
Abstract
Repetitive traumatic brain injury (rTBI) occurs as a result of mild and accumulative brain damage. A prototype of rTBI is chronic traumatic encephalopathy (CTE), which is a degenerative disease that occurs in patients with histories of multiple concussions or head injuries. Boxers have been the most commonly studied patient group because they may experience thousands of subconcussive hits over the course of a career. This study examined the consequences of rTBI with structural brain imaging and biomolecular imaging and investigated whether the neuropsychological features of rTBI were related to the findings of the imaging studies. Five retired professional boxers (mean age, 46.8 ± 3.19 years) and four age-matched controls (mean age, 48.5 ± 3.32 years) were studied. Cognitive-motor related functional impairment was assessed, and all subjects underwent neuropsychological evaluation and behavioral tasks, as well as structural brain imaging and functional-molecular imaging. In neuropsychological tests, boxers showed deficits in delayed retrieval of visuospatial memory and motor coordination, which had a meaningful relationship with biomolecular imaging results indicative of neuronal injury. Morphometric abnormalities were not found in professional boxers by structural magnetic resonance imaging (MRI). Glucose metabolism was impaired in frontal areas associated with cognitive dysfunction, similar to findings in Alzheimer's disease. Low binding potential (BP) of 18F-flumazenil (FMZ) was found in the angular gyrus and temporal cortical regions, revealing neuronal deficits. These results suggested that cognitive impairment and motor dysfunction reflect chronic damage to neurons in professional boxers with rTBI.
Introduction
R
Clinically, rTBI presents with complex behavioral, psychiatric, cognitive, and/or motor-related symptoms. Neuropsychological features and cognitive dysfunctions are characterized by impairments in memory and executive function, behavioral changes, motor-related signs, and personality changes. 7 –9 Behavioral disturbances are often the earliest finding and include aggression, depression, apathy, and impulsivity. 10 Executive function involving planning, organization, multi-tasking, and decision-making is also often impaired in subjects with repetitive brain trauma. These neuropsychological changes may predict neurodegenerative disease progression. 1 Motor impairment in boxers may include mild dysarthria and difficulty balancing, progressing to ataxia, spasticity, impaired coordination, and parkinsonism—an entity distinct from idiopathic Parkinson's disease.(PD). 11,12
Imaging modalities to detect and assess brain injury are constantly improving, but computed tomography (CT)/magnetic resonance imaging (MRI) often show normal structures despite a host of symptoms.
13
Ross and colleagues found no correlation between the duration of damage or behavioral symptoms, and findings from CT and electroencephalography in 38 retired boxers.
14
CT was used to examine 338 active professional boxers, whose scans were normal in 93% of cases, with 7% showing “borderline” atrophy.
15
These negative results led many researchers to use MRI, and abnormalities were found in boxers with normal CT findings.
16
Volumetric MRI has been proposed for diagnosing rTBI by detecting atrophy of the whole brain as well as specific areas (e.g., amygdala),
3
and its utility was demonstrated in five symptomatic former professional contact-sport athletes.
17
However, MRI findings are inconsistent in rTBI.
18
Diffusion tensor imaging (DTI) and magnetic resonance spectroscopy (MRS) have also been proposed for detecting axonal injury or significant chemical changes in TBI, but these imaging methods cannot clearly disclose the mechanism of rTBI progression. Recently, biomolecular imaging has emerged as an ideal method for examining biochemical mechanisms in the human brain. 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) and more recently, 18F-flumazenil (FMZ) PET can reveal metabolic brain function and neuronal integrity. 18F
We focused on examining neuronal deficits in patients with chronic brain damage with biomolecular imaging, and we expected these techniques to provide unique information on the cellular and molecular aspects of rTBI. In addition, we administered various neuropsychological tests to investigate whether neuropsychological features are related to the findings of imaging studies.
Methods
Subjects
Five retired professional boxers (mean age, 46.8 ± 3.19 years; range 42–49 years) and four age-matched controls (mean age, 48.5 ± 3.32 years; range 46–53 years) were studied. All subjects were right-handed (assessed by the Edinburgh Handedness Questionnaire; Oldfield, 1971) 25 and were screened for neurological and psychiatric diseases. Informed consent was obtained from each subject in accordance with the research protocol for human subjects approved by the Medical Ethics Committee of Seoul University Bundang Hospital (IRB no. B-1212-182-004). The characteristics of the subjects are listed in Table 1. Details of their boxing careers can be seen in Table 2. The following inclusion criteria were fulfilled for the professional boxers: >10-year career in professional boxing (including duration as an amateur); right-handed males, age 30–55 years; written informed consent obtained.
n.s., non-significant difference between groups; SD, standard deviation.
Each boxer within this study group; includes matches fought (bouts), whether the bout was a win or loss, the career duration, and weight division in boxing. KO, knockout: reveals that boxers were down for the count in the match.
The duration of exposure to the repetitive brain damage of boxing of the study subjects was a minimum of 22 years (mean, 27.6 years; range, 22–30 years) from their initial exposure to boxing.
The following exclusion criteria were used for all subjects, including boxer and control groups: history of cerebral hemorrhage or neurological brain surgery, active (or history of) neuropsychiatric disease, claustrophobia, metal substance in the body (e.g., cardiac pacemaker, prosthetic appliance), usage of any medication, poor compliance with the investigator's instructions.
To investigate the subjects' daily symptoms that were associated with brain trauma, we interviewed the individuals about their self-reported symptoms in the following categories: headache; dizziness; body tremor; sense of physical discomfort; cognitive status, memory, and decision-making; and quality of sleep. Among the five professional boxers, subject 1 complained of chronic dizziness that occurred 2–3 times a week. Subject 2 complained chronic headaches and recent memory difficulties in object naming. Subject 4 had been treated for chronic headaches in the hospital for 3 years. The other two subjects did not complain of any daily symptoms.
Screening and neuropsychological testing
Unified Parkinson's Disease Rating Scale
For the clinical estimation of motor-related functional impairment in boxers and to assess whether they have Parkinson's-like symptoms, we used the Unified Parkinson's Disease Rating Scale (UPDRS) on all subjects. This scale is used to follow disease progression and to evaluate surgical, medical, and other interventions for PD. 26,27 The UPDRS consists of four components: 1) mentation, behavior, and mood; 2) activities of daily living; 3) motor examination; and 4) complications of therapy. The clinician-scored motor evaluation was based on part III of the UPDRS, which assesses the objective motor symptoms based on a scale ranging from 0 (no impairment) to 4 (severe impairment). The UPDRS-III items assess specific motor symptoms: speech; facial expression; tremor at rest in head, arms, and legs; action and postural tremor of hands; rigidity of neck, arms, and legs; finger tapping; hand movements; rapid alternating movements; leg agility; arising from a chair; posture; gait; postural stability; and body bradykinesia. In our study, a neurologist evaluated all subjects using the UPDRS-III.
Chronic Brain Injury Scale
The chronic brain injury (CBI) scale quantifies the clinical findings of motor, cognitive, and psychiatric deficits associated with boxing-related brain injury. 28 Scores on the CBI scale range from 0 to 9, with higher scores reflecting greater impairment. The cognitive component incorporates the boxer's score on the Mini-Mental State examination (MMSE).
Neuropsychological tests
To investigate impaired neuropsychological performance in professional boxers, we used various neuropsychological assessments. All subjects underwent a neuropsychological evaluation using the following standardized tests: MMSE, the Beck Depression Inventory (BDI), 29 and the Barratt Impulsiveness Scale-11 (BIS-11). 30 BIS-11 consists of three subscales: motor impulsiveness, attentional impulsiveness, and non-planning impulsiveness. To examine the cognitive ability of professional boxers, all subjects underwent various cognitive tasks: 1) the Hopkins Verbal Learning Test (HVLT): verbal memory; and 2) the Rey-Osterrieth Complex Figure Test (RCFT): visuospatial memory.
Buss-Durkee Hostility Inventory
The Buss-Durkee Hostility Inventory (BDHI) is one of the best-known self-report measures of aggressive personality. 31 The BDHI is a written questionnaire designed to assess different types of aggression. The questionnaire includes a 4-point Likert scale. From the BDHI, we selected 21 items from three subscales: behavioral aggression (assault), verbal aggression, and indirect aggression. Behavioral aggression (nine items) is defined as physical violence against others, including getting into fights with others, but not destroying objects. Sample items from this scale include “If someone hits me first, I let him have it,” and “Once in a while I cannot control my urge to harm others.” Verbal aggression (seven items) represents negative affect expressed in terms of arguing, shouting, or screaming, with content including threats, curses, or being overly critical (“When I get mad, I say nasty things,” or “When people yell at me, I yell back”). Indirect aggression (five items) includes both roundabout (malicious gossip or practical jokes) and undirected (temper tantrums or slamming doors) aggressive behavior. For example, “I sometimes spread gossip about people I don't like,” and “I can remember being so angry that I picked up the nearest thing and broke it.” Higher scores on this measure indicate more aggressive behavioral tendencies.
Purdue Pegboard test
The Purdue Pegboard test (PPB) 32 is widely used for measuring hand agility and bimanual coordination. The pegboard consists of a board with two parallel rows, each with 25 holes into which cylindrical metal pegs are placed by the examinee. The test involves a total of four trials. The subsets are for preferred hand, non-preferred hand, both hands, and assembly performance using both hands. After one practice trial, subjects were required to place the pins in the holes as quickly as possible, with the score being the number of pins placed in 30 sec (right, left, and both hands) and 1 min (assembly). Poor PPB performance is a sign of deficits in complex, visually guided, or coordinated movements that are likely mediated by circuits involving the basal ganglia. 33,34
Image acquisition
Structural MRI
High-resolution T1- and T2-weighted structural images and DT images were acquired in a single session using a 3.0 T MR system (Intera Achieva 3T, Phillips Medical Systems, Best, The Netherlands). The three-dimensional (3D) T1-weighted turbo field echo (T1TFE) sequence used the following parameters: repetition time [TR] = 8.1 msec, echo time [TE] = 4.6 msec, flip angle = 8 degrees, 175 slices, thickness = 1 mm, and matrix size = 256 × 256.
18F-FDG PET
18F-FDG PET images were acquired using a Phillips Allegro PET scanner (Phillips Medical Systems, Cleveland, OH) in 3D mode. All subjects fasted for at least 6 h before scanning. After intravenous administration of 4.8 MBq/kg of [18F]-FDG, subjects were allowed to rest, while staying awake in a dimly lit room for 40 min during the uptake phase. Ten-minute emission scans and attenuation maps were obtained using a 137Cs transmission source. Attenuation-corrected images were reconstructed using the 3D row-action maximum-likelihood algorithm with a 3D image filter as 128 × 128 × 90 matrices with a pixel size of 2 × 2 × 2 mm.
18FMZ PET
18FMZ was synthesized from 4-methylphenyl-mazenil iodonium tosylate by aromatic radiofluorination in the TRACERlab FX-FN module (GE Healthcare, Milwaukee, WI) according to the literature. 35 4-methylphenyl-mazenil iodonium tosylate, prepared from commercially available isatoic anhydride in five steps based on a previously reported procedure, 36 is commercially available from Bio Imaging Korea Co., Ltd. (Seoul, Korea). 18FMZ PET images were obtained using a Discovery VCT PET/CT scanner (GE Medical Systems, Milwaukee, WI). Dynamic 18FMZ PET was performed on all subjects. The scan commenced with a simultaneous intravenous bolus injection of 18F-FMZ (206.46 ± 9 MBq). We obtained dynamic scans in a sequence of 54 frames (12 frames ×10 sec, 16 frames × 30 sec, 8 frames × 1 min, 18 frames × 4 min) for a total acquisition time of 90 min to satisfy the pharmacokinetic properties of 18F-FMZ in human brain. 20 PET images were reconstructed into a 25-cm diameter, 256 × 256 transaxial matrix using the Fourier rebinning with filtered back projection (FORE-FBP) point ordered-subset expectation maximization algorithm with a 5.4 mm cutoff (GE Healthcare). Attenuation correction was based on a 3.75-mm-thick CT image set.
Statistical analysis
Neuropsychological tests
Neuropsychological assessment was compared between two groups with Student t test using SPSS software 15.0 (SPSS Inc., Chicago, IL).
Structural MRI analysis
Voxel-based morphometry (VBM) is an automated analysis technique used to investigate focal differences in brain anatomy using VBM tools on SPM (Statistical Parametric Mapping, Wellcome Department of Cognitive Neurology, Institute of Neurology, London, UK,
In addition, amygdala and hippocampal volumes were measured manually in accordance with a previously described method. 37 Structures were manually delineated in the coronal plane using a total software package (Syngo.via, Siemens Healthcare, Germany). Amygdala and hippocampal volumes were compared between the boxer group and normal control group by the Mann-Whitney U test.
18F-FDG PET data analysis
Preprocessing and statistical analysis were performed using SPM5 software implanted in MATLAB 7.6 (The Mathworks, Natick, MA). The 18F
18FMZ PET data analysis
All raw Digital Imaging and Communications in Medicine (DICOM) images were converted to 54 analyzed format files in each frame. For realignment of all images, mean images were constructed using the first 30 frame images within the initial 10 min. We then realigned the images from frames 31 to 54 to mean images. After the alignment, all PET images were co-registered to individual T1 3D MR images. All preprocessing of images was performed using PMOD 3.1 software (PMOD Inc., Zurich, Switzerland). Spatial normalization was performed using SPM5. Individual dynamic PET images were spatially normalized to the MNI template. Time-activity curves (TACs) were generated using dynamic PET frames on PMOD software. To examine 18FMZ binding in the brain, we employed established kinetic compartment analysis on TACs using the simplified Reference Tissue Model (SRTM) with the pons as a reference region. 20 Group comparisons between the boxer group and the control group with age as a nuisance variable were conducted with an uncorrected threshold of p < 0.005 set on a voxel value of 30.
For linear regression analysis between neuropsychological parameters and 18FMZ binding potential, the ROI value was extracted based on the group-comparison results using MarsBaR for each activation cluster. The ROI was defined based on the areas with significant changes of FMZ uptake in the group comparison SPM results with proportional scaling in which the images were scaled to a value of 50 using the mean global values obtained in each image. We performed a linear regression analysis of the FMZ ROI values and neuropsychological scores. In addition, we conducted a bootstrap analysis on group comparison. Bootstrap resampling was used to create 1,000 different populations that yielded 95% confidence intervals and BCa confidence interval type using Stata 9.0.
Results
Clinical screening using UPDRS and CBI scale
The UPDRS scores were higher in the professional boxer group than in controls (boxer group sum: 10; normal control group sum: 0), although all subjects were still within the normal range. The CBI scores were higher in the professional boxer group (boxer group sum: 5; normal control group sum: 0); the results of the neurodiagnostic evaluation are presented in Table 3.
BG, boxer group; CBI, chronic brain injury; MMSE, Mini-Mental State examination; NC, normal control group; UPDRS, the Unified Parkinson's disease Rating Scale.
Neuropsychological tests
No significant differences between groups were found in cognition (MMSE), depressive symptoms (BDI), and aggressive behavior (BDHI). Motor impulsiveness from the BIS-11 scale was significantly different between groups. In cognitive tasks, a significant difference between the groups was only found in the RCFT delayed recall scores. There were no significant differences in HVLT scores, RCFT immediate recall, and RCFT recognition scores. Results of neuropsychological tests for the boxer and control groups are presented in Table 4. We tested motor-related performance using the PPB. There was a significant difference in assembly performance between groups (p < 0.05). There were no differences between groups in performances for the right hand, left hand, and both hands. The t test results for the PPB are presented in Table 5.
p < 0.05.
BDI, Beck Depression Inventory; BDHI, Buss-Durkee Hostility Inventory; BIS-11, Barratt Impulsiveness Scale-11, HVLT, Hopkins Verbal Learning Test; MMSE; the Mini-Mental State examination; RCFT: Rey-Osterrieth Complex Figure Test; SD, standard deviation.
p < 0.05.
SD, standard deviation.
Structural brain imaging results: MRI
We conducted two types of structural brain analysis. One is a group comparison using SPM for VBM and the other is the absolute volume extracted using VBM tools. Group differences in GM were considered significant at p < 0.05, FDR corrected. We did not find significant differences in GM using SPM analysis. There were no differences in GM, WM, CSF, and total whole brain volumes between the groups. These results are shown in Table 6 and Figure 1. In an additional analysis, volumes (cm3) of the amygdala [right: boxers, 1.86 ± 0.24; controls, 1.68 ± 0.14 (p = 0.28); left: boxers, 1.89 ± 0.22; controls, 2.03 ± 0.43 (p = 0.98)] and hippocampal [right: boxers, 4.24 ± 0.57; controls, 4.74 ± 0.51 (p = 0.41); left: boxers, 4.47 ± 0.61; controls, 4.4 ± 0.68 (p = 0.73)] did not differ between the boxer and normal control groups (figures not shown).
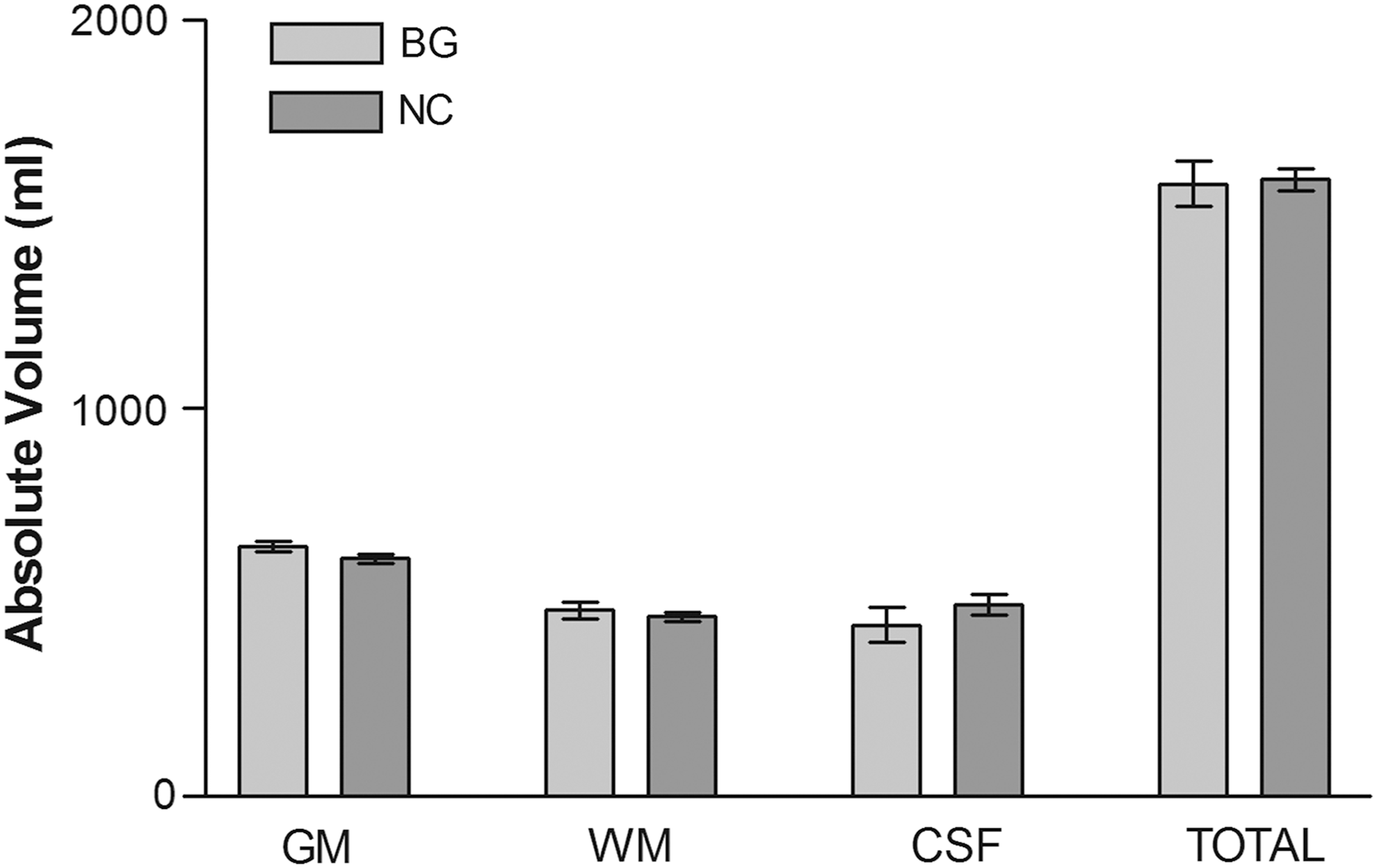
VBM analysis: independent sample t test results comparing groups for absolute volume of GM, WM, CSF, and whole brain total volume. CSF, cerebrospinal fluid; GM, gray matter; VBM, voxel-based morphometry; WM, white matter.
CSF, cerebrospinal fluid; GM, gray matter; n.s., non-significant difference between groups; VBM, Voxel-based morphometry; WM, white matter.
Biomolecular imaging results: 18F-FDG PET, and 18FMZ PET
In the 18F

Rendered images from SPM analysis reveal hypo-metabolism in the boxer group and the normal control group (for resting brain activity), with decreased glucose uptake in the right mOFC and bilateral DLPFC (p < 0.005 uncorrected, k = 50). DLPFC, dorsolateral prefrontal cortices; mOFC, middle orbitofrontal cortex; SPM, Statistical Parametric Mapping. Color image is available online at
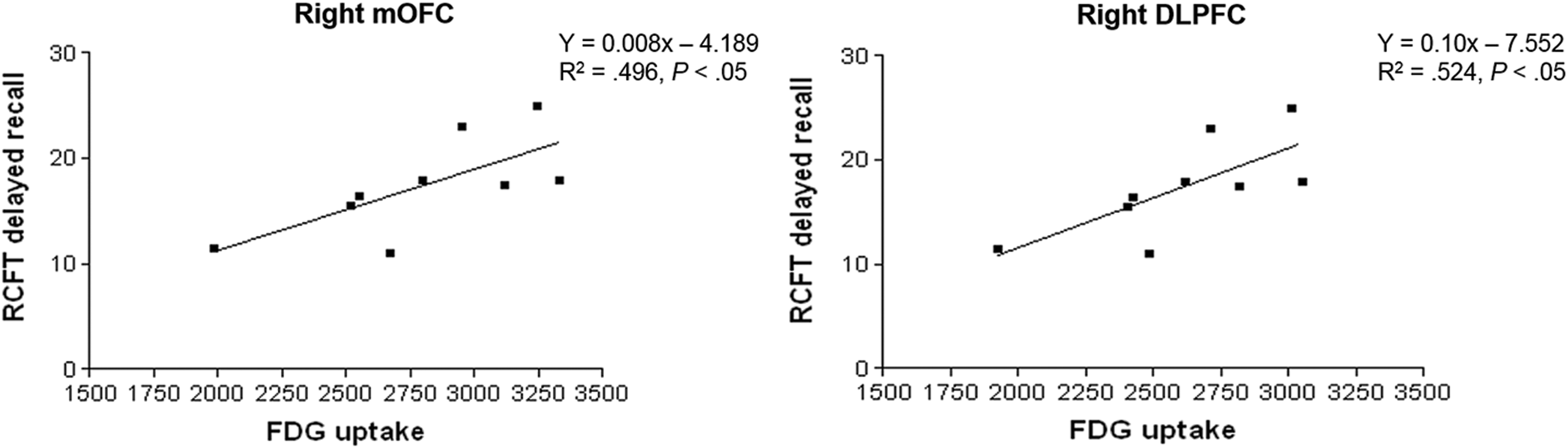
Linear regression analysis between values for brain ROIs and neuropsychological test scores: RCFT delayed recall scores were significantly correlated with 18F
18
t = 3.71; p < 0.005 uncorrected, k = 50.
18F
Group comparisons showed significantly lower FMZ uptake in the left angular gyrus (BA 39), left orbitofrontal cortex, left inferior temporal cortex, left superior temporal cortex, right precuneus, and right cerebellum of the professional boxer group compared with the normal control group (Fig. 4 and Table 8). FMZ uptake was higher in the right post-central gyrus, pre-central gyrus, superior occipital cortex, and inferior parietal cortex in the boxer group than in the control group (Fig. 5 and Table 9) (p < 0.005 uncorrected, extent threshold k = 30). We also conducted a linear regression analysis of the neuropsychological test scores and ROI values of the regions with significant changes in the group comparison results. The RCFT delayed recall score was significantly correlated with FMZ uptake in the left angular gyrus (BA 39) (y = 1.108x −76.105, R
2 = 0.63, p < 0.05) (Fig. 6). PPB assembly scores to assess the motor coordination performance showed a significant correlation with uptake in FMZ ROI regions, without there being any significant relationship with uptake in 18F
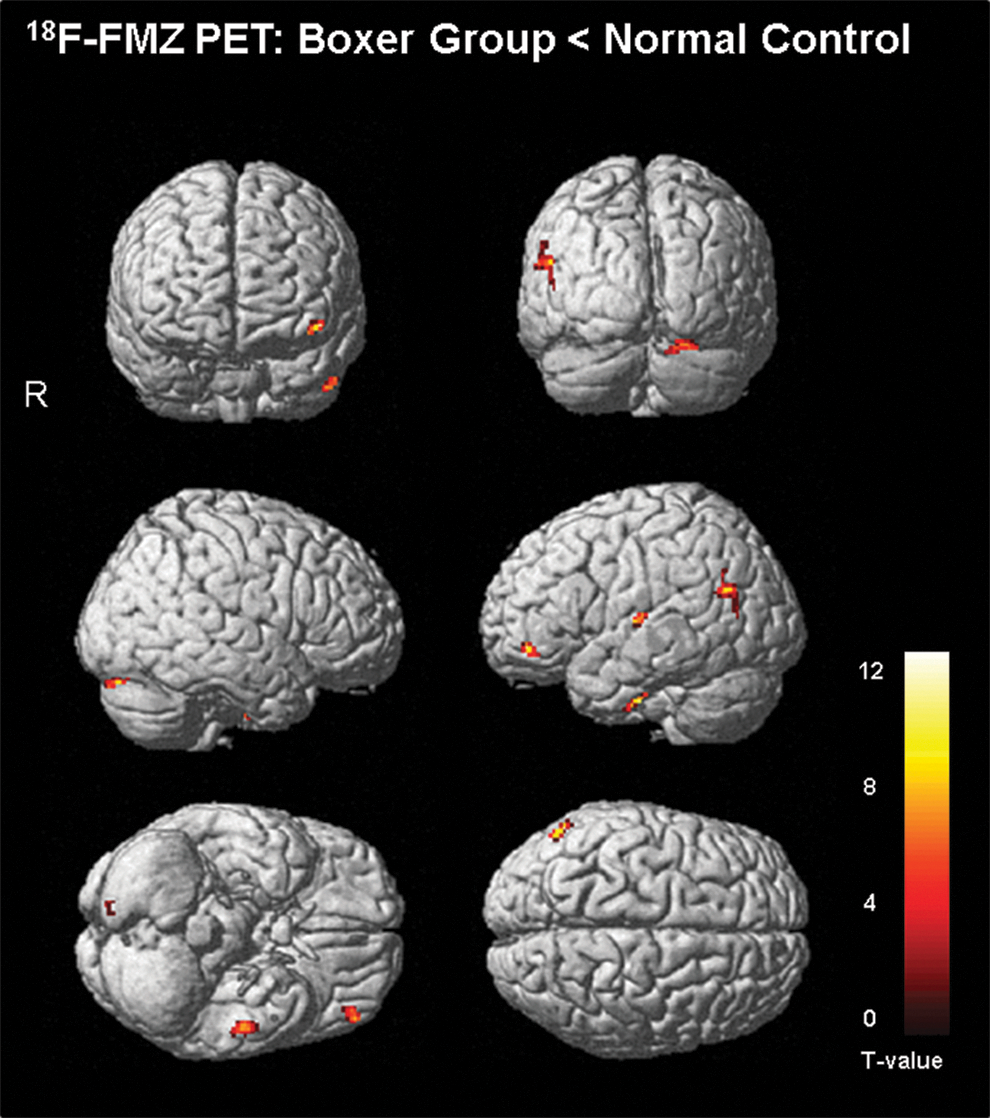
18F-FMZ PET rendered images from SPM analysis showing group comparisons between the boxer group and control groups for the FMZ BP map. Lower FMZ uptake in boxer group than in controls was apparent in the left angular gyrus, orbitofrontal cortex, inferior temporal cortex, superior temporal cortex, right precuneus, and right cerebellum (p < 0.005 uncorrected, k = 30). 18FMZ, 18F-flumazenil; BP, binding potential; PET, positron emission tomography; SPM, Statistical Parametric Mapping. Color image is available online at

18FMZ PET rendered images from SPM analysis showing group comparisons between boxer and normal control groups for the FMZ BP map. Higher FMZ uptake in the right precentral gyrus, postcentral gyrus, superior occipital cortex, and inferior parietal cortex was apparent in the boxer group than in the controls (p < 0.005 uncorrected, k = 30). 18FMZ, 18F-flumazenil; BP, binding potential; PET, positron emission tomography; SPM, Statistical Parametric Mapping. Color image is available online at

Linear regression analysis results for RCFT delayed recall scores: a significant positive correlations between RCFT delayed recall scores and FMZ uptake in the left angular gyrus. 18FMZ, 18F-flumazenil; RCFT, Rey-Osterrieth Complex Figure Test.
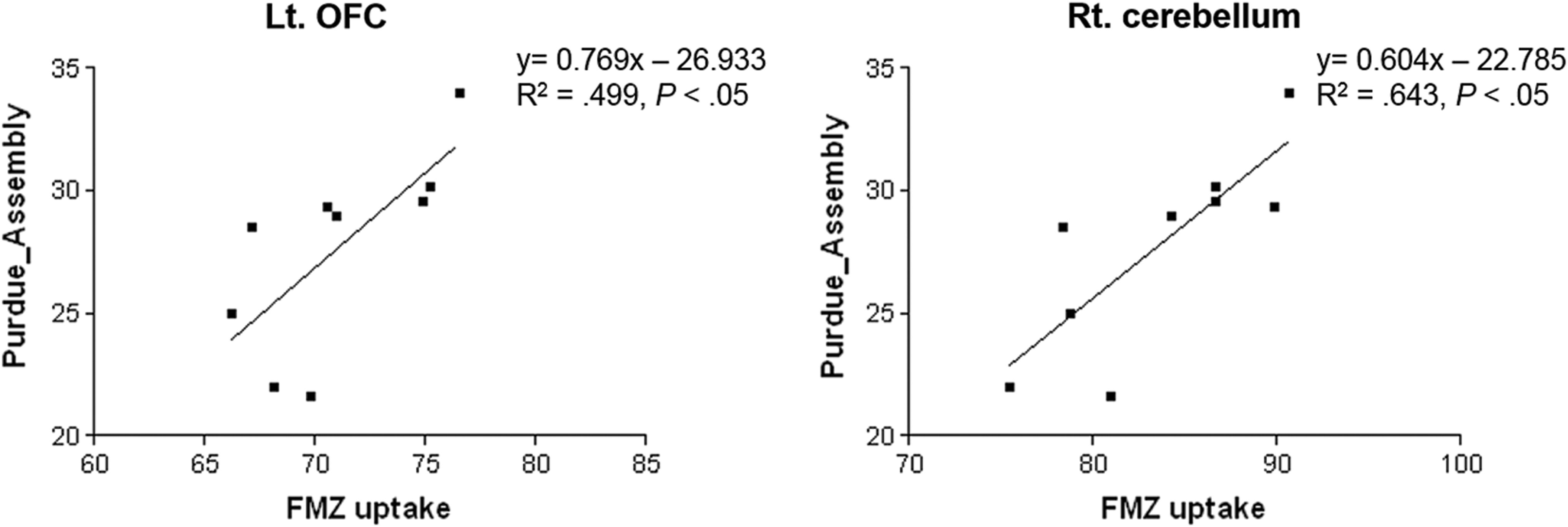
Positive correlations were found between assembly scores to assess motor coordination and FMZ uptake in ROIs in the left orbitofrontal cortex (left) and right cerebellum (right). 18FMZ, 18F-flumazenil; ROI, region of interest.
18
t = 3.71; p < 0.005 uncorrected, k = 30.
18F
18
t = 3.71; p < 0.005 uncorrected, k = 30.
18F-FMZ PET, 18F-flumazenil positron emission tomography; BA, Brodmann area; NC, normal controls.
Discussion
Amateur boxers do not usually exhibit any significant signs of neuropsychological dysfunction,
39
or significant abnormalities when examined using CT and MRI.
8
The level of competition (i.e., professional versus amateur) and the duration of the boxing career may all confer different degrees of CTE risk.
40
For these reasons, we recruited retired professional boxers with careers spanning more than 10 years. This study evaluated the cognitive and motor function of professional boxers using various neuropsychological tests, and investigated brain mechanisms underlying repetitive TBI using structural MRI, 18F
Strictly, CTE can only be definitively diagnosed at autopsy. 41 However, criteria have been proposed for the diagnosis of CTE in patients, and these classify the clinical features into four categories in line with other neurological diseases: definite, probable, possible, and improbable CTE. 39 Neuroimaging studies can provide evidence to support the CTE classification. Jordan also proposed a CBI screening scale to classify CTE in patients with repetitive brain damage. 28 According to the CBI screening criteria, only three of the five professional boxers in our study seemed to exhibit possible CTE. However, we included all of the professional boxers in our analyses because previous studies only considered careers or periods of athletic activity. UPDRS-III and CBI screening provided a wealth of information on the symptoms of subjects.
Most of the neuropsychological tests did not show significant differences between the groups. Professional boxers performed significantly worse than controls in the RCFT delayed-recall, and the “assembly” task in the PPB. Motor impulsivity (sub-score of BIS-11) was higher in the boxer group than in controls, reflecting tendencies to act on the spur of the moment. CTE has previously been associated with mood disorders such as depression, agitation, social withdrawal, poor judgment, and aggression. 4 The PPB provides a reliable measurement for diagnosing compromised motor function under clinical conditions, especially motor coordination involving both hands.
We conducted structural brain imaging using MRI but there were no significant differences in GM, WM, and CSF volumes between groups. Additionally, amygdala and hippocampal volumes did not significantly differ between the groups. Previous studies have revealed difficulties in reliably detecting CBI using CT or MRI scans. 42,43 DTI methods provide insight into the brain's WM microstructures, but few studies have been performed on boxers. Diffusion defects were also found in whole brains of boxers before brain abnormities were detectable on standard MRI. 18
We used various biomolecular imaging techniques to investigate the brain mechanisms underlying repetitive brain trauma. CTE encompasses gait disorders, speech slowing and extrapyramidal signs, and neuropsychiatric and behavioral symptoms. 6 In the first study of repetitive brain injury by Martland in 1928, 44 “punch drunk syndrome” referred to a parkinsonian syndrome that results from long-term cumulative consequences of subclinical concussions to the head. The motor manifestations of CTE such as spasticity, intention tremor, ataxia, dysarthria, and coordination problems, reflect injury to the pyramidal tracts, the extrapyramidal system, and the cerebellum. In the studies by McKee and co-workers movement abnormalities eventually developed in 42% of the 51 CTE patients. 3 In our study, three of the five boxers were diagnosed with some slight impairment of hand movements. Nevertheless, they were still within the normal range for UPDRS scores.
In the resting state, a decrease in glucose metabolism in the brain is commonly thought to reflect functional abnormalities. In our 18F
In previous studies, TBI patients without abnormalities on MRI have demonstrated low BP on 18FMZ PET, which reflects slow neuronal integrity and neuronal cell loss in the brain. 48 Our 18FMZ PET results are consistent with neuronal cell loss caused by repetitive brain damage. In group comparison analyses, significantly lower FMZ uptake was seen in the left angular gyrus (BA 39), left orbitofrontal cortex, left inferior temporal cortex, left superior temporal cortex, right precuneus, and right cerebellum in boxers than in normal controls. These regions of low uptake indicate neuronal damage: damage to the angular gyrus (BA 39) is known to play a role in dyslexia and semantic aphasia 49,50 ; neurofibrillary tau pathology in CTE is found in temporal lobe structures 3 ; and marked cortical atrophy of the right temporal lobe has been observed in boxers. 51 However, increased FMZ uptake was observed in the boxer group compared with the controls, and this increase may have reflected an upregulation of benzodiazepine binding sites. These results suggested the presence of a compensatory mechanism involving the post-traumatic cortical neurogenesis and the endogenous brain-derived neurotrophic factor. 52 Although the damage is selective in TBI, formation of new neurons has been observed in damaged brain circuitry after neuronal injury. 53 Our results showed significant positive correlations between assembly scores and FMZ uptake in the left orbitofrontal cortex and right cerebellum. The orbitofrontal cortex is involved in activation and maintenance of task goals and action selection in behavior. 54 A previous study of the cerebellar involvement in motor function showed that Purkinje cells, which are a class of GABAergic neurons in the cerebellum, have a crucial relationship with motor coordination. 55,56
This study has several limitations that need to be addressed. First, the small sample size was definitely a limitation, even though it was difficult to recruit professional boxers who met our standard criteria. Therefore, in the small population, we conducted bootstrapping as a resampling statistical method involving 1,000 repeated populations in order to strengthen the statistical power. And yet, in a future study, a larger sample size is needed to obtain a smaller variance and higher statistical power of verification. Second, we did not obtain congruity between the 18F
To summarize the important issues raised in this study, the main symptomatology in punch drunkenness can be regarded as parkinsonian and Alzheimer's-like. 7 The molecular brain imaging results in the professional boxers indicated some impairments of cognitive function, hypometabolic rates of glucose metabolism, and lower FMZ BP values, which resemble Alzheimer's-like symptoms. The motor-related deficits in assembly performance and the slight impairments in the hand/finger movements suggested parkinsonism. However, this study indicated that CTE was not an extension of Alzheimer's disease or PD. We suggest that cognitive impairment and motor-related dysfunction are due to neuronal damage caused by CBI in professional boxers experiencing repetitive trauma. These changes were revealed by molecular brain imaging although no abnormalities were seen on structural brain MRI.
Footnotes
Acknowledgment
This research was supported by grants from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HI14C1072) and the National Research Foundation of Korea (NRF) grant funded by the Ministry of Science, ICT and Future Planning, Republic of Korea (NRF-2014M3C7A1046042).
Author Disclosure Statement
No competing financial interests exist.