
Abstract
The purpose of this study was to evaluate cardiac autonomic modulation in university athletes during the post-acute to late phase (mean, 95 days ±63) of injury at rest and during physical exertion. We also sought to evaluate the effect of time since injury and number of injuries on heart rate variability (HRV). We hypothesized that physical exertion would reveal persisting modifications in HRV following a concussion. We included, in a cross-sectional design, athletes who sustained a concussion and matched controls. Concussions were identified by a medical doctor using established criteria. Twelve male concussed and 12 control athletes took part in the study. Control participants were teammates who were chosen to match the concussed athletes with regard to their height, weight, education, and age. The beat-to-beat electrocardiogram intervals of the participants were measured at rest and during physical exertion (isometric hand grip contraction; IHGC), which was sustained for 3 minutes at 30% of the participants' maximum. Linear and nonlinear parameters of HRV were calculated. The ratio between low and high frequency (LF/HF) bands was calculated to assess the sympathovagal balance. During the IHGC, but not at rest, concussed athletes presented significantly lower power in HF bands, leading to a significantly higher LF/HF ratio (p ≤ 0.05). Thus, asymptomatic athletes still may exhibit modifications in cardiac autonomic modulation weeks to months following injury. These modifications may only become apparent during physical exertion. Monitoring HRV may aid diagnosis and provide insight about safe return to play.
Introduction
A
The acute clinical symptoms of sport-related concussion (SRC) are believed to reflect the functional disturbance of the central nervous system, with symptoms often resolving within 7–10 days of injury. 3 However, deficits in multiple aspects of nervous system function have been observed well beyond the acute phase of recovery. For example, concussed adults who were tested months (6.3 ± 3.5) after their injury present deficits in working memory. 4 Moreover, concussed university athletes present deficits in auditory processing several years following injury. 5 Together, evidence suggests that a concussion can have a broad effect on the brain, with deficits that persist beyond the post-acute phase of the injury. 1
It is possible that a concussion affects other components of the nervous system, 3 such as those involved in regulatory functions. One of these includes the autonomic nervous system (ANS), which continuously attempts to modulate the rhythm of the heart in response to blood pressure oscillations, respiration, thermoregulation, and circadian biorhythm. 6 This autonomic activity leads to a natural physiological phenomenon known as heart rate variability (HRV), where the time interval between consecutive heart beats varies slightly. 7 In general, greater HRV suggests that the ANS is appropriately responding to the requirements of the environment, whereas lower HRV suggests that the ANS is not modulating heart rate as efficiently. The analysis of HRV has been used in numerous studies as a reliable marker of autonomic impairment, 7 including for patients who experienced a traumatic brain injury. 8 –13
Little is known about the consequences of an SRC on HRV. Gall and colleagues 14 evaluated the HRV of 14 concussed athletes at 2 and 7 days following the injury. At rest, no significant difference was found between the concussed athletes and matched controls. However, sub-maximal exercise on a cycle ergometer exposed changes in HRV. This modification was indicated by a significantly lower absolute power of low and high frequencies in the power spectrum density of heart rate.
Similarly, La Fountaine and colleagues 15 evaluated the HRV of three concussed athletes at rest and during a sustained isometric hand grip contraction (IHGC). At rest, the HRV of concussed athletes was not significantly different from matched controls, but during grip contraction performed 48 h following the injury, concussed athletes had less complex heart rate patterns, as indicated by lower approximate entropy. However, 2 weeks following the injury, no statistical difference was observed in HRV between the concussed and control athletes.
Together, the literature suggests that an SRC can modify cardiac autonomic modulation, at least up to 7 days following the injury. However, the consequences beyond the acute phase are still unknown. Further, it is unknown whether these consequences vary with the number of prior injuries. Given that persistent deficits are reported for other brain processes, 1 the purpose of this study was to evaluate HRV in concussed athletes beyond the acute phase of injury (95 ± 63 days) at rest and during physical exertion. We hypothesized that no differences would be observed between groups at rest but that physical exertion (IHGC) would reveal modifications in HRV.
Methods
Participants
Preliminary power analysis based on the results of La Fountaine and colleagues 15 were performed via G*Power statistical software (University of Düsseldorf, Germany). Results indicated that at a 1-β of 0.80, 11 participants are required for each group to detect differences in linear metrics of HRV and seven participants are required for each group for the non-linear metric of HRV. Accordingly, 24 athlete—12 with a history of concussion and 12 matched controls (teammates)—were recruited to participate in this study. Each group consisted of 11 football athletes and one volleyball athlete. The ethics committee at the University of Montreal approved the study and all participants were aware of the purpose of the study and procedures before providing their consent.
Concussions were diagnosed by the team physician (on field) at the time of injury, and injuries were verified by a clinical neuropsychologist using the criteria of the American Academy of Neurology 16 and those proposed in the consensus statement of the 3rd International Conference on Concussion in Sport. 3 Concussed athletes were identified and recruited via the university sports medicine clinic in coordination with the university athletic association. Concussed athletes completed a Post-Concussive Symptoms Checklist. 17 At the time of the injury, concussed athletes reported 12.7 ± 4.8 symptoms, including headaches, dizziness (n = 11); impression of being idle, difficulty concentrating (n = 10); pressure in the head (n = 9); not feeling well, sensitivity to light, sensitivity to sound, difficulty remembering, fatigue or lack of energy, irritability, neck pain (n = 7); confusion (n = 6); and being more emotional, balance problems, sleeping more than usual, and nausea (n = 5). No athlete incurred loss of consciousness or amnesia from the injury. It is important to note that all athletes reported being symptom free at the time of testing. Concussed athletes were evaluated on average 95 ± 63 days (median [25 percentile-75 percentile] = 110 [29–138] days) following injury.
Controls were teammates who were matched with regard to age, level of education, height, and weight. Control athletes were recruited through the university athletic association and were required to be free of a history of concussion. All athletes were required to be free of a history of alcohol and/or substance abuse, psychiatric illness/psychotropic medication, learning disability, neurological disorders (seizure disorder or brain tumor), or history of more severe brain injury. All athletes were actively engaged in their sports at time of testing. Group details are presented in Table 1.
Characteristics of the groups; values are reported as means ± SD.
SD, standard deviation; BMI, body mass index.
Protocol
This protocol is similar to that of another study that assessed HRV in concussed athletes. 15 Testing took place in a quiet room with regulated ambient temperature and stable humidity, and concussed participants and their matches came to the lab at approximately the same time of day. All participants were instructed to eat a complete breakfast or lunch and to abstain from training, and from drinking alcoholic or caffeinated beverages on the day of the assessment. Beat-to-beat electrocardiography intervals (RR intervals) were continuously measured for each participant during rest and physical exertion. Athletes were instrumented with a heart rate monitor (RS800CX from Polar Electro, Kempele, Finland), enabling the continuous measurement of RR intervals with a 1 msec resolution.
The resting phase of testing lasted 5 min. Participants sat in an armchair in an upright position with their forearms resting on the armrests. Prior to physical exertion, the athletes performed two maximal voluntary isometric contractions with their dominant hand using a handgrip dynamometer (T.K.K.5001 Grip A; Takei Scientific Instruments, Tokyo, Japan). The arm was positioned on the side at approximately 30° from the sagittal plane with the elbow extended. The trials were separated by 90 sec of rest. Physical exertion lasted for 3 minutes and consisted of an isometric hand-grip contraction at 30% of grip maximum.
HRV calculations
RR intervals were manually inspected and edited for ectopic beats. 7 Once ectopic beats are eliminated, RR intervals are known as normal-to-normal (NN) intervals. Data analyses were conducted for the last 3 minutes of the rest period and for the total 3 min of physical exertion.
Analyses of linear HRV indexes in the time and frequency domains, as well as non-linear indexes, were performed with Kubios HRV, version 2.0 (Biosignal Analysis and Medical Imaging Group, Kuopio, Finland). Time domain parameters included the mean value of NN intervals (
In addition, the calculation of non-linear power spectral density was obtained by parametric methods (autoregressive model). This model was chosen because it renders the best sensitivity to fast NN changes and is more suitable for recordings of shorter duration. 7 Approximate entropy (ApEn) provides a measure of irregularity or complexity within the NN intervals. 18 Low values of ApEn are less desirable, as they indicate a more regular and predictable signal, and consequently less HRV.
Frequency domain parameters included the calculation of low-frequency (LF; 0.04–0.15 Hz) and high-frequency (HF; 0.15–0.4 Hz) components. 7 The LF and HF components are considered to be markers of sympathetic and parasympathetic activity, respectively. Although, the interpretation of the LF component remains controversial, the ratio between the LF and HF components (LF/HF) is accepted as an important marker of sympathovagal balance. 7
Statistical analysis
Separate analyses were conducted for each HRV parameter using a series of two-way repeated measure analyses of variance (ANOVAs) with concussion (concussed, control) as the between-subject factor and condition (rest, exercise) as the within-subject factor. A Greenhouse–Geisser correction for sphericity was applied. Planned comparisons were performed to identify the source of the interactions by means of independent samples t-tests with Bonferroni corrections. Lastly, bivariate correlations were carried out to evaluate the relation between injury characteristics (time since injury, number of prior injuries) and HRV indexes. Statistical analyses were conducted with SPSS software version 20.0.0 (IBM Corporation, Armonk, NY).
Results
Participants
T-tests comparing control and concussed athletes did not reveal significant differences regarding age, level of education, height, weight, or body mass index (all, p > 0.10).
HRV Parameters
Figure 1A presents the
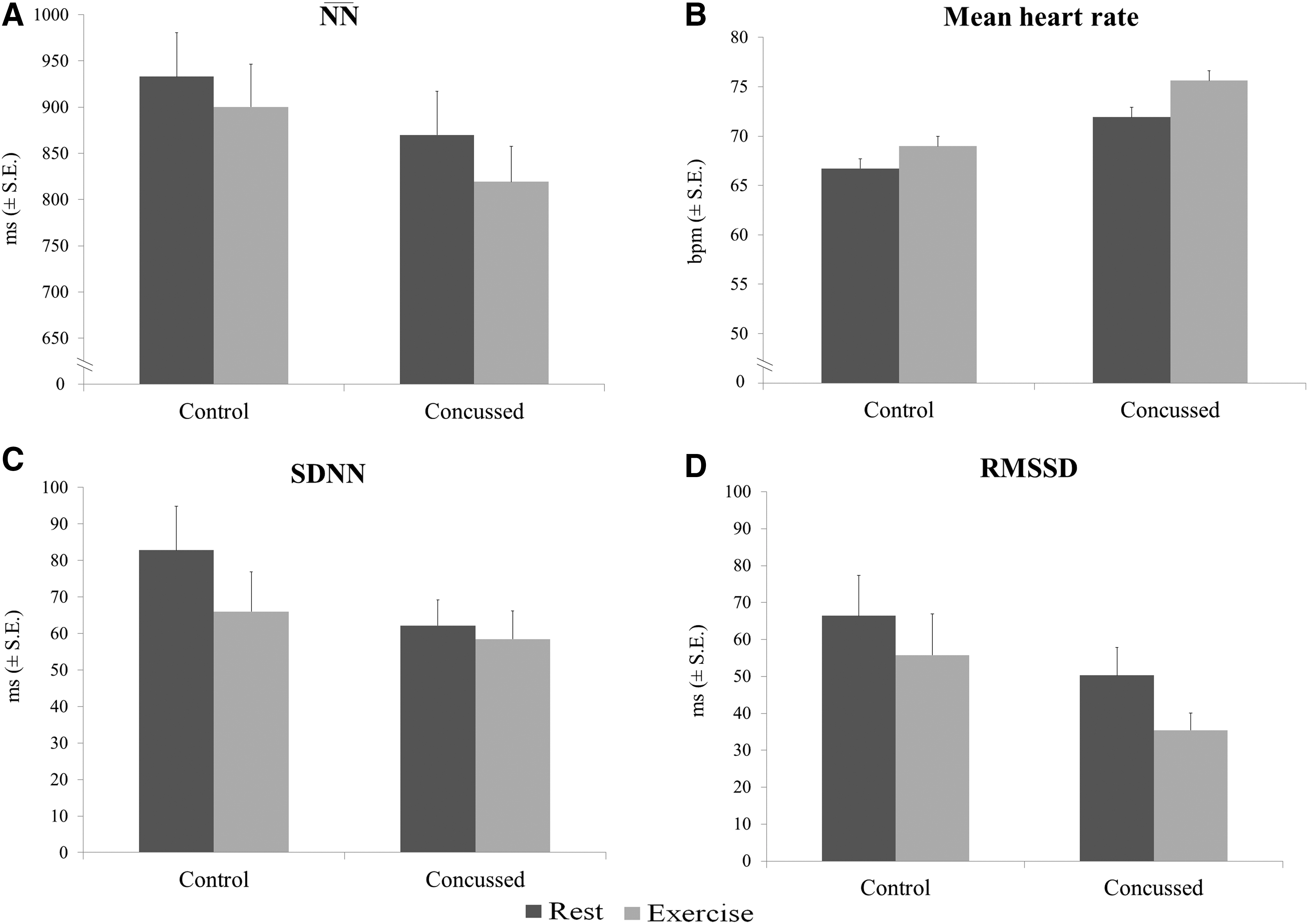
Figure 1B presents the mean HR measured at rest and during exertion for concussed and control athletes. The ANOVA revealed a main effect of condition (F[1,22] = 11.422; p = 0.003), indicating that all athletes exhibited significantly higher HR during physical exertion (M = 72.3; SD = 12.8), compared with at rest (M = 69.2; SD = 13.3; p = 0.002; d = 0.23). No significant effect of group or condition × group interaction was observed, indicating the HR values were similar for the concussed and control athletes, both at rest and during physical exertion.
Figure 1C presents the mean SDNN at rest and during exercise for concussed and control athletes. The ANOVA revealed a main effect of condition (F[1,22] = 5.124; p = 0.034), indicating that all athletes exhibited significantly lower SDNN during physical exertion (M = 62.23; SD = 31.91), compared with at rest (M = 72.48; SD = 34.91; p = 0.037; d = 0.31). However, there was no significant condition x group interaction or main effect of group. Therefore, the SDNN of the concussed and control athletes are similar at rest and tend to decrease similarly in response to physical exertion.
Figure 1D presents the mean RMSSD at rest and during exercise for concussed and control athletes. The ANOVA revealed a main effect of condition (F[1,22] = 6.523; p = 0.002), indicating that all athletes exhibited significantly lower RMSSD during physical exertion (M = 45.61; SD = 30.73), compared with at rest (M = 58.34; SD = 32.76; p = 0.01; d = 0.40). However, there was no significant condition × group interaction or main effect of group. Therefore, RMSSD for concussed and control athletes are similar at rest and tend to decrease similarly in response to physical exertion.
Figure 2D presents the mean ApEn at rest and during exercise for concussed and control athletes. The ANOVA did not reveal a significant condition × group interaction or a main effect of condition or group. Therefore, the ApEn at rest and exercise are similar for concussed and control athletes.
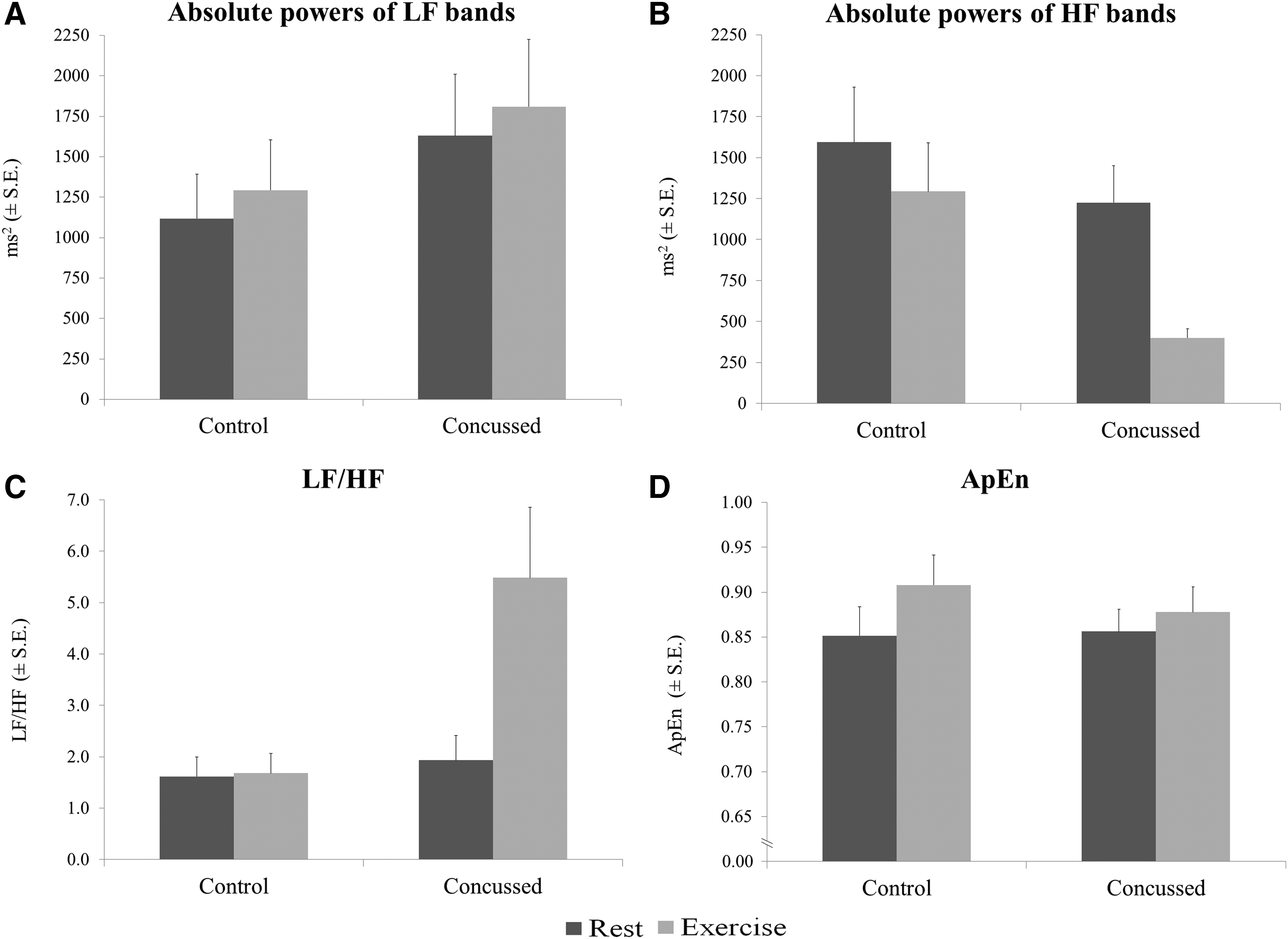
Figure 2A presents the mean absolute power of LF bands at rest and during exercise for concussed and control athletes. The ANOVA did not reveal a condition × group interaction or a main effect of condition or group. Therefore, the LF bands for concussed and control athletes are similar at rest and during physical exertion.
Figure 2B presents the mean absolute power of HF bands at rest and during exercise for concussed and control athletes. The ANOVA revealed a condition × group interaction (F[1, 22] = 20.906; p = 0.044). Tests of simple effects revealed that concussed athletes exhibited significantly lower absolute power during physical exertion (M = 399.4; SD = 197.0), compared with at rest (M = 1225.6; SD = 777.5; p = 0.002; d = 1.46). Moreover, concussed athletes exhibited significantly lower absolute power, compared wih controls (M = 1293.8; SD = 1029.2; p = 0.01; d = 1.20) during physical exertion. Therefore, being concussed is associated with a decrease in absolute power for the HF bands but only during physical exertion.
Figure 2C presents the mean LF/HF ratios at rest and during exercise for concussed and control athletes. The ANOVA revealed a condition × group interaction (F[1,22] = 9.264; p = 0.006). Tests of simple effects indicated that concussed athletes exhibited significantly higher LF/HF ratio during exercise (M = 5.48; SD = 4.78), compared with at rest (M = 1.93; SD = 1.66; p = 0.01; d = 0.99). Moreover, concussed athletes exhibited a significantly higher ratio, compared with controls (M = 1.68; SD = 1.33; p = 0.02; d = 1.08) during physical exertion. Therefore, being concussed is associated with an increase in LF/HF ratio but only during physical exertion.
Bivariate correlations
The analysis did not reveal any significant correlations between the number of prior injuries and any index of HRV. However, trends were noted for LF/HF ratio during physical exertion (r 2 = 0.51; p = 0.09), absolute power for the HF bands at rest (r 2 = 0.54; p = 0.07), and ApEn at rest (r 2 = 0.56; p = 0.06). The analysis did reveal significant correlations between time since injury and several HRV indexes, including RMSDD at rest (r 2 = 0.62; p = 0.03), absolute power of HF bands at rest (r 2 = 0.68; p = 0.02), and ApEn at rest (r 2 = 0.69; p = 0.01), suggesting that HRV indexes at rest were normalized over time.
Discussion
The present study demonstrates that asymptomatic athletes in the post-acute stage of injury still present distinct modifications in HRV, compared with non-concussed athletes. These modifications were observed only during physical exertion (sustained IHGC), which stimulates the ANS. 17,13 By means of sustained IHGC, we found that concussed athletes exhibited a modification in sympathovagal balance, as indicated by their higher LF/HF ratio, compared with controls. This modification appears to be explained by a higher withdrawal of parasympathetic activity, as indicated by the lower absolute power of HF bands, whereas sympathetic activity remained unchanged. Together, the data suggest that concussed athletes exhibit modifications in cardiac autonomic activity in response to ANS stimulation. Two previous studies report abnormalities in HRV in concussed athletes during exercise, but only during the acute phase of the injury (up to 7 days). 14, 15 The present findings extend these results by highlighting that HRV modifications persist beyond the acute phase injury.
In addition, time since injury was associated with several indexes of HRV at rest, indicating that concussed athletes' HRV likely normalizes over time while at rest. These findings underscore the importance of assessing concussed athletes during physical activity, as persistent nervous system modifications may go unnoticed when evaluated at rest. Conversely, bivariate correlations failed to reveal any significant relation between the number of prior injuries and any of the HRV indices.
SRCs are known to cause disturbances to several functions of the brain, with differences in recovery time being observed. Some studies suggest that adults recover within 1–2 weeks post-injury. 1 For example, performance on neuropsychological tests returns to baseline within 5–10 days, 19,20 deficits in postural stability of collegiate athletes resolve within 3–5 days, 21 and clinical symptoms dissipate within 3–10 days. 22 –24 Similarly, in a preliminary study that evaluated HRV in concussed athletes, 15 deficits in cardiac autonomic modulation were present 2 days following the injury and seemed to resolve after 2 weeks.
In contrast, many studies report disturbances that persist several weeks and even months after a concussion. For example, deficits in sensory processing, 5,25 and executive functions 26,27 have been noted for weeks to months following injury, and abnormalities in the electrical responses, 28,29 metabolic balance, 30,31 and oxygen consumption 32,33 of neurons persist several months following a concussion. Similarly, the results from the present study suggest that cardiac autonomic modulation is modified in concussed athletes for weeks to months following injury.
Further, our results are in partial agreement with those from studies that evaluated HRV in patients who suffered a mild to severe traumatic brain injury (TBI) that was unrelated to sport. 8 –13 Those studies report abnormalities in HRV at rest, while we only observed deficits under conditions of physical effort. For example, Hilz and colleagues 11 assessed HRV in 20 mild-TBI patients tested anywhere from 5 to 43 months following the injury. At rest and during an active stand up test, patients presented changes in cardiac autonomic modulation. This was indicated by a significant reduction of overall HRV and an increase in sympathovagal balance (LF/HF). Thus, it is possible that injuries resulting from sport may be less severe than those resulting from non-sport etiologies (vehicular accident, blast wave, etc.). It should be noted, however, that contemporary methods of evaluating HRV might not be sensitive enough to reveal potentially subtle cardio-autonomic modifications at rest in concussed athletes. 35 Indeed, an exploratory experiment implementing more sophisticated cardio-electrophysiological assessment revealed cardio-electrical instability in three concussed athletes while they were at rest. 34 As such, a combination of injury severity and technological sensitivity may account for discrepant results.
Although the results from our experiment suggest that an SRC causes changes in cardiac autonomic modulation, the underlying mechanisms of dysfunction are still unknown, and several possible explanations exist. For example, Goldstein and colleagues 10 hypothesized that modifications in cardiac autonomic modulation result from an “uncoupling” in the neuroanatomical pathway between the autonomic and cardiovascular systems. La Fontaine and colleagues 15 proposed that the transient changes in HRV might be due to an “impairment of efferent autonomic activity to the heart.” and Hilz and colleagues 11 suggested that the modifications in sympathovagal balance might result from “minute lesions in tracts or neurons assuring sympathovagal balance.” Although the exact mechanisms contributing to brain injury–related cardiac autonomic dysfunction remain unclear, what is clear is that concussive injuries result in cardiac autonomic dysfunction. Further, the current results indicate that this cardiac dysfunction not only persists beyond the acute phase of recovery, but also may be evident only during physical exertion. As such, future research will need to investigate longitudinally the cardiac autonomic activity at rest and during exertion in order to fully elucidate the mechanisms underlying concussion-related cardiac autonomic dysfunction.
Limitations and conclusion
The current study also has some limitations that should be considered. First, the pressure associated with high-level athletic performance could motivate some individuals to minimize or even deny their symptoms. 36,37 This is a concern given that concussions do not necessarily have outwardly visible signs, making them difficult to recognize. 1 However, this is unlikely to be a concern in the current study, given that concussions were identified by team physicians and symptoms managed by the university sports medicine clinic.
It also could be argued that differences in ventilation rate influence HRV, 35 including the LF/HF ratio. 36 However, this influence is likely marginal and unlikely to be a concern under the present conditions. First, ventilation rate is not modified during the IHGC. 37 Further, several studies report that there is no significant relation between respiration frequency and HRV or respiratory sinus arrhythmia, 38 –44 and an increase in ventilation rate associated with physical activity does not significantly influence the spectral analysis of HRV. 45 Therefore, an IHGC may be used to induce the hemodynamic stress of physical activity 46 while minimizing the effects on ventilation rates, 37 making the IHGC a sensitive, specific, and reproducible method of assessing cardiac autonomic function in normal and clinical populations. 47 That being said, future research will benefit from measuring ventilation rates in order to gain a more comprehensive understanding of the influence of an SRC on autonomic function.
In conclusion, an SRC induces significant modifications in cardiac autonomic activity that can last well beyond the acute phase of recovery and the return to play. Importantly, these modifications may only manifest during physical exertion. The present findings carry clinical implications, as before returning to play, guidelines recommend that concussed athletes be asymptomatic at rest and during physical activity. The measurement of HRV is relatively simple, fast, and inexpensive, and can easily be measured on the field. Thus, with additional research, HRV could eventually be used to monitor recovery and contribute to guidelines for the safe return to play.
Footnotes
Acknowledgments
This research was funded by grants from the Canadian Institutes for Health Research and the Canadian Foundation for Innovation to Dave Ellemberg. Acknowledgement to Vincent Slythe, BSc, for evaluating several athletes and to Benedicte Robitaille, MSc, for implementing the pre-manipulations of the protocol.
Author Disclosure Statement
No competing financial interests exist.