
Abstract
Nicotinamide (vitamin B3) was the first drug selected for cross-model testing by the Operation Brain Trauma Therapy (OBTT) consortium based on a compelling record of positive results in pre-clinical models of traumatic brain injury (TBI). Adult male Sprague-Dawley rats were exposed to either moderate fluid percussion injury (FPI), controlled cortical impact injury (CCI), or penetrating ballistic-like brain injury (PBBI). Nicotinamide (50 or 500 mg/kg) was delivered intravenously at 15 min and 24 h after injury with subsequent behavioral, biomarker, and histopathological outcome assessments. There was an intermediate effect on balance beam performance with the high (500 mg/kg) dose in the CCI model, but no significant therapeutic benefit was detected on any other motor task across the OBTT TBI models. There was an intermediate benefit on working memory with the high dose in the FPI model. A negative effect of the low (50 mg/kg) dose, however, was observed on cognitive outcome in the CCI model, and no cognitive improvement was observed in the PBBI model. Lesion volume analysis showed no treatment effects after either FPI or PBBI, but the high dose of nicotinamide resulted in significant tissue sparing in the CCI model. Biomarker assessments included measurements of glial fibrillary acidic protein (GFAP) and ubiquitin carboxyl-terminal hydrolase-1 (UCH-L1) in blood at 4 or 24 h after injury. Negative effects (both doses) were detected on biomarker levels of GFAP after FPI and on biomarker levels of UCH-L1 after PBBI. The high dose of nicotinamide, however, reduced GFAP levels after both PBBI and CCI. Overall, our results showed a surprising lack of benefit from the low dose nicotinamide. In contrast, and partly in keeping with the literature, some benefit was achieved with the high dose. The marginal benefits achieved with nicotinamide, however, which appeared sporadically across the TBI models, has reduced enthusiasm for further investigation by the OBTT Consortium.
Introduction
N
Interest in nicotinamide as a potential therapeutic for TBI was initially triggered by studies showing decreased tissue damage and improved outcome in models of oxidative stress 4,5 and stroke. 6 –8 Critically, nicotinamide has demonstrated considerable therapeutic efficacy in improving neurobehavioral and neuropathological outcome in a number of pre-clinical TBI studies in the lateral fluid percussion injury (FPI) model, as well as lateral and bilateral-frontal controlled cortical impact (CCI) brain injury models. 9 –15
Initial studies in TBI models showed that systemic administration of nicotinamide (500 mg/kg) improves neurofunctional (sensorimotor and cognitive) outcome and provides significant protection against edema, blood–brain barrier permeability, apoptosis, glial activation, and lesion volume expansion. 9,16,17 Further studies showed doses of 50 mg/kg to be efficacious when administered for 5–12 consecutive days post-injury, with a promising 4 h therapeutic window for both sensorimotor and cognitive tasks. 11,12 Most recently, studies have reported significant beneficial effects after chronic infusion of nicotinamide alone 14,15,18 or in combination with progesterone. 19
Nicotinamide rapidly reaches high levels in the brain related to the presence of a specific uptake mechanism 20 and has been used extensively in clinical trials over the past 40 years for the management of a variety of disorders including pellagra, type 2 diabetes, and Alzheimer disease. Because nicotinamide has generally demonstrated good safety/tolerability profiles, it has been affirmed as GRAS (Generally Recognized as Safe) by the Food and Drug Administration (Select Committee on GRAS Substances Database) and is approved for use as a food additive. Therefore, nicotinamide represents a compound that could be moved forward readily into clinical trials for TBI if found to show benefit across brain injury models.
The current study was designed to evaluate the therapeutic efficacy of nicotinamide across three established pre-clinical models of TBI including (1) FPI, 21 (2) CCI injury, 22 and (3) penetrating ballistic-like brain injury (PBBI). 23,24 The specific doses tested (50 and 500 mg/kg) were selected based on key references available in the TBI literature at the time of this study.
Importantly, as a pre-clinical test base for potential clinical trial neuroprotection drugs, OBTT prefers whenever possible to use the intravenous (IV) route as the most clinically relevant route of administration for the patient with severe TBI. In support of using this route of administration for nicotinamide, Sakakibara and associates 25 in 2002 demonstrated that IV administration of nicotinamide reduced infarct volume after transient middle cerebral artery occlusion using doses ranging from 500–750 mg/kg across a variety of rat strains. Similarly, when nicotinamide (500 mg/kg) was administered IV at 2 h post-injury in a stroke model, 26 it reduced infarct volume in both Sprague-Dawley and Wistar female rats, and the reduction in infarct size was larger with IV administration than in previous reports using intraperitoneal (IP) administration. 26
Methods
Male Sprague-Dawley rats (270 to 320 g) were used for all experiments. Animals were housed individually under a normal 12 h light/dark cycle. All experimental procedures were approved by the Institutional Animal Care and Use committee at each respective institution, and experiments were conducted in compliance with the Animal Welfare Act and adhere to the principles stated in the Guide for the Care and Use of Laboratory Animals (National Research Council; 2011 edition), and other federal statutes and regulations relating to animals and experiments involving animals.
Animal models
FPI model—Miami
Animals were anesthetized (70% N2O, 1–3% isoflurane, and 30% O2) 24 h before injury and surgically prepared for parasagittal FPI as described previously. 27 Briefly, a craniotomy (4.8 mm) was performed at 3.8 mm posterior to bregma and 2.5 mm lateral to midline. A plastic injury tube was placed over the exposed dura and affixed to the skull with cyanoacrylic adhesive and dental acrylic. The scalp was then sutured closed, and the animals were allowed to recover before returning to their home cage. After fasting overnight, the animals were anesthetized (70% N2O, 1–3% isoflurane, and 30% O2), intubated (Ugo Basile rodent ventilator; Stoelting), and subjected to a pressure pulse of moderate (1.8–2.2 atm) intensity. 21
Before the FPI, catheters were placed in the tail artery and jugular vein to monitor arterial blood pressure and blood gases and blood sampling for biomarker analysis, respectively. The tail artery catheter was removed after trauma, and the jugular catheter was removed after the 24 h blood draw. Blood gas levels were assessed in arterial samples 15 min before and 30 min after moderate FPI.
FPI served as our sentinel model for assessing the effects of therapies on acute physiological parameters including hemodynamics and blood gases, and the 30 min time point provided an assessment of the effect of TBI and treatment at 15 min after drug administration. Brain temperature was measured indirectly by a thermistor probe placed in the right temporalis muscle, and core temperature was measured by rectal thermistor probe. Sham animals underwent all surgical procedures except for fluid percussion insult. After TBI, the animals were returned to their home cages with food and water available ad libitum.
CCI model—Pittsburgh
Animals were initially anesthetized with 4% isoflurane in 2:1 N2O/O2. The trachea was intubated with a 14-gauge angiocatheter. Anesthesia was maintained using 2% isoflurane in 2:1 N2O/O2. After intubation, rats were placed on a thermal blanket to regulate body temperature (37°C), and the animal's head was placed in a stereotaxic frame. A parasagittal craniectomy (center of craniectomy at AP: +4.0 mm, L: +2.8 mm from lambda) 8 mm in diameter was performed to expose the brain to allow access for the impactor tip of the CCI device (Pittsburgh Precision Instruments, Inc.). CCI at a depth of 2.6 mm at 4 m/sec was performed as reported previously. 22,28 After injury, the surgical area was closed by silk sutures, and animal recovery was monitored by measuring tail pinch and righting reflexes. Sham animals underwent craniectomy only and no CCI.
PBBI model—Walter Reed Army Institute of Research (WRAIR)
All surgical procedures were performed under isoflurane anesthesia (3–5% for induction and 2% for maintenance) and aseptic conditions with careful monitoring of physiological vital signs. PBBI surgery was performed as described previously. 23,29 Anesthetized rats were placed on a thermal blanket to regulate body temperature (37°C), and the animal's head was secured in the stereotaxic device for insertion of the PBBI probe.
After a midline scalp incision, a right frontal cranial window (diameter = 4 mm) was created using a dental drill to expose the right frontal pole (+4.5 mm AP, +2 mm ML to bregma). The PBBI probe was then advanced through the cranial window into the right hemisphere to a depth of 1.2 cm from the surface of the brain. Once the probe was in place, the pulse generator was activated by a computer to release a pressure pulse calibrated to produce a rapid expansion of the water-filled elastic tubing to induce an elliptical shaped balloon (diameter = 0.633 mm, duration = 40 msec) to a volume equal to 10% of the total brain volume. After deflation, the probe was manually retracted from the brain, the cranial opening was sealed with sterile bone wax, and the skin incision closed with wound clips. Sham animals underwent craniectomy only with no insertion of the PBBI probe.
Drug administration
Nicotinamide (MW 122.12) was purchased from Sigma (catalog number N3376), and two specific doses (50 mg/kg or 500 mg/kg each dose dissolved in 1 mL) were tested in each animal model. Nicotinamide was dissolved fresh daily in sterile physiologic (0.9%) saline (30–32°C) using high speed agitation. 16 Once dissolved, the drug was stored in a warm water bath (30–32°C) to prevent precipitation before administration (this was particularly important to avoid precipitates forming with the 500 mg/mL concentration). Note that in preliminary assessments, it was observed that an IV bolus of nicotinamide at the high dose transiently reduced mean arterial blood pressure (MABP), and thus in our studies across the models, both drug and vehicle were administered over 15 min to prevent hypotension while also maintaining blinding.
Each dose was administered via an indwelling jugular venous catheter (in FPI and PBBI models) or tail vein (in the CCI model). The drug was infused in each model at both 15 min and 24 h post-TBI. At each study site, drug doses were prepared and coded by persons other than those who performed the injury and/or performed the primary and secondary outcome assessments (i.e., behavioral testing and histopathological analysis). Group numbers for each study site are summarized in Table 1.
TBI, traumatic brain injury; FPI, fluid percussion injury; CCI, controlled cortical impact; PBBI, penetrating ballistic-like brain injury; WRAIR, Walter Reed Army Institute of Research.
Biomarker blood sample preparation
Blood samples (0.7 mL) were collected at 4 h and 24 h post-injury (before administration of the 24 h dose) and at the terminal end-point. In the FPI and PBBI models, samples were collected from an indwelling jugular catheter and processed as serum. In CCI, plasma samples were obtained via the tail vein using a heparinized syringe. Terminal samples (21 days) were collected via cardiac puncture for all animals. Immediately after collection, blood samples were transferred to 1.2 mL serum clotting tubes, stored at room temperature (RT) for 60 min to allow clotting, and then stored on ice (to prevent protein degradation) until all samples were ready for the centrifugation step.
Tubes were centrifuged at 5000g (RT) for 5 min. The supernatant was then transferred into sterile 1.2 mL Eppendorf tubes and snap-frozen on dry ice and stored at −80°. Each sample was coded for study site, rat number, and sample collection time (i.e., 4,h, 24 h, or final). Sampling for biomarkers that coincided with drug dosing (i.e., 24 h) was performed before drug administration. Samples were shipped via FedEx priority overnight (on dry ice) to Banyan Biomarkers where they were processed to detect ubiquitin carboxyl-terminal hydrolase-1 (UCH-L1) and glial fibrillary acidic protein (GFAP). 30 –33 Details of the biomarker methods are provided in one of the companion articles in this issue. 34
Primary outcome metrics
Descriptions for the outcome metrics for FPI, CCI, and PBBI models have been organized in the following categories: (1) sensorimotor, (2) cognitive, (3) neuropathology, and (4) biomarkers and summarized as concisely as possible to avoid redundancy with other articles in this issue. Additional methods for each of the respective outcome metrics have been provided in the introductory article on OBTT in this issue. 35
Sensorimotor methods
FPI model
Spontaneous forelimb use was assessed using the forelimb asymmetry task. 36 Baseline measures were recorded immediately before FPI and again at 7 days post-injury. The number of times the animal placed either its right (ipsilateral to the injury), left (contralateral to the injury), or both forelimbs on the wall of the cylinder during rearing episodes was scored. Data were normalized for statistical comparison using the following formula: index of asymmetry (IA) = (ipsilateral +½ both)/(ipsi + contralateral + both). The gridwalk task was used to assess forelimb and hindlimb sensorimotor integration. At 7 days post-injury, rats were placed on a wire grid (25 mm square openings) for 5 min. The number of foot faults each rat made per limb was recorded and is expressed as a percentage of the total number of steps taken using that particular limb.
CCI model
Gross vestibulomotor function was assessed on a beam balance task in which the time the animal remained on an elevated, 1.5-cm–wide wooden beam was recorded (up to a maximum of 60 sec). Animals were trained to criteria, and baseline performance was assessed 1 day before CCI injury. Finer components of vestibulomotor function and coordination were assessed using a modified beam walking task that used aversive stimuli (i.e., bright light/loud noise) to motivate the animals to traverse the beam to reach a darkened goal box. 37 Performance was assessed by measuring the latency to traverse the beam. Rats were given three trials per day with a 30 sec intertrial interval (ITI) at 1 day before CCI (pre-injury baseline) and daily for 5 days post-CCI. The primary outcome measure for this task was the mean latency (three trials) to traverse the beam.
PBBI model
Neurological deficits were evaluated at 15 min post-PBBI (before drug treatment) and at 1, 7, 14, and 21 days post-injury using a modified battery of tests. 38 Neurological scores were based on a 12-point sliding scale ranging from 0 (normal) to 12 (severely impaired) comprising the following four neurological tests: (1) contralateral forelimb flexion during tail suspension, (2) shoulder adduction (body upward curling behavior) during tail suspension, (3) open-field circling behavior, and (4) impaired resistance to lateral push (maximum score for each component = 3).
Motor coordination and balance were evaluated using a fixed-speed rotarod task. 29 Before surgery, rats were trained to criteria on the rotarod task (i.e., maintain balance for a minimum of 50 sec at 10 rpm). Rats were tested 1 day before PBBI (baseline levels) and at 7 and 10 days after injury at sequential fixed-speed increments of 10, 15, and 20 rpm for a maximum of 60 sec per trial (two trials/speed; 60-sec ITI). The primary outcome metric for this task was mean latency to fall during each fixed-speed increment (i.e., 10, 15, 20 rpm) across both testing days (mean motor score).
Cognitive testing
The Morris water maze (MWM) task was used for cognitive testing at each site. The diameters of the MWM apparatus used by each laboratory testing site were: 140 cm diameter for the FPI model (Miami), 180 cm diameter for the CCI model (Pittsburgh), and 175 cm diameter for the PBBI model (WRAIR). All trials were digitally recorded for computer software-assisted analysis. The testing protocols used for each model are described below.
FPI model
Spatial learning performance was assessed from 13–16 days post-injury in the FPI model. All rats were given four trials per day with a 60 sec duration, 10 sec reinforcement, and 4-min ITI. Primary outcome metrics consisted of the latency to locate the hidden platform and swim distance. Animals were tested for retention of the hidden platform location in a probe (missing platform) trial at 17 days post-injury.
Working memory was evaluated on post-injury days 20 and 21. For this task, each animal was given 60 sec to find a submerged (noncued) platform. If the rat failed to locate the platform within 60 sec, it was placed on the platform for 10 sec. Five seconds after trial one (location) for the same rat, a second identical trial (match) was conducted. Rats were placed under a heat lamp for 4 min between each paired trial. After running the group of rats as above, the platform was moved to the next location of the maze, and the procedure was repeated with this location. Five paired trials were given for each rat on each testing day.
CCI model
Spatial learning performance was assessed from 14–18 days post-injury in the CCI model. All rats were given four trials per day with a 60 sec duration, 10 sec reinforcement, and 4-min ITI. Latency to locate the hidden platform served as the primary outcome measure. Animals were tested for retention of the hidden platform location in a probe (missing platform) trial at 21 days post-injury. After assessment of spatial learning performance, animals were tested on a visible platform task for 2 additional days (days 19–20) where the platform was raised 2 cm above the water's surface. The visible platform task was used as a control procedure to determine the contributions of nonspatial factors (e.g., sensorimotor performance, motivation, and visual acuity) on MWM performance.
PBBI model
Spatial learning performance was assessed from 13–17 days post-injury in the PBBI model. All rats were given four trials per day with a 90 sec duration, 10 sec reinforcement, and a 30-min ITI. Primary outcome metrics consisted of the latency to locate the hidden platform and thigmotaxic (wall-hugging) behavior. Animals were tested for retention of the hidden platform location in a probe (missing platform) trial at 19 days post-injury.
Histopathological assessments
After behavioral testing, rats were anesthetized and perfused with 4% paraformaldehyde (FPI and PBBI) or 10% phosphate-buffered formalin (CCI). Brains were processed for paraffin embedding/slicing (FPI and CCI) or frozen sectioning (PBBI). Coronally sliced serial sections (1 mm intervals) were processed with basic hematoxylin and eosin stain for quantitative volumetric analysis of the injury. Lesion volume (mm3) was determined by calculating the area of the lesion (mm2) and then by multiplying the sum of the lesioned areas obtained from each section by the distance between sections (1 mm). Ipsilateral and contralateral hemispheric tissue volume (CCI and PBBI) or cortical tissue volume (FPI) were quantified using the same approach. Both lesion volume and tissue volume loss were expressed as a percent of the contralateral (noninjured) hemisphere (CCI and PBBI) or as a percent of the contralateral cortex (FPI). Analysis of FPI relative to cortex rather than the entire hemisphere was used because the focal lesions were quite small, and this also represented the standard approach used in that laboratory.
Biomarker assessments
Initial analysis focused on two biomarkers. Blood levels of the neuronal cell body damage marker UCH-L1 and the cytoskeletal glial protein GFAP were measured at 4 h and 24 h post-injury. Primary outcome metrics consisted of (1) evaluating the effect of drug treatment on blood biomarker levels at 4 h and 24 h post injury and (2) the effect of drug treatment on difference between 4 h and 24 h (delta 24–4 h) levels. UCH-L1 and GFAP (rat) levels were assayed with sandwich enzyme-linked immunosorbent assay described previously. 32,33
OBTT outcome scoring matrix
The primary outcome metrics were summarized in an overall outcome scoring matrix. The OBTT scoring matrix was constructed for the purpose of ranking the therapeutic efficacy of individual drugs across OBTT studies. Each therapy tested can generate a maximum of 22 points at each center (with cognitive outcome given the highest weight) and a maximum grand total score of 66 points across all three TBI models. Details of our overall approach to drug ranking and the scoring matrix were provided in the initial companion article in this issue. 35
Statistical analysis
All statistical analyses were performed using SAS (SAS version [9.2] of the SAS System, © 2002–2008 by SAS Institute Inc., Cary, NC) and Sigmaplot v.11.0 (Systat Software, Inc., Chicago, IL). Data are expressed as mean ± standard error of the mean or median (interquartile range) as appropriate. Physiological data, contusion and tissue volumes, sensorimotor tasks, and probe trial were analyzed with a one-way analysis of variance (ANOVA). Repeated measures ANOVA was used to analyze the hidden platform and working memory task. When appropriate, post hoc analyses using the Student-Newman Keuls test were performed.
Delta 24–4 h biomarker levels were evaluated as the difference between 24 h and 4 h biomarker concentrations. The differences in biomarker concentration and delta among the various experimental groups in each brain injury model were analyzed with the Kruskal-Wallis test followed by a Mann-Whitney U post hoc test and Bonferroni correction. All statistical tests were two-tailed, and a p value <0.05 was considered significant.
Results
Physiological parameters
Physiological parameters of MABP, PaO2, PaCO2, and arterial pH taken in the FPI model (Miami) are provided in Table 2. Physiological variables were taken before and after TBI. All physiological values were within normal range, and there were no significant differences between the various experimental groups in terms of MABP, PaO2, PaCO2, and arterial pH.
TBI, traumatic brain injury; MAP, mean arterial pressure.
Sensorimotor parameters
FPI model
Animals were assessed using the cylinder (forelimb asymmetry) task for spontaneous forelimb use (Fig. 1A). The one-way ANOVA was not significant between groups (p = 0.230). At 7 days post-injury, all injured animals exhibited contralateral forelimb placing deficits with an asymmetry index of less than 0.5. There was a slight trend for improved contralateral forelimb use in TBI animals treated with 500 mg/kg of nicotinamide, but this was not significant.

Sensorimotor outcome. Fluid percussion injury (FPI) model (
Sensorimotor integration was analyzed using the gridwalk test (Fig. 1B). Each forelimb and hindlimb is assessed independently for foot faults. Data are expressed as a percent of total steps for each limb. One-way ANOVA for both contralateral forelimb and hindlimb were not significant between groups (p = 0.423 and p = 0.503, respectively). Similar findings were found for ipsilateral forelimb and hindlimb placement. One-way ANOVA for ipsilateral forelimb and hindlimb was not significant for group (p = 0.569 and p = 0.256, respectively). Nicotinamide treatment did not improve sensorimotor function as assessed by the gridwalk test.
CCI model
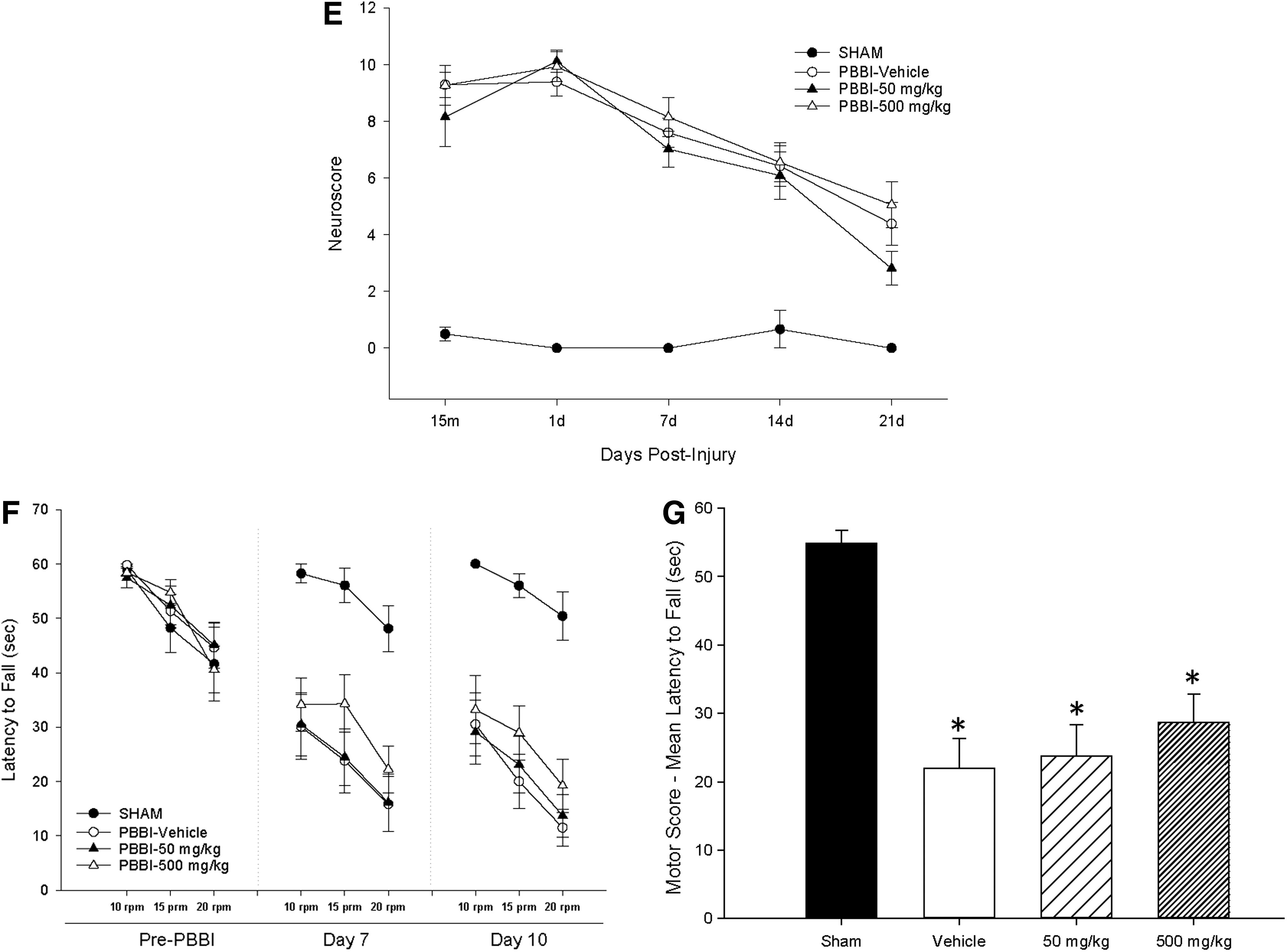
Beam balance performance was determined by measuring the daily latencies to stay on the beam for 5 consecutive days after CCI (Fig. 1C). A repeated measures ANOVA revealed a significant group main effect (p = 0.005) with reduced latencies evident in all three injured groups. Post hoc comparisons, however, showed that only the CCI + vehicle (VEH) and CCI + 50 mg/kg dose treated groups differed significantly from the sham group (p = 0.007 and p = 0.014, respectively). The CCI + 500 mg/kg dose did not significantly differ (p = 0.16) from the sham group, indicating an intermediate beneficial effect of the higher dose of nicotinamide. This intermediate benefit of high-dose nicotinamide generated +1 point for this outcome (half of the total points that could be awarded) in the OBTT scoring matrix.
Beam walking performance was determined by measuring the daily latencies to traverse a narrow beam for 5 consecutive days after CCI. A repeated measures ANOVA detected a significant group main effect (p < 0.0001) for beam walking latencies over 5 days post-injury (Fig. 1D). All injury groups performed significantly worse after CCI versus sham. There were no significant differences between any of the treated and untreated injury groups.
PBBI model
Neuroscore assessments were used to evaluate neurological deficits at 15 min post-injury (before drug treatment) and at 1, 7, 14, and 21 days post-injury (Fig. 1E). ANOVA results revealed significant abnormalities in all injured groups that were sustained out to 3 weeks post-PBBI (p < 0.05) regardless of treatment.
Motor and balance coordination were assessed on a fixed-speed version of the rotarod task (Fig. 1F,G). Repeated measures ANOVA for mean motor performance (four groups × three speeds) revealed significant between-group effects at 7 days (p < 0.001) and 10 days post-injury (p < 0.001) but no significant interaction (Fig. 1F). The overall mean motor score averaged across both testing days was reduced by 60 ± 8% (PBBI + VEH), 60 ± 8% (PBBI + 50 mg/kg), and 48 ± 9% (PBBI + 500 mg/kg) versus sham (p < 0.05) (Fig. 1G). PBBI rats treated with the high dose (500 mg/kg) of nicotinamide showed modest, albeit not significant, improvement on the rotarod task (p > 0.05).
Cognitive testing
FPI model
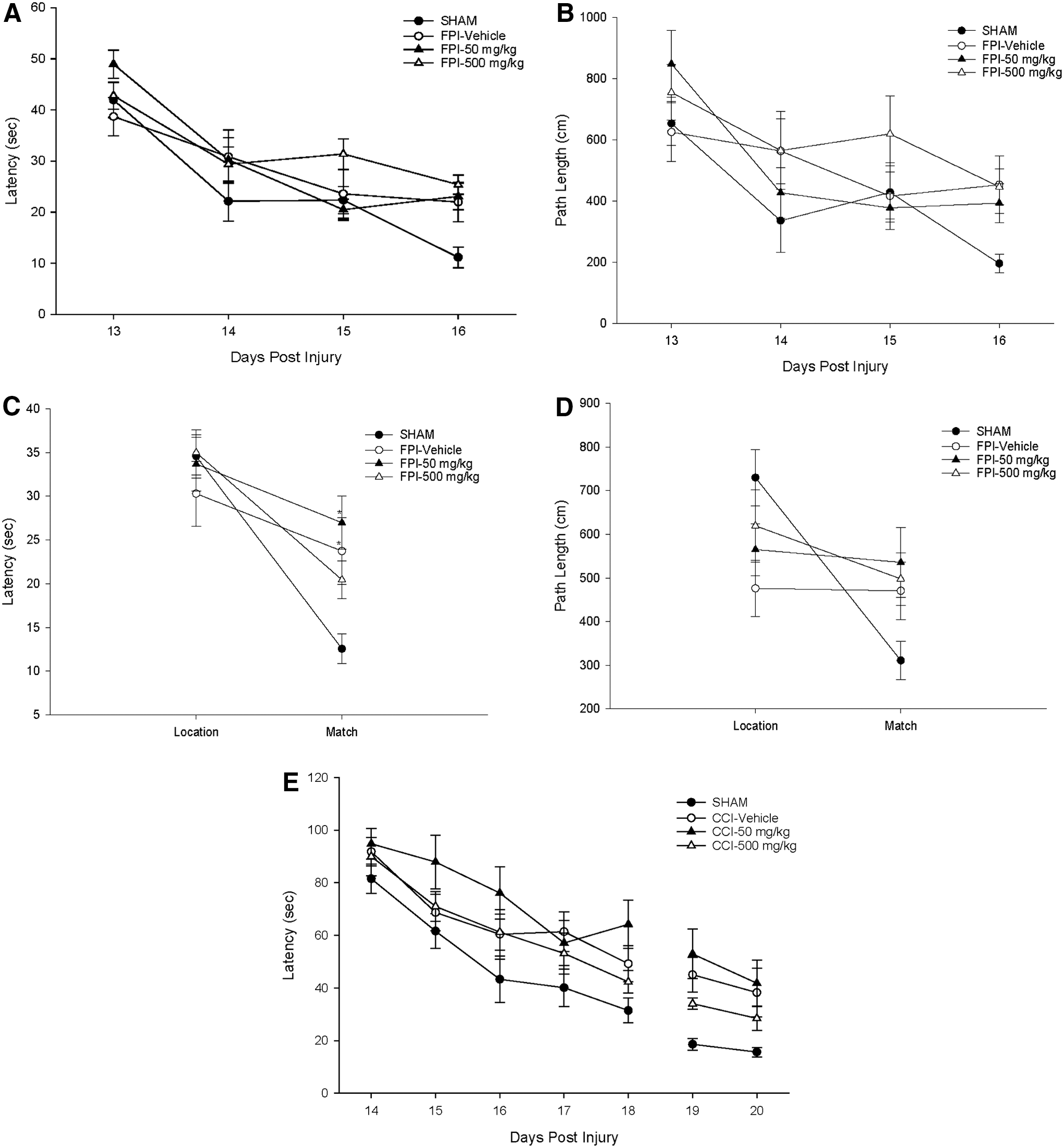
Cognitive function was assessed using a simple place task (Fig. 2A,B) tested over 4 days followed by a probe trial (Fig. 2H,I) then a working memory test (Fig. 2C,D). For the simple place task or hidden platform task, sham animals showed decreased latencies over the 4 day testing period. All three TBI groups had higher latencies than sham. Repeated measures ANOVA for latency was significant for day (p < 0.001) but not for group (p = 0.089) or group × day (p = 0.064). Similar findings were seen in the path length analysis as well. Repeated measures ANOVA for path length was significant for day (p < 0.001) but not for group (p = 0.231) and group × day (p = 0.187).
Cognitive outcome. Fluid percussion injury (FPI) model (
Drug treatment did not appear to improve learning and memory using this paradigm. This result can also be seen in the probe trial analysis. One-way ANOVA was not significant for group (p = 0.489) in the probe trial, although sham animals did appear to spend more time in the goal quadrant than the TBI groups. Note that probe trial is part of the pooled analysis data and is presented for all sites in Figure 2I.
On the working memory task, repeated measures ANOVA for working memory latency was significant for trial (p < 0.001) and group × trial (p = 0.004) (Fig. 2C). Student-Newman Keuls post hoc analysis was significant (p < 0.05) for the sham and FPI + 500 mg/kg groups in performance between the location-to-match trials. While sham animals showed the greatest improvement in the delayed match-to-place task, rats treated with 500 mg/kg nicotinamide demonstrated significant improvement in working memory performance on this task as well. This intermediate benefit again resulted in half (+1) of the total points that could be awarded for this task for the high dose nicotinamide group in the OBTT scoring matrix.
There were no significant differences between groups within the location trial. Significant differences were detected in the “match” trials between sham and FPI + VEH and FPI + 50 mg/kg, however, confirming an injury effect and no benefit of low dose nicotinamide on this treatment. Although there was no significant difference between the FPI + 500 mg/kg group and FPI + VEH, there was a trend for the TBI animals treated with 500 mg/kg to show improvement in the working memory test.
Similar results were seen for the working memory path length analysis (Fig. 2D). Repeated measures ANOVA for working memory path length was significant for trial (p < 0.001) and group × trial ( p = 0.002). Student-Newman Keuls post hoc analysis was significant (p < 0.05) for the sham group in performance between the location-to-match trials. Post hoc analysis within the location trial for groups was significant between sham and FPI + VEH groups. The analysis of group differences within the match trial demonstrated no significant differences between groups.
CCI model
Spatial memory performance was determined by measuring the daily swim latencies to find a hidden platform in the MWM test (Fig. 2E). A repeated measures ANOVA found a significant group main effect (p = 0.034). In this study, there were no significant differences between the sham group versus the CCI + VEH and CCI + 500 mg/kg nicotinamide groups (p = 0.37 and p = 0.45, respectively). The 50 mg/kg nicotinamide group, however, had significantly longer swim latencies that the sham group (p = 0.018), suggesting that the low dose impaired performance with an intermediate detrimental effect. This intermediated detrimental effect resulted in negative half (-2.5) of the total points that could be awarded for this task for the low dose nicotinamide group in the OBTT scoring matrix.
The probe trial (see pooled data, Fig. 2I) measured the percent time spent searching the target quadrant after completion of the acquisition phase of the MWM. A one-way ANOVA revealed a significant group main effect (p = 0.042). Post hoc tests revealed that all three injury groups were significantly different from sham (p < 0.05), indicating an injury effect but no effect of therapy.
PBBI model
Repeated measures ANOVA revealed significant deficits in all injury groups with the average latency to find the hidden platform (across all testing days) increased by 121 ± 13% (PBBI + VEH), 115 ± 12% (PBBI + 50 mg/kg), and 132 ± 13% (PBBI + 500 mg/kg) versus sham (Fig. 2F; p < 0.05). Similarly, swim pattern analysis showed that all injured groups spent a significantly greater percentage of time circling the outer perimeter of the maze compared with sham animals (Fig. 2G; p < 0.05). No significant therapeutic effects were detected on either measure in the spatial learning testing paradigm. In the probe (missing platform) task, a one-way ANOVA revealed a significant group main effects (p < 0.05). Post hoc tests revealed that all three injury groups spent significantly less time searching the target quadrant versus sham (p < 0.05), indicating an injury effect. No beneficial treatment effects were detected in the probe trial (see pooled data, Fig. 2I).
Pooled analysis of therapeutic effects across OBTT
Cognitive outcomes
Figures 2H,I show the effect of nicotinamide therapy across models in OBTT. It is evident from this figure that in this initial drug study in OBTT, the injury severity levels selected in FPI were relatively modest for inducing deficits in latency to find the hidden platform in MWM, but more robust in the more severe CCI and PBBI models (Fig. 2H). Surprisingly, the only significant effect of nicotinamide on this outcome as assessed using this cross-model comparison strategy was a deleterious effect of low dose nicotinamide, as discussed previously. A similar overall lack of benefit was seen in a cross-model assessment of the effect of nicotinamide on the probe trial (Fig. 2I). A trend toward impairment of this outcome after TBI in VEH treated rats was seen in FPI, while significant impairments were seen in both CCI and PBBI. No treatment effect was seen, however.
Histopathological outcomes
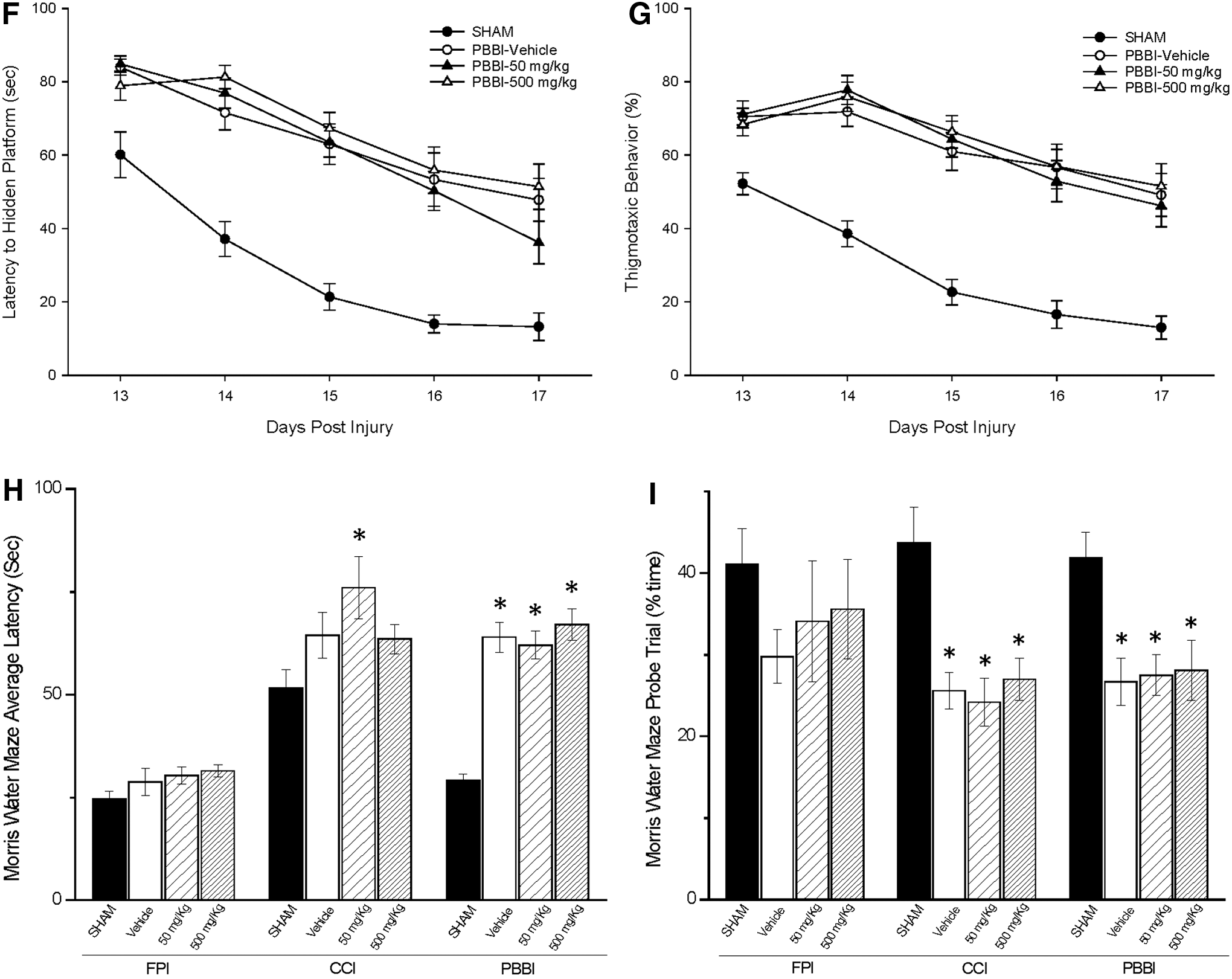
Cross-model comparisons of gross histopathological measurements are shown for FPI, CCI, and PBBI in Figure 3A–E. This includes representative serial sections from each treatment group in each model for general comparison (A [FPI], B [CCI], and C [PBBI]) and the pooled analyses results for lesion volume (D) and tissue loss (E) across the models and treatment groups. These detailed serial section images across the entire hemisphere in each model are presented here in this first treatment article within the investigations of OBTT to allow the reader to appreciate the differences in injury severity across models and to visualize the anatomic location of the damage in each model. Additional images in TBI + VEH treated animals in each model are also presented later in article #7 34 on OBTT in this issue of the journal, which shows the correlations between histology and circulating biomarker levels.
Histopathology. Pictures (left panel) show the extent and placement of the lesion for each traumatic brain injury (TBI) model (
FPI model
There were no significant differences between FPI animals treated with VEH and either dosage of nicotinamide in lesion volume (p = 0.765, Fig. 3D). Results of one-way ANOVA for mean percent change in the ipsilateral cerebral cortex relative to the contralateral (uninjured) side (Fig. 3E) were significant for group (p = 0.002). Post hoc analysis indicated that all three injured groups showed more cortical tissue loss compared with the uninjured sham (p < 0.05). A dose-dependent trend for benefit in cortical tissue loss was detected in the brains of animals treated with nicotinamide versus FPI VEH-treated animals, but this effect was not significant.
CCI model
Lesion volumes (% contralateral hemisphere) were 11.18 ± 1.16, 8.48 + 1.01, 8.36 ± 1.23 for the CCI + VEH, CCI + 50 mg/kg, and CCI + 500 mg/kg groups, respectively (Fig. 3D). There was no significant difference between the nicotinamide and VEH-treated groups. Hemispheric volume loss (% contralateral hemisphere) was 0.24 ± 0.67, 20.73 ± 1.29, 18.08 ± 1.50, and 15.74 ± 1.70, for sham, CCI + VEH, CCI + 50 mg/kg, and CCI + 500 mg/kg, respectively (Fig. 3E). The 500 mg/kg nicotinamide group showed significantly less hemispheric tissue loss versus CCI + VEH (p < 0.05). This was also reflected comparing the 500 mg/kg dose versus the VEH treated group in the serial sections in this model (Fig. 3B). This resulted in full points (+2) for this outcome for the high dose nicotinamide group in the OBTT scoring matrix. In addition, a dose-dependent trend for benefit of nicotinamide on hemispheric tissue loss was suggested by the data.
PBBI model
Nicotinamide did not affect PBBI-induced lesion volume measured at 22 days post-injury (% contralateral hemisphere): PBBI + VEH = 15 ± 2%, PBBI + 50 mg/kg = 15 ± 2%, and PBBI + 500 mg/kg = 13 ± 1% (Fig. 3D). Nicotinamide treatments also failed to reduce PBBI-induced hemispheric volume loss: PBBI + VEH = 25 ± 3%, PBBI + 50 mg/kg = 24 ± 4%, and PBBI + 500 mg/kg = 24 ± 1% (Fig. 3E).
Biomarker assessments
Biomarker data were available on 127 of the 142 rats in this report with missing data resulting from problems with sampling. Effects of drug treatment on post-injury TBI circulating biomarker (UCH-L1 and GFAP) levels are shown in Fig. 4A–C. Treatment effects were also analyzed on the difference in UCH-L1 and GFAP expression detected between 4 and 24 h (delta) post-injury (Fig. 5A–C). This value takes into account the physiological within-subject fluctuation of biomarker levels by comparing an early 4 h time point (reflecting the primary injury) and a delayed 24 h time point (reflecting drug effect, release into blood, and/or clearance).

Box plots illustrating circulating glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) levels at 4 h and 24 h post-injury. GFAP and UCH-L1 concentrations at 4 and 24 h post-injury in fluid percussion injury (FPI) (
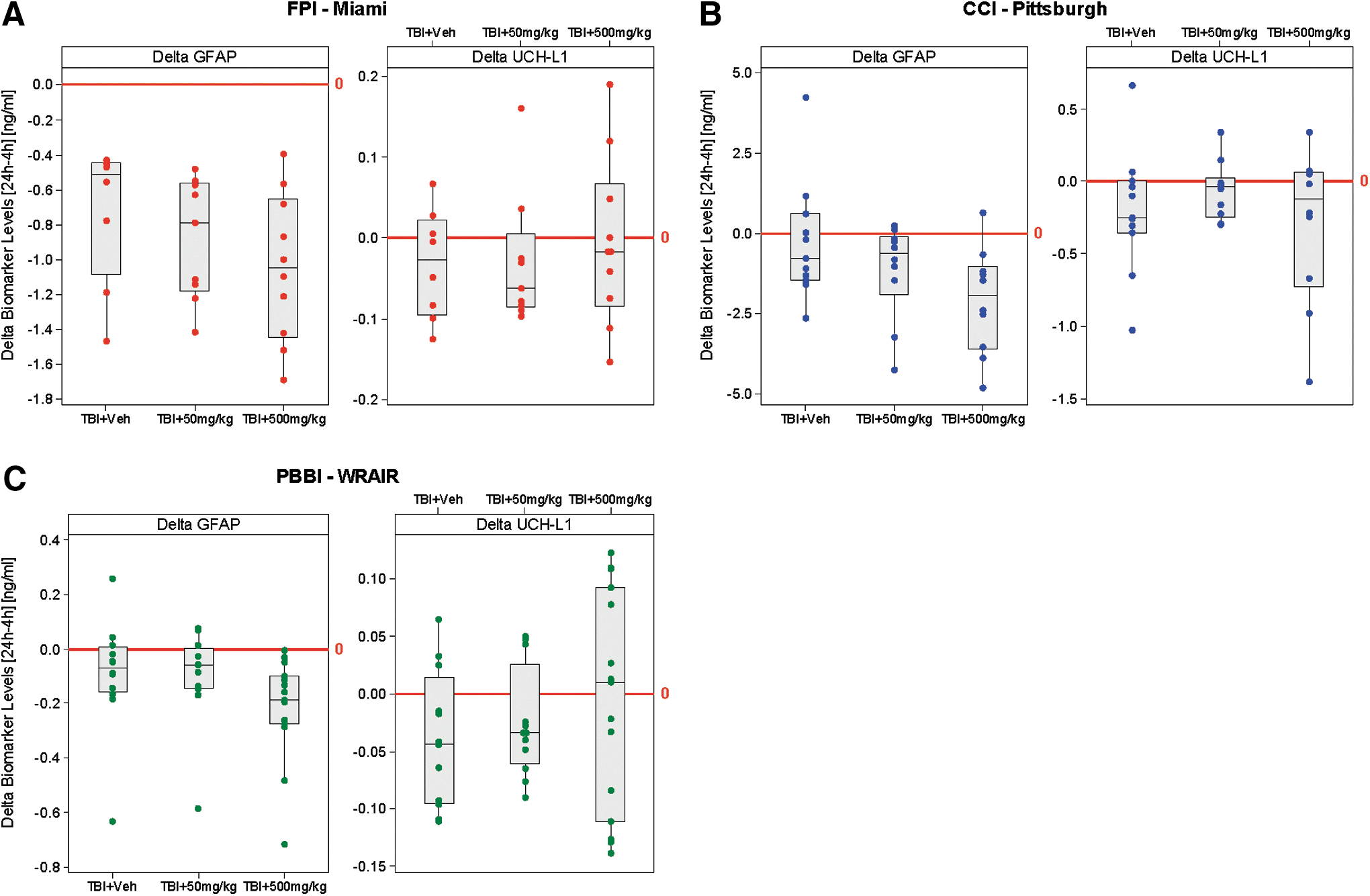
Box plots illustrating delta (24–4 h) circulating glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) levels. Delta 24–4 h GFAP and UCH-L1 levels in fluid percussion injury (FPI) (
FPI model
A Kruskal-Wallis test revealed a significant main effect on GFAP levels at 4 h post-injury (p < 0.0001) with all injured groups demonstrating significant elevations in GFAP (vs. sham) but no evidence of a significant treatment effect. Significant between-group effects on post-injury levels of GFAP were also detected at 24 h post-injury (p = 0.02), but surprisingly, only the low dose (50 mg/kg) treatment group showed significant increases in serum GFAP levels (p < 0.05) versus shams (Fig. 4A). This intermediate detrimental effect resulted in negative half (−0.5) of the total points that could be awarded for this task for the low dose nicotinamide group in the OBTT scoring matrix.
There were no treatment effects on delta GFAP in FPI. In contrast, there were no significant between-group effects on post-injury levels of UCH-L1 at 4 h or 24 h (p = 0.2 and p = 0.7, respectively) and on delta 24–4 h UCH-L1 levels (Fig. 5A).
CCI model
Significant between-group effects on post-injury levels of GFAP were detected at 4 h (p < 0.001) and 24 h (p < 0.001) post-injury. No significant treatment effects were detected at 4 h post-CCI on injury-induced increases in GFAP. At 24 h post-injury, GFAP levels were only significantly increased in the two CCI + treatment groups versus sham (p < 0.05) (Fig. 4B). This may have been influenced by a high degree of variability in the CCI + VEH group, which actually had the highest median value. Nevertheless, this intermediate detrimental effect resulted in negative half (-0.5) of the total points that could be awarded for this task for both nicotinamide groups in the OBTT scoring matrix.
In contrast, there was a strong trend toward a reduction in delta 24–4 h GFAP levels with high dose (500 mg/kg) treatment p = 0.05 versus sham (Fig. 5B), but this did not reach significance. There were no significant between-group effects on post-injury serum levels of UCH-L1 at 4 h or 24 h (p = 0.07 and p = 0.3, respectively) (Fig. 4B) and on delta 24–4 h UCH-L1 levels (Fig. 5B).
PBBI model
Significant between-group effects on post-injury levels of GFAP were detected at 4 h (p = 0.014) and 24 h (p = 0.0003). At 24 h post-injury in the PBBI model, high dose (500 mg/kg) nicotinamide significantly reduced GFAP levels compared with the PBBI + VEH group (p < 0.05), producing a full +1.0 point treatment effect (Fig. 4C). A parallel trend toward improved delta 24 h–4 h GFAP levels was also seen in the high dose group, but this did not reach significance (Fig. 5C). Significant between-group effects on post-injury levels of UCH-L1 were detected at 4 h (p = 0.007) and 24 h (p = 0.0008) (Fig. 4C). Post hoc analysis, however, indicated that only the injured animals treated with nicotinamide (both doses) showed paradoxically higher serum levels of UCH-L1 versus sham animals at 24 h post-PBBI (p < 0.05 low dose; p < 0.001 high dose). This intermediate detrimental effect resulted in negative half (-0.5) of the total points that could be awarded for this task for both nicotinamide groups in the OBTT scoring matrix. There were no significant between-group effects on delta 24–4 h UCH-L1 levels (Fig. 5C).
OBTT outcome scoring matrix
The overall scoring matrix for the effect of nicotinamide across models in OBTT is shown in Table 3. Results from the FPI, CCI, and PBBI models are shown, respectively. Results show that low dose nicotinamide was actually marginally deleterious, receiving negative 4.0 points, which was largely related to its detrimental effect on MWM latency in CCI. In contrast, high dose nicotinamide was marginally beneficial overall (+4.0) with a significant reduction in hemispheric tissue loss versus VEH in the CCI model, an intermediate motor benefit in CCI, and several mixed effects on serum biomarker levels across models. The largest positive overall effect for high dose nicotinamide in any model was a +3.0 score in CCI.
MWM, Morris water maze; GFAP, glial fibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase-L1; WRAIR, Walter Reed Army Institute of Research.
( ) = point value for each outcome within each model.
Drug: Nicotinamide; Dose 1 = 50 mg/kg; Dose 2 = 500 mg/kg.
Discussion
In the current study, the OBTT consortium evaluated the therapeutic efficacy of nicotinamide across three established rat models of TBI using a dosing regimen similar to that which was used in studies published previously. Of the two doses tested, the low dose (50 mg/kg) failed to show any therapeutic effect and, in fact, generated some negative scores on serum biomarker levels of GFAP (FPI model) and UCH-L1 (PBBI model) and on cognitive outcome in the CCI model (Table 3). In contrast, and partly in keeping with the literature, the high dose of nicotinamide produced some modest benefit, including improved motor function and reduced tissue damage in the CCI model, an intermediate benefit on working memory in the FPI model, and a benefit on GFAP levels in PBBI.
Initial studies, investigating nicotinamide as a TBI therapeutic, used bolus IP injections of 500 mg/kg after bilateral frontal and unilateral CCI. The results of those studies consistently demonstrated significant therapeutic effects on neurobehavioral (motor and cognitive) measures along with marked reductions in edema, astrocytosis, apoptosis, and lesion size. 9,16,17 Subsequent studies comparing doses of 50 and 500 mg/kg (CCI and FPI models) found that both doses provided acute neuroprotection, with greater efficacy evident at the higher (500 mg/kg) dose, particularly on cognitive outcome measures. 13,39 In addition, studies investigating the time frame for nicotinamide administration have demonstrated a promising 4–8 h therapeutic window in TBI models with repeated dosing over multiple days. 11,12
More recently, several studies have reported results of chronic administration of nicotinamide after CCI. 14,18,19 In those studies, CCI-injured rats were treated with an initial loading (75 mg/kg) dose of nicotinamide delivered at 4 h post-injury, immediately followed by a 3–7 day continuous infusion via Alzet osmotic minipumps. Results showed improvement in neurobehavioral and neuropathological measures consistent with those observed in previous studies using bolus IP dosing regimens.
Importantly, while nicotinamide has demonstrated significant therapeutic efficacy across TBI models, negative results have been reported as well. With the exception of an intermediate effect on edema, a study examining the effects of nicotinamide administration on aged (14 month) rats failed to demonstrate any significant beneficial effect on behavioral or histopathological measures. 40 Moreover, that same study identified trends indicative of deleterious effects that were most evident at higher doses, suggesting age as a critical variable to be considered with respect to treatment efficacy.
In the current study, it is evident that the injury levels were relatively modest for inducing motor deficits in the FPI model, but more robust in the more severe CCI and PBBI models. This resulted in a wide range of injury severities for measuring putative therapeutic effects. Regardless, when measured across all three OBTT TBI models, the overall beneficial effects of nicotinamide were intermittent at best.
Specifically, results showed an intermediate effect on balance beam performance with the high dose in the CCI model. No significant benefit was detected, however, on any other motor task across the OBTT TBI models. This was surprising, given that sensorimotor/motor recovery represents one of the most consistently reported benefits of nicotinamide in both the FPI and CCI models. 9,11 –13,16,17,39 In keeping with this seemingly “hit or miss” pattern, modest improvements measured on cognitive outcome by nicotinamide treatment in the FPI model were countered by evidence of significant deleterious effects after administration of the low (50 mg/kg) dose of nicotinamide in the CCI model.
The most novel and significant effects of nicotinamide treatment in the current studies were obtained from blood biomarker analysis of post-injury GFAP levels. Despite remarkable differences in the models reflecting a range of injury severity levels and heterogeneity, GFAP was significantly increased at 4 h and/or 24 h post-injury across all three TBI models. Importantly, at 24 h post-injury, consistent with an injury-specific treatment response, no significant therapeutic effects were detected in the FPI model, whereas a trend toward reduced serum GFAP levels was detected in the CCI model. This trend was only evident in the high dose nicotinamide group and appeared in conjunction with the tissue sparing effect of nicotinamide in the CCI model.
Similarly, at 24 h post-injury, the high dose (500 mg/kg) nicotinamide significantly reduced serum GFAP levels versus the VEH group in the PBBI model, suggesting either reduced secondary injury or reduced magnitude of the blood–brain barrier breakdown 40 by high dose nicotinamide. It is also interesting that, consistent with the modest deleterious effects of low dose nicotinamide across models, the serum biomarker data also suggested modest deleterious effects of low dose treatment across models.
Given the tissue sparing effects of high dose nicotinamide in the CCI model, it is possible that this drug is reducing secondary injury, particularly in astrocytes. These findings also suggest that serum GFAP may represent a sensitive marker for injury effect on histology. This is discussed in greater detail later in the investigations by OBTT of levetiracetam, where a very specific theranostic effect was observed, and in the summary article. 41,42 We did not see significant increases in GFAP or UCH-L1 in any of the models at 21 days post-injury (data not shown). Other markers of delayed injury (i.e., autoantibodies, miRNAs, etc.) might present themselves to be more germane to developing neurodegenerative processes such as chronic traumatic encephalopathy, and thus future studies will continue sample collection to 21 days post-injury.
Conclusion
The current study showed that the high dose of nicotinamide produced some modest beneficial effects across the TBI models. The effects, however, did not display a consistent pattern across the TBI models and were often countered by evidence of modest deleterious effects at the low dose. While the results of this study were disappointing, we cannot rule out that better results may have been obtained with different dosing regimens or extended treatment durations. Because nicotinamide was the first drug selected for investigation by the OBTT consortium, we were not able to take into account more recent publications demonstrating improved beneficial effects after low-dose chronic infusion of nicotinamide in TBI models. Thus, while the results of the current study preclude any further investigation of nicotinamide by the OBTT consortium, there is evidence to indicate this compound may be worthy of further consideration using extended dosing regimens or as a combination therapy.
Footnotes
Acknowledgment
We are grateful to the U.S. Department of Defense grants WH81XWH-10-1-0623 and WH81XWH-14-2-0018 for generous support. We would like to thank Col. Dallas Hack for his strong support of our program, his vision for TBI research, and his scientific input. We also thank Dr. Kenneth Curley for his administrative support and his many contributions to identification of emerging therapies. We thank Dr. Brenda Bart-Knauer for her support of our program and her administrative assistance. We thank Linda Ryan for administrative support with budgetary issues across the consortium, Fran Mistrick for other administrative and coordinating support, and Marci Provins and Natalie Nieman for assistance with manuscript preparation, and Vincent Vagni for assistance with Figure preparation. We thank Rebecca Pedersen, Justin Sun, Ofelia Furones-Alonso, Milton Martinez, Juliana Sanchez-Molano, William Moreno, Ryan Treu, Jessie Truettner, Hong Q. Yan, PhD, Michelle Ma, Jeremy Henchir, and Keri Feldman for outstanding technical support in the individual TBI models across the consortium.
This material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the authors, and are not to be construed as official, or as reflecting true views of Department of the Army or Department of Defense.
Author Disclosure Statement
Dr. Hayes owns stock and is an officer of Banyan Biomarkers Inc. Dr. Hayes is an employee and receives salary and stock options from Banyan Biomarkers Inc. Dr. Wang is a former employee of Banyan Biomarkers Inc. and owns stock. Drs. Hayes and Wang also receive royalties from licensing fees and as such all of these individuals may benefit financially as a result of the outcomes of this research or work reported in this publication. For the remaining authors, no competing financial interests exist.