 Cre in WM during the semi-acute stage of mTBI. Others have reported both decreased Glu or Glx in the primary motor cortex 16 and WM 21 following injury, as well as increased Glx in GM 21,25 and deep GM nuclei. 23 In addition, increased mI has been reported in the putamen following single-episode mTBI, 23 but not in global WM or GM. 18,27 Finally, increased Cho/Cre has also been observed during the semi-acute injury stage in WM, 28 GM, 13 and subcortical structures. 28
Emerging evidence from studies on professional athletes 7,8 suggests a higher incidence of frontal and medial temporal lobe atrophy in individuals with chronic traumatic encephalopathy (CTE), and atrophy is commonly noted in more severe forms of TBI. 29 Previous work with a chronically symptomatic (81.3% with post-traumatic stress disorder), mixed injury (mTBI and moderate TBI) cohort reported longitudinal differences in whole brain parenchyma and cerebral WM 1–2 years post-injury. 30 Others report atrophic whole-brain changes for complicated mTBI patients 6 months post-injury. 31 Typical mTBI patients show no evidence of atrophy during similar or even shorter post-injury times, 31 –33 although atrophy has been observed at 1 year post-injury. 33
Atrophic changes may also occur as a function of repetitive injury. For example, smaller subcortical volumes have been documented in professional fighters, 34 and fight exposure has been found to inversely correlate with subcortical volume in a mixed sample of boxers and MMA fighters. 35 Changes in subcortical structure volume in this sample were also inversely correlated with measures of impulsivity. 36 Further, a study of noncombative martial artists reported increased GM volume in pre- and supplementary motor areas. 37 Finally, a recent study indicated decreased hippocampal volumes in football players relative to athlete controls, with a history of mTBI also a contributing factor for volume loss. 38 To our knowledge, there have been few studies examining atrophic changes on a longitudinal basis in high-risk athletes.
Based on our previous work in single-episode mTBI, 21,32 we conducted a preliminary investigation on whether biomarkers of brain chemistry (spectroscopy: NAA, Glx, and Cre) and structure (atrophy: cortical thickness, total WM volume, and thalami/hippocampi volume) were different between high-risk athletes (MMA) and HC without a history of contact sport participation. Supplementary analyses were conducted on both Cho and mI. Our second aim examined whether these biomarkers changed over a 1-year period, presumably as a function of participation in a sport with a high risk for repetitive mTBI. Where feasible, case study data are also presented to determine how these metrics were affected by acute mTBI.
Methods
Participants
A total of 14 MMA and 16 HC were recruited for the current study. All fighters were recruited from a local training gym in Albuquerque, New Mexico. To be included in the study, MMA fighters were required to be between the ages of 18 and 45 years, have no contraindications for magnetic resonance imaging (MRI) scanning and to be participating in a regular training routine, including professionally organized fighting events as well as weekly sparring. The majority of controls were directly recruited to match patients in terms of gender, age (±4 years), and education (±4 years). HC were also required to be physically active (strenuous exercise at least 2 times per week), and have no history of regular, organized participation in a contact sport.
Participants were excluded if there was a history of mental illness or neurological disorders, a previous TBI with more than 30 minutes of loss of consciousness, and a recent history of substance abuse. One MMA was diagnosed with a preexisting neurological disorder by an independent physician during the course of the study and was subsequently eliminated, leaving a total of 13 MMA (11 males, 2 females; 28.2 ± 4.9 years old; 13.9 ± 1.7 years of education). Two HC were excluded prior to analyses due to failures with data acquisition (e.g., MRI-induced claustrophobia), leaving a total of 14 matched HC (12 males, 2 females; 28.1 ± 5.1 years old; 15.8 ± 2.3 years of education) in the final sample. All participants provided informed consent according to institutional guidelines at the University of New Mexico.
All participants were evaluated both clinically and with an extensive neuroimaging battery. MMA fighters were asked to return for a repeat scan approximately 1 year from their initial visit (mean = 385.9 ± 32.2 days), and all fighters were asked to complete a fight history diary (professional fights, sparring events, concussions) using a method similar to the Timeline Followback Calendar.
39
Fighters completed the diary every 3–5 months by phone or at the time of a clinical visit. HC were evaluated identically to MMA in terms of clinical and neuroimaging assessments, with the exception that the follow-up visit occurred between 3 and 6 months post-baseline (mean = 169.3 ± 37.3 days). HC were also not required to complete a fight diary. Clinical and imaging protocols occurred the same day for the majority (>90%) of visits. A total of 5 MMA participants self-reported experiencing acute mTBI during the course of the 1-year follow-up period. Three of the self-reported mTBIs were confirmed within 24 h by a clinical neuropsychologist (A.M.). One of the 3 participants experienced multiple concussions, which were also confirmed by the study team. These subjects were rescanned serially (acute [within 72 h], n = 3; semi-acute [1 month], n = 2; and early chronic [∼4 months], n = 3) post-injury. Structural images from each scan were reviewed by a certified radiologist for any abnormal findings and are summarized in Supplementary Table 1 (see online supplementary material at
Clinical assessment
Composite indices were calculated for the following cognitive domains: attention (Paced Auditory Serial Addition Test [PASAT], Stroop color-word scores, and Wechsler Adult Intelligence Scale-Third Edition [WAIS-III] Digit Span), working memory (WAIS-III Letter Number Sequence and WAIS-III Digits Backward), processing speed (WAIS-III Digit Symbol Coding, Trails A), executive function (Trails B and Controlled Oral Word Association FAS-test), and memory (Hopkins Verbal Learning Test- Revised Edition: immediate recall, long-delay free recall, discrimination index). The Wechsler Test of Adult Reading (WTAR) was also used to provide an estimate of overall pre-morbid intellectual functioning. The Test of Memory and Malingering (TOMM) allowed assessment of participant effort and cooperation.
Self-report for measures of somatic, cognitive, and emotional complaints common in concussion (Neurobehavioral Symptom Inventory; NBSI), history of previous concussions and the degree of symptoms associated with previous concussions (a modified version of the Rivermead Post-Concussion Symptoms Questionnaire; RPSQ), and general emotional status (State-Trait Anxiety Index and Beck Depression Inventory-Second Edition; STAI and BDI-II, respectively) were also assessed. Balance was assessed with the Balance Error Scoring System (BESS). For all measures, raw data were converted to T-scores using published age-specific norms whenever possible.
Image acquisition
All imaging sequences were collected on a Siemens 3 Tesla TrioTim scanner (Siemens Medical Solutions USA Inc., Malvern, PA) with a 12-channel head coil. High-resolution T1-weighted (TE [echo time] = 1.64, 3.5, 5.36, 7.22, 9.08 msec, TR [repetition time] = 2.53 sec, TI [inversion time] = 1.2 sec, 7-degree flip angle, number of excitations [NEX] = 1, slice thickness = 1 mm, FOV [field of view] = 256 mm, resolution = 256 × 256), T2-weighted (TE = 77.0 msec, TR = 1.55 sec, flip angle = 152 degrees, NEX = 1, slice thickness = 1.5 mm, FOV = 220 mm, matrix = 192 × 192, voxel size = 1.15 × 1.15 × 1.5 mm3), FLAIR (fluid-attenuated inversion recovery; TE = 88.0 msec, TR = 10.4 sec, flip angle = 160 degrees, NEX = 1, slice thickness = 3 mm, FOV = 256 mm, matrix = 320 × 320, voxel size = 0.8 × 0.8 × 3 mm3), susceptibility-weighted imaging (SWI; TE = 20.0 msec, TR = 28 msec, flip angle = 15 degrees, NEX = 1, slice thickness = 1.5 mm, FOV = 240 mm, matrix = 256 × 256, voxel size = 1.0 × 0.9 × 1.5 mm3), and magnetic resonance angiography (MRA; TE = 3.59 msec, TR = 20 msec, flip angle = 18 degrees, NEX = 1, slice thickness = 0.5 mm, FOV = 200 mm, matrix = 384 × 384, voxel size = 0.5 × 0.5 × 0.5 mm3) images were collected for all participants at the baseline visit. All anatomical scans were repeated at the follow-up visits with the exception of the MRA.
The 1H-MRSI sequences used in the current study were identical to previous publications.
21,25
Specifically, phase-encoded versions of a point-resolved spectroscopy sequence (PRESS), both with and without water pre-saturation (TE = 40 msec, TR = 1500 msec, slice thickness = 15 mm, FOV = 220 × 220 mm, circular k-space sampling [radius = 24], total scan time = 572 sec), were collected for all participants for all visits. The nominal voxel size was 6.875 × 6.875 × 15 mm after zero-filling in k-space to 32 × 32 samples. The 1H-MRSI volume of interest (VOI) was prescribed off the T2 image and was located approximately 1.8 cm above the lateral ventricles roughly parallel to the anterior-posterior commissure axis (Supplementary Fig. 1; see online supplementary material at
Statistical analysis
T1 structural data
Statistical Parametric Mapping (v5) (FIL Methods Group,
1H-MRSI processing
A Hamming filter with a 50% window width was first applied to the 1H-MRSI data followed by a 2D spatial Fourier transformation. The time domain 1H-MRSI data were analyzed using LCModel (v6.2-0T; s-provencher.com) on a voxel-wise basis with tissue water as a concentration reference.
41
LCModel spectra were corrected for partial volume effects (CSF, WM, and GM content) and for T1 and T2 relaxation effects based on SPM segmentation results using previously described methods (see Supplementary Fig. 2 for example spectra; see online supplementary material at
Quality assurance protocol
Outlier analyses were performed on all data prior to analyses. One HC was an outlier on the Visit 1 TOMM score and exhibited poor performance on other neuropsychological domains across both visits. However, the participant responded consistently on other clinical measures (i.e., reverse scoring items), and the HC's quality assurance metrics for imaging data were within normal ranges. Therefore, this participant's neuropsychological data were eliminated from all further analyses, whereas demographic, clinical (i.e., self-report), and imaging data were retained.
One MMA was an outlier on GM NAA concentration and on mean NAA line-width measure. Another MMA was an outlier on GM Glx concentration, and both participants were removed from the specific metabolite analyses. There were no outliers on any of the other metabolites (Glx, Cre, Cho, or mI). The amount of overlap between the aligned baseline and follow-up visits PRESS voxels was calculated to verify that tissue sampling was comparable across visits. Two MMA participants exhibited minimal voxel overlap (<60%) at the 1-year follow-up visit, and supplementary longitudinal 1H-MRSI analyses were conducted without data from these participants to verify primary results. Effect sizes are reported using either Cohen's d or a repeated measures (RM) effect size that correctly accounts for correlation between time-points given the limited sample size. 43
Results
Neuropsychological and clinical measures
Please see Table 1 for all clinical data. There were no differences between the two groups on age, sex, levels of testing effort, balance performance, or hand preference (p > 0.10). Both educational attainment (t25 = 2.47, p = 0.021) and estimated pre-morbid intelligence (t1,24 = 2.29, p = 0.031) were greater for HC relative to fighters. The composite indices of attention, working memory, memory, processing speed, and executive functioning were correlated to varying degrees (r ranging from 0.01 to 0.71). A multivariate analysis of covariance (MANCOVA) examining difference in cognitive functioning (WTAR as a covariate) was not significant for the multivariate effect of group (p > 0.10), although univariate tests indicated significantly reduced performance for MMA fighters for both memory (F1,23 = 5.75, p = 0.025) and processing speed (F1,23 = 4.45, p = 0.046).
Means, SDs, and effect sizes for neuropsychological indices reported following correction for WTAR as covariate.
Normalization presented as ratio of number of days reporting activity to number of days between baseline and follow-up visit.
Indicates number of participants who experienced mTBI between baseline and follow-up visit.
BESS, Balance Error Scoring System; BDI-II, Beck Depression Inventory–Second Edition; EF, executive function; HC, healthy controls; HQ, handedness quotient; MMA, mixed martial artists; mTBI, mild traumatic brain injury; N/A, not applicable; PS, processing speed; RPSQ & NBSI-Cog, Rivermead Post-Concussion Symptoms Questionnaire and Neurobehavioral Symptom Inventory cognitive complaints (Emot, emotional complaints; Som, somatic complaints); SD, standard deviation; STAI-S, State-Trait Anxiety Index–State; TOMM, Test of Memory Malingering; WM, working memory; WTAR, Wechsler Test of Adult Reading.
Baseline self-reports of somatic, cognitive, and emotional issues common in concussion (NBSI) were strongly correlated (r ranging from 0.80 to 0.90). A multivariate analysis of variance (MANOVA) indicated that multivariate effect of group was non-significant (p > 0.10), although univariate tests indicated significantly elevated somatic complaints (F1,25 = 4.39 p = 0.046) in MMA fighters.
As expected, a higher proportion of MMA fighters reported experiencing at least one previous mTBI (χ2 = 10.56, p = 0.001; 6/14 HC; 13/13 MMA), and also reported a significantly (Mann-Whitney U = 170.00, z = 4.00; p < 0.001) higher average lifetime incidence of mTBI (HC = 0.43 ± 0.5; MMA = 2.23 ± 1.1). A MANOVA examining the average acute somatic and cognitive symptoms resulting from previous head injuries (modified version of the RPSQ) returned a significant multivariate effect of group (F2,16 = 4.57, p = 0.027), with univariate tests indicating that MMA fighters reported significantly more cognitive (RPSQ-Cog; F1,17 = 9.51, p =0.007) symptoms during the recovery from their previous mTBIs.
Please see Table 1 for a semi-quantitative analysis of self-reported fight history for the MMA participants during the course of the study.
Baseline 1H-MRSI
There were no significant differences (p > 0.10) between the groups on NAA line-width (MMA = 0.035 ± 0.003; HC = 0.036 ± 0.004), signal-to-noise ratio (MMA = 16.171 ± 0.778; HC = 15.916 ± 1.008) or percentage of usable spectra (Supplementary Table 2). One-way ANOVAs were conducted to examine group differences in WM and GM metabolites (NAA, Cre, and Glx), using the Bonferroni method to control for false-positives within each tissue type. The univariate effects of diagnosis were not significant (p > 0.10) for either GM or WM metabolites (GM Cohen's d: −0.38 to 0.17; WM Cohen's d: −0.25 to 0.60). Supplemental analyses examining Cho and mI were also negative (p > 0.10).
Baseline structural results
There were no significant differences in total intracranial volume between groups at the baseline visit (p > 0.10). Three ANCOVAs examining for significant volumetric differences for total WM (p > 0.10; Cohen's d: −0.62) or in key subcortical structures (p > 0.10; Cohen's d: thalami = −0.03, hippocampi = 0.22) were not significant following Bonferroni correction. Results from the FreeSurfer analyses indicated that MMA fighters had significantly reduced thickness in the left posterior cingulate gyrus/precuneus as well as in the right occipital lobule relative to HC following corrections for multiple comparisons (Fig. 1).
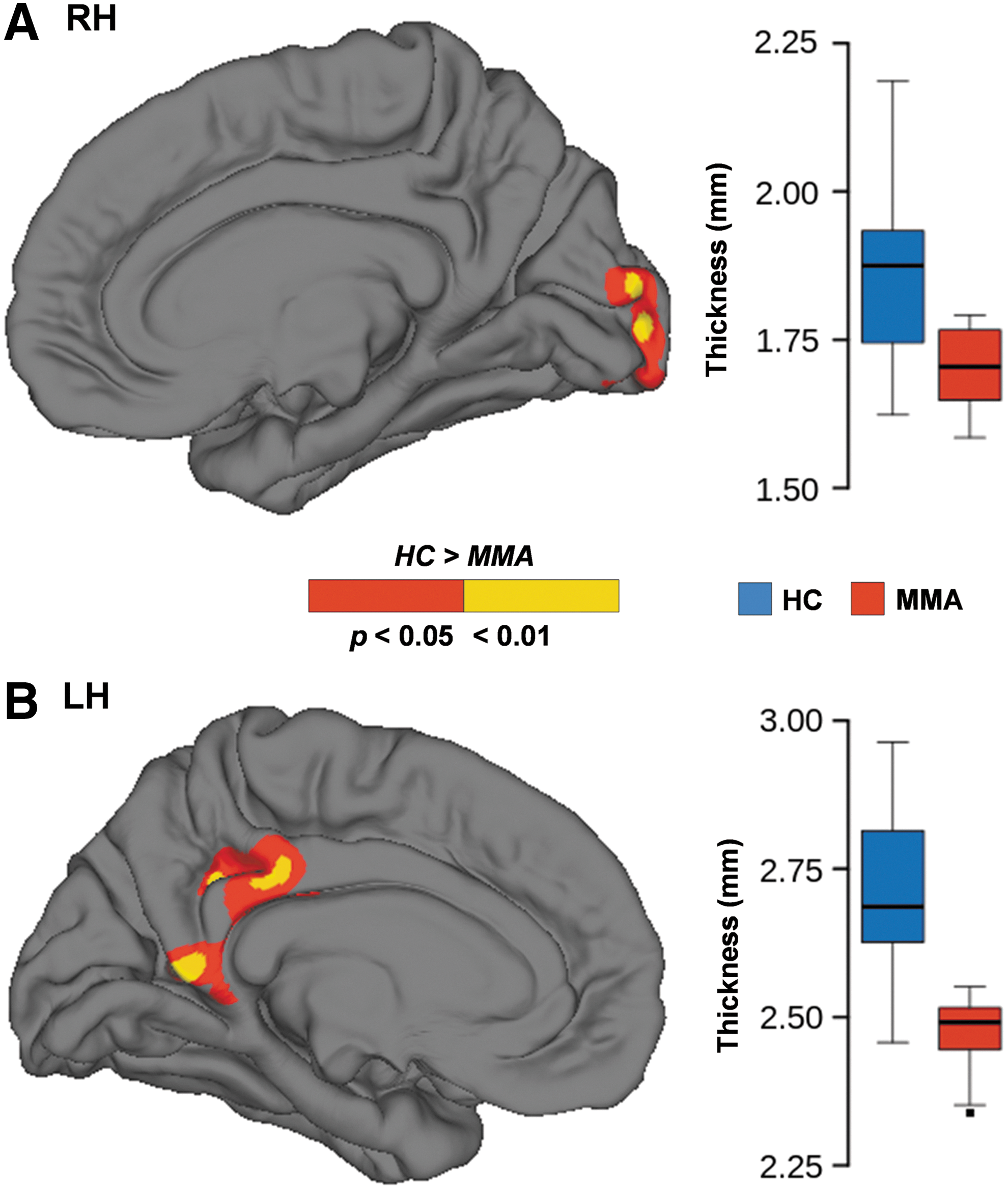
Figure 1 depicts baseline differences in cortical thickness between HC (blue) and MMA (red) in the right
Longitudinal analyses
Ten of the 13 eligible MMA fighters and 10 of the 14 HC returned for follow-up visit. Follow-up 1H-MRSI data for one MMA were lost secondary to acquisition issues. MMA showed a significant decrease in WM concentration of NAA between the baseline and follow-up visits (t8 = −2.90; p = 0.020; RM effect size: −1.02), with no differences in GM concentrations (p > 0.10). There were no significant differences across visits for HC for either WM or GM Cre and Glx concentrations (p > 0.10; RM effect size: −0.39 to 0.24). Supplemental analyses indicated that the significant difference in MMA WM NAA was only a statistical trend (t6 = −1.99; p = 0.094) when the two participants with poor voxel overlap were eliminated. However, the effect size remained similar (RM effect size: −0.80) suggesting that this was a result of reduced power. There were also no differences in Cho and mI for fighters (p > 0.10).
There were no significant longitudinal differences between groups in terms of changes in total intracranial volume (p > 0.10). FreeSurfer results indicated that HC and MMA exhibited significantly different rates of change in cortical thickness within the left rostral middle and superior frontal gyrus, with HC SPC increasing from baseline and MMA decreasing (Fig. 2). Repeated measure ANCOVAs indicated that there was a significant decrease in WM volume for the MMA group over the 1-year interval (F1,8 = 11.02, p = 0.011; RM effect size = −1.40), with no changes in thalamic or hippocampal volumes (p > 0.10). In contrast, HC exhibited no changes in WM or thalamic volume (p > 0.10), with a non-significant finding of decreased hippocampal volume at the second visit (F1,8 = 4.04, p = 0 .079; RM effect size = −0.72). Effect sizes were variable for both MMA (RM effect size: −1.40 to 0.56) and HC (RM effect size: −0.72 to −0.06).
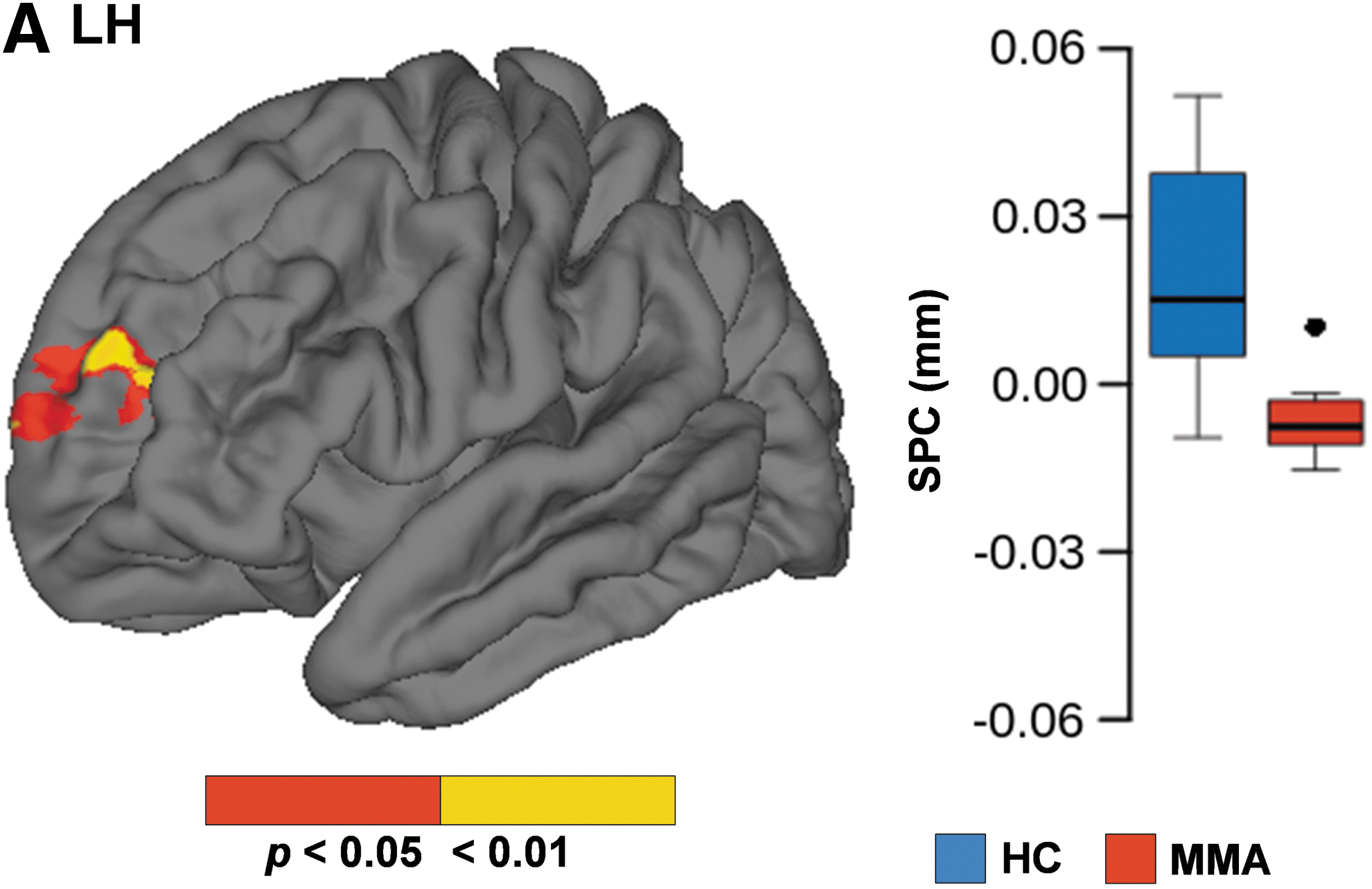
SPC values for cortical thickness over the course of the study (follow-up to baseline visit) for HC (blue) and MMA (red). Box-and-whisker plots indicate increased thickness at follow-up scans for HC and decreased thickness for MMA relative to their respective baseline evaluations. HC, healthy controls; LH, left hemisphere; MMA, mixed martial artists; SPC, symmetrized percent change.
Two multiple regressions examined whether significant changes in WM NAA and volume (dependent variables) were related to self-reported number of fights, normalized days sparring and history of a post-baseline mTBI (independent variables) in MMA fighters. However, the overall model was not significant for predicting change in WM NAA levels or total volume (p > 0.10).
Effects of acute concussions
A total of 5 out of 10 MMA participants self-reported an acute mTBI during the course of the study. Acute events for 3 of the 5 participants were verified by a clinical neuropsychologist within 24 h of injury and were followed with serial neuroimaging. Supplemental analyses were therefore performed comparing MMA participants with and without a self-reported history of acute mTBI during the 1-year study period. There were no significant differences (p > 0.10) for changes (follow-up to baseline visit) in WM volume, WM NAA concentrations, or relative cortical thinning within the left rostral middle and superior frontal gyrus for those with a history of acute mTBI (Fig. 3).
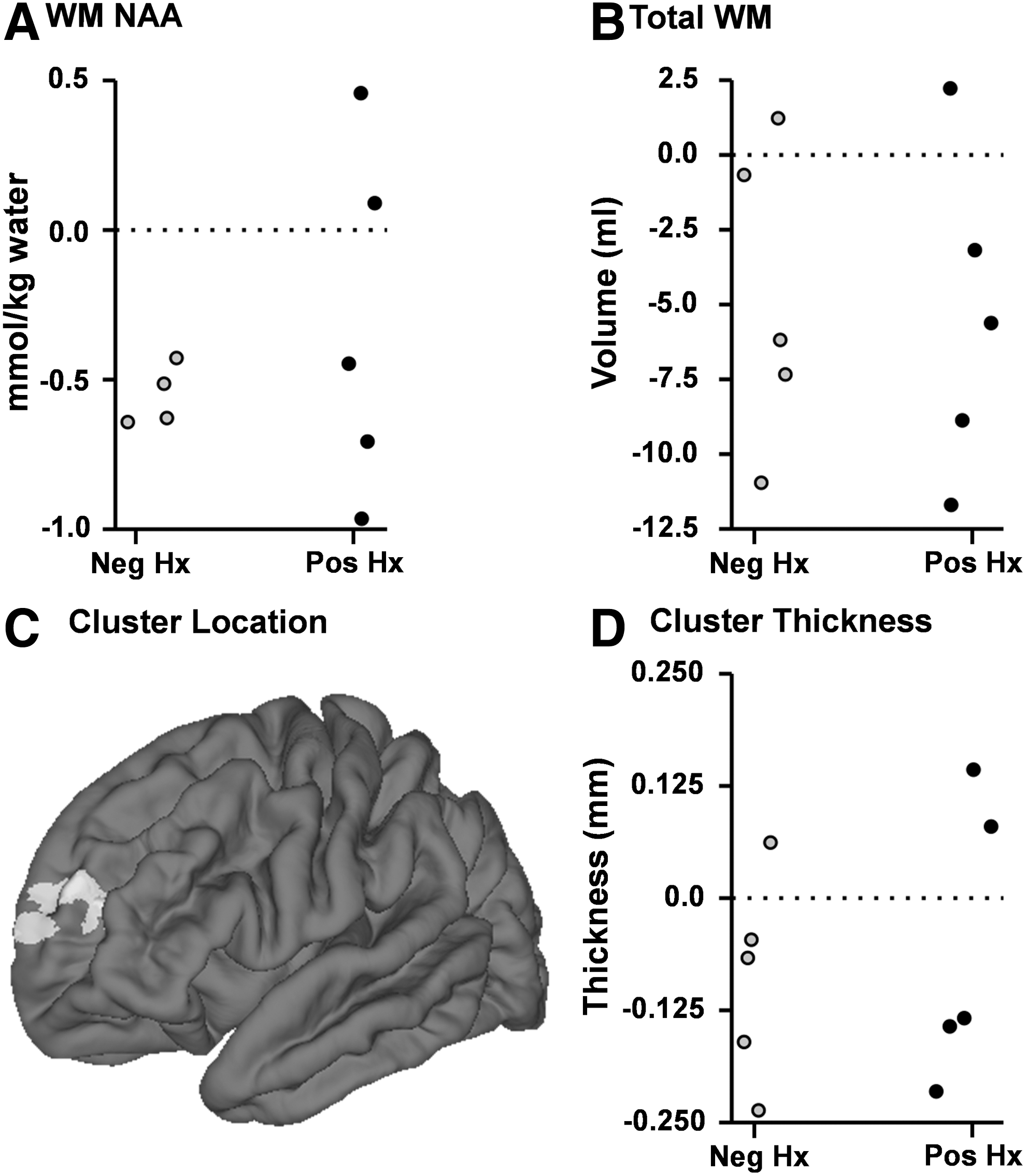
Figure 3 depicts the potential effects of acute concussion over the 1-year follow-up period on significant longitudinal findings in MMA. Scatter plots depicting change scores between the baseline and follow-up visits are presented for MMA with (Pos Hx; black circles) or without (Neg Hx; light gray circles) a self-reported (n = 2) or acutely verified (n = 3) concussion.
Serial 1H-MRS metabolite data (Fig. 4A,B) and volume estimates (Fig. 4C) are plotted for the three MMA fighters who were evaluated for acute mTBI while participating in this study. Due to the small number, these data were not evaluated quantitatively. Means and two times the standard deviation for HC at baseline (n = 14), HC at follow-up (n = 10) and MMA not scanned serially (n = 10) are also provided for an unbiased reference. A qualitative examination of the case study data indicates varying patterns of both metabolites and volume estimates from 3 days to approximately 4 months post-injury.

Serial 1H-MRS and volumetric case study data for three MMA with an acute concussion during the study follow-up period. Data from HC at baseline (C1; white diamonds) and 6-month follow-up (C2; gray diamonds) and from MMA fighters (F; black diamonds; excluding data from serial cases) are presented as a reference point, with error bars equaling 2 times the SD. The average GM and WM matter metabolite concentrations for NAA
Discussion
Recently, there has been a dramatic sea change in public and scientific opinions regarding the consequences of mTBI. It was initially believed that concussion resulted in limited behavioral and no long-term neurological consequences, 44 with standard clinical neuroimaging methods (computed tomography scans; T1- and T2-weighted images) typically negative for the majority of concussed patients. 45 However, recent data suggest that the life-long effects of concussion may be more severe, 7 especially when concussions occur on a repetitive basis over extended periods of time (i.e., years). Currently, there is a large gap in knowledge regarding the more immediate consequences of concussion and repetitive head trauma. Our results indicate longitudinal changes in WM NAA concentrations, WM volume, and relative cortical thinning in a high-risk sample of actively competing MMA athletes. These changes occurred over the course of a single year, providing preliminary evidence that progressive brain changes may occur over a relatively short time period.
Not surprisingly, 46,47 MMA athletes in the current sample reported a higher lifetime incidence of mTBI, increased cognitive symptoms during past concussion recovery, and more somatic complaints relative to controls. These findings are consistent with previous results suggesting that a history of concussion is a risk factor for both prolonged recovery as well as for experiencing new concussions. 4 MMA fighters also performed worse on formal tests of memory and processing speed, consistent with previous work demonstrating a dose-dependent relationship between the number of previous concussions and baseline neurocognitive performance. 48 Although these cognitive domains are frequently implicated in studies of TBI, 49 the two groups also differed in years of education and estimated pre-morbid intelligence, both of which contribute to formal cognitive testing 50 and serve as potential confounds for the current study.
Unlike our previous results, 21,25 we did not observe cross-sectional differences in either GM or WM metabolites between MMA and HC during the baseline assessment. These null findings may be secondary to sample characteristics (sub-acute versus more chronic injuries, single versus repetitive mTBI) or relative to the unique samples that were studied (e.g., MMA fighters). However, MMA fighters exhibited a significant decrease in WM NAA over the course of our 1-year follow-up period. NAA is an amino acid that is synthesized in the neuronal mitochondria 51 and is widely interpreted as a marker of GM and WM integrity. 52 An initial decrease and subsequent recovery of NAA has also been observed in rodent models of TBI in regions of brain without axonal injury or histological evidence of cell death. 22 Moreover, as reviewed in the introduction, a decrease in WM and GM NAA is one of the most widely reported findings across the spectrum of TBI 12 including the acute and sub-acute phases of concussion. 16 –20 Changes in NAA correlate with initial Glasgow Coma Scale 53 and predict long-term cognitive outcome following TBI. 54 Thus, current findings suggest that participation in high-risk combat athletics may result in changes in WM integrity, a supposition that can be further evaluated with diffusion tensor imaging. 55 However, longitudinal results from other non-diagnosed athletic samples have reported no changes in NAA concentration, 24 suggesting the need for replication in an independent sample.
MMA fighters also exhibited cortical thinning in the right occipital cortex, the left posterior cingulate cortex, and precuneus relative to controls at baseline, which may be a result of previous history of concussions. The posterior cingulate gyrus/precuneus corresponds to the posterior hub of the default mode network (DMN), 56 exhibiting both high metabolic activity and high connectivity with the rest of the brain. 57 The posterior hub of the DMN has also been found to exhibit differences in functional connectivity in previous studies of mTBI 58 and more severe TBI. 59 Moreover, longitudinal evidence of a differential rate of cortical thinning (increased for MMA fighters) was also observed in the left rostral middle and superior frontal gyrus over the course of 1 year, as well as a decrease in total WM volume. Previous work suggests that atrophy may occur only in the later stages of mTBI, 32,33 may be limited to patients with complicated mTBI, 31 or may be limited to chronically symptomatic patients. 30 In addition, cross-sectional differences in subcortical and ventricle volumes have been documented in professional fighters, 34 with an inverse relationship between fight exposure and subcortical volumes 35 and impulsivity and change in subcortical volume. 36 Others have reported decreased hippocampal volumes in American football athletes relative to controls, with a further reduction for individuals with a self-reported history of mTBI. 38 As evidenced by prior research, 33 the longitudinal design of the current study as well as the longer follow-up period may have increased the sensitivity for detecting subtle differences resulting from repeated exposure to traumatic events.
Current findings have several potential implications for participation in sports with a high likelihood of concussion. First, future studies aimed at improving the safety of participants are needed, such as recent data indicating that the use of protective boxing gloves and head padding can significantly reduce the impact force of simulated head strikes 60 as well as rule changes in American football that may decrease the incidence of concussion (i.e., kick-offs). Second, current and previous results highlight the critical need for objective biomarkers that indicate neuronal injury progression rather than reliance on subject self-report that may reflect non-specific symptomatology and/or symptom underreporting. The latter is a common problem in athletes following mTBI, and it has been estimated that the failure to report concussion symptoms in high school football may be as high as 53%. 61 Others have shown that a second concussion occurring during the semi-acute stage of injury results in a further decrease in NAA and/or further delays the recovery of NAA to baseline levels. 19 Therefore, the identification of reliable longitudinal biomarkers related to repeated concussive and subconcussive hits should ultimately produce physiological targets for the development of objective diagnostic (did this patient suffer a significant concussion?) as well as prognostic (can this patient safely return to play?) decisions. However, as illustrated by our serial neuroimaging data, identifying concussions by any single biomarker is likely to be challenging.
There are several limitations to the study that should be noted. First, the current study was based on a relatively small sample of MMA fighters as well as controls, which increases the likelihood of sampling bias and under-powered results in between group designs. Second, the amount of time between follow-up visits was different across the two groups, which may have potentially reduced the sensitivity of longitudinal data. To mitigate both of these limitations, the majority of our longitudinal analyses were based on within-subject comparisons, and effect sizes are reported throughout the manuscript. Third, 5 of 10 of the returning MMA fighters self-reported a concussion between the baseline and follow-up scans, with concussions for 3 of the fighters verified within 24 h post-injury by the study team. Although there were no differences between MMA fighters with and without a concussive event at the follow-up visit, we cannot disambiguate whether longitudinal changes resulted from “diagnosable” events or repetitive trauma, or were due to some other factor. Finally, our control group was purposely selected based on their levels of physical fitness and their history of non-participation in contact sports. The selection of this control group reduced the likelihood of potential exercise confounds, 37 and reduced the likelihood of other confounding factors (e.g., history of performance enhancing drugs) present in a former contact-sport athletic control group. 38 However, the current control sample included a subset of participants (6/14) with a history of head trauma, which may have contributed to null findings during group-wise metabolite comparisons. Similarly, other factors unique to the MMA cohort (e.g., diet, more strenuous exercise routine, supplement usage, etc.) may have also contributed to observed cross-sectional differences.
In summary, there is a growing body of literature highlighting the possible deleterious effects of repetitive hits as well as concussions in athletes over a relatively short period of time. 11,55 Current results suggest that participation in high-risk athletic events may alter basic WM neurochemistry (decreased NAA) as well as result in structural changes in both GM and WM. Future studies that include larger sample sizes are needed to both replicate current effects as well as potentially delineate the effects of acute trauma.
Footnotes
Acknowledgments
We would like to thank the staff and mixed martial artists at Jackson's Mixed Martial Arts Gym in Albuquerque, New Mexico, for their help and participation in the current study.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.