
Abstract
An enhanced understanding of agreement levels between adolescents and parents for reporting athletic events and symptoms can help inform surveillance systems as well as clinical and epidemiological investigations of sports-related concussions. We sought to quantify agreement levels between high school athletes and parents for reporting: (1) number of games; (2) number of practices; (3) occurrence of an injury resulting in any concussion symptoms; and (4) presence of each specific symptom on the date of that injury among high school boys' football and girls' soccer athletes playing in Autumn 2012 in Washington State. There was substantial agreement on reporting the number of athletic events. Agreement levels were greater for games (kappa = 0.82; 95% confidence interval [CI]: 0.79–0.85 in boys' football; kappa = 0.75; 95% CI: 0.72–0.79 in girls' soccer) than for practices (kappa = 0.64; 95% CI: 0.62–0.67 in boys' football; kappa = 0.65; 95% CI: 0.62–0.67 in girls' soccer). There was moderate to substantial agreement on the occurrence of injury resulting in any concussion symptoms; however, agreement on the presence and severity of each symptom varied from poor to almost perfect. Overall, athletes reported greater severity of symptoms than parents did; notably, no difference in mean symptom scores was found when the athlete had a history of concussion. Agreement levels were greater when information was ascertained within 1 week of injury than when it was obtained later than 1 week. Including both athletes' and parents' reports of sports-related events and ascertaining information as soon as possible after injury are important considerations in designing injury surveillance systems.
Introduction
I
While such a study is possible, the logistical, sample size, follow-up time, and cost implications may prove to be prohibitive, especially in large populations. Therefore, concussion surveillance and research may rely on reporting by athletes or key persons such as athletic trainers, coaches, and parents to provide information pertaining to the number of events, injuries, and contributed time at risk. 2 –5 This information is needed to construct estimates of the cumulative incidence or incidence rate of SRCs. The accuracy of such estimates directly depends on the validity of measurement methods and has important implications for interpreting results. Bias can stem from inaccurate estimates in analytic studies in which the risk of injuries is compared between selected groups and in descriptive studies in which the frequency of injuries is assessed in a certain population over a specific period in a defined setting.
There now exists a body of evidence indicating that SRCs are often underreported. 6 –11 In designing a study, investigators are often faced with questions regarding the choice of participants who are most reliable to provide exposure information and concussion symptoms. Current surveillance methods rely heavily on athletic trainers to collect data; however, there are many settings in which the presence of athletic trainers at sports-related events is limited or nonexistent, most notably in youth sports. An enhanced understanding of agreement levels for reporting sports-related events between athletes and key persons may help such decision making. This information gains special importance in studies of high school athletes or younger age groups in which additional data about children and adolescents obtained from adults might be needed.
We conducted a prospective cohort study to examine the incidence of SRCs in boys' football and girls' soccer among high school athletes in Washington State in 2012. 11,12 In that study, we obtained information on athletic events and concussion symptoms on a weekly basis from both parents and athletes. We used athletes' reports of their symptoms throughout the study unless they did not report at all in a certain week; if so, we used parents' reports to maximize the number of athletes on whom we had weekly data.
As such, data collected in that study provided us with a unique opportunity to gauge the validity of using a parent's report in lieu of an athlete's report by examining agreement levels between athletes and parents for reporting sports-related events. In addition, we were able to examine whether agreement levels differed by certain factors for which data had been collected as part of the original study.
Findings in the literature on differential reporting of the number, type, or severity of concussion symptoms by sex remain mixed, 13 –19 and there is a paucity of information on whether agreement levels for reporting sports-related events by athletes and key persons is different between female and male players. In terms of the type of activity, football has historically been the main sport in which serious concerns about concussion have been raised. Accumulated evidence over the past decade, however, on high incidence rates of concussion among soccer players younger than college age has led to heightened awareness about the risk of these injuries in soccer. 19 –25
There is also some suggestion that athletes with a previous concussion may report symptoms differently than those without such a history, 16 but there is a dearth of information on whether experiencing a concussion has an impact on accuracy of reporting subsequent sports-related events. Finally, documenting agreement levels for reporting symptoms by time of data collection after an SRC can directly contribute to the evidence base informing surveillance systems in this area.
Our primary specific aim in this investigation was to quantify the agreement level between athletes and parents for reporting: (1) number of games; (2) number of practices; (3) occurrence of an injury while playing that resulted in any symptoms consistent with a concussion; and (4) each specific symptom on the date of that injury. The secondary specific aim was to examine whether sex or type of sport, type of event, previous concussion status, and timing of information ascertainment on symptoms in relation to the date of injury affected the agreement level.
We hypothesized that the athlete-parent agreement level for reporting sports-related events would be substantial, and that it would be greater for games (than for practices), among athletes with a previous concussion (than those without such a history), and when the information was ascertained closer in time to the date of injury (than when it was ascertained further in time after injury). We further hypothesized that sex or type of sport would not affect the athlete-parent agreement level for reporting sports-related events.
Methods
Study design, setting, and population
Data for this investigation on athlete-parent reporting agreement were obtained as part of a prospective cohort study. One aim of that study was to determine the risk of SRCs among high school athletes. 11 Briefly, a listing of all public school districts (n = 299) in Washington State was obtained and divided into two strata of urban (n = 87) and rural (n = 212) as classified by the Washington State Department of Health. We then sampled districts within each urban or rural stratum, and selected one high school within each district stratum to reach the final sample, with replacement if a school was not interested in participating. High schools had to have a boys' football team, a girls' soccer team, and a boys' soccer team to be eligible. Procedures were piloted on a small sample in boys' soccer before collecting data for the other two groups; in this article, we report results exclusively for boys' football and girls' soccer.
Athletes completed a baseline survey about previous athletic experiences and history of both SRCs and nonsports-related concussions. The preferred contact method (i.e., e-mail, text, or automated telephone call) for the weekly reminder was obtained from both athletes and parents. Athletes and parents were contacted weekly during the 2012 Autumn sports season (i.e., 10 weeks), reminding them to each call a toll-free number that activated an interactive voice response (IVR) system.
Using the keypad of a telephone, athletes reported the number of practices and games in which they participated that week as well as whether they had sustained any blow to the head or body while playing that resulted in any of the symptoms consistent with a concussion outlined in the Sports Concussion Assessment Tool Version 2 (SCAT-2). 26 Hereafter in this article, we refer to such an impact as “injury” for simplicity.
The 22 symptoms used in this study represent three main dimensions of somatic, cognitive, and neurobehavioral
27
–29
(Supplementary Table 1; see online supplementary material at
Statistical analysis
For the purpose of this investigation, we excluded pairs who had no IVR report. From the remaining pairs, we excluded information on pairs who either did not have at least one weekly report each from parent and athlete. A subset of pairs with IVR data reported an injury and subsequently participated in a more detailed telephone interview. For such pairs, we analyzed those with at least one record from each of the parent and athlete matched according to the date of injury.
While athletes and parents reported separately, it is conceivable that they had already discussed with each other sports-related activities during that week; as such, reporting by athletes and parents cannot be considered statistically independent from each other. That dependence, however, was indeed of interest in this investigation; our goal was to examine whether a parent's report can be used as a proxy for an athlete's report. We computed concordance and kappa to gauge agreement levels between athletes and parents for reporting: (1) number of games; (2) number of practices; (3) occurrence of an injury; and (4) presence of specific symptoms after that injury.
Concordance (observed percent agreement) is the proportion of all tested subjects for whom both measurements were the same; it does not account for the level of agreement that chance alone could produce. 30 Kappa, on the other hand, corrects for chance agreement. We used one of the most commonly cited guidelines for interpretation of the agreement level on the basis of kappa statistic as the following: (1) 1.00–0.81: Almost perfect; (2) 0.61–0.80: Substantial; (3) 0.41–0.60: Moderate; (4) 0.21–0.40: Fair; (5) 0.00–0.20: Slight; and (6) <0.00: Poor. 31
The value of kappa depends in part on the true prevalence of the characteristic being measured. Specifically, it has been shown that kappa declines as prevalence of the outcome of interest approaches 0% or 100% in the study population. 32 Because of this limitation of kappa, it has been recommended to present its values alongside concordance to enhance the interpretation of findings. 33 For instance, a high concordance value alongside a low kappa value suggests that the interpretation of agreement is more ambiguous than the one suggested by traditional guidelines. We present values of both concordance and kappa along with their corresponding 95% confidence interval (CI) throughout this article.
Weighted kappa, a variant of kappa typically used for ordinal measures, was also calculated for the ordered categorical variables of interest (i.e., number of games, number of practices, and symptom score) to give “credit” on the basis of how far apart the measurements were. For instance, if the athlete and parent reported the number of practices as 4 and 5, they would receive a larger weight than if they reported those as 4 and 6. As the number of categories increases, weighted kappa effectively approaches intraclass correlation coefficient in magnitude. Among pairs who reported an injury, we determined mean symptom scores for athletes and parents at both composite and item-specific levels. Correlations between symptom scores for athletes and parents were also calculated.
We compared athlete-parent agreement levels by pre-specified factors of type of sport (boys' football vs. girls' soccer), type of event (game vs. practice), previous concussion status (yes vs. no), and interview time in relation to the date of injury (within 1 week vs. more than 1 week). We chose this cutoff point because athletes and parents reported on a weekly basis; as such, it was conceivable that the new events pertaining to the most recent week would cloud their memory for reporting events occurring in previous weeks. Sensitivity analyses were conducted to examine the robustness of findings to the exclusion of outlier observations, specifically pairs in whom the interview for at least one member took place more than 28 days after the injury date.
Kappa statistic asymptotically follows a normal distribution, especially in large samples. To formally compare two kappa statistics, we calculated the difference in absolute kappa values divided by the squared root of the sum of variances of the two estimates to obtain the Z score (i.e., standard normal deviate) and its corresponding p value. All tests were two-sided, the significance level was set at 0.05, and analyses were conducted using Stata (StataCorp, College Station, TX).
Results
A total of 778 athlete-parent pairs were enrolled in the original prospective cohort study. We excluded 102 pairs who had no IVR reports. Of the remaining 676 pairs, we excluded records of 36 male soccer athletes, and 65 pairs who either did not have at least one report each from parent and athlete. In total, data from 575 athlete-parent pairs reporting on 3425 athlete-weeks of play were analyzed. Athletes were distributed across all four high school grades, with the majority being at the 9th or 10th grade. The majority of athletes were non-Hispanic white and did not qualify for the free lunch program, a measure used as a proxy for socioeconomic status. Most athletes had been playing their sport for at least 4 years, and about 20% of them reported having received an SRC diagnosis in the past (Table 1). In total, 143 and 81 pairs of injury reports in boys' football and girls' soccer were analyzed, respectively.
Values are expressed as n (%). Some columns do not add up to the totals because of missing data.
There was substantial agreement between athletes and parents on reporting the number of games and practices using IVR (Table 2) with kappa ranging from 0.64 (95% CI: 0.62–0.67) for number of practices in boys' football to 0.82 (95% CI: 0.79–0.85) for number of games in boys' football. In both sports, kappa was significantly greater for reporting the number of games than for practices (p < 0.01). Weighted kappa values also indicated substantial agreement between athletes and parents on reporting the number of games and practices; however, differences between agreement levels for reporting the number of games and practices were less pronounced than those obtained using kappa, and in girls' soccer, the two estimates were almost identical.
CI, confidence interval.
When stratified by previous concussion status, the same pattern of greater agreement for reporting the number of games than for practices was observed; however, within the category of games, kappa values did not differ by previous concussion status (p = 0.16). Within the category of practices, athlete-parent agreement levels were greater for athletes without a previous concussion (kappa = 0.67; 95% CI: 0.65–0.69) than those with such a history (kappa = 0.61; 0.58–0.64); however, these kappa values were close in magnitude.
Agreement on reporting the occurrence of an injury was substantial with kappa values of 0.62 (95% CI: 0.58–0.67) in boys' football and 0.60 (95% CI: 0.55–0.66) in girls' soccer, respectively (Table 3). In the analyses that focused on pairs who had indicated the presence of any symptom after an injury, the mean symptom score was greater among athletes than among parents in both sports. Correlations between symptom scores for athletes and parents were 0.70 and 0.74 in boys' football and girls' soccer, respectively. The difference in mean symptom scores between athletes and parents was greater among pairs in whom the athlete had no previous concussion than among pairs in whom the athlete had such a history; in fact, mean symptom scores for athletes (mean = 15.6; 95% CI: 11.0–20.2) and parents (mean = 15.3; 95% CI: 9.0–21.6) in the latter group were nearly identical.
The information presented on concordance and kappa pertains to the question on the weekly survey that asked whetherthe athlete had sustained a blow to the head or body while playing in a practice or game resulting in any of the 22 concussion symptoms (“Yes” or “No”). The information presented on athlete mean, parent mean, and correlation pertains to the composite score of 22 concussion symptoms among pairs who were subsequently interviewed because they had answered “Yes” to the question on presence of any symptom after that impact.
CI, confidence interval.
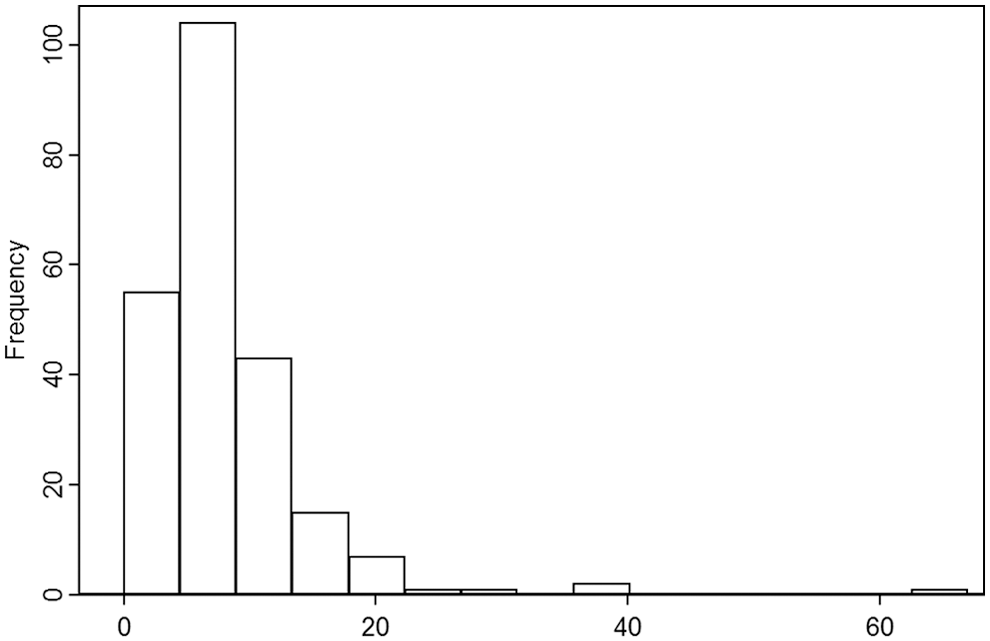
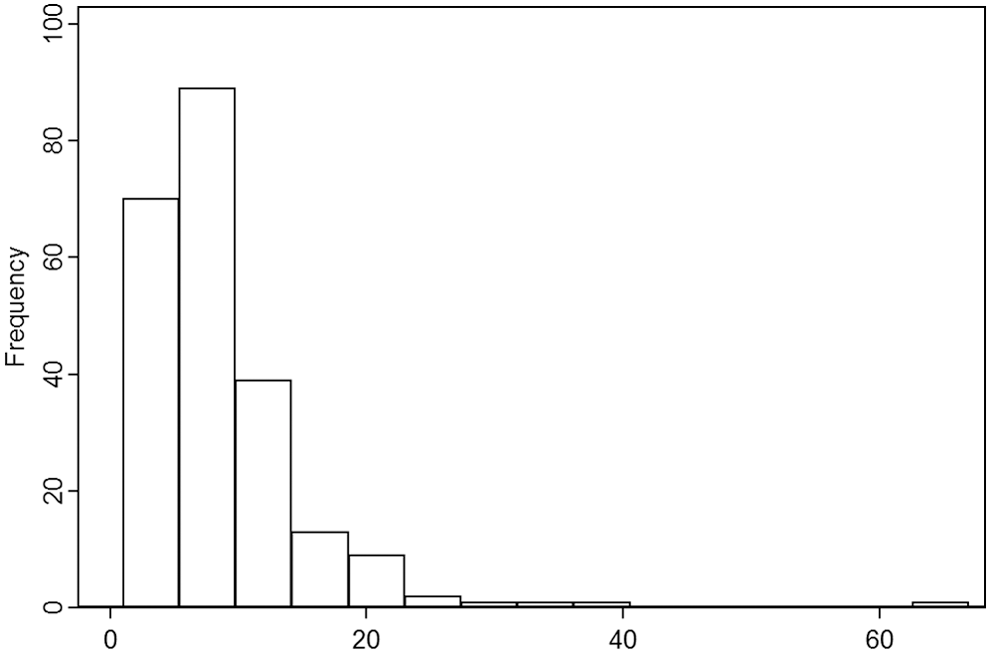
The majority of interviews took place within 1 week after injury (Fig. 1
–3). For 129 pairs, the interview for both athlete and parent took place within 1 week after injury, and for 55 pairs, the delay was greater than 1 week for both athlete and parent. For 28 pairs, the athlete was interviewed within 1 week after injury, while the parent's interview took place later than 1 week; conversely, for 14 pairs, the parent was interviewed within 1 week after injury, while the athlete's interview took place later than 1 week. The correlation between the athlete's and parent's symptom scores was greater when maximum delay between interview and injury dates was less than or equal to 1 week than when it was greater than 1 week (Table 4). The difference in mean symptom scores between athletes and parents was more substantial when the maximum delay was greater than 1 week compared with when it was within 1 week. The exclusion of outlier observations (i.e., pairs with a maximum delay of greater than 28 days) did not materially change the results (Supplementary Table 2; see online supplementary material at

Time of athlete's interview in days after injury date.
Time of parent's interview in days after injury date.
Time of athlete-parent pair's interview in maximum number of days after injury date.
CI, confidence interval.
There was notable heterogeneity in agreement levels by specific symptoms and across the two sports (Supplementary Tables 3–6; see online supplementary material at
In both sports, all three symptom dimensions presented both lower and upper ends of agreement levels; there was no single dimension in which the vast majority of symptoms were reported with low or high agreement levels. For most symptoms, agreement levels were greater when the interview took place within 1 week of injury than when it occurred later than 1 week.
Discussion
We found that there was substantial agreement between athletes and parents on reporting the number of athletic events. The agreement was moderate to substantial for reporting that an injury (i.e., a blow to the athlete's head or body resulting in any symptoms consistent with concussion) had occurred. On the other hand, agreement on reporting specific symptoms after injury varied considerably by type of symptom and across the two sports of boys' football and girls' soccer. For some symptoms, the agreement was only fair, and it further declined to slight or even poor when the information was ascertained more than 1 week after injury. Agreement levels were overall greater for games than for practices, and athletes generally reported greater symptom severity than parents did.
To our knowledge, this is one of the first investigations that examine agreement levels between high school athletes and their parents for reporting the number of athletic events and concussion symptoms. SRCs among adolescents have gained national attention in recent years. 25 There is also an increasing emphasis on improving parents' knowledge about causes, correlates, and consequences of these injuries because they are ultimately in control of whether their adolescent seeks medical care and is removed from play. 34 It is not, however, entirely known to what extent parents are aware of details of their young athlete's involvement in sports-related events, and what factors specifically determine the quality of communication between them if an injury does indeed occur.
Investigations such as ours have the potential to inform injury surveillance systems. A robust epidemiologic surveillance program can provide valuable data on the occurrence of SRCs. Such data may in turn be used to inform the development and evaluation of appropriate interventions to reduce the incidence of SRCs. 25 Much of the national data on SRCs among athletes younger than college age are currently provided by the National Electronic Injury Surveillance System–All Injury Program (NEISS-AIP) through medical record abstraction among persons treated for injuries in participating emergency departments, 35 and the High School Reporting Information Online (High School RIO™) through reports by athletic trainers at participating high school programs. 5
While these two systems provide highly valuable information, neither fully captures all SRCs in this age group. NEISS-AIP only captures concussions in persons who present to emergency departments, and High School RIO only captures concussions identified by athletic trainers at high school settings and for a selected number of sports.
Findings of our investigation suggest that parents may be reasonable reporters of sporting events and concussion symptoms, even though they are bystanders of the injury risk and exposure. Parents are not the ones participating in the athletic events; however, their quantification of time at risk and occurrence of injury does tend to generally agree with athletes who themselves are at risk and exposed. As sports-related injury surveillance systems among youth continue to develop and grow in scope, we may have to rely on parents to track their child's participation in sports and potential injuries.
In the United States President's Budget Request for the Centers for Disease Control in fiscal year 2016, $5 million has been devoted to begin a national concussion surveillance system to determine the incidence of SRCs, including those among youth ages 5–21. 36 This survey will ask parents or caregivers to identify whether each of the children in the household has experienced a recent head injury and describe any symptoms experienced as a result of each head injury. For head injuries that meet established symptom criteria, parents or caregivers will be asked to describe the circumstances surrounding the injury. 37 The accuracy of parental report in such surveillance system will be of paramount importance.
Beyond injury surveillance systems, evaluating athlete-parent agreement levels for reporting symptoms has implications for clinical care. The inclusion of key adults in monitoring and managing symptoms in a child or adolescent is considered essential. 38 Parents need to be able to recognize and act on concussion symptoms experienced by their child. Because adolescents may not report their symptoms at all, or misrepresent or underreport the severity of their symptoms, timely recognition by parents is crucial for the provision of appropriate care. The parent is also an important participant in the treatment and recovery process, including return to school, return to sports, and return to everyday social and home activity. 39
While athletes and parents overall showed substantial agreement on the presence of any concussion symptoms in our study, we found considerable variability between them in reporting specific symptoms. Only a small subset of symptoms were reported with substantial or greater level of agreement between athletes and parents. Notably, difficulty remembering was reliably reported in both sports. On the other hand, trouble falling sleep showed low levels of agreement in both sports. We also found that the pattern of agreement was not consistent in the two sports. For instance, sensitivity to light showed substantial agreement in boys' football but slight agreement in girls' soccer.
Athletes and parents may not understand and react to specific questions about symptoms equally, and parents may not be aware of their child's every specific symptom. For instance, it has been hypothesized that children may report certain symptoms to their parents more readily, or that some symptoms (e.g., cognitive) may be more easily observable than others (e.g., somatic). 27 On the other hand, certain symptoms may be less defined for the child to reliably identify. 38
In a previous investigation of mild TBI, parents and children displayed only modest agreement on the rating of post-concussive symptoms; item-level correlations ranged from −0.01 to 0.40 on Post-Concussive Symptom Interview and from −0.08 to 0.41 on the Health and Behavior Inventory. 40 In that study, correlations tended to be greater on the cognitive symptom dimension than the somatic one.
Similar to results of that study, we also found that athletes overall reported greater symptom severity than their parents did. In our study, we had not planned to formally conduct domain-specific analyses of agreement levels; however, there did not appear to be a clear and recognizable pattern of agreement by symptom dimension as judged by the observed wide ranges of kappa, weighted kappa, and mean symptom scores in each dimension category. Future studies with larger sample sizes of injured athletes can formally address this question. Considering the totality of evidence, investigators have advocated for both parents' and childs' ratings to be collected to fully assess concussion symptoms. 38
We evaluated the impact of several factors on observed agreement levels. One finding of our study was that the agreement on reporting the number of games was greater than that for practices. The difference was particularly notable in boys' football. One explanation might be that games are less frequent, more eventful, and easier to remember than practices. We also found that a shorter delay in ascertaining information on sports-related events was consistently associated with greater agreement levels highlighting the importance of timely data collection.
Several studies have suggested that athletes with a previous concussion tend to be more symptomatic, experience longer symptoms, and at greater risk of repeated injury than those without such a history; 16,41 –43 however, our knowledge on how having sustained a previous concussion may impact the actual reporting of symptoms by athletes and key individuals has been limited.
We hypothesized that athletes with a history of concussion, and their parents, would be more vigilant for concussion and as such would both report symptoms with a heightened level of care resulting in greater agreement levels. We did not find meaningful differences in agreement levels for reporting the number of events by previous concussion status; however, the difference in reported symptom severity between athletes and parents was much more pronounced among pairs in whom the athlete had no previous concussion than among pairs in whom the athlete had such a history. In fact, mean symptom scores for athletes and parents among pairs in whom the athletes had a history of concussion were almost identical in line with our hypothesis. This finding is potentially important because it may indicate that athletes with a history of concussion more freely share the type and severity of their symptoms with their parents after a new injury.
A number of limitations need to be considered for the interpretation of findings. First, we did not include comparable sports among male and female athletes, which in turn limited our ability to make comparisons by sex. Any differences in athlete-parent agreement levels between sports observed in this study could be attributable to the type of sport, sex, or both. Second, about 30% of enrolled athlete-parent pairs either did not report weekly to the IVR system or did not have at least 1 week of IVR data in which both athlete and parent completed a report. If such pairs were different than those who did report weekly to the IVR system in terms of characteristics that have bearing on the level of agreement, it may have introduced bias in our results. For instance, if athlete-parent pairs were more likely to report to the IVR system during weeks when the athlete sustained an impact with symptoms, compared with weeks during which the athlete played but sustained no impact with symptoms, the resulting bias would likely overestimate agreement levels.
Third, our findings only pertain to high school athletes involved in two school sports in one state with the demographic characteristics described previously; they may not be generalizable to other groups such as athletes who are younger, present a different set of demographic characteristics such as race, ethnicity, and socioeconomic status, engage in sports activities outside the school setting, or play sports other than football and soccer.
Finally, as mentioned previously, the value of kappa depends in part on the true prevalence of each symptom. Because the frequency of various symptoms is not expected to be the same, the comparison of kappa values across them needs to be made with caution.
Conclusion
Our findings suggest that athlete-parent agreement on reporting the number of athletic events is substantial, but it varies considerably for the presence and severity of specific concussion symptoms. Athletes report greater symptom severity than their parents do, but agreement is substantial among those with a history of concussion. In addition, the timing of information ascertainment about symptoms experienced on the date of injury has an impact on the agreement level. Including both the athlete's and parent's report of the number of athletic events as well as presence and severity of symptoms, and ascertaining information as soon as possible after injury are important considerations in designing injury surveillance systems as well as clinical and epidemiologic studies of SRCs. From the clinical perspective, it is imperative to inform parents about concussion and discuss symptoms so they can detect this injury in a timely manner in their young athlete.
Further investigations designed to examine agreement levels between athletes, parents, and other key persons among gender comparable sports and younger children are needed to inform practice and policy and reduce the burden of concussions.
Footnotes
Acknowledgment
The authors would like to thank the athletic staff of the participating schools, the athletes, and their parents for their involvement in the study. They would also like to acknowledge the contribution of Christina Schwien, Megan Fesinmeyer, Shana Chung, Matthew Vaughn, Katherine Lepere, Adam Strizich, Asha Thomas, Charla Jones, Denise Hopkins, Sierra Rotakhina, Melissa Rudd, Adessa Churape, Rachel Silverstein, Reba Blissell, Jennifer Maeser, and Christopher Mack.
The study was funded by the Public Health Law Research Program of the Robert Wood Johnson Foundation and by the Seattle Pediatric Concussion Research Collaborative at Seattle Children's Research Institute.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.