
Abstract
These are exciting times for the translation of promising interventions for spinal cord injury (SCI) into testing with clinical trials. These interventions include acute surgical decompression, neuroprotection, neural repair, cell replacement, activity-based rehabilitation, and medical devices, including devices requiring surgical implantation. By nature, clinical trials can have strict inclusion and exclusion criteria, which narrow down the pool of potential participants. Meeting enrollment numbers for properly powered trials is a daunting task. Therefore, it is important that trials are designed in a manner that facilitates participation. The purpose of this research study was to learn more about the factors that encourage or interfere with the decision to participate in clinical trials from the perspective of people living with SCI. A multi-national survey was conducted, primarily online, in which 802 participants with SCI ranked 32 factors as facilitators or barriers, using a Likert-type scale. There were 13 universal facilitators, five universal barriers, and three universally neutral factors. The number one facilitator was possible improvement in functionality and the number one barrier was possible decline in functionality—as may be expected. However, many unexpected facilitators and barriers were identified. There also were certain factors that were strong barriers or facilitators to certain sub-groups of people living with SCI. All of these factors should be taken into careful consideration when designing clinical trials so as to promote enrollment and enable adherence to different protocols.
Introduction
T
Recruitment and enrollment for clinical trial participation can be impacted by many factors, as highlighted throughout the literature across diseases. Some of these factors may be less amenable to change due to the research question, such as inclusion/exclusion criteria, and other factors may be dependent upon financial resources, such as the number of trial sites that can be funded. However, once appropriately qualified individuals are identified, there is no guarantee that they will decide to participate in a trial. There has been some study of factors that influence the choice to participate from the perspective of individuals living with cancer, the older adult population, and individuals living with sickle cell anemia 1 –4 . In cancer, for example, barriers to participation that have been identified by potential participants include the understanding of randomization, assignment to placebo or treatment, possible adverse effects, unease with research, complex protocols, financial burden, transportation logistics, and trust in physicians. 1 In the older adult population, for example, barriers to participation in interventional trials include understanding complex documents (e.g., overly complex consent forms), distrust of research, transportation, lack of understanding of the study protocol, concern about excessive intrusiveness, and family members acting as gatekeepers/proxies. 2,3 In sickle cell anemia, barriers to participation include general mistrust of research, emotional and practical concerns, the possibility of randomization, and unknown long-term risks; facilitators include more education—specifically, peer education and improved education in study rationale. 4 In the current study, we chose barriers to be evaluated that are common across the three populations for which there is literature to determine if they are common in the SCI population, as well.
To design clinical trials targeting SCI in a manner that facilitates participation, it is important to obtain information from the perspective of potential participants (i.e., people living with SCI). One method of obtaining information from large numbers of people is to do a survey. The Internet has become a useful tool by which to conduct research. 13 Online research methods have many potential benefits, including the possibility of increasing the geographical span, as well as inclusion of individuals with mobility or communication difficulties. 13 Previous studies show that people with SCI prefer to receive research information over the Internet 5 and important scientific information can be gained from Internet-based research survey to guide research priorities. 6 –9
A survey was developed targeting a multi-national population of individuals living with SCI to determine whether a host of factors, drawn from the literature, were viewed as facilitators or barriers to making a decision to participate in an interventional clinical trial.
Methods
Survey design
A questionnaire was used to acquire information about facilitators and barriers to the decision to participate in interventional clinical trials from persons living with SCI worldwide. The questionnaire was divided into two sections: factors related to clinical trials and demographics. Thirty-two factors related to interventional clinical trials were presented with the instructions to rate whether each would encourage (facilitate) or discourage (be a barrier) participation. A Likert-style rating scale was used from −3 to +3 (-3 strong barrier, −2 intermediate barrier, −1 weak barrier, 0 neither a barrier nor a facilitator, +1 weak facilitator, +2 intermediate facilitator, +3 strong facilitator). This was followed by seven basic demographic questions. The survey was purposefully kept short to encourage participation from a large number of individuals.
The questionnaire was administered online using the software program SurveyMonkey™. A detailed description of SurveyMonkey security features is available at
All survey questions and answer choices are available in the Supplementary Material (see online supplementary material at
Participant recruitment
To qualify for the study, individuals had to have a spinal injury and be 18 years of age or older (obtained via self-report). A waiver of signed consent was granted by the UM IRB. All of the elements of informed consent were described on the study information page, which was displayed on the first page of the survey. Consent and qualification were inferred by agreement and further participation in the survey. Individuals who did not agree to the information provided on the study information page elected to not complete the survey. The survey link was emailed directly to 1,900 individuals living with SCI.
Participants were recruited by word of mouth through people with spinal cord injuries, postings on the World Wide Web, support groups, and multiple consumer organizations, such as the Global SCI Consumer Network, the European Spinal Cord Injury Federation, the United Spinal Association, the Rick Hansen Institute, the Miami Project, the Spinal Cord Injury Network, the Australian Quadriplegic Association of Victoria, the Disability Wellnes Center, the New Zealand Spinal Trust, the Spinal Cord Injuries Association of Turkey, the Nina Foundation, and the Sri Lanka SCI group. Enrollment occurred between March 2014 and August 2014.
Data reporting and analyses
Current age and injury duration groups were reported based on the international SCI basic data set recommendations.
10
For reporting of sample demographics, we followed the International SCI Core Data Set recommendations.
11
Geographical macroregion groupings for Asia and Africa, Canada, Europe (includes the United Kingdom), Latin America and Caribbean, Oceania, and United States were drawn from the United Nations Statistics Division (
For each of the 32 factors, participant responses were analyzed to determine the majority perception. For a response to be considered the majority perception, it had to have a prevalence of at least 50% as a barrier (across −3, −2, −1), facilitator (across +3, +2, +1), or neutral (represented as 0). When a majority perception did not exist, the factor was considered divided. Data were analyzed based on gender, current age group, injury level, injury duration group, and geographical regions described above.
Results
Demographics
A total of 802 participants rated all 32 factors (this represents an estimated 42% response rate base on the information available); however, 33 of those respondents did not provide answers to the demographic questions; therefore, analyses presented here are for the 769 participants who completed the entire survey. The population was 66% male and 50% tetraplegic (15% cervical 1–4; 35% cervical 5–8; 50% thoracic 1-sacral 5). The mean age of the population was 48 ± 13 years (standard deviation). The primary cause of injury was transport related (42%), followed by sports (17%), falls (14%), non-traumatic (13%), other traumatic (8%), assault (5%), and unknown (2%). (These categories were used per the International SCI Core Data Set. 11 ) The mean post-injury duration was 16 ± 12 years (standard deviation), with a distribution of 0.3% <1 year, 22.7% 1–5 years, 19% 6–10 years, 15% 11–15 years, 12% 16–20 years, and 31% > 20 years (these categories were used for reporting based on the international SCI basic data set recommendations). 10 The distribution of participants from macro-geographical world regions was as follows: Asia and Africa, 4%; Canada, 13%; Europe and United Kingdom, 13%; Latin America and Caribbean 3%; Oceania, 11%; and U.S., 56%.
Factors that are universally facilitators, barriers, or neutral
As described in the Methods section, a factor was considered to be universal if at least 50% of the respondents in at least 15 of the 17 sub-groups analyzed rated it as a facilitator, barrier, or neutral (for a full reporting of results for all 17 sub-groups analyzed, see Supplementary Table 1; see online supplementary material at
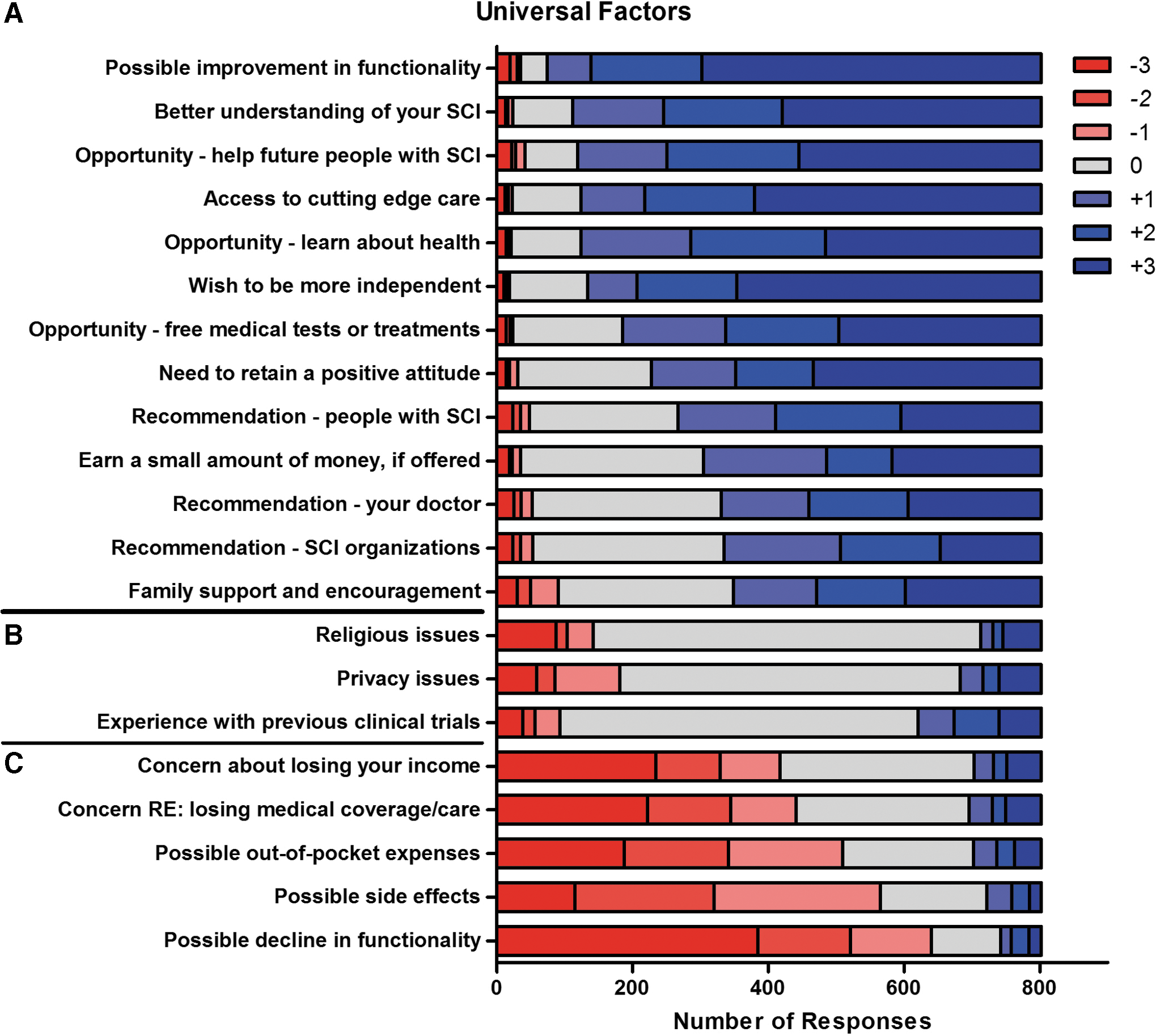
Universal factors.
Factors that were divided
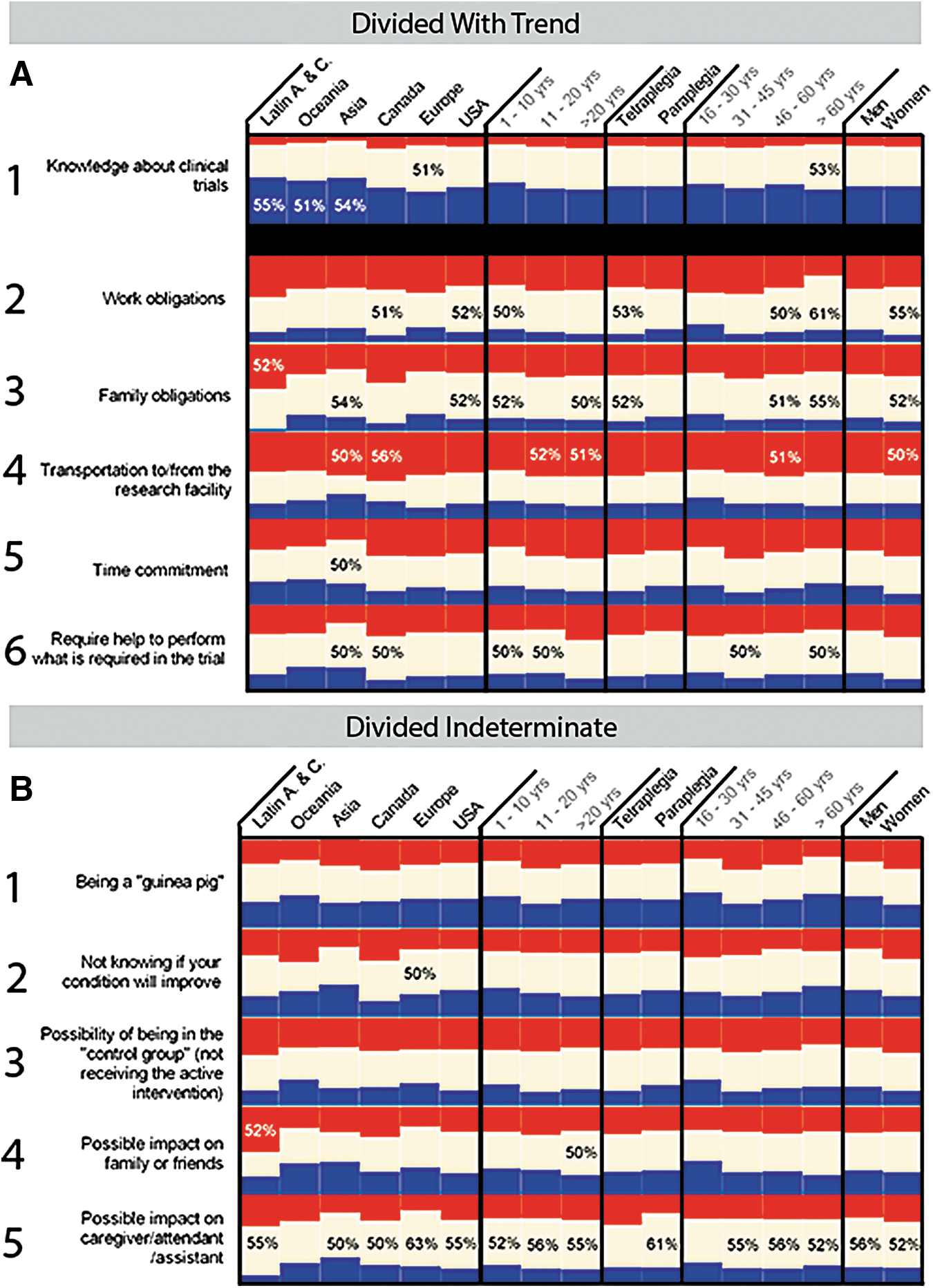
The remaining 11 factors evoked divided responses that overall were not strong facilitators or barriers (Fig. 2). One of the divided factors, knowledge about clinical trials, trended towards being a facilitator, with 89% of respondents considering it to be neutral or a facilitator. Figure 3 shows the variety of responses regarding these 11 factors from the 17 subgroups analyzed. More than 50% of the Latin America and Caribbean, Oceania, and Asian subgroups rated this as a facilitator (Fig. 1A). Five other factors trended towards being barriers (Fig. 3A). Transportation to/from the research facility (Fig. 3A) was a clear barrier for the Asian and Canadian subgroups, the 11-20 and >20 years post-injury subgroups, the 46–60 years age subgroup, and the female subgroup. Family obligations (Fig. 3A) was rated as a barrier by 52% of the Latin America and Caribbean subgroup. The final five factors had no clear trend towards being either a facilitator or a barrier (Fig. 3B). Interestingly, all 17 subgroups were near equally divided on how they rated being a “guinea pig” (Fig. 3B) and possibility of being in the “control group” (Fig. 3B). Possible impact on caregiver/attendant/assistant was close to being scored as universally neutral, with 14 of 17 subgroups viewing it as neutral (Fig. 3B).
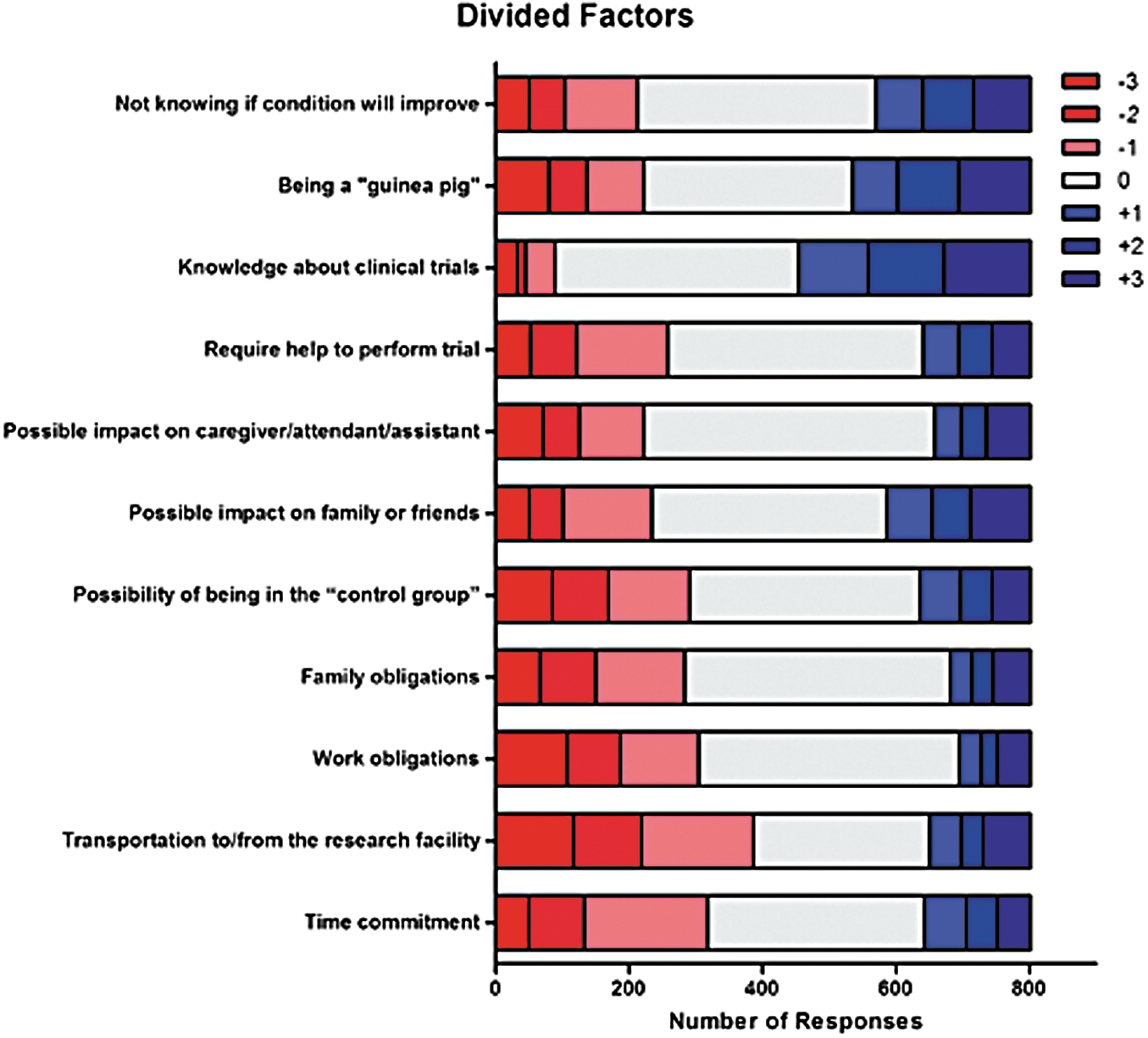
Factors that yielded divided responses. Color image is available online at
Divided factors.
Discussion
A multi-national survey was conducted in which a large sample of individuals living with SCI, primarily chronic injury, ranked 32 factors as facilitators or barriers to their decision making process regarding participation in interventional clinical trials. There were 13 universal facilitators, five universal barriers, and three universally neutral factors.
Some of the high ranking universal facilitators were factors that one would intuitively think would be important when making a decision about clinical trial participation, such as the possible improvement in functionality and the wish to be more independent, which are both related to the ultimate goal of the intervention being efficacious. However, when efficacy is unknown, for example with Phase I trials, or when a control group is required, for example in Phase II and III trials, there are other unexpected factors that can strongly facilitate participation. These include the opportunity to learn more about your general health and to better understand your SCI, recommendation from SCI peers, and the simple desire to participate in something that maintains hope. These are factors that could easily be taken into consideration during the design of trials by creating educational feedback opportunities to participants, as well as engaging other individuals living with SCI to be team members.
Similarly, some of the universal barriers were factors to be expected, such as the possibility of adverse effects and possible decline in function, which are strongly considered when weighing the risk versus benefit probabilities of translating an intervention. However, many barriers were identified that are not related to physical/medical risks—specifically, the possibility of out-of-pocket expenses, concern about losing medical coverage, and concern about losing income. It is true that research procedures in a clinical trial are not charged to the participant. However, if travel is required and not paid for by the research team, it is an out-of-pocket expense; if an attendant is needed to assist with completion of certain tasks for the trial and the cost is not paid for by the research team, it is an out-of-pocket expense. Medical coverage or disability income is often tied to certain definitions of disability (for the U.S., see the Social Security Advisory Board definition of disability. There is a legitimate fear that participating in a clinical trial could improve function enough to disqualify the person from maintaining their medical coverage or disability income, yet not improve function to the degree that those supplements are no longer needed. Similarly, a concern for those individuals who are already working and bringing in a steady income is that the time commitment of participating in a clinical trial may be so onerous that it may negatively impact their work and cause them to lose essential income. All of these factors should be taken into careful and active consideration when designing clinical trials so as to promote enrollment, reduce participant burden, and enable adherence to different protocols.
There also were certain factors that were stronger barriers or facilitators for certain sub-groups of people living with SCI (Fig. 3). There may be a need to tailor design based on “geographic” region, taking into account sociocultural sensitivities. For example, survey participants in Latin America and the Caribbean rated family obligations and possible impact on family/friends as barriers. It would be important to understand more about these concerns, for example, do individuals with SCI living in these countries rely more heavily on family and friends for their care and income? If so, then it would be critically important to design protocols that do not overly burden the family. Transportation to/from the research facility was a barrier for multiple sub-groups (see Fig. 3A). This can be addressed in multiple ways in protocol design, for example reimbursing transportation costs, providing actual transportation, reducing the number of visits to the research facility, and/or using more telemonitoring. Minimizing the time commitment also can reduce the impact on work and family obligations, thus reducing multiple barriers.
Ultimately, when designing clinical trial protocols, a balance has to be made between obtaining the most data possible and actually being able to complete the trial. If a trial is designed in a manner that generates too many barriers, people either will not participate or they will enroll and then drop out—neither of which enables translation. The data presented here have identified multiple barriers that can be removed or lessened and multiple facilitators that can be enhanced in relatively easy ways. One has to be careful, however, that facilitators are not used to the extent that they become coercive. In the end, there is still risk of functional loss and adverse effects when testing experimental interventions and potential participants need to be made aware of the risks that may be involved.
Consumer engagement has been largely untapped in the SCI clinical trial realm. In the cancer literature, there is a strong push for participant advocates, peer mentors, and participant navigators to enhance clinical trial recruitment and retention. 1 The survey results presented here demonstrate that recommendations from SCI peers is a very strong facilitator. Additionally, approaches used in community-based participatory research are recommended by the cancer field, as well, such as the inclusion of community stakeholders in trial design. 1 Results from the current survey can be used as a first step in engaging SCI consumers in protocol design. Community physicians (e.g., physicians who care for people living with SCI who do not have expertise in SCI medicine, or physicians who are not associated with academic medical centers) are also stakeholders who should be engaged. 1 They can be valuable sources of referral to clinical trial investigators and, based on the data presented here, they can facilitate the decision of individuals with SCI to participate (see Fig. 1B). This also could also be a barrier, however, if community physicians are unaware of clinical trials for SCI or have a negative viewpoint. Improved education or awareness of this referral source could be an activity taken on by SCI professional organizations.
A recent systematic review of the literature demonstrates that participant engagement in various types of health care research is highly feasible, can be conducted in many different settings, and via a variety of methods. 12 It has been shown to increase enrollment, help secure funding (note the new and growing Patient Centered Outcomes Research Institute funded by the U.S. government, which is heavily focused on engagement), aid in study design, and of particular importance to help improve the choice of relevant outcome measures. There can be challenges, of course—the most commonly cited ones being the extra time and funding needed for engagement and the worry that “engagement” reflects a token commitment. 12
Limitations
We acknowledge the limitations of this survey: that it was conducted in only English and was administered primarily online. Our sample could therefore be biased towards persons who frequent the Internet and who understand English. We did purposefully keep the survey short in an effort to make it less cumbersome and burdensome to participants. It is impossible to know how many additional individuals saw the survey link due to the wide array of Internet-based recruitment outlets and consumer organizations. The questions and statements also were vetted and edited by individuals in the U.S., Europe, Canada, and Australia prior to being finalized. However, these countries are in developed regions of the world and the language may therefore have been biased towards individuals with a higher education and socioeconomic status. Despite this, there was some feedback from individuals for whom English was their second language regarding the interpretation of some questions. Additionally, the vast majority the individuals who participated in the survey were one year or more post-injury. This could have been due to many factors, such as newly-injured individuals still being in the hospital and/or not yet integrated into the community, therefore not accessible via the recruitment methods used here, or learning about the survey and choosing not to participate. Facilitators and barriers to clinical trial participation may be different in the acute and subacute time period, and that information would likely need to be obtained in a different format, such as in-person interviews.
Conclusion
The value of creating a mutually respected partnership between SCI consumers and researchers to better inform and enable successful clinical trials is well worth any challenges that may need to be overcome. The data presented here provide one avenue by which we can begin to think about changing small but significant aspects in clinical trial design that could have an amplified effect on trial success.
Footnotes
Acknowledgments
The authors would like to thank the partners of this project: the Global SCI Consumer Network; the Rick Hansen Institute; the Institute for Safety, Compensation, and Recovery Research; and the Ontario Neurotrauma Foundation. Importantly, the authors would like to thank all the individuals living with SCI around the world who took the time to provide input for this study.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.