
Abstract
Early decompression may improve neurological outcome after spinal cord injury (SCI), but is often difficult to achieve because of logistical issues. The aims of this study were to 1) determine the time to decompression in cases of isolated cervical SCI in Australia and New Zealand and 2) determine where substantial delays occur as patients move from the accident scene to surgery. Data were extracted from medical records of patients aged 15–70 years with C3-T1 traumatic SCI between 2010 and 2013. A total of 192 patients were included. The median time from accident scene to decompression was 21 h, with the fastest times associated with closed reduction (6 h). A significant decrease in the time to decompression occurred from 2010 (31 h) to 2013 (19 h, p = 0.008). Patients undergoing direct surgical hospital admission had a significantly lower time to decompression, compared with patients undergoing pre-surgical hospital admission (12 h vs. 26 h, p < 0.0001). Medical stabilization and radiological investigation appeared not to influence the timing of surgery. The time taken to organize the operating theater following surgical hospital admission was a further factor delaying decompression (12.5 h). There was a relationship between the timing of decompression and the proportion of patients demonstrating substantial recovery (2–3 American Spinal Injury Association Impairment Scale grades). In conclusion, the time of cervical spine decompression markedly improved over the study period. Neurological recovery appeared to be promoted by rapid decompression. Direct surgical hospital admission, rapid organization of theater, and where possible, use of closed reduction, are likely to be effective strategies to reduce the time to decompression.
Introduction
A
Pre-clinical data examining early decompression consistently demonstrate improved outcomes, albeit in models not always consistent with the nature and time course of human injury. 5 Clinical studies of cervical SCI suggest that early decompression within 24 h of injury improves neurological function in a small proportion of patients, 6 –10 with decompression not appearing to influence neurological recovery when performed beyond this time. 11 –16 The proportion and magnitude of benefit may increase as the time to surgery shortens, consistent with animal studies. 7,17 Early surgery also appears to reduce complications and shorten hospital length of stay. 6,7,18,19 However, performing early decompression is often challenging because of the time occupied by the complicated process of care from accident scene to surgery. Delays can occur at many stages, including paramedic retrieval and transportation, pre-surgical hospital admission, surgical hospital assessment, medical stabilization, investigation, and operating theater access. To minimize the time to early decompression, it is crucial to understand and determine the duration of each step in the process of care from accident scene through to surgery. This allows substantial delays to be identified and focused solutions can then be developed to reduce these delays.
The aims of this study were to 1) determine the median time to decompression in cases of isolated cervical SCI over a period of 4 years in Australia and New Zealand and 2) determine where substantial delays occur as patients move from the accident scene to surgery.
Methods
Study design and ethical approval
A retrospective analysis of cases with isolated cervical SCI who underwent decompression over a 4-year period (2010 to 2013) was conducted within Australia and New Zealand. The following hospitals were involved in this study: Austin Hospital (Melbourne, Australia), the Alfred Hospital (Melbourne, Australia), Royal Adelaide Hospital (Adelaide, Australia), Royal Perth Hospital (Perth, Australia), Princess Alexandra Hospital (Brisbane, Australia), Royal North Shore Hospital (Sydney, Australia), Prince of Wales Hospital (Sydney, Australia), Middlemore Hospital (Auckland, New Zealand), and Christchurch Hospital (Christchurch, New Zealand). A list of all traumatic cervical SCI admission cases was obtained from each hospital for the defined data collection period. All relevant human research ethics committees were advised of the project and data audit or low-risk human research ethical approvals were obtained where required at each institution.
Inclusion and exclusion criteria
Patients between ages 15 and 70 years with a C3-T1 fracture, fracture-dislocation, and disc and/or ligamentous injury in association with an acute traumatic SCI with neurological deficits were included in the study. Spinal decompression was achieved either by closed or open reduction. Patients were excluded from the study if the time of injury and time of spinal decompression were not available.
Excluded from the study were patients with: multiple traumatic injuries (defined as trauma to at least one other major organ, significant abdominal bleeding or retro-peritoneal hemorrhage likely to require intervention, pelvic fracture likely to require intervention, more than two long bone fractures requiring operative fixation); Injury Severity Score >16; significant head injury (defined as a sustained Glasgow Coma Scale [GCS] score <13 at the scene); and penetrating SCI (not involving decompression surgery). Patients with traumatic central cord syndrome (TCCS) were excluded, as the urgency of treatment for these patients varied across institutions. In addition, patients with pre-existent major neurological deficits or disease (e.g., stroke, Parkinson's disease) were excluded.
Data collection and management
A data dictionary was created to ensure standardized data collection across sites. All data was entered as a de-identifiable format using a Research Electronic Data Capture, a secure (username and password protected) Web-based database hosted by the Florey Institute of Neuroscience and Mental Health. 20
For each included case, the following data fields were collected: demographics (date of birth and gender); injury event (date and time of injury, location of accident, cause of accident, initial GCS); metropolitan, rural, or remote accident location (based on the population size and distance to the nearest urban center); ambulance (date and time paramedic call was received, date and time ambulance arrived at patient, transporting ambulance departure date and time, date and time of arrival at first hospital); hospital admission (date and time left first hospital, date and time of arrival at surgical hospital); date and time of spinal computed tomography (CT) scan; and date and time of spinal magnetic resonance imaging scan (MRI). In addition, data were collected on injury characteristics (level and type of spinal fracture, level of neurological deficit, extent of lesion, and American Spinal Injury Association Impairment Scale (AIS) grade at surgical hospital admission and at rehabilitation discharge and surgical intervention (i.e., type of surgery, date and time of closed reduction, date and time of initiation of decompression surgery defined as the first anesthetic entry of surgery, date and time of completion of decompression surgery defined as the last anesthetic entry of surgery).
Data analysis
On completion of data collection, all data were scrutinized for completeness and accuracy, and then de-identified prior to analysis. The following epochs were calculated for each individual case: time of injury to first ambulance arrival, first ambulance arrival to ambulance departure, ambulance departure to first hospital admission, total paramedic time (time between injury and first hospital admission), pre-surgical hospital time (time between admission at first hospital and admission to the surgical hospital), hospital admission and spinal CT scan, hospital admission and spinal MRI (time of the first spinal CT/MRI was used, regardless of at which hospital radiology was performed), and surgical hospital admission (time between surgical hospital admission and spinal decompression). Time to spinal decompression was defined as the time of injury to the midpoint between initiation and completion of decompressive surgery.
For the purposes of this study, patients were regarded as having undergone closed reduction if the procedure was performed prior to and separate from open cervical spine decompression surgery. 17 If closed reduction was performed and deemed successful, the time of closed reduction was taken to be the time of spinal decompression. Closed reduction was regarded as successful if the treating spinal or neurosurgical team felt that reduction and realignment were adequate on post-reduction MRI or CT imaging. Simple cervical traction was not regarded as attempting urgent closed reduction unless combined with clinical follow-up prior to surgery and post-reduction imaging. Surgical approaches for patients who underwent decompression surgery were divided into anterior decompression and stabilization, posterior decompression and stabilization, or both (anterior and posterior approach). The main data outcomes (total time to decompression and time to decompression by year) were analyzed for each site. As the overall process of care followed the same course at all sites, further data were combined for analysis.
Statistical analysis
Non-parametric data were compared using Mann-Whitney U t-test (two-tailed) and significance was set at p < 0.05. The chi-square test was used to investigate associations between categorical variables, with Fisher's exact test employed where the expected frequencies were <5. Data are presented as median and interquartile range (IQR), unless otherwise stated. Statistical analyses were performed using Prism software (version 6, GraphPad, CA) and Igor Pro 6.0 software (WaveMetrics, Portland, OR).
Results
Demographics
A total of 192 patients met the inclusion criteria and were included in the study. Demographic and injury details are shown in Table 1. The mean age was 36 years ±17 (mean ± standard deviation) and the majority of patients (83%) were male. The majority of SCIs (56%) occurred in a metropolitan area and were commonly a result of high-speed motor vehicle accidents (speed >60 km/h). High falls (>1 m) and water-related accidents (e.g., diving, surfing) also were a common cause of injury. The most frequent neurological level of injury was C5 (30%). A slightly smaller proportion of patients had a C4 (26%) or C6 (22%) neurological level of injury (Fig. 1).
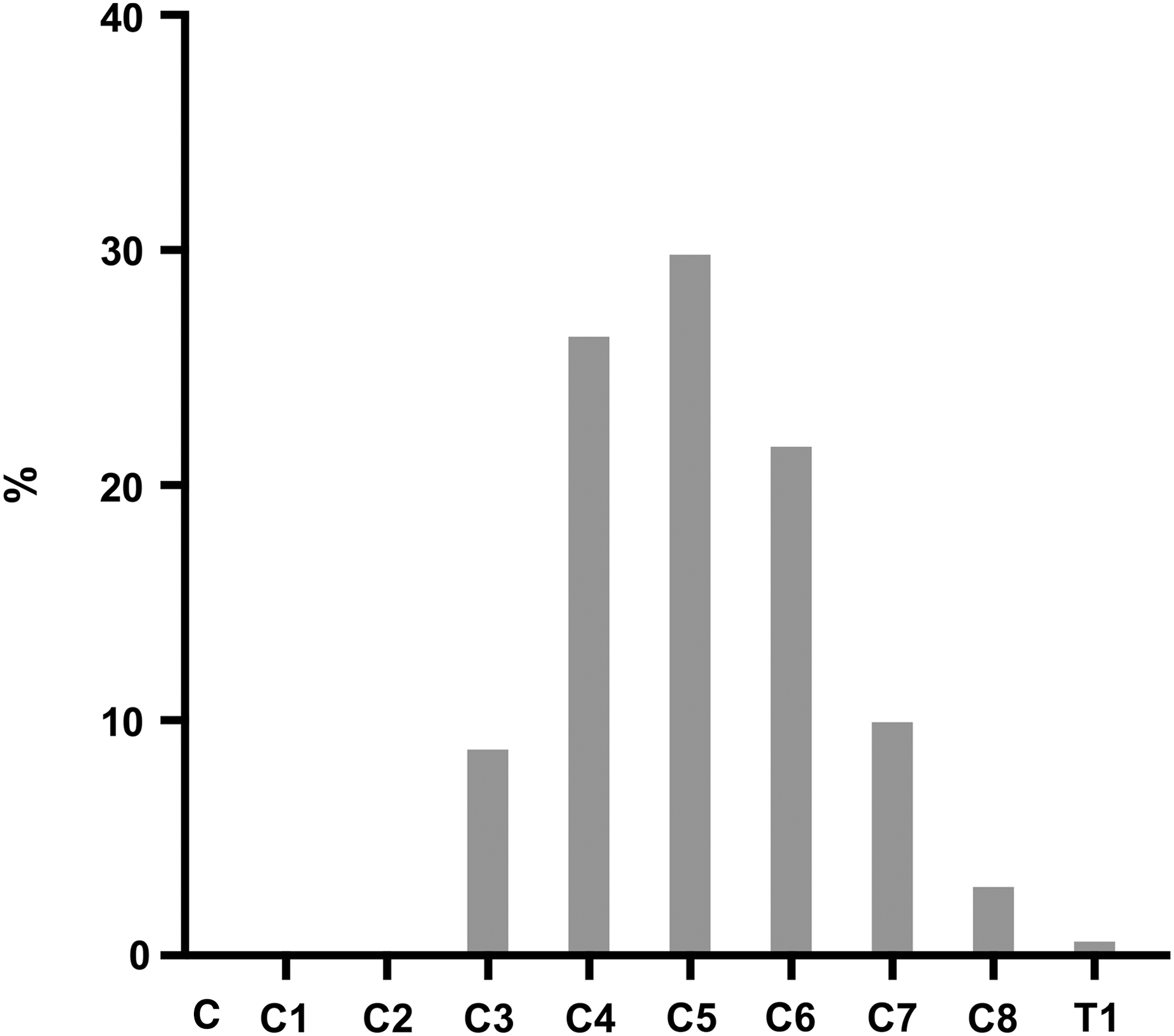
Distribution of level of injury. Histogram showing the proportion of patients included at each neurological level of injury.
SD, standard deviation; AIS, American Spinal Injury Association Impairment Scale.
The majority of patients (76%) who were treated with surgical decompression underwent anterior spinal decompression and stabilization. A posterior approach to decompression and stabilization was employed in 12% of patients, while both approaches were used in a further 12% of cases.
Timing of spinal decompression
The median time between accident and spinal decompression (open or closed) throughout Australia and New Zealand was 21 h (IQR, 12–41; Fig. 2) over the study period. The median time to spinal decompression was similar among sites. The IQR, however, varied between sites and as expected, was larger (because of an increase in the upper range) for sites with a more geographically dispersed population (e.g., Queensland and Western Australia). In Victoria (n = 52), Western Australia (n = 27), and Queensland (n = 56), the time to spinal decompression, respectively, was 21 h (IQR, 11–32), 20 h (IQR, 10–159), and 22 h (IQR, 12–41). South Australia (n = 11) and New South Wales (n = 8) had slightly lower median times to decompression (14 h, IQR, 11–26 and 19 h, IQR, 14–28, respectively). Both sites in New Zealand—Christchurch (n = 26) and Auckland (n = 12)—also had similar median time to decompression (29 h, IQR, 13–49 and 26 h, IQR, 14–70, respectively).
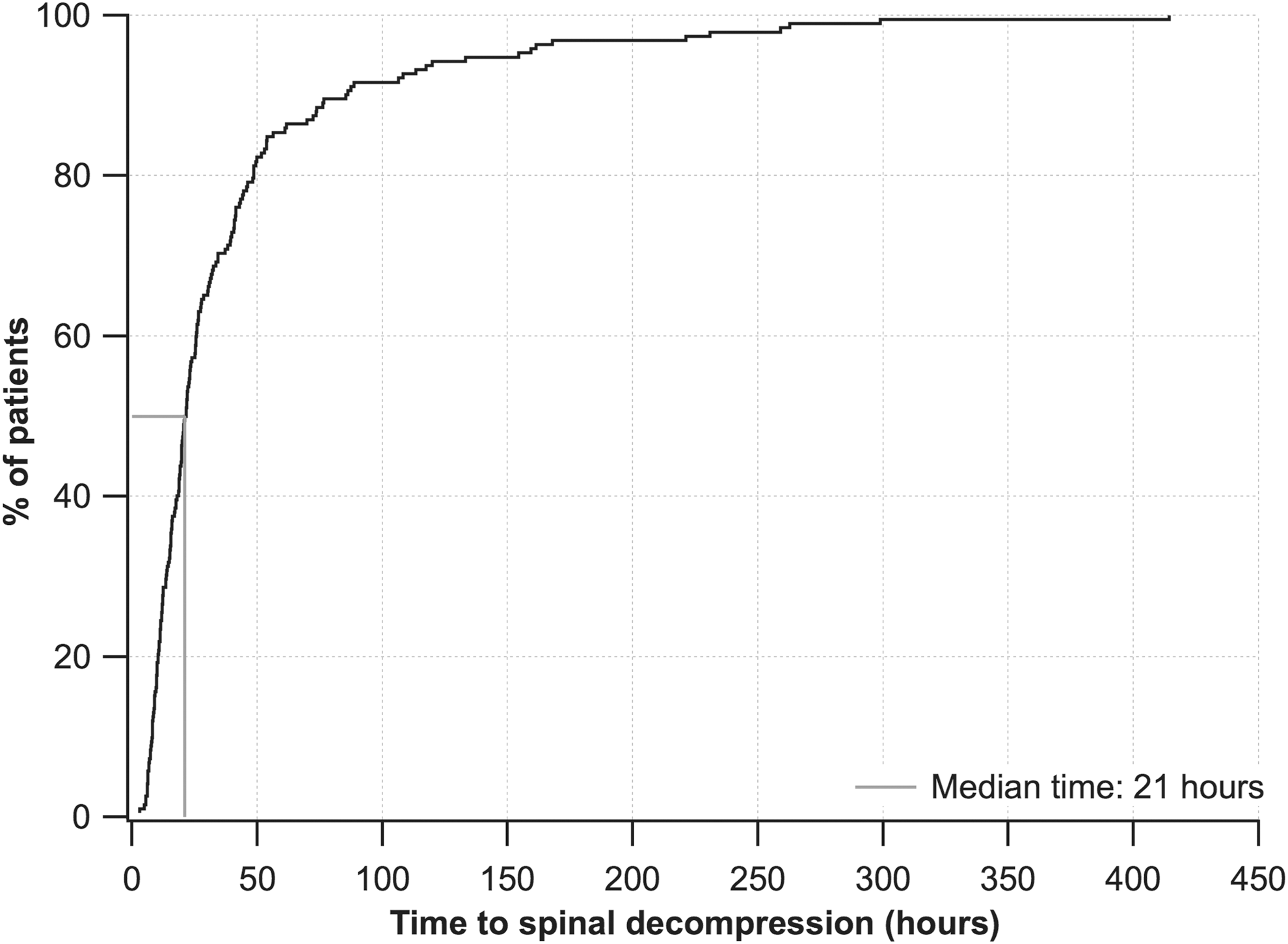
Timing of spinal decompression. Cumulative histogram showing the proportion of patients decompressed at different times (black line). The median time of spinal decompression is indicated by the vertical gray line.
Process of care
In order to understand the process of care from accident scene to decompression, this period was divided into three broad phases. The initial phase (paramedic time) was the period between time of injury and first hospital admission. This period was remarkably brief, with an overall median time of 1.1 h (IQR, 0.7–1.5). The next phase was admission to a pre-surgical hospital (time between admission at first hospital and admission to the surgical hospital). The median time for this phase was 8.9 h (IQR, 5.8–16). Admission to a pre-surgical hospital before transfer to a spinal surgical hospital occurred in 59% of cases, while direct transfer following paramedic assessment occurred in 41% of cases. The final phase was that of surgical hospital admission (time between surgical hospital admission to spinal decompression). This period had the longest median time (12.5 h, IQR, 7.6–21) and encompassed the time taken to complete radiological investigations and organize surgery. The timing of radiology is important, as surgical decisions are commonly based on these investigations. As expected, the median time taken to complete spinal CT scans was significantly shorter than the median time to complete spinal MRI (1.2 h, IQR, 0.7–2.1 and 4.5 h, IQR, 2.8–13, respectively; p < 0.0001). However, the time taken to complete radiology was a fraction of the total time from surgical hospital admission to spinal decompression (12.5 h, IQR, 7.6–21).
Improvement in the timing of spinal decompression
The median time to spinal decompression steadily decreased in each of the analyzed years (Fig. 3A). In 2010 (n = 44), the median time to decompression was 31 h (IQR, 15.9–52.2), decreasing to 22 h (IQR, 11.2–45.7) and 20 h (IQR, 11.8–42.8) in 2011 (n = 47) and 2012 (n = 51), respectively. By 2013 (n = 50), the median time to spinal decompression was significantly lower than 2010 (19 h, IQR, 11.1–26.7; p = 0.008). The yearly median time to spinal decompression, together with a cumulative histogram of the time to decompression for each individual site, can be found in Supplementary Figures 1A and 1B, 1C and 1D, 1E, and 1F and 1G (see online supplementary material at
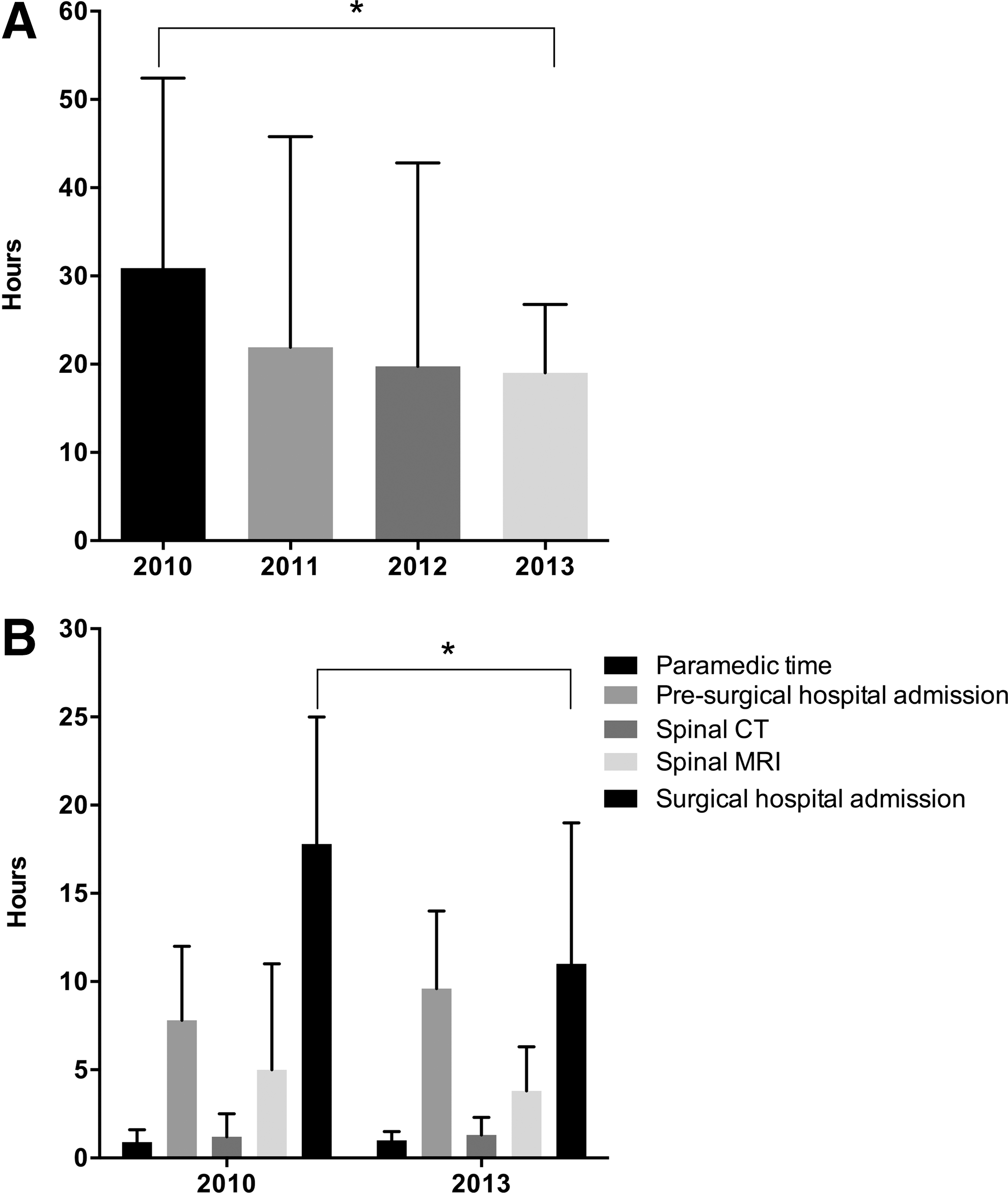
Time to spinal decompression by year.
To identify where improvements occurred over the study period, each of the three phases in 2010 was compared with those from 2013 (Fig. 3B). The median time from paramedic arrival to delivery of the patient to hospital was close to 1 h in both years (0.9 h and 1.0 h, respectively). The median duration of pre-surgical hospital admission also was not significantly different between these years (7.7 h in 2010 and 9.6 h in 2013). The median time from surgical hospital admission to decompression was the only phase that improved significantly between 2010 and 2013 (17.8 h and 11.0 h, respectively; p = 0.02). This did not appear to be a result of faster completion of radiological investigations, as the median time between hospital admission and CT and/or MRI scan was similar between 2010 and 2013 (CT, 2010 = 1.3 h and 2013 = 1.4 h; MRI, 2010 = 5.1 h and 2013 = 3.8 h). Collectively, these data suggest that the improvement in the process of care observed over the study period resulted mainly in reduced time to the operating theater.
One important factor contributing to the reduced time to decompression over the study period was an increase in the rate of direct admission to the surgical hospital. The percentage of cases taken directly to a surgical center demonstrated a gradual increase over the 4 years (2010 = 34%, 2011 = 40%, 2012 = 41%, and 2013 = 46%).
Factors associated with early and delayed spinal decompression
The main factor influencing the timing of spinal decompression was whether patients were taken straight from the accident scene to a surgical hospital or via a pre-surgical hospital. The process of care for these two groups of patients is represented in Figure 4. The overall median time to spinal decompression for cases taken via a pre-surgical hospital (26 h, n = 114) was significantly greater than for cases taken directly to a surgical hospital (12 h, n = 78; p < 0.0001). For patients admitted directly to a surgical hospital, the median paramedic time was 1.1 h (IQR, 0.8–1.5). The median time of the surgical hospital admission phase (time between surgical hospital admission and spinal decompression) was 11 h (IQR, 7.8–22). Within this phase, spinal CT and MRI were completed in a median time of 1.3 h (IQR, 0.7–2.2) and 4.1 h (IQR, 3.3–13), respectively, following admission.
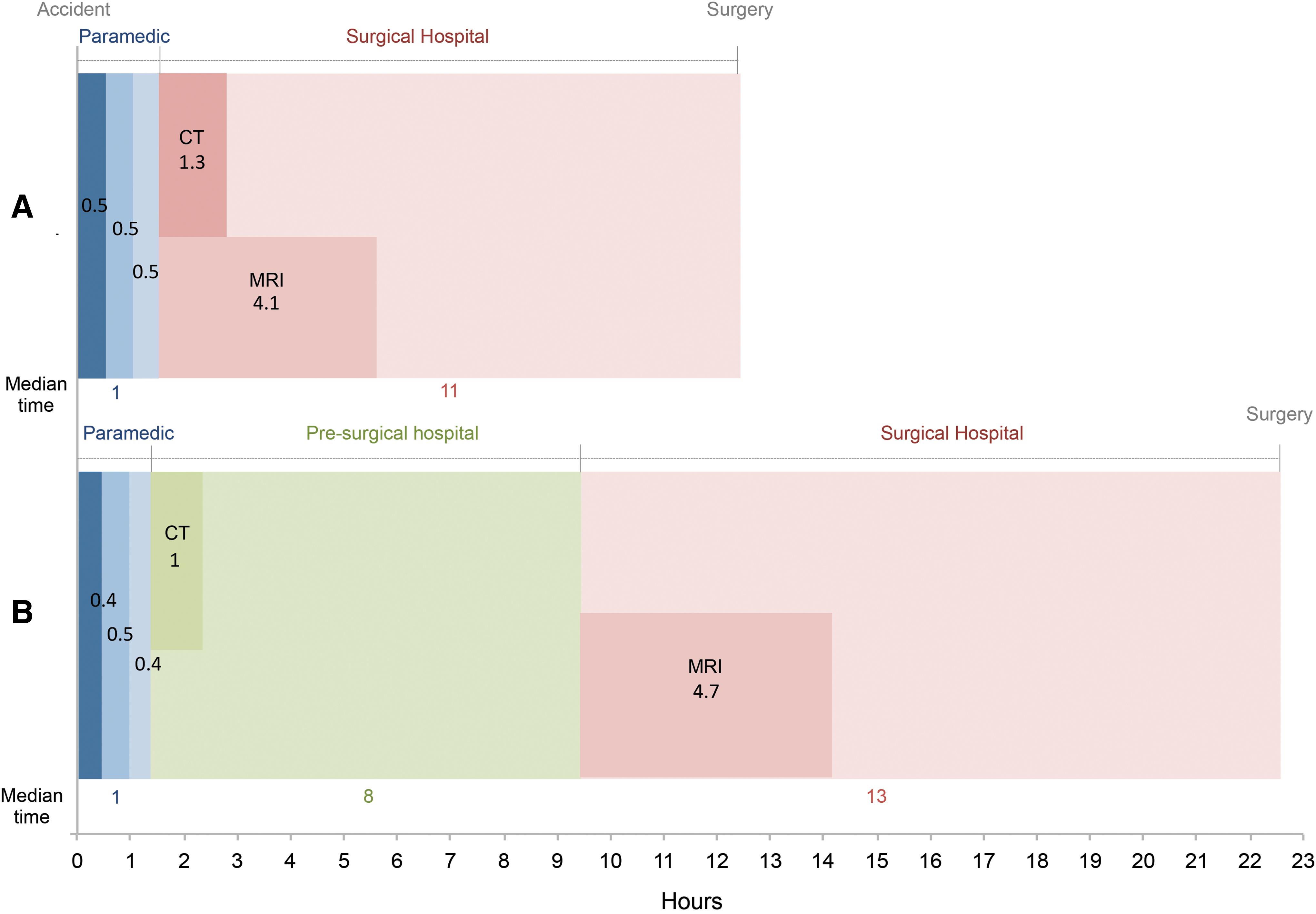
Horizontal bar chart showing the process of care for patients taken directly to a surgical hospital
For cases taken via a pre-surgical hospital, the paramedic time was also brief (1.1 h; IQR, 0.71–1.5). The median time of pre-surgical hospital admission was 8.9 h and this was consistent over the study period. The median time of surgical hospital admission in this group was 13 h (IQR, 7.4–21). While spinal CT was commonly performed at the pre-surgical hospital (90% of cases), spinal MRI scanning was usually undertaken at the surgical hospital (78% of cases). The median time between hospital admission and completion of radiology (CT, 1.0 h, IQR, 0.6–2.0; MRI, 4.7 h, IQR, 2.5–12) was similar to that for patients taken straight to a surgical hospital.
Another factor associated with early or delayed spinal decompression was the geographical location of injury. Patients injured in remote areas (10% of cases) had a significantly higher median time to decompression, compared with patients injured in metropolitan areas (34 h, IQR, 21–51 and 16 h, IQR, 10–26, respectively; p = 0.0002, Fig. 5A).
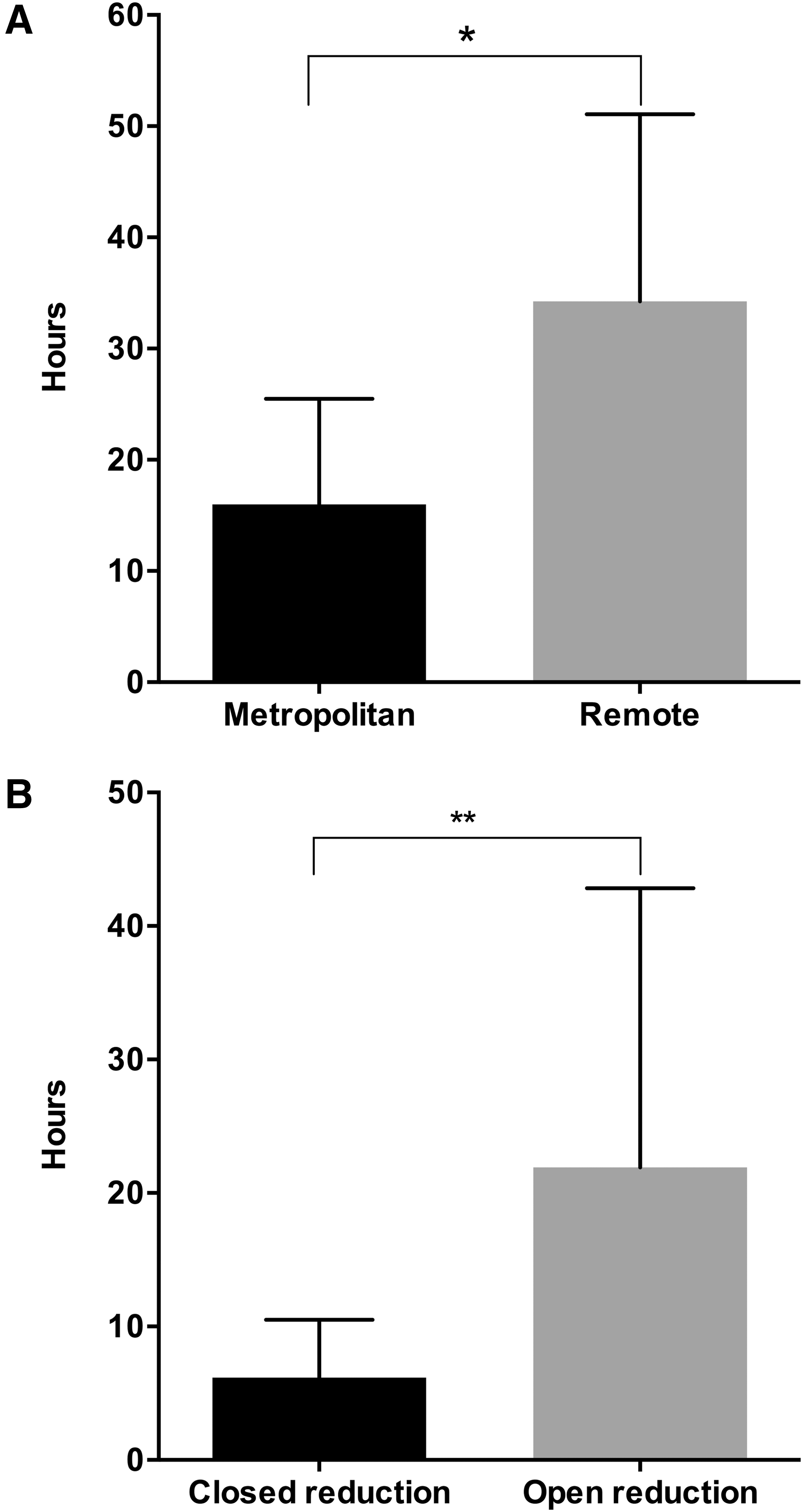
Factors associated with early and delayed spinal decompression.
The final important factor influencing the timing of spinal decompression was the method of reduction. Of the 192 cases included, only nine (5%) had successful closed reduction of the cervical spine (all performed in New Zealand). The median time to closed reduction was significantly lower, compared with the median time to open reduction (6 h, IQR, 4–11 vs. 22 h, IQR, 13–43; p < 0.0001; Fig. 5B).
Timing of spinal decompression and neurological change
The degree of neurologic improvement was measured by the change in AIS grade from acute surgical hospital admission to rehabilitation discharge. From 165 patients with documentation of the AIS grade data at these two time-points, 97 (59%) had no change in the AIS grade, while 45 (27%) and 18 (11%) cases had an improvement in the AIS by 1 and 2 grades, respectively. A 3-grade (A to D) improvement occurred in only four (2%) cases. One case (0.6%) changed from AIS B at surgical hospital admission to AIS A at rehabilitation discharge. None of the included patients improved to AIS E.
The median time to spinal decompression of patients who had no change or 1 grade improvement in the AIS was 24 h (IQR, 12–45) and 22 h (IQR, 13–34), respectively. The median time to spinal decompression of patients that improved by AIS 2–3 grades was lower, compared with the above patients (15 h; IQR, 8–38). This difference was not significant. In an analysis similar to the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS) trial, 6 we found that 16% of cases decompressed ≤24 h improved 2 or 3 AIS grades, whereas the same improvement occurred in 11% of cases decompressed more than 24 h after injury. This difference also was not significant (chi-square test, p = 0.35).
A relationship between the time of spinal decompression and the proportion of patients improving by 2–3 AIS grades was evident when the data were divided by time (Fig. 6). A progressively lower proportion of patients improved by 2–3 AIS grades as the time to decompression increased (Fisher's exact test, p < 0.005). The benefit of early decompression appeared to rapidly decrease with time and the relationship between the timing of decompression and the proportion of patients improving by 2–3 AIS grades fitted a power curve (r 2 = 0.97; Fig. 6).
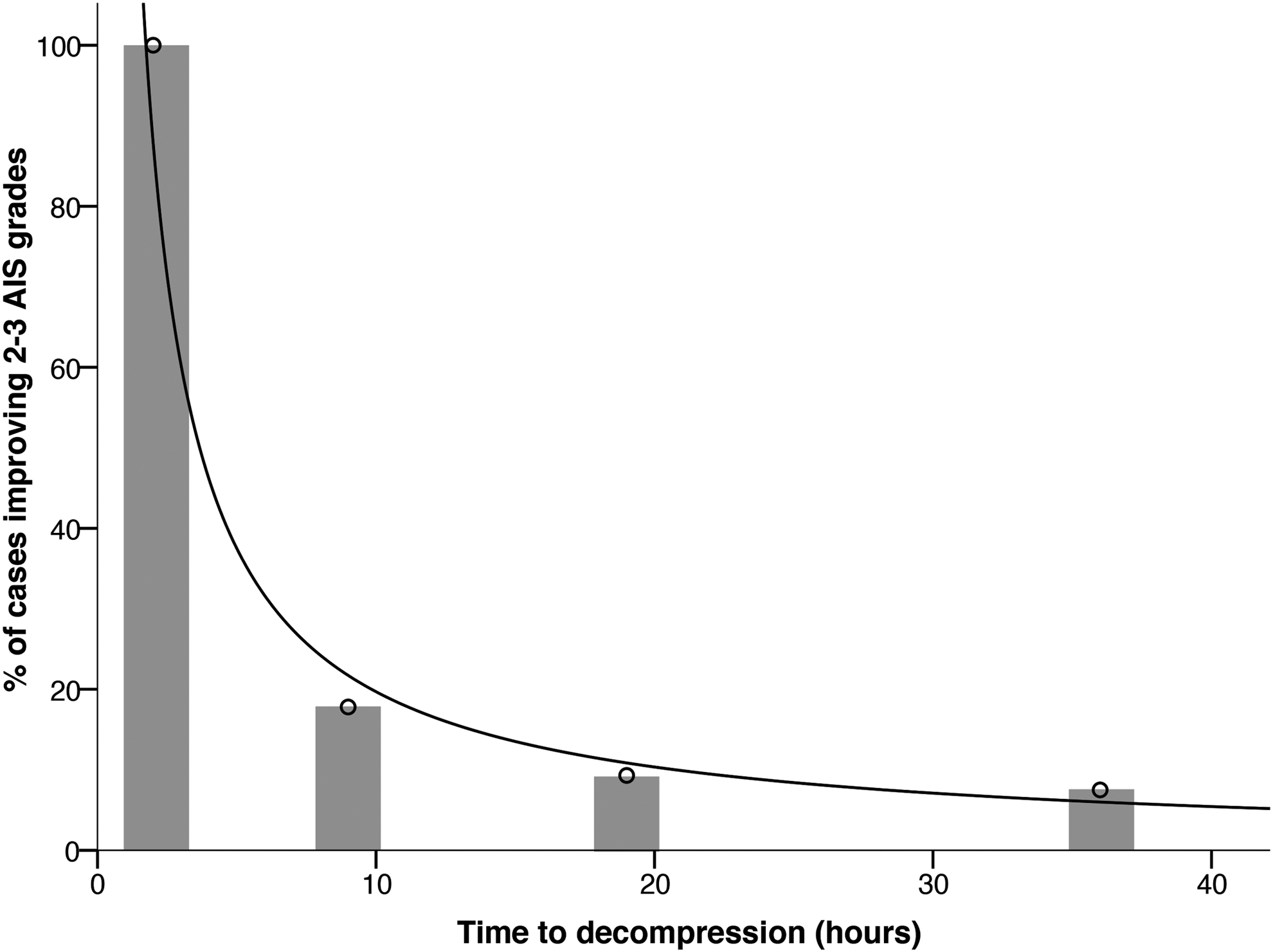
Timing of spinal decompression and neurological change. Bar graph showing the proportion of patients improving by 2–3 American Spinal Injury Association Impairment Scale (AIS) grades vs. time to decompression. A significantly lower proportion of patients improved by 2–3 AIS grades as the time to decompression increased (Fisher's exact test, p < 0.005). Number of patients improving by 2–3 AIS grades in each group: 0–4 = 2/2, 4–14 = 8/45, 14–24 = 4/43 and 24–48 = 3/40. The proportion of patients improving by 2–3 AIS grades rapidly decreased with time. The regression curve obeyed a power-law distribution (r 2 = 0.97).
We also analyzed the proportion of patients improving by 2 or more grades and undergoing closed or open reduction. Four of the eight patients treated with closed reduction within 12 h post-injury improved by 2 or more grades (median time to decompression = 5.8 h; IQR, 4–10). Only two of the fastest eight patients undergoing open reduction (median time to decompression = 6.2 h; IQR, 6–6.5) improved by 2 or more grades. However, this difference was not statistically significant.
Discussion
This study analyzed the process of care for patients with isolated cervical SCI and identified areas of major delay in the period from the accident scene to surgery. Identifying delays using current data allows the development of strategies to improve the efficiency of patient management. 21,22 In this study, we found the median time to decompression for cases of isolated cervical SCI within Australia and New Zealand was 21 h and this improved significantly from 31 h in 2010 to 19 h in 2013. The improvement in surgical timing over the study period was primarily due to a decrease in the time taken to access the operating theater following arrival at the spinal surgical hospital and, to a lesser extent, an increase in the proportion of patients admitted directly to a surgical center. Medical stabilization and radiological investigations did not appear to greatly influence the time to surgery.
We analyzed the overall process of care in seven different regions across two countries. A finding common for all services was a significant difference in the timing of decompression when patients were directly admitted to a spinal surgical hospital, compared with patients who were admitted to a pre-surgical hospital (12 h vs. 26 h, respectively). This difference in the timing of surgery was not simply a reflection of the duration of the pre-hospital admission and transfer, as the median time of these components was only 8.9 h. It may be that the urgency with which investigation and treatment are undertaken is driven to some extent by how rapidly a patient arrives. For example, if a patient arrives in the early morning or many hours following injury, investigations and surgery might be deferred until staff and facilities are routinely available.
Eliminating pre-surgical hospital admission would likely shorten the time to decompression. Our data demonstrate that this is gradually occurring in Australia and New Zealand, with the proportion of direct admissions increasing from 34% of cases in 2010 to 46% of cases in 2013. However, it is unlikely that pre-surgical hospital admission can be avoided all together. An important factor driving pre-surgical hospital admission in Australia and New Zealand are the adult major trauma guidelines, which stipulate the triage of patients to the highest level of the trauma service within 45 min. An additional factor is the difficulty of excluding other serious injuries in patients with cervical SCIs, particularly given the significant hypotension that complicates these injuries. 23,24
Another key area associated with surgical delay was the time taken to reach the operating theater following admission to a surgical center (median time 12.5 h). The bulk of this time occurred following medical stabilization, assessment, and investigation. Factors limiting access to the operating theater are unclear, but are likely to revolve around competitive surgical access 25 in the context of continuing uncertainties regarding the value and optimal timing of decompression. 6 –10
The areas of delay found in this study are in line with those identified by Furlan and colleagues. 21 These authors also reported that delay to decompression following cervical SCI was mainly determined by the period in a pre-surgical hospital, and the time waiting for a surgical decision following admission to a surgical center. 21 Although broadly similar, the delays in the Australasian and Canadian systems differ in several important ways. In the Canadian system, patients generally attended two and sometimes three pre-surgical hospitals before admission to a spinal surgical hospital. Delays associated with multiple transfers were long, with patients who underwent early decompression (< 24 h; n = 23) spending a median of 9.5 h at the first pre-surgical hospital alone and over 33 h if decompression was delayed. In contrast, our data demonstrate that in Australia and New Zealand, patients usually attend only one pre-surgical hospital with a median duration of 8 h.
Optimal timing of early decompression
The improvement in the timing of spinal decompression in Australia and New Zealand likely reflects the growing awareness of the value of early surgery. A number of studies and reviews have suggested that early decompression may be of value in facilitating neurological recovery. 6,8 –10 The largest study in this area (STASCIS), demonstrated a ≥2 AIS grade improvement in 19.8% of patients with cervical SCI undergoing early decompression (mean 14.2 h ± 5.4), compared with 8.8% of patients undergoing late decompression (mean 48.3 h ± 29.3). 6 The results of this study have added to the already favorable view of early decompression among surgeons worldwide. 26
A critical question driving further improvements is the optimal timing of spinal decompression. Pre-clinical studies consistently demonstrate that decompression is best performed as soon as possible following injury. In both small and large animal models attempting to replicate human injury, compression of the traumatized cord results in rapid neurological decline, with severe paraplegia developing within 3–8 h. 10,27 –33 Although spinal surgeons generally believe that operating early is optimal, preferably within 6 h for patients with severe incomplete injuries, 26 only Newton and colleagues 17 have examined decompression in humans at very early time-points. This study evaluated the benefit of closed reduction following low velocity fracture-dislocation injuries in rugby players. Of the 11 patients with complete motor paralysis decompressed within 4 h, eight made a complete recovery. None of the patients decompressed after this time made a complete recovery, while only three out of 30 (10%) recovered to AIS grade D. While encouraging, uncertainty remains and perhaps it is not possible to fully resolve the efficacy of early decompression and surgical stabilization without a clinical trial. No other study has examined decompression within the optimal time frame suggested by the pre-clinical literature, although Papadopoulos and colleagues 7 found that outcomes following decompressive surgery were inversely proportional to the time to decompression.
The data from the present study support the argument that decompression should be performed as early as possible. Although retrospective and based on small patient numbers, our data suggest that the proportion of patients likely to benefit from early surgery rapidly declines with time. Based on Newton and colleagues' data, 17 the optimal time for early decompression may be within the first 4 h following injury. Closed reduction, performed in a median time of 6 h in this study, appears to be the method most likely to achieve rapid realignment of the vertebral column within this time frame. The proportion of patients that might benefit from decompression within 4 h is unclear, although more than half appeared to benefit in Newton and colleagues' study. 17 It is likely that patients with adverse factors, such as bleeding into the cord, a long lesion length, 34 or a high initial force of injury, would improve less. Because of the apparent small effect size of decompression beyond 4 h, adequately powered studies would need to be large to detect differences between groups undergoing surgery before and after 24 h. We could not detect a clear relationship between the timing of early decompression and improvement in AIS grade in our study population when analyzed in this way.
Minimizing the time to decompression
The data from this study suggest a number of approaches that may facilitate early decompression in patients with cervical SCI: 1. Direct admission to a surgical center. 2. Decreased pre-surgical hospital admission time. 3. Rapid access to the operating theater following medical stabilization and investigation.
Several measures have the potential to help achieve these changes. First, it is important that paramedics are able to confidently identify cases of isolated SCI. This may help the decision on hospital destination and enable early notification of the spinal team involved at surgical centers. Early notification may enable medical staff involved in the care of spinal patients to organize radiological investigations and access to the operating theater. Prioritizing treatment and theater access using a “Code Spine” would perhaps be optimal. Systems that identify and give priority to certain groups of patients, as well as dedicated emergency theaters, have been shown to reduce pre-operative delays and improve theater efficiency. 35 Avoiding pre-surgical hospital admission would be optimal; however, as discussed, in many cases this is unavoidable. Reducing the duration of the pre-surgical hospital admission would seem logical in these cases. This might be facilitated by increased awareness of the urgency of early surgery, pre-hospital spinal management guidelines, as well as paramedic pre-notification of the spinal surgical center to help guide management and transfer.
Study limitations
In this study, analysis of the process of care was limited to patients with isolated cervical SCI within Australia and New Zealand. Exclusion criteria were carefully chosen so as to give the clearest picture of the areas in which delays occurred. Patients with multi-trauma were excluded, as spinal surgery may be delayed while other life threatening injuries are managed. Patients with TCCS also were excluded because of the current lack of consensus on the timing of surgery. Similarly, patients older than 70 were excluded because of the frequent occurrence of TCCS in this population and the potential for comorbidities delaying surgery. We also excluded patients with high cervical spinal cord injury (C0-C2), as the surgical management of these patients is often complicated. Analysis of the relationship of the timing of surgery to outcome was limited to AIS grade, as data on other outcomes including ASIA motor and sensory scores, was not collected as part of this study.
Conclusion
The median time to decompression in cases of isolated cervical SCI across Australia and New Zealand improved significantly over the study period. The fastest times to decompression occurred with closed reduction. Time to decompression appeared to be an important factor related to outcome, with a rapid reduction in the proportion of cases demonstrating substantial (2 to 3 AIS grade) recovery as time to decompression increased. Across Australia and New Zealand, the timing of decompression surgery was principally determined by two factors: admission to a pre-surgical hospital and the time taken to access the operating theater. Direct admission to a spinal surgical hospital, rapid access to the operating theater, and where indicated, closed reduction of cervical SCI are likely to be the most effective strategies to reduce the time to decompression.
Footnotes
Acknowledgments
This study is supported by the National Health and Medical Research Council; Institution for Safety, Compensation and Recovery Research; Spinal Cord Injury Network and Neurotrauma Research Program.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.