
Abstract
Primary prevention programs of pediatric abusive head trauma (PAHT) exist and early screening is proposed, but negative effects of mislabeling parents as abusers, an important issue, are not well documented. The aim of our study was to simulate the possible impact of programs for the primary prevention and screening of PAHT. We developed Markov models that simulate the life histories of PAHT with no intervention, with primary prevention program only, with screening program, and with both programs in a hypothetical cohort of 800,000 newborns in a high-income country. Screening program would be addressed to all families until children are 2 years old, during repeated consultations. Potential side effects for parents being mislabeled as abusers were supposed to increase the probability of PAHT and decrease participation in screening. Time horizon was 2 years with cycles of 15 days. Outcomes were number of deaths and abused children avoided. Uncertainty was specified with probability distributions. After 2 years, the median number of deaths avoided through primary prevention would vary from 6 (95% confidence interval [CI] 2–11) to 28 (95% CI 6–51) per 100,000 newborns. Screening could prevent up to 6 (95% CI 0–29) or cause up to 66 (95% CI 0–361) deaths per 100,000 children born alive. The impact of both programs was uncertain. Our model confirmed the potential benefits of primary prevention and documented the uncertainty associated with screening of PAHT.
Introduction
P
Several studies suggest that children could be victims of repeated episodes of PAHT before it is detected, 12 or that physicians miss cases of PAHT. 13 For these reasons, several authors advocate systematic screening of PAHT, for example among infants presenting to the emergency department. 14,15 The understanding of how PAHT occurs has also improved. The role of infant crying has been recognized as the most common stimulus for PAHT. 16,17 Crying, especially when parents do not understand its meaning, can provoke negative, destructive, survival-endangering responses resulting in PAHT. PAHT could result from a failure of normal iterative interactions between infants and their parents. 17 Theoretically, this abnormal interaction could be the target of screening, before any head trauma.
The impact of possible prevention or screening programs is difficult to estimate, in particular because of the lack of knowledge about the beginning of PAHT, and difficulties in measuring all cases of PAHT. Large and expensive cohorts would be necessary in view of PAHT incidence. Negative effects of mislabeling parents as abusers are yet not well documented, but several authors have raised the issue of the potential impact of such stigmatization. 18 Consequently, a clinical study considering early screening of PAHT before children have serious consequences or when children have only abnormal interaction with their parents is not ethically acceptable. To overcome this difficulty, computer modeling has many advantages. The impact of strategies as a systematic early screening could be studied, whereas in reality such strategies could cause ethical problems. Cost of computer stimulation is very low and no expensive and time-consuming studies are necessary. Alternative strategies can be easily compared and; even if better knowledge about PAHT remains to be acquired, the contributions of each parameter or research hypothesis to uncertainty about the potential impact of programs can be estimated. 19
We developed a Markov modeling of the evolution of PAHT, for four alternative strategies: no intervention, primary prevention program, screening program, and both primary prevention and screening programs. Our objective was to evaluate the possible impact, on a cohort of newborns, of primary prevention and screening programs targeted at PAHT.
Methods
Decision model
Our Markov model compared the evolution of PAHT with: no intervention, primary prevention alone, screening alone, and both primary prevention and screening. The simulated population was a cohort of 800,000 newborns, corresponding approximately to the annual number of newborns in France.
20
The model of natural evolution had five possible and mutually exclusive states (Fig. 1): 1. Normal interaction: Children are healthy with normal interaction between them and their parents. 2. Subclinical: Children have no clinical symptoms, but parents have negative interactions with their children. 3. Reversible clinical: Children have reversible, clinical, temporary consequences of PAHT, consecutive to a first shaking or another mechanism of inflicted trauma; these consequences can result in the child faint with spontaneous recovery. 4. Irreversible clinical: Children have irreversible consequences of PAHT without spontaneous recovery, consecutive to repetitive shaking or when first shaking was extremely violent, such as motor deficit with paralysis and spasticity, epilepsy. 5. Death: At each state child could die from PAHT or other causes.
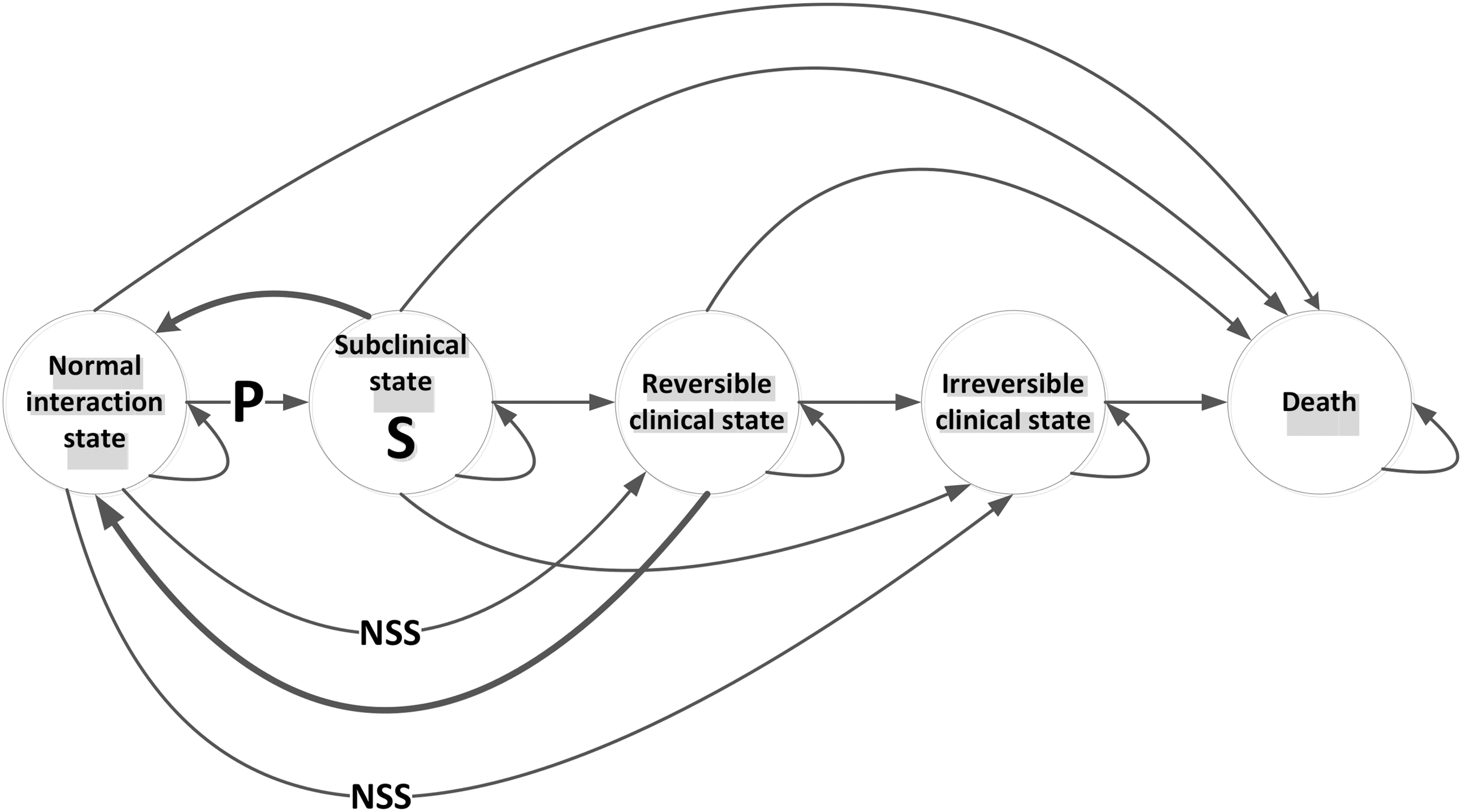
Markov model of the impact of prevention and screening programs of pediatric abusive head trauma. Normal interaction state: child healthy with normal interaction with his/her parent(s); subclinical state: asymptomatic child with abnormal interaction; reversible/irreversible clinical state: child with reversible/irreversible consequences. Arrows: transitions between states; thick arrows: transitions increased by programs. NSS, no when subclinical state is considered; P, targeted by prevention; S, targeted by screening.
Because the existence of a subclinical state is not formally defined, we considered two evolutions of PAHT: a model with a subclinical state and a model without a subclinical state. Each Markov cycle was 15-days long.
Interventions
A primary prevention program aims to prevent PAHT before it ever occurs, that is, before the possible subclinical state, when parent and child have negative interactions, or if no subclinical state exists, before a reversible clinical state. The modeled primary prevention program would be offered to all parents with their consent. The proposed intervention would be based on current PAHT education interventions, such as the Dias or Altman program or in the first stage of the PURPLE program. 5,8,9 These programs were delivered during the postpartum hospital stay, immediately following delivery. For example, the PURPLE program used an educational package that includes a 10-min DVD and an 11-page booklet to explain to the parents that infant crying is normal, what are the appropriate responses to inconsolable crying, and the danger of shaking a baby. No side effects were considered. 21
Screening aims at identifying PAHT when children have no symptoms or signs and are apparently in good health, which corresponds to the potential subclinical state and the reversible clinical state when the child has spontaneously recovered a normal state. A screening program would include all actions to identify early children who are victims of PAHT, and improve their health by avoiding severe consequences. It would include the initial screening test, a confirmation diagnostic strategy, and an intervention. Several authors have explored screening tests such as serum biomarkers, 22 but no formal screening program currently exists. A hypothetical screening program was defined to be directed to all parents and children until the latter are 2 years old and had no irreversible consequences; it would be provided by family physicians or pediatricians during repeated follow-up consultations, monthly during the first 6 months of the child's life, and at 9, 12, 16, 20, and 24 months. If detection were positive, an education intervention would be proposed to stop PAHT evolution. Because the potential harm associated with mislabeling parents as child abusers has been emphasized, 18 we modeled side effects for parents wrongly detected as abusers. Indeed, some parents could be identified as parents who have negative interactions with their children (subclinical state, reversible clinical state), whereas they have in fact normal interactions with their children (normal interaction state). These parents would be false-positive. The effects of this stigmatization might lead to an increase of parent's stress and of their anxiety. 18 We also assumed that these parents could experience losing confidence in themselves, poor self-esteem, depression or paranoia, and social isolation. As these effects have been identified as risk factors of child abuse, 23,24 this stigmatization may place children at greater risk to become abused than before the screening. Thus, we assumed that potential side effects of screening could be to increase the probability of PAHT and to decrease future participation in the screening program.
Model parameters and assumptions
Whenever possible, transition probabilities were extracted from the literature (Table 1). Transition probability between normal and clinical states of PAHT varied over time. It was more important when the child was less than one year of age. 25,26 When considering a subclinical state, we chose two extreme scenarios: most in favor and most in disfavor of screening. The scenario most in favor of screening assumes that all parent/child pairs are in a subclinical state after the first Markov cycle, and remain in this state until children have clinical symptoms. In this scenario, no parents could be false-positive. Indeed, after screening intervention, some parents are in a normal interaction state but in the following cycle all these parents return to a subclinical state. The impact of simultaneous primary prevention and screening programs could not be estimated in this case. The scenario is most in disfavor of screening when transition probability to remain in a subclinical state is nil. Parents and children are in a subclinical state during only the 15 days before clinical manifestations of PAHT.
PAHT, pediatric abusive head trauma; pmortaBL, probability to die from causes other than PAHT.
For the two above-mentioned extreme situations and the model without a subclinical state, we have modeled three scenarios based on maximum, minimum, and median estimations of the incidence of PAHT in high-income countries, varying according to definitions used and populations. 3,25 –27 Shanahan and colleagues and Parrish and associates used the definition recommended by the Centers for Disease Control and Prevention in 2012. 11,25,27 Fujiwara and co-workers used the International Classification of Diseases, 10th edition codes. 26 Because Shanahan and colleagues estimated incidence only for children younger than one year old, we used the incidence estimation of Keenan and associates for children aged one and two years old. 3,27 Keenan and associates focused only on serious or fatal PAHT. 3 The case-fatality of PAHT was estimated at around 20%, 3,28,29 sometimes less (6.7%), as in a study in the United States. 30 Thus, we had this parameter vary from 0 to 0.3. When neither data nor estimations were available, we assumed variation between extreme possible values. These values were zero, and the sum of transition probabilities from one state was 1. We assumed a probability of participation for a primary prevention program to be between 0.6 and 1 5,9,31 and effectiveness between 0.4 and 0.8. 5,9
Outcomes
Outcomes were measured after 2 years. Numbers of children in each state for 100,000 children born, the number of avoided or added deaths, and the difference of number of children in clinical states were reported.
Data analysis
We used Microsoft Office 2013's Excel (Microsoft, Redmond, WA) to run the model. Children moved from state to state during 49 cycles. For each scenario considering or not a subclinical state, we conducted probabilistic sensitivity analyses with three scenarios for transition probability between normal state and clinical states of PAHT. Beta distributions were used for transition probability between normal state and clinical states of PAHT and, when lack of knowledge did not allow estimating distributions, uniform distributions between extreme values. For the beta distributions, alpha and beta estimations were obtained by the method of moments. Random numbers bounded by these distribution assumptions were generated to calculate outputs for each cycle. We used 1000 simulations, where the analysis modeled uncertainty for all parameters simultaneously.
Results
Potential impact of primary prevention
Primary prevention programs would reduce mortality and morbidity (Table 2). Depending on the level of incidence, the application of primary prevention alone would avoid 6 (95% confidence interval [CI] 2–11) to 28 (95%CI 6–51) deaths per 100,000 children. The number of irreversible consequences of PAHT avoided would vary from 0 (95%CI 0–5) to 1 (95%CI 0–26) per 100,000 children. The number of children who would remain in a normal or subclinical state as a consequence of prevention would vary from 7 (95% CI 4–11) to 32 (95% CI 18–54) per 100,000 children.
NE, not estimable.
Potential impact of screening
The impact of screening was uncertain (Table 2). If being wrongly identified as an abuser would decrease participation in screening programs and increase the probability to become an abuser, screening could cause more cases of PAHT. Screening could prevent, after 2 years of evolution, up to 6 (95%CI 0–29) deaths per 100,000 children, or cause up to 66 (95%CI 0–361) deaths per 100,000 children. The number of children with irreversible consequences could be reduced to 0 (95%CI 0–11) per 100,000 children or increased to 5 (95%CI 0–152) per 100,000 children (Table 2).
Potential impact of associating primary prevention and screening
Simultaneous application of primary prevention and screening would not reduce mortality and morbidity with certainty (Table 2). In scenarios without any subclinical state, application of both primary prevention and screening could cause from 19 (95% CI −5 to 77) to 91 (95% CI 21–355) deaths per 100,000 children. When considering a subclinical state lasting only 15 days, from 16 (95% CI −6 to 76) to 85 (95% CI –21 to 375) deaths per 100,000 children could be caused. With a subclinical state lasting more than 15 days, screening would be more effective, because more parents would be potentially detected early, and fewer would be wrongly identified as abusers. Primary prevention would decrease the incidence of PAHT and increase the number of parents wrongly identified as abusers. The latter would less participate in subsequent rounds of screening and would be more likely to become abusers.
Discussion
We examined the potential impact of primary prevention and screening programs on PAHT in a hypothetical cohort from a high-income country, taking into account major uncertainties. We showed the potential benefit of a primary prevention program and the uncertainties concerning screening. We hypothesized that false identification of parents as abusers could either have no impact on the evolution of PAHT or increase the probability of becoming abusers. Under the latter hypothesis, a screening program could potentially increase mortality and morbidity. Very few studies have considered the effects of being wrongly identified as an abuser. When parents were victims of separation from their children because of false allegations of child abuse, they described the loss of the sense of being competent parents and a modification of their attachment to their child. 32 These feelings would lead some parents to relations with a disorganized attachment with their child. Although the link between child maltreatment and disorganized attachment is unclear, maltreatment could be the cause of disorganized attachment and vice-versa. 33,34 Research on the potential effects of being wrongly identified as an abuser is very important to the consideration of screening programs.
We hypothesized in two models that a true subclinical state preceded the clinical state in which parents are acting out and become physically violent with their child. During this potential subclinical state, parents would go through stages of emotions such as accumulation of frustration or anger, especially because of a child's persistent crying. 7,17 Because of their incapacity to control and overcome these emotions, some parents could become violent. Parents could learn how to recognize and cope with these emotions through different stress techniques. For instance, the Perinatal Shaken Baby Syndrome Prevention Program uses coping strategies with an “anger thermometer.” Parents are reassured about the experience of anger that crying can cause and they identify strategies for dealing with anger. 7 Screening of child-parent interaction difficulties should not result in a negative perception, but in positive parenting support measures, especially because many parents with these difficulties could never become authors of PAHT.
We often chose extreme limits for distributions of transition probabilities between stages leading to PAHT used in probabilistic sensitivity analyses. Indeed, few studies have documented the mid- and long-term outcomes of PAHT. 1,2,35,36 In these studies, the definition and qualification of injury varied, as well as initial severity, age at time of injury, follow-up periods, and outcome measures; attrition rates were often high. The use of a consensual definition, better follow-up of all victims, and measures of any possible consequences of PAHT are necessary.
We used available information about the incidence, based on the International Classification of Diseases. Several studies have documented the lack of accuracy of external cause coding in hospital records, in particular its low sensitivity. 37,38 A recent study estimated, however, the sensitivity and specificity respectively at 92% and 96%. 39 Consequently, the incidence of PAHT might be underestimated in our models, so that the benefits of a primary prevention program are underestimated. Similarly, we did not take into account the incidence variation during the first year of life by lack of precise estimations, but incidence is higher the younger the children and the benefits of the screening program would be underestimated. 16
In our model, we have considered that without intervention, child health could deteriorate gradually but not improve. However, after the occurrence of PAHT, some improvement of child health over time could occur. 40 Consequences of the same PAHT would be also more important for younger children because of higher physiological vulnerability during early infancy. 41
The effectiveness of primary prevention was considered constant over time but might decrease over time. The impact of this decrease is likely to be small, because of a decrease of the incidence over time. We considered that effectiveness of screening was constant over time. However, the effectiveness of screening could vary according to the state of detection and the age of the children. Similarly, we chose probability of screening participation constant over the time in each group (parents who were never false-positive and parents who were already at least once false-positive). But screening participation could change over the time.
We have considered a primary prevention program directed to all parents of newborns. A primary prevention program could be also only targeted for families with risk factors for PAHT. However, identification of high-risk families, before the occurrence of PAHT could be responsible for stigmatization of these families and a negative effect could be foreseen. Moreover, the predictive value of risk factors should be very strong, and should not imply missing opportunities to prevent occurrence of PAHT in other families. Current scientific knowledge is insufficient to define an adequate high-risk population. Actually, proposed primary prevention programs are systematic programs. 5,8,9 A screening program could be considered in a high-risk population seen in emergency departments; similarly, current knowledge is insufficient to define such a population. The rhythm at which screening tests should be repeated, who would be the program actors, and the type of intervention remain to be defined. We have chosen a decreasing frequency of screening tests because of age-specific incidence curves of PAHT. 16 Actors who would screen should accept this procedure. Finally, no early intervention is well defined, but coping strategies to better react to infant crying could be adapted for parents who have negative interactions with their child. 7
Following current recommendations that cost-effectiveness analysis should only be carried out for programs with a demonstrated effectiveness, we have not considered the economic impact of the modeled programs. 42 Nevertheless, the cost-effectiveness ratio is important and should be estimated before implementation of prevention or screening programs. Further, the full cost of PAHT to society is not well documented today, precluding any full cost-effectiveness analysis. Medical costs has been studied, 43 but indirect costs of PAHT have never, to our knowledge, been considered. PAHT has an impact on educational pathways of affected children and, later, on their social integration and working capacity, in particular when they have severe physical or psychic disability. 43 These long-term consequences and their cost have not been sufficiently studied.
Conclusions
Our models confirm the relevance of primary prevention of PAHT. Before considering screening, future research should focus on describing the effects of wrongly identifying parents as abusers, and developing and evaluating tests to identify earlier children with PAHT.
Footnotes
Author Disclosure Statement
No competing financial interests exists.