
Abstract
Traumatic intracerebral hemorrhage (TICH) represents 13–48% of the lesions after a traumatic brain injury (TBI). The frequency of TICH-hemorrhagic progression (TICH-HP) is estimated to be approximately 38–63%. The relationship between the impact site and TICH location has been described in many autopsy-based series. This association, however, has not been consistently demonstrated since the introduction of computed tomography (CT) for studying TBI. This study aimed to determine the association between the impact site and TICH location in patients with moderate and severe TBI. We also analyzed the associations between the TICH location, the impact site, the production mechanism (coup or contrecoup), and hemorrhagic progression. We retrospectively analyzed the records of 408 patients after a moderate or severe TBI between January 2010 and November 2014. We identified 177 patients with a total of 369 TICHs. We found a statistically significant association between frontal TICHs and impact sites located on the anterior area of the head (OR 5.8, p < 0.001). The temporal TICH location was significantly associated with impact sites located on the posterior head area (OR 4.9, p < 0.001). Anterior and lateral TICHs were associated with impact sites located at less than 90 degrees (coup) (OR 1.64, p = 0.03) and more than 90 degrees (contrecoup), respectively. Factors independently associated with TICH-HP obtained through logistic regression included an initial volume of <1 cc, cisternal compression, falls, acute subdural hematoma, multiple TICHs, and contrecoup TICHs. We demonstrated a significant association between the TICH location and impact site. The contrecoup represents a risk factor independently associated with hemorrhagic progression.
Introduction
T
The contrecoup phenomenon has been a matter of discussion for many decades. Several theories explaining the mechanism of production of TICH have been postulated. 13 –17 The relationship between the site of impact and TICH location has been widely described in autopsy-based series. This association, however, has not been consistently demonstrated since the introduction of computed tomography (CT) in the study of TBI. Only a few studies in the literature are based on CT scans to study the frequency of contrecoup TICH. 18,19
The primary objective of our study was to determine the association between the impact site and TICH location in patients with moderate and severe TBI. At the same time, the frequency and location of the contrecoup TICH were determined.
As a secondary objective, we analyzed the associations between TICH location, the impact site, the mechanism of production (coup or contrecoup), and TICH-HP.
Methods
Inclusion and exclusion criteria
We retrospectively analyzed the records of 408 patients older than 15 years of age who were consecutively admitted after having a closed (nonmissile) moderate or severe TBI, which was defined as a score of 3 to 13 points on the Glasgow Coma Scale (GCS) after nonsurgical resuscitation within the first 48 h after trauma, between January 2010 and November 2014 at University Hospital 12 de Octubre, Madrid.
For the analysis of the impact site and TICH location, the inclusion criterion was to exhibit one or more TICH on the initial or control CT. We identified 177 patients with a total of 369 TICHs. The impact site could not be determined in 19 cases. Therefore, we performed the subsequent analysis based on a total of 350 TICH.
To determine the progression of TICH, 16 patients were excluded because of the lack of a control CT as the result of death (n = 10) or an immediate neurosurgical procedure including evacuation of the TICH (n = 6). Therefore, 161 patients with 343 TICHs met the selection criteria.
Analysis of the geometric relation and the study of hemorrhagic progression were both performed based on individual TICH rather than individual patients (Fig. 1).

Flow diagram of patients who met the inclusion/exclusion criteria for the study population. TBI, traumatic brain injury; TICH, traumatic intracerebral hemorrhage.
Variables assessed
We collected radiologic, demographic, clinical, and treatment information; this information is summarized in Table 1. Data were collected at the bedside in a standardized manner based on previous research 20 –23 and were also used to create the TBI database of 12 de Octubre Hospital. 24,25
tSAH, traumatic subarachnoid hemorrhage; IVH, intraventricular hemorrhage; EDH, epidural hematoma; SDH, subdural hematoma; TICH, traumatic intracerebral hemorrhage.
Radiological and geometric variables
The radiological features that we analyzed are summarized in Table 1. The initial CT scan was defined as the scan performed immediately after a patient was admitted to the hospital. The control CT scan was performed following the protocol of the Intensive Care Unit (ICU) of our hospital, approximately 4 to 6, 12, 24, and 48 to 72 h after TBI, considering the time between the TBI and first CT, 26 or after clinical deterioration or increased intracranial pressure (ICP). The control CT was defined as the scan with the poorest radiologic features. 27 The times between the head trauma, initial CT, and control CT were recorded.
CT scans were classified according to the Marshall 28 classification and individual radiological features, including the following: (a) traumatic subarachnoid hemorrhage (tSAH), which was defined as the presence of blood in the subarachnoid space either over the convexity or fissures or in the basal cisterns; (b) intraventricular blood (IVH), which was categorized as present or absent; (c) basal cisterns, which were categorized as normal or abnormal (compressed or absent); (d) the presence and type of associated mass lesions: epidural hematoma (EDH) and acute subdural hematoma (ASH); and (e) midline shifts (MLS) (shifts ≤5 mm vs. shifts >5 mm).
We defined TICHs as traumatic intraparenchymal hemorrhagic lesions with a solid and well-defined appearance (hematoma) and fewer well-defined areas of mixed attenuation. 29 Petechial lesions with a classic pattern of diffuse axonal injury (DAI) were excluded. According to the morphology of the TICH, we recognized three patterns: solid, coalescent lesions, and salt and pepper appearance 30 (Fig. 2).
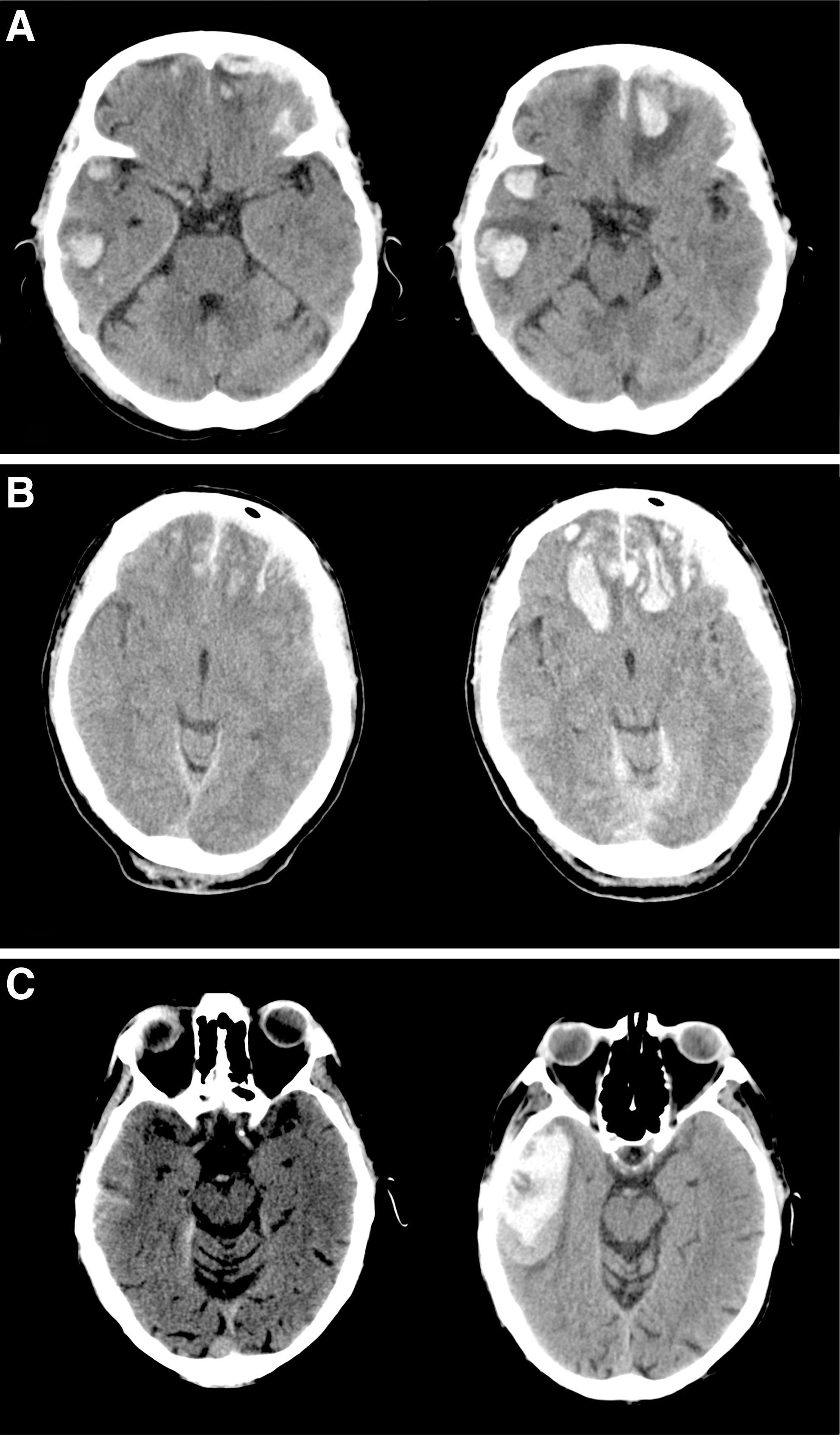
Traumatic intracerebral hemorrhage patterns and progression on the control CT. (
TICHs were categorized based on their initial volume measured in cubic centimeters (cc) into the following groups: 1–5 cc, 6–10 cc, 11–15 cc, 16–20 cc, 21–25 cc, 26–30 cc, 31–35 cc, and ≥36 cc.
TICHs were classified according to their location and number as single, focal, multiple unilateral, or multiple bilateral.
All CT scans were assessed by two senior neurosurgeons (PAG, AL). The Picture Archiving and Communications System (PACS) installed in our hospital was used to acquire CT images. The images were stored in the Digital Imaging and Communication in Medicine (DICOM) format and analyzed on a personal computer.
The TICH volume was calculated in an individual manner using volumetric CT-based software (Analyze 10.0 – Biomedical Imaging Resource (BIR) - Mayo Clinic – Overland Park, KS). Following the region of interest (ROI) method, regions of hemorrhage (hyperdensity) on CT scans were delineated in each slice using an established threshold of density: window width (W) = 100 and window level (L) = 50. Hypodensity areas, such as surrounding edema or nonhemorrhagic contusions, were not included.
The Analyze system uses semiautomatic segmentation tools, such as region growing, edge tracing, and connected thresholding tools, as well as a manual pixel selection tool, all of which were used to segment data in this study. The semiautomated method consists of selecting a pixel inside the volume to be segmented, which is called a seed. The software then automatically connects the neighboring pixels of the initial seed that have a similar intensity. The observer chooses the intensity threshold to be selected to obtain the entire region to be segmented in each slice. Therefore, from the initial point or seed, a region of similar intensity is developed that is chosen by the observer in a semiautomatic region-growing algorithm.
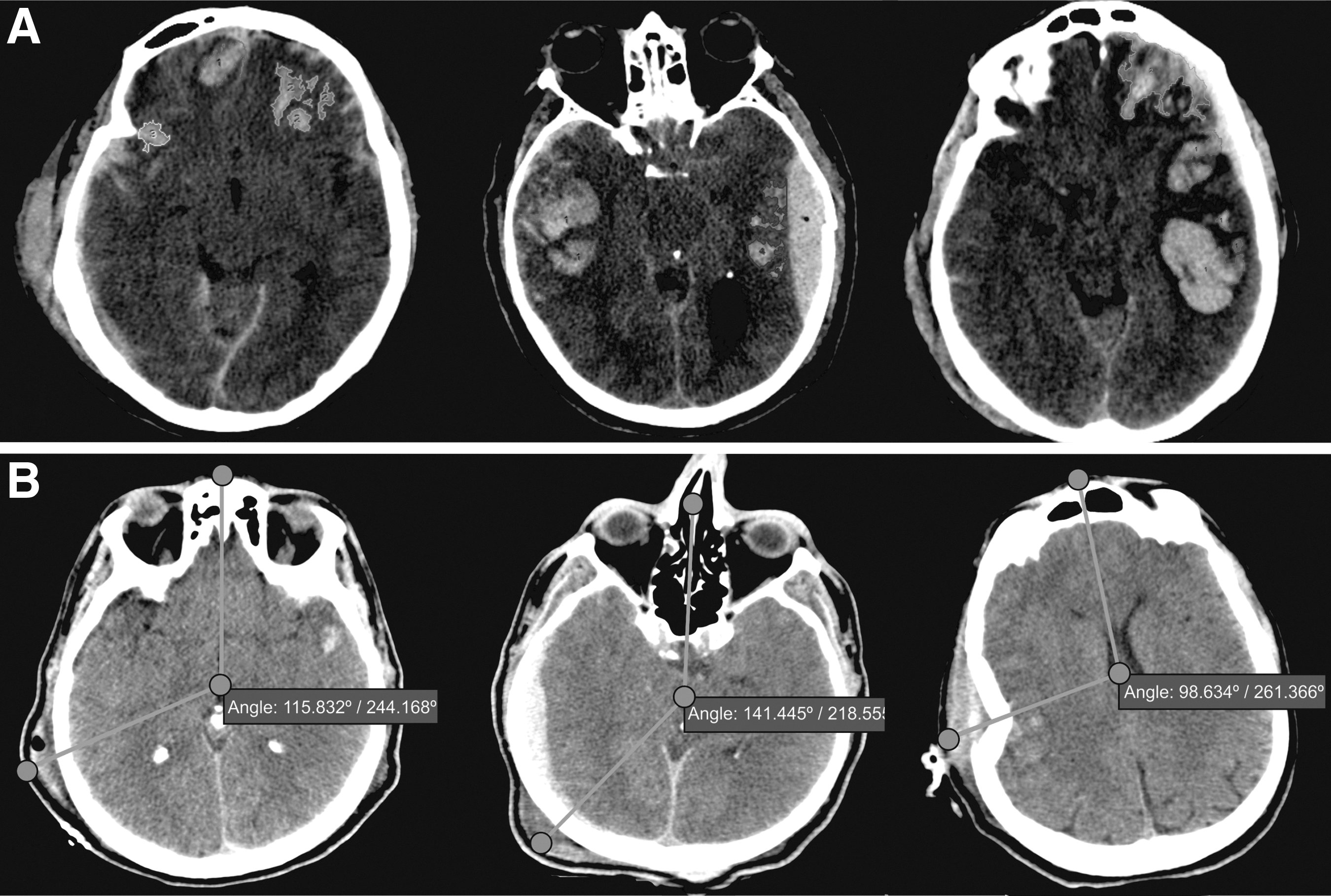
As an adjunct to this semiautomatic method, the ROI in each slice can be modified by edge-tracing or limit-tracing tools to better adjust the ROI to the actual area to be segmented. The different hemorrhagic areas are automatically added up slice by slice by the computer to obtain a final individual volume for each TICH (Fig. 3A).
We used OsiriX image processing software (OsiriX 6.5, Pixmeo, Switzerland) to identify the impact site. The impact site was defined as the area with maximum scalp swelling that could be visualized in circumscribed morphology (cephalohematoma) in the majority of patients. In patients with extensive scalp swelling, rewindowing adjustments were made to determine the presence of blood in the subcutaneous tissue; multiplanar and tridimensional reconstructions were also applied to identify the most affected area (Fig. 4). Other signs of head injury were used, including surgical staples, fracture lines, and skin disruptions.
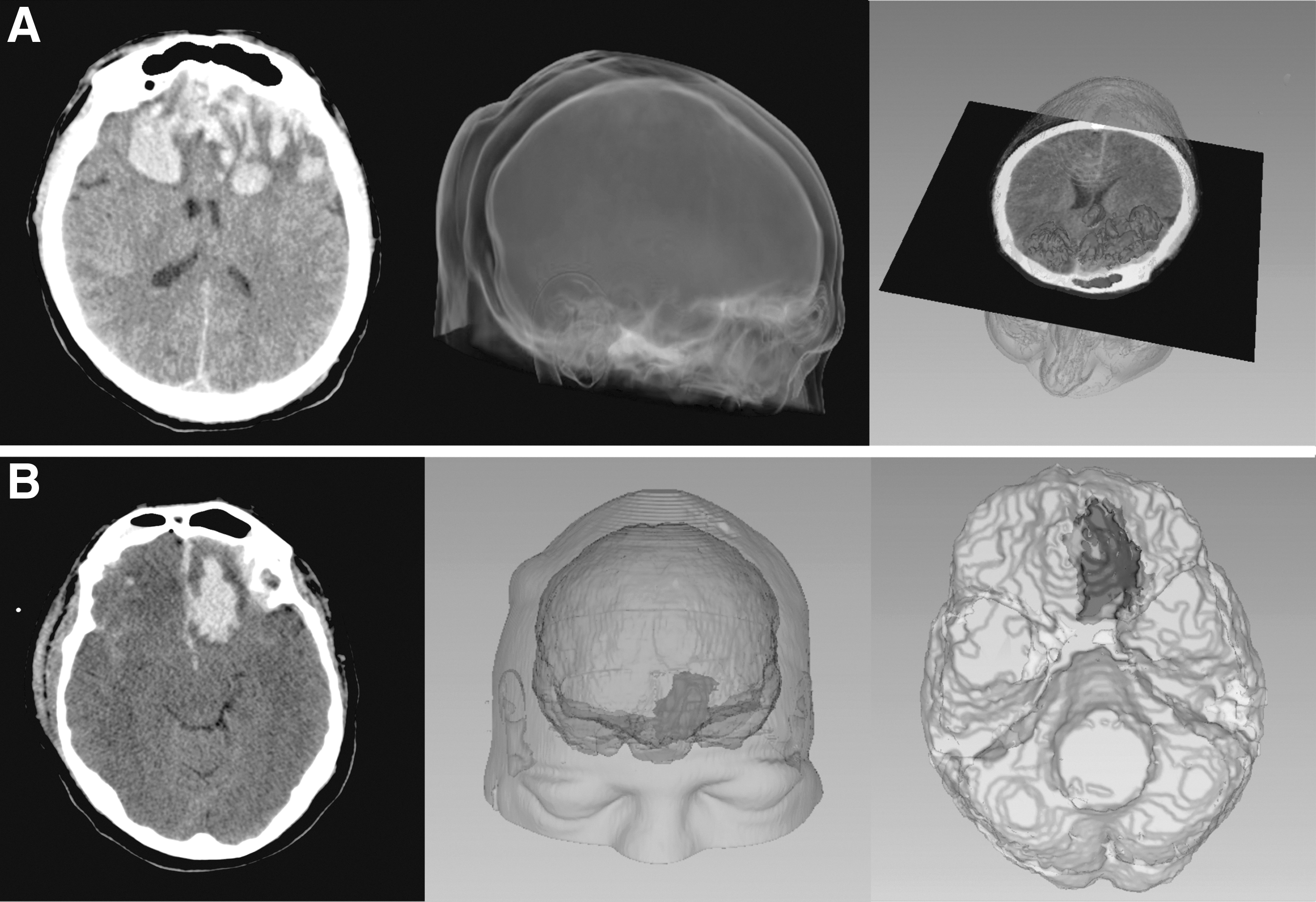
Samples of three-dimensional and volumetric reconstructions. (
For the geometric estimation, we applied the system used in previous publications. 18,19 Using the angle measure tool of OsiriX, the angles between the nasion and the impact site and TICH location were recorded in degrees.
One point of the angle is located in the intersection of the inner table of the skull and the sagittal midline above or at the level of the nasion. The vertex of the angle was the midpoint between the inner table of the skull along the sagittal midline. The third point of the angle is located in the impact site (area of maximum scalp swelling) or in the center of TICH. In cases of large hematomas, the center of TICH was located in the intersection of two perpendicular lines following the maximum diameters of TICH. The angles were registered in a clockwise manner from the nasion without modification of the CT reverse (left/right) image orientation (Fig. 3B) (Video 1; see online supplementary material at
The TICH location was classified into anatomical (lobar) and geometric groups.
According to the anatomic location, the TICHs were divided into: (a) frontal, (b) temporal, (c) parietal, (d) occipital, and (e) cerebellar locations.
Following their geometric distribution, the TICHs were grouped into: (a) anterior or frontal: 0–60 degrees and 301–360 degrees, (b) lateral or temporal: 61–135 degrees or 226–300 degrees, and (c) posterior: 136–225 degrees.
Treatment variables
Patients were classified as operated and nonoperated. Surgical procedures were classified as follows: (1) craniotomy: evacuation of the lesion or lobectomy and debridement with bone flap replacement; (2) decompressive craniectomy: removal of the bone flap without evacuation of the TICH; and (c) others: elevation of bone fragments and cerebrospinal fluid drainage, among other procedures.
Primary end point
The groups based on the values registered in degrees were used in the analysis of the association between the impact site and TICH location.
Definition of contrecoup
The contrecoup variable was defined as the TICH located at more than 90 degrees from the impact site. Because we measured the angles in a clockwise manner from the nasion, the coup TICHs were those located 0–90 degrees and 271–360 degrees from the impact site, whereas the contrecoup TICH were those located 91–270 degrees from the impact site.
Secondary objective
The variable used as a secondary objective was the presence or absence of hemorrhagic progression. We defined progression as an increase equal to or greater than 33% of the initial volume of the TICH or the appearance of a new lesion on a control CT scan. 31 We also estimated the absolute change of volume in cc from the initial to the control CT scan.
Outcome variable
According to the Glasgow Outcome Scale (GOS), 32 we classified patients as favorable (GOS score 4–5) and unfavorable (GOS score 1–3) and used this classification as a dichotomous variable. Patients had a minimum follow-up of 6 months.
Statistical analysis
We used the chi-square test for dichotomous variables to study the association between the impact site and TICH location. This test was also used to analyze the association between the TICH location and contrecoup variable.
A univariate analysis was performed to identify the factors associated with TICH-HP. Univariate comparisons were performed using the Student t test for continuous variables, the chi-square test for dichotomous variables, and the analysis of variance test for multicategorical variables.
Logistic regression analysis was used to estimate the association between the risk factors (i.e., clinical findings, laboratory findings, and neuroimaging characteristics) and the main outcome variable (hemorrhagic progression). The initial examination included a set of seven potential predictors that were collected at the time of admission; these predictors are consistently referenced in the literature including a previous publication by our group. 3,5,7,8,22,33,34
The relationship between a predictor and progression was estimated using a crude odds ratio (OR) 35 and R2 of Nagelkerke. 36 A p ≤ 0.05 was considered statistically significant.
In addition, we assessed the interobserver agreement of the method applied to determine the impact site. For that purpose, 50 cases were randomly selected; two observers (PAG, AL) independently determined the impact site in each case following the technique previously described. We classified the impact site according to three systems: (a) 25 groups (1–15; 16–30; 31–45; 46–60; 61–75; 76–90; 91–105; 106–120; 121–135; 136–150; 151–165; 166–180; 181–195; 196–210; 211–225; 226–240; 241–255; 256–270; 271–285; 286–300; 301–315; 316–330; 331–345; 346–360 degrees and undetermined); (b) 5 groups (301–60; 61–135; 136–225; 226–300 degrees and undetermined); and (c) quantitative angle measurement. Weighted kappa coefficients were calculated to assess the interobserver reliability of the method applied to determine the impact site. Intraclass correlation coefficients (ICCs) were calculated to assess the interrater reliability of angle measurements.
Statistical analyses were performed with SPSS 22.0 software (IBM, Chicago, IL) and Epidat 3.0 (Xunta de Galicia, Spain) for the interobserver agreement.
Results
Patient characteristics
The epidemiological and clinical characteristics are shown in Table 2. Of the 343 TICH patients, 292 (85.1%) were male and 51 (14.9%) were female. The mean age was 48.6 years, ranging from 15 to 87 years.
GCS, Glasgow Coma Scale; CT, computed tomography; INR, international normalized ratio; MLS, midline shifts; EDH, epidural hematoma; ASH, acute subdural hematoma; IVH, intraventricular hemorrhage; tSAH, traumatic subarachnoid hemorrhage; TICH, traumatic intracerebral hemorrhage; GOS, Glasgow Outcome Scale.
The mean time between trauma and admission was 1.63 h; the mean time was 1.5 h in the group that demonstrated progression and 1.75 h in the group that did not exhibit progression. These values were not significantly different between groups.
The main mechanism of trauma was fall (182 [53.1%] patients), followed by traffic accident (126 [36.7%] patients), and impact and other mechanisms (35 [10.2%] patients). According to the GCS score at admission, the cases were described as moderate in 87 (27.5%) patients and severe in 229 (72.5%) patients.
The mean time between the trauma and first CT scan was 2.23 h, and the mean time between the trauma and control CT scan was 16.74 h. The mean time between the trauma and first CT was 2.27 h in the group that demonstrated progression and 2.09 h in the group that did not exhibit progression. These values were not significantly different between groups.
The motor scores at admission were distributed as follows: low 28 (8.2%), mid: 12 (3.5%), and high 113 (33%). The motor score was not reliable in 189 (55.3%) cases, mainly because of the effects of sedation.
Table 2 illustrates the radiologic features of the initial CT scans. According to the Marshall classification, 5 (1.5%) cases corresponded to type II, 224 (65.3%) cases corresponded to type III, 16 (5%) corresponded to type IV, and 97 (28.3%) cases corresponded to types V–VI.
We observed the presence of tSAH in 324 (94.5%) cases, IVH in 147 (42.9%) patients, and skull fracture in 221 (64.4%) patients.
A MLS greater than 5 mm was present in 48 (14%) cases. Compressed or absent cisterns were visualized in 91 (26.5%) cases.
We also observed the presence of EDH in 103 (30%) and ASH in 246 (71.7%) cases. With respect to the number and location of TICHs, 280 (81.6%) cases showed multiple TICHs.
The mean volumes of the TICH on the initial and control CT scans were 1.9 and 6.23 cc, respectively. In classifying the initial TICH volume into groups, 309 (90%) cases presented a volume of less than 5 cc; 19 (5.5%) cases presented a volume of 6–10 cc; 8 (2.3) cases presented a volume of 11–15 cc; 4 (1.2%) cases presented a volume of 16–20 cc; and 3 (0.9%) patients presented a volume of more than 20 cc.
Hemorrhagic progression was observed in 226/343 (65.9%) cases. The mean increase in volume was 4.5 cc. In 154 (68.1%) cases, there was an increase of less than 5 cc; an increase of 6–10 cc occurred in 32 (14.2%) cases; 11–15 cc in 16 (7.1%) cases; 16–20 cc in 4 (1.8%) cases; 21–25 cc in 8 (3.5%) cases; 26–30 cc in 2 (0.9%) cases, and >30 cc in 10 (4.4%) cases.
The outcome at the 6-month follow-up was favorable in 162 (48.2%) cases and unfavorable in 174 (51.8%) cases. The mortality rate at 6 months was 25.2% (88 cases). We found a significant association between progression and an unfavorable outcome. The outcome was unfavorable in 140 (80.5%) cases in the group that demonstrated progression and in 34 (19.5%) cases in the group that did not exhibit progression (OR 2.62, p < 0.001). The absolute change in volume of TICH showed a significant association with outcome; patients with favorable outcomes had a mean growth of TICH of 3.21 cc, whereas the group of patients with unfavorable outcomes showed a mean growth of 5.97 cc. This relationship was statistically significant (p < 0.02).
Relationship between the impact site and TICH location
In 19/369 (5.15%) cases, the impact site could not be determined because of a lack of radiological signs of head trauma, extensive areas of scalp swelling, evidence of more than one impact site (rebound injury), or impact located on the cranial vertex. The TICH locations, impact sites, and their associations are summarized in Table 3.
TICH, traumatic intracerebral hemorrhage; OR, odds ratio.
An interobserver agreement assessment of the method used to determine the impact site was performed. For the angular measurements, the ICC was 0.6, IC 95% (0.32–0.78), p < 0.001. For the classification system of the impact site into 25 groups, the weighted kappa was 0.68, IC 95% (0.21–1), p = 0.002, and the ICC was 0.74, IC 95% (0.53–0.86), p < 0.001. For the classification system of the impact site into five groups, the weighted kappa was 0.97, IC 95% (0.93–1), p < 0.001. The classification of the impact site into five groups (including the undetermined category) was used for the statistical analysis.
As noted above, TICH location was registered according to two classification systems: anatomical and geometric groups.
The association between these classification systems was analyzed. Frontal TICHs were associated with the anterior location group (0–60 degrees; 301–360 degrees), temporal TICHs were associated with the lateral location group (61–135 degrees; 226–300 degrees) and parietal, occipital, and cerebellar TICHs were associated with the posterior location group (136–225 degrees). Every TICH classified geometrically corresponded with the anatomical location in all cases. Thus, the geometric classification system appears able to perfectly characterize the anatomical or lobar location of TICH.
The associations between the two systems of classification were statistically significant at p < 0.001. Based on these results, we decided to apply the geometrical classification system for both analyses: the association of the impact site and TICH location and the assessment of hemorrhagic progression.
TICH location had the following distribution: (a) anterior or frontal: 172 (49.1%) of cases; (b) lateral or temporal: 156 (44.6%), and (c) posterior: 22 (6.3%).
The location of the impact sites had the following distribution: (a) anterior or frontal: 148 (42.3%) of cases; (b) lateral or temporal: 46 (13.1%), and (c) posterior: 156 (44.6%) (Fig. 5).
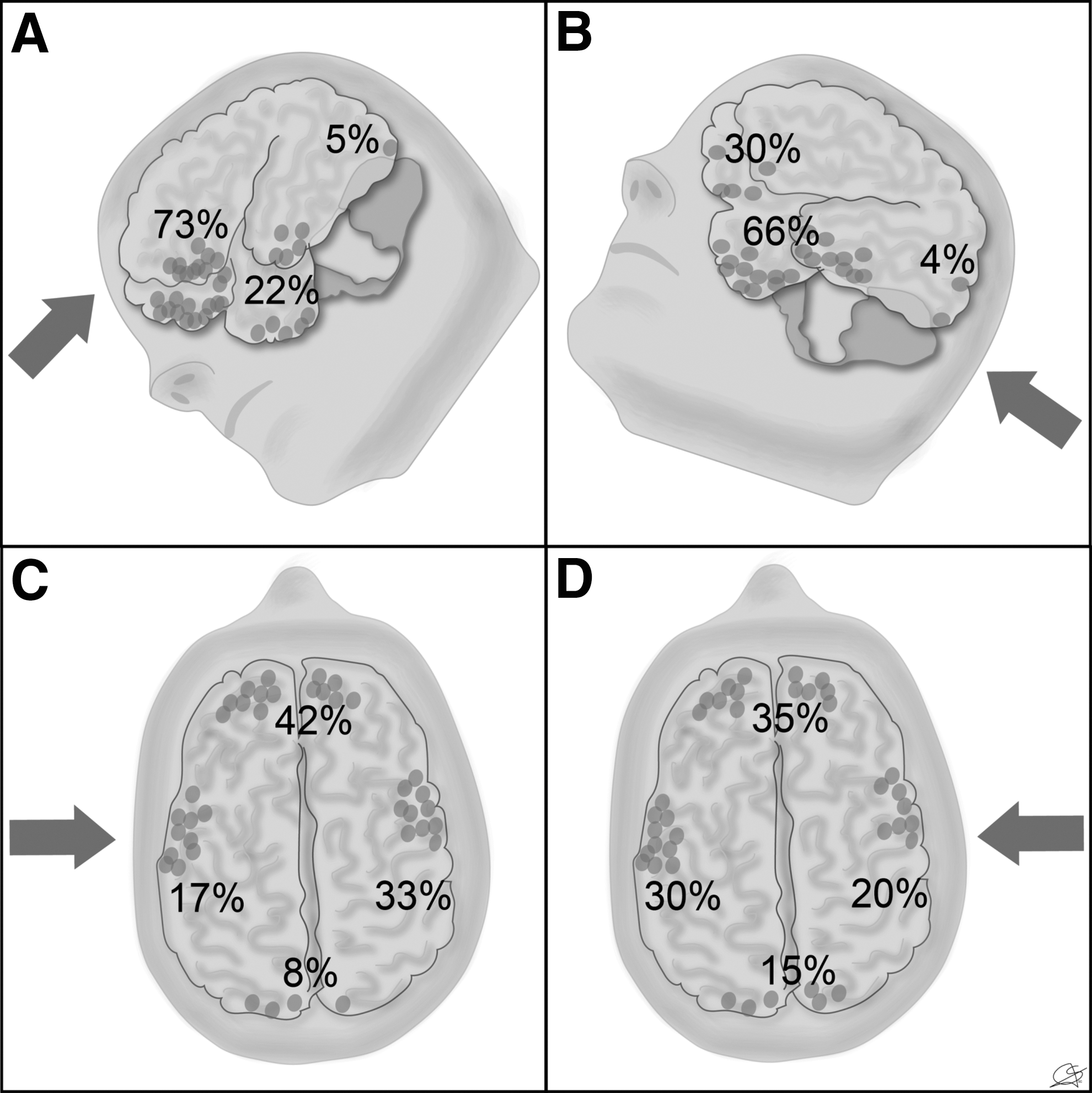
Schematic representation of the distribution of traumatic intracerebral hemorrhage (dots) according to the impact site (arrow). (
We found a statistically significant association between frontal TICHs and impact sites located on the anterior area of the head (OR 5.8, p < 0.001). The temporal TICH location was significantly associated with impact sites located in the posterior area of the head (OR 4.9, p < 0.001).
The analysis of the association between the location of TICHs and the coup/contrecoup variable is summarized in Table 4. According to our results, anterior TICHs were associated with impact sites located at less than 90 degrees (coup) (OR 1.64, p = 0.03). Posterior TICHs showed a strong association with impact sites located at less than 90 degrees (coup), but this association was not statistically significant (p = 0.08). Lateral TICHs were associated with impact sites located at more than 90 degrees (contrecoup) (OR 1.98, p = 0.003).
TICH, traumatic intracerebral hemorrhage; OR, odds ratio.
Relationship between the geometrical variables and other risk factors associated with hemorrhagic progression
Table 2 shows the results of the univariate analysis of the association between hemorrhagic progression and clinical, radiologic, and geometric variables.
We did not find any statistically significant association between the TICH location or impact site and hemorrhagic progression. A subgroup analysis of the contrecoup TICHs was performed, however; contrecoup lateral TICHs were more likely to show hemorrhagic progression compared with frontal and posterior locations of the contrecoup subgroup (OR 2.08, p = 0.037).
Of all variables analyzed, those that showed a statistically significant association with TICH-HP included falls as the mechanism of trauma (OR 2.25, p < 0.001), cisternal compression (OR 2.13, p = 0.01), MLS >5 mm (OR 2.26, p = 0.04), ASH (OR 2.32, p = 0.001), multiple TICHs (OR 2.31, p = 0.003), an initial volume of <1 cc (OR 1.63, p = 0.04) and decompressive craniectomy (OR 3.69, p = 0.002).
Contrecoup TICHs were significantly associated with an increased risk of progression (OR 1.92, p = 0.02).
We also performed a univariate analysis to determine the association between the variables collected and the absolute increase in TICH volume measured in cc. These results are summarized in Table 5.
GCS, Glasgow Coma Scale; CT, computed tomography; MLS, midline shifts; EDH, epidural hematoma; ASH, acute subdural hematoma; IVH, intraventricular hemorrhage; tSAH, traumatic subarachnoid hemorrhage; TICH, traumatic intracerebral hemorrhage; GOS, Glasgow Outcome Scale.
Variables that showed a statistically significant association with an increase in volume included: female (OR 1.02, p = 0.031), low motor score at admission (OR 1.02, p = 0.015), Marshall classification of the first CT scan (OR 1.2, p = 0.03), cisternal compression (OR 1.04 p < 0.001), MLS >5 mm (OR 1.03, p < 0.001), swelling (OR 1.05, p < 0.001), ASH (OR 1.09, p = 0.005), a salt and pepper TICH pattern (OR 1.05, p < 0.001), lateral TICHs (OR 1.03, p = 0.03), and decompressive craniectomy (OR 1.04, p < 0.01).
The variables that showed a statistically significant association with hemorrhagic progression were used in the multivariate analysis (Table 6). Factors independently associated with TICH-HP obtained through the logistic regression included an initial volume of <1 cc, cisternal compression, falls, ASH, multiple TICHs, and contrecoup TICHs.
CI, confidence interval; OR, odds ratio, ASH, acute subdural hematoma; TICH, traumatic intracerebral hemorrhage.
Discussion
The results of our study demonstrate an association between the TICH location and impact site. Further, the contrecoup mechanism represents a risk factor independently associated with TICH-HP.
One of the strengths of our study is that we had a sufficiently large sample. Another positive aspect of our work was performing the analysis based on individual TICHs rather than individual patients, which enabled us to study the evolution of each TICH in cases presenting as multiple lesions in the same patient.
Another remarkable aspect of our study was the application of geometric variables to enable us to collect data in a systematic manner.
Since the beginning of the “CT era,” there have been few publications that aimed to determine the association between the impact site and TICH location. The first methodological challenge that faces this type of study is the data collection technique. Based on the studies published by Besenski and associates 18 and subsequently by Ratnaike and colleagues, 19 we used the measurements in angles relative to the nasion, and thus we were able to classify the impact sites and TICHs.
The main limitations of these previous studies include the lack of a sufficiently large sample and performing the analysis based on the number of patients instead of individual TICHs, which can lead to mistakes in analyzing the evolution of patients with multiple TICHs. In addition, the definition of contrecoup was not clear in previous works. Finally, none of the previously mentioned authors performed a statistical analysis between the impact site and TICH location.
Determination of the impact site exclusively using CT images might seem complex; however, in our study, we were able to determine the impact site with confidence in 95% of the cases; in previous publications, this proportion varied from 80% 18 to 90% 19 of cases. Further, we demonstrated that our method has good interobserver agreement.
The TICH distribution in our series was predominantly in the frontal (50.4%) and temporal (44%) lobes, followed by parietal (2.6%), occipital (2%), and cerebellum (0.9%). This finding correlates with previous works and is similar to post-mortem and CT image-based series. 5,9,18,19,37 –40
The primary objective of our study was to determine the association between the TICH location and impact site. According to a previous study by Jamieson and Yelland, 41 frontal TICHs are typically produced by occipital blows (46%) and rarely by frontal blows. Temporal TICHs are produced by lateral impacts (61%) and are ipsilateral in 58% of cases. Courville 42 confirmed that frontal blows produce frontal TICHs but not occipital TICHs. Schneider and coworkers 43 observed the appearance of temporal TICHs associated with impacts on the posterior area of the head.
According to our results, frontal TICHs are significantly associated with impacts located on the anterior region of the head (62.8%). Temporal TICHs were associated with posterior impacts (65.2%). Posterior TICHs did not have a significant association with any region of impact.
The term “contrecoup” has been used to describe a specific type of traumatic intracranial lesion. The first application of the term was likely made by Hippocrates, when he described a skull fracture that appeared on the opposite site of the impact. 44
The first studies were based on direct observation of post-mortem series and later with the development of imaging techniques, such as CT scans. Several authors have described various types of traumatic lesions secondary to contrecoup, including epidural hematomas, ASHs, intracerebral hematomas, and skull fractures. 45 –50
The first publications about the location and mechanism of production of TICH were by Lindenberg and Freytag 16,37 and Gurdjian and colleagues 51 and Gurdjian. 52 Since then, several authors have focused on determining the frequency of the appearance and distribution of TICH and on formulating a hypothesis regarding the mechanism of production of this type of traumatic lesion. 14,17,39,42,53 –58 Nonetheless, a serious limitation of previous works is their descriptive nature; an important bias occurs because they are based on autopsies and thus include only the most severe cases.
One of the main considerations when planning the current study was to define the contrecoup in a clear and precise manner. In this regard, there is an ambiguity of criteria in the literature. Since the publications of Lindenberg and Freytag, 16 it has been postulated that coup TICHs are produced under the area of impact, whereas contrecoup TICHs are produced by impacts located on the opposite site or lobe respective to the lesion; other authors have confirmed this definition. 42,55,59 Gurdjian and coworkers 51 defined contrecoup TICH as lesions located in the region diametrically opposed to the impact site; however, Gurdjian 38 defined contrecoup TICH as lesions located in an area other than the region of impact. The contrecoup term is applied in numerous publications; however, most of the authors did not provide a clear definition of this mechanism.
It might seem easy to classify a TICH as coup or contrecoup in current practice; however, to perform an individualized analysis of this type of traumatic lesion, it is essential to determine a rigorous and measurable definition of contrecoup. This definition must be able to eliminate any subjective influence. In a recent publication, coup TICHs are defined as lesions located between 271–90 degrees from the impact site, whereas contrecoup TICHs are defined as lesions located between 151–210 degrees from the impact site. 19 Nevertheless, the author did not consider the regions located at 91–150 degrees and 21–270 degrees.
Despite the singular geometry of the cranial vault, to create a simple system of reference, we assumed that the skull was a sphere that is projected on every axial CT slice. In this manner, the antipodes correspond to the points of the sphere that are diametrically opposed. We considered that the definition of coup and contrecoup should not be strict with geometric measures and criteria because both TICH and impact sites can extend beyond a point in the sphere. Cerebral lobes correspond to wide regions instead of points. Thus, we decided to define contrecoup TICHs as the lesions produced by impact sites located more than 90 degrees from the lesion.
In our study, the frequency of contrecoup TICH reaches 32.9% (115/350) of the cases. Besenski and colleagues 18 analyzed a series of 45 patients and found that 13% of patients had exclusively contrecoup TICH, 20% had coup TICH, and 67% had both types of TICH. The author added categories as “predominantly” coup or contrecoup; however, a clear definition of these categories was not established.
In another publication, the frequency of contrecoup TICH was estimated at 77%; nevertheless, in cases of multiple TICH, the author used the TICH of greater volume for the analysis. The difference in the frequency of contrecoup TICH between our series and other publications is because of the methodology that we used.
According to our results, frontal TICHs tend to be produced more frequently by coup in 72.7% of the cases, and temporal TICHs were produced by contrecoup in 41.1% of the cases. These associations were statistically significant. There are several references in the literature regarding the association of the impact site and TICH location. Ommaya and associates 55 noted that frontal impacts generally produce lesions by coup, whereas the temporal and occipital impacts can produce either coup or contrecoup TICHs with similar probability. In another publication, 56 occipital impacts produced contrecoup TICH in 90% of cases, and frontal impacts produced coup lesions in 93% of cases.
Several hypotheses have been proposed regarding the mechanism of TICH production. Drew and Drew 60 summarized these hypotheses as follows: (a) positive pressure theory or contact, (b) negative pressure theory or cavitation, (c) rotational shear stress theory, and (d) angular acceleration theory. These theories were drafted by Rowbotham 61 in the 15th century. Some authors postulate that positive theory could explain the coup lesions and cavitation theory could explain contrecoup TICHs. 13,14,16 A plausible explanation for contrecoup TICH, however, could be a mixture of rotational shear stress and angular acceleration combined with the irregular surface of the region where the majority of the contrecoup TICH appears, the middle cranial fossa. 17,52,55,62
Our study did not aim to analyze the biomechanics of TICH production; our goal was to find a geometric relationship between the impact sites and the location of this type of intracerebral lesion. For a comprehensive study of the complex mechanisms of trauma, it would be necessary to use experimental models 63 –66 or apply new technologies, such as finite element analysis. 67 –71
As a secondary objective, we established an association between contrecoup TICHs and hemorrhagic progression. To our knowledge, this is the first study in the literature that focused on this association. The only previous reference to this issue is provided by Adams and coworkers, 39 who did not study hemorrhagic progression but rather used a severity index based on the location and extension of TICH. He found that frontal and temporal TICH were the most severe; however, a second study by Adams and colleagues 54 could not demonstrate that contrecoup TICH had a greater severity index.
In our series, we observed a TICH-HP frequency of 65.9%. In a previous publication by our group, we obtained a progression frequency of 63%. 3 Other authors describe growth frequencies between 16.4% and 65%. 4,5,7,9,10,33,72
We also studied the association between other risk factors and progression. In our study, age tended to be associated with TICH-HP but did not reach statistical significance. In other publications, age represented a risk factor for progression. 3,72
With respect to the mechanism of trauma, falls, the main mechanism of trauma, were associated with TICH-HP. This finding is correlated with the change in the demographic profile of TBI. 25
We did not find an association between hemorrhagic progression and either the GCS score for pre-hospital care or the GCS score at the time of admission. We also analyzed eye, motor, and verbal scores and did not obtain significant results. Our results are similar to those of other publications. 3,4 The results of our study may be explained by circumstances such as unreliable GCS scores recorded during pre-hospital care and the interference of sedation with the neurological assessment of the patient at admission. Nevertheless, regarding the change in TICH volume, patients with low motor scores at admission showed greater increases in TICH volume on the control CT.
According to previous studies, abnormalities in coagulation parameters and the platelet count have been described in patients with expanding traumatic intracranial lesions. 4,72 –76 Nevertheless, similar to our previous work, 3 we were unable to identify a statistical association between the laboratory variables analyzed and hemorrhagic progression.
One topic of discussion regarding our study has been the mean initial volume of TICH. In this study, the mean initial volume of TICH was 1.9 cc. Further, 90% of the TICH analyzed had an initial volume less than 5 cc. We found similar proportions in previous publications, in which a TICH volume less than 3 cc represented between 77% and 85% of the samples. 5,7,10 Conversely, other publications describe larger initial TICH volumes than our series. 3,8,9,33 A possible explanation for this variation could be that our study was based on individual TICH volume, whereas in previous publications, the initial volume corresponded to the total volume of intraparenchymal bleeding for each patient. Moreover, we measured only the hemorrhagic component (hyperdensity) of each TICH, as described above.
TICHs with an initial volume of <1 cc were more likely to undergo progression. In a previous publication, 3 we proposed a hypothetical explanation for this result: small lesions have more space inside the cranial cavity for expansion, whereas large TICHs must overcome the higher pressures of surrounding structures to increase in volume.
Another factor that we found to be significantly associated with progression was the presence of multiple TICHs in either the same or contralateral hemisphere. One possible explanation for this result could be the coalescence of several small lesions that together generate a greater volume in the control CT. 3
Regarding the TICH location, we found a significant association in the univariate analysis between contrecoup temporal TICHs and progression; moreover, temporal TICH showed a greater increase in volume than TICH in other locations. The intricate anatomy of the middle cranial fossa could be involved in the production of TICH with a tendency to reach greater volumes.
The TICH pattern on CT scans is another interesting aspect of our results. The salt and pepper pattern proposed by Fukamachi and associates 30 showed a greater increase in volume than the solid or coalescent patterns. The significance of this finding could be difficult to explain and also controversial because this pattern could represent a technical difficulty at the time that the volume was calculated.
The presence of decompressive craniectomy was significantly associated with progression and with a greater increase of volume; however, this association was not confirmed in the multivariate analysis. Some authors describe decompressive craniectomy as a risk factor of TICH-HP. 3,77 In another publication, however, this association could not be demonstrated. 78
The effect of decompressive craniectomy should be further analyzed considering the interactions with other variables, such as cisternal compression, ASH, and initial TICH volume.
We are aware of the limitations of this study. These limitations include patient and treatment selection biases because of its retrospective nature. Another limitation is that we included patients with moderate and severe TBI; it is essential to encompass the entire TBI patient spectrum to comprehensively analyze and better characterize the relationship between the initial neurological status of the patient and the appearance of TICHs and their probability of progression.
Another potential limitation was the precision of the method that we applied to determine the impact site based on CT images. The appropriate manner to determine the impact site is the direct identification of external signs of head trauma on physical examination.
Another possible limitation was that we excluded cases in which the impact site could not be determined; however, this was a small proportion of cases (5.15%).
The geometric association between the impact site and TICH location has been observed for more than 50 years; however, the association of these variables with hemorrhagic progression has not been studied. We acknowledge the limitations of our study; to obtain better results, further studies should be designed in a prospective manner, include more patients and mild TBI, determine the impact site with data from physical examinations, and measure the areas of edema around the TICH.
Conclusions
We demonstrated that there is a significant association between the TICH location and impact site. According to the geometric relationship, frontal TICHs are produced by coup and temporal TICHs are produced by contrecoup. The contrecoup represents a risk factor independently associated with hemorrhagic progression.
Footnotes
Acknowledgments
This study was funded by grant no. 2010-007 from the Mutua Madrileña Foundation (Spain) to Pedro A. Gómez, MD, PhD, and by grant FIS PI14/01457 co-financed by Instituto de Salud Carlos III (ISCIII) and FEDER. Portions of this work were presented in abstract form as proceedings at the XX Congress of the Spanish Society of Neurological Surgery, Pamplona, Spain, May 19, 2015.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.