
Abstract
Despite an improved understanding of traumatic head and neck injury mechanisms, the impact tests required by major motorcycle helmet standards have remained unchanged for decades. Development of new test methods must reflect the specific impact loads causing injury in real crashes as well as test criteria appropriate for the observed injury profiles. This study analysed a collection of in-depth crash investigations of fatally injured helmeted riders in the Adelaide metropolitan region between 1983 and 1994 inclusive to review the head and neck injury patterns that resulted from specific types of impact.
Inertial brain injury was sustained in 49% of examined cases, most often resulting from facial impacts but also in a large proportion of tangential, run over, and occipital impact cases. Focal brain and brainstem injury was also common (53%) and regularly associated with skull vault (11/12) and skull base fractures (22/31). Prevention of these fractures in impacts outside the area of required protection and in impacts with a straight edge would provide a significant increase in helmeted rider protection. Cervical spinal cord injury was sustained in facial, straight edge, and tangential impacts on the head.
Motorcycle helmets are effective for preventing local skull fractures in impacts for which they are designed, whereas other serious injuries such as basilar skull fracture (BSF) and inertial brain injury persist despite helmet protection. Further impact test procedures should be developed for injurious impact types not currently assessed by major helmet standards, in particular facial impacts, and using test criteria based on commonly observed injuries. This study provides the necessary link, from impact load to injury, for guiding impact test development.
Introduction
M
The protective effect of a helmet is largely determined by the governing standards and regulations that outline minimum performance requirements. In many countries, these standards have remained substantially unchanged for decades 4 including Australian and New Zealand Standard AS/NZS 1698 Protective Helmets for Vehicle Users (AS/NZS 1698) and U.S. Federal Motor Vehicle Safety Standard 218 (FMVSS 218), on which AS/NZS 1698 is based. Since these standards were introduced in the 1970s, the impact tests required to ensure helmet compliance and effectiveness have not changed, whereas our knowledge of motorcycle crashes and head injury biomechanics has improved significantly. For example, our understanding that the brain is sensitive to rotational impulses 5 –7 has developed since the introduction of motorcycle helmet standards. The impact tests in major existing standards are unable to assess the effectiveness in preventing or reducing the risk of many types of head and neck injuries. New experimental procedures are required.
The process of designing an effective protective system for prevention of injury requires an appropriate test method based on understanding the mechanism of injury, quantifying the response of body tissues and systems to the impact condition, and determining the level of response at which the tissues or system will fail to recover. 8 Using these four pieces of information (the impact condition, the mechanism of injury, the response of the tissue, and the tissue tolerance), a meaningful experimental method for assessing a protective system, such as the helmet, can be developed.
Crash investigation studies provide an invaluable source of information for assessment of injury prevention devices beyond laboratory test procedures and with real injury consequences. 9 In a detailed European study describing 409 head lesions in 81 helmeted motorcyclists, with mostly fatal outcomes, skull fractures at the point of impact were overrepresented in crash events producing isolated translation or no kinetic consequence for the head, whereas brain lesions were the major injuries in rotational events. 2 These findings have significant implications for helmet design; however, the specific impact events leading to isolated translation or rotation were not clearly defined, with the authors noting that various types of helmet impacts produce head rotation.
The aim of this study was to review the patterns and distribution of head and neck injury sustained by helmeted motorcyclists in specific types of impact based on a detailed case-by-case analysis of the crash circumstances and helmet damage. In doing so, this study identifies and links the type of forces experienced by the head and neck of the helmet-protected rider (impact condition) with the head and neck injuries sustained. The information obtained will be used to guide further experimental studies for assessing the effectiveness of motorcycle helmets in preventing head and neck injury.
Methods
The National Health and Medical Research Council (NHMRC) Road Accident Research Unit (now the Centre for Automotive Safety Research, CASR) performed in-depth crash investigations of all fatally injured road users (vehicle occupants, pedestrians, cyclists, and motorcyclists) in the Adelaide metropolitan region between 1983 and 1994 inclusive.
10
A selection of the motorcycle crashes from this database was analysed in detail. Case selection criteria were as follows: • Helmeted motorcycle rider in fatal crash; • Helmet remained on for the duration of the crash; • Damage to the helmet was known; and, • Rider sustained more than superficial head or neck injury (i.e., fracture, brain or spinal cord injury).
In all, 47 of 173 motorcycle crash cases contained in the database met the criteria. Cases were most commonly excluded due to missing data (n = 64) or a helmet was not worn or was ejected during the crash (n = 46).
Circumstances of the crashes were reported in the database based on in-depth investigation of the crash site,the vehicle or vehicles involved, and the helmet. In 41 cases, the helmets had been retained by the original investigators and were reinspected for this study. The type of damage and damage location on the helmet were recorded and photographed. For the remaining six cases, the helmet damage was obtained from either a detailed description of the damage or photographs contained in the case file. Helmets in all cases displayed impact damage. Helmet weight was not collected for this study.
Injury data were collected at autopsy. All marks on the body were recorded and photographed paying particular attention to the head and face. Injuries to the scalp and skull were noted by inspecting both their inner and outer surfaces. In each case, the coroner removed the brain for subsequent detailed analysis by a neuropathologist who macroscopically examined 10-mm coronal sections of the whole brain, cerebellum, and brainstem. 10 Microscopic examinations were performed in 35 of the 47 cases. Of the remaining 12 cases, histology status was unknown for six cases, not performed for four cases with minimal survival time (less than 40 min), no noticeable brain trauma and a cause of death unrelated to the head and neck, and also not performed in two cases of severely traumatized brain (extensive lacerations with no evidence of reactive hemorrhage or contusion at the margins). Tinctorial stains were used to detect the presence of axonal injury as detailed by Blumbergs and colleagues 11 and included Nissl's method using cresyl violet, Weil stain for myelin, hematoxylin and eosin (H&E), and silver methods such as the Glees and Marsland and Palmgren techniques for axons.
A detailed case-by-case analysis was performed using the crash circumstances, helmet damage, and injuries sustained by the rider to classify each of the rider's injuries according to Table 1, based on the head injury mechanisms described by Gennarelli 12 with some modifications.
SDH, subdural hematoma.
Local contact injuries were directly at the site of impact and typically included skull vault and facial fractures corresponding to damage on the helmet and consistent with the crash circumstances. Contusions and lacerations to the brain or brainstem and subdural hematoma (SDH) were classified as local contact injury if located in the same area as a local contact skull fracture. Cervical injury was classified as a local contact injury if it was determined that the injury was caused by a direct impact during the crash.
Remote contact injuries did not occur at the point of impact but were the result of transmitted force from the impact site. Skull fractures and cervical spine injuries resulting from impact to some other part of the head were classified as remote contact injuries. Contusions and lacerations to the brain or brainstem and SDH were classified as remote contact injury if associated with a remote contact skull fracture.
Inertial injuries were related to the inertia of the brain causing injury in the crash. Coup lesions, contrecoup lesions, and SDH not located with skull fractures were classified as inertial injuries. Petechial hemorrhages and gliding contusions in the white matter of the cerebral hemispheres, the corpus callosum, and the brainstem were identified in the microscopic neuropathological examinations and were considered marker lesions of diffuse axonal injury (DAI). DAI is particularly difficult to diagnose, especially in cases of short survival time after the trauma. 13 It has been recognized that axons are often damaged around focal lesions such as petechiae and these marker lesions can be observed even in patients of short survival time. 6 However, using these marker lesions has shortcomings and is a limitation of this study. Types of these lesions can occur due to non-traumatic cerebrovascular disease, 14 and DAI lesions can also be non-hemorrhagic. 15 Nevertheless, petechiae and gliding contusions in the white matter and corpus callosum were classified as inertial injuries. To avoid misdiagnosis, cases with petechial hemorrhages only in the brainstem were excluded as inertial injuries because of their occurrence as secondary injuries in pathologies such as transtentorial herniation. 16
To provide an indication of crash severity, the somatic (below the neck) injuries were assessed in each case. Cases were grouped based on the severity of the most severe somatic injury sustained by the rider. Injury severity was coded in accordance with the Abbreviated Injury Scale (AIS), 1990 revision.
Two researchers independently assessed the predominant impact, or primary head impact type, experienced by the rider in each case based on the crash circumstances, the type and location of the observed helmet damage, and the injuries sustained by the rider (including external superficial injuries). When assessing helmet damage, shell cracks were considered to result from a more severe impact to the head than areas of shell scratches or scuff marks.
Results
The examined cases consisted of 46 males and one female with an age range of 17 to 43 years. The most common cause of death was brain or brainstem injury (n = 21) followed by ruptured aorta or heart (n = 15). Neck injury was the cause of death in six cases. Survival time was recorded in 44 cases with most surviving less than 2 h (n = 38). Table 2 indicates that white matter petechiae were more commonly observed in riders that survived longer than 60 min (9 of 10 cases with confirmed histology) than the remainder (7 of 23 with confirmed histology).
DOA, dead on arrival.
Estimated pre-crash speed was recorded in 39 cases with a mean of 82.7 ± 34.2 km/h (range 5 to 160 km/h). The majority of crashes (n = 28) were multiple vehicle collisions with the most common collision opponent being passenger cars (n = 14) followed by trucks/prime movers (n = 12). Roadside poles/trees were the most common non-vehicular collision opponent (n = 12).
All helmets were labelled as satisfying the required performance standard, and included 39 full-face helmets and eight open-face helmets. The protective energy absorbing liner was expanded polystyrene foam (EPS) in all cases. Shell material was obtained from the helmet labelling in 39 cases and found to be predominantly fiberglass (n = 27), thermoplastic (n = 11), and in one case, Kevlar® and glass fiber. These construction materials remain commonly used for motorcycle helmets today.
Table 3 shows the frequency of head and neck injuries sustained. At the point of impact (local contact injuries), facial fracture occurred in 10 and skull vault fracture in 12 cases (three cases had both types of fracture). Underlying local contact brain contusions/lacerations were not observed in cases of only local facial fracture (below the frontal bone), but were frequently observed underlying skull vault fractures (11 of 12) including three cases of both frontal and facial bone fractures. Most cases of local contact fractures to the face or vault also sustained a remote facial fracture or remote skull base fracture (16 of 19), either through transmission of force from the point of impact or from progression of the fracture to the remote region. Remote contact BSF was the most frequently observed injury and also occurred in the absence of injury at the point of impact (15 of 31). Contusion/laceration to the brain or brainstem associated with a remote fracture occurred in 22 of 31 cases.
SDH, subdural hematoma.
The relationship between fracture types and associated focal brain injury is presented in Figure 1 as a Venn diagram. Contusions/lacerations underlying fractures occurred in 25 of 34 cases that sustained a skull fracture.

Venn diagram of local contact facial fracture cases (n = 10), local contact skull vault fracture cases (n = 12), and remote contact skull fracture cases (n = 31) compared with local and remote contact cortical contusion/laceration cases (n = 25). Diagram produced using Venny 2.0.2. 27
Inertial injury to the brain was sustained in 23 cases. The most common injury was petechial hemorrhages to the hemispheric white matter (18 cases). Contusions and SDH not underlying a skull fracture occurred in 11 and six cases, respectively. Three cases of inertial SDH occurred without other brain injury (contact or inertial).
One local contact cervical spine fracture was caused by direct impact with a wire fence. However, the majority of the cervical spine injuries (13 cases) resulted from an impact to the head (remote contact injuries). Most involved a fracture and concomitant cord damage (nine cases), but there were three cases of cord damage without fracture and one case of a remote fracture without cord damage.
The association of cervical spine injury to the main head injury types is presented in Figure 2, which shows that the majority of remote cervical spine injury cases also sustained some head injury (11 of 13), either with a skull fracture (seven cases) or brain injury (four cases) but not all three together.
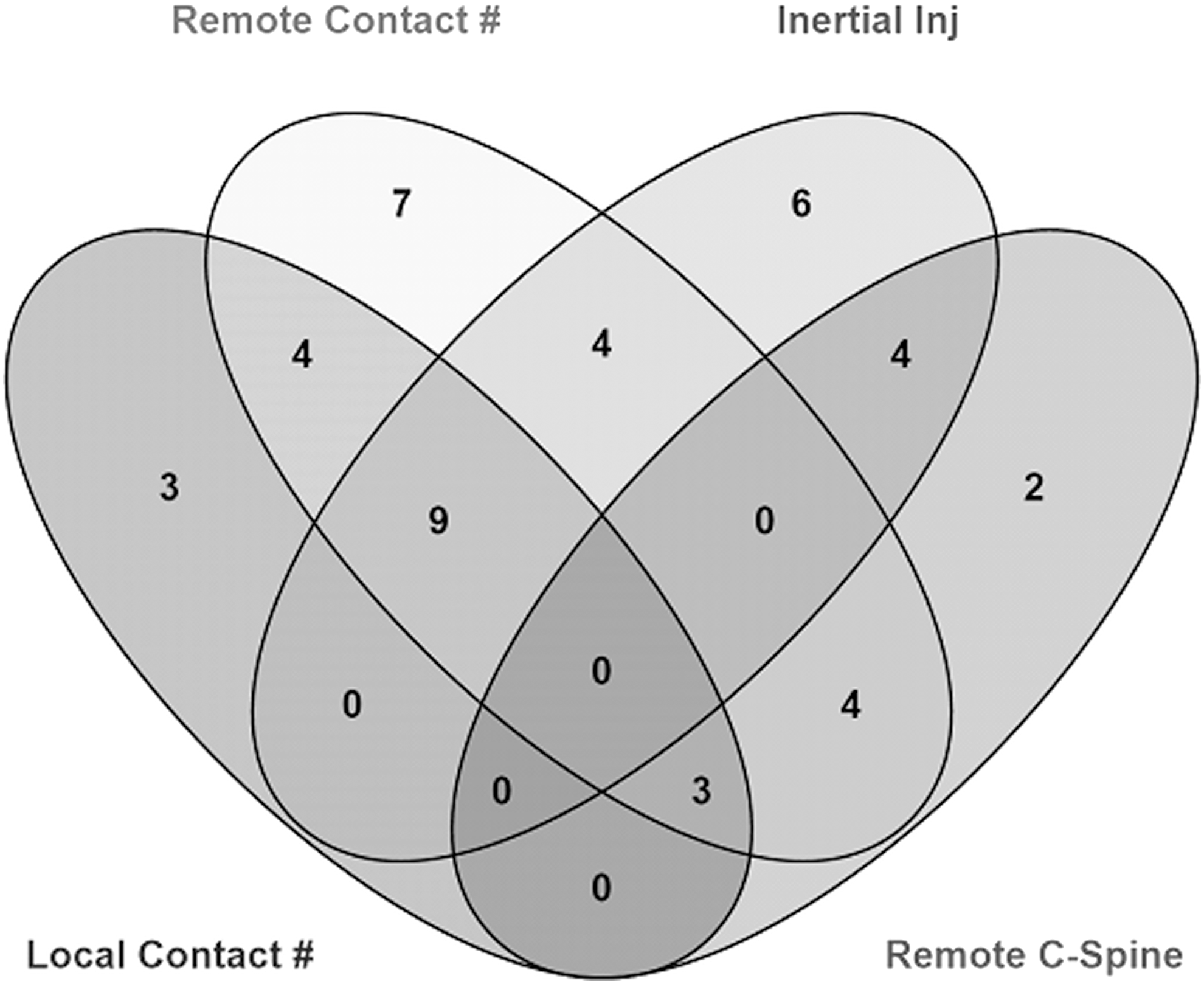
Venn diagram of local contact skull fracture cases (n = 19), remote contact skull fracture cases (n = 31), and inertial brain injury cases (n = 23) compared with remote cervical spine injury cases (n = 13). Diagram produced using Venny 2.0.2. 27
Somatic (below the neck) injury severity was used as a measure to compare the level of forces acting upon the rider. Figure 3 shows the interaction of head injury incidence with cases that sustained a severe (AIS 4+) somatic injury (high severity crashes). Most of the high severity crashes resulted in a skull fracture (18 of 24), but skull fracture was also sustained in cases considered to have a lower severity (8 of 19 local fractures and 16 of 31 BSFs). Inertial brain injury was more commonly sustained in cases without severe somatic injury (15 of 23) suggesting that this type of brain injury can be sustained in crashes of a lower severity.
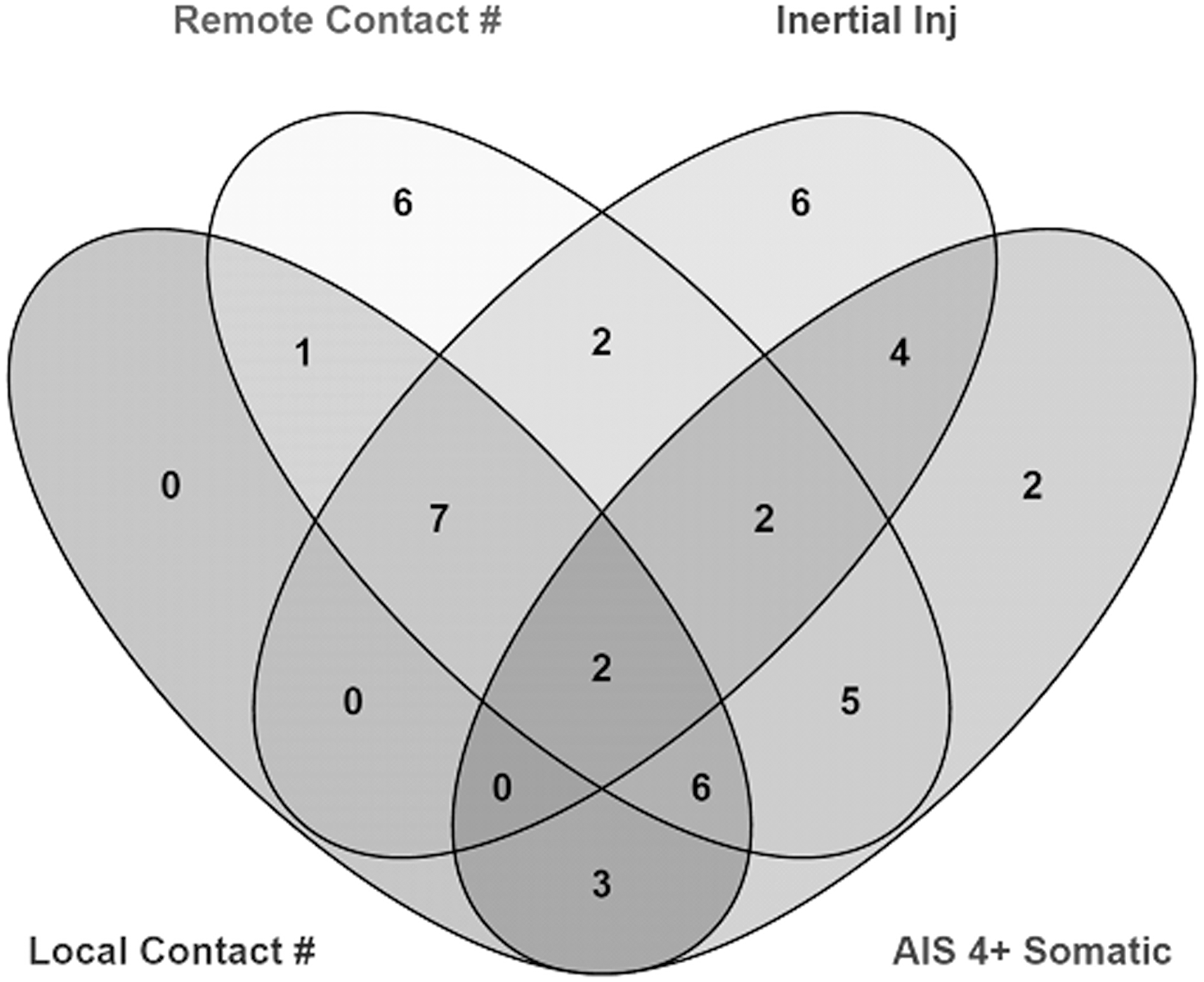
Venn diagram of local contact skull fracture cases (n = 19), remote contact skull fracture cases (n = 31), and inertial brain injury cases (n = 23) compared with AIS 4+ somatic injury cases (n = 24). Diagram produced using Venny 2.0.2. 27 AIS, Abbreviated Injury Scale.
A summary of the primary head impact types and the main head and neck injuries is shown in Table 4. Impacts to the facial region of a full-face protected rider were the most common primary head impact type (20 cases) followed by impacts with a straight edge within the region of the impact attenuation test of AS/NZS 1698 (seven cases).
Note that a single case often sustained multiple types of injury. The total in this column reflects the total number of cases of each primary head impact type.
AIS, Abbreviated Injury Scale; SDH, subdural hematoma.
Cases where the helmet was run over (six) displayed similar patterns of helmet damage consisting of an area of deep scratches combined with impact damage to the other side of the helmet. In four of the run-over cases black scuff marks, likely from a tire, were present on the helmet. All run-over helmets retained their original shape suggesting they were not subjected to the full weight of a vehicle, but were rather involved in a complex multiple impact event in collision with the vehicle (in most cases the tire) and the roadway. Tangential type impact damage was rarely the primary head impact type (two cases).
Local contact skull fractures were usually sustained from impacts outside the area of impact attenuation prescribed by AS/NZS 1698 (facial, occipital, run-over, and unprotected impacts totalling 14 of 19 cases), and in straight-edge impacts to the area of protection (five cases). Similar insults resulted in remote BSF and, in addition, three cases of flat impacts within the area of required impact attenuation resulted in skull base fracture.
Facial impacts were the main contributor to cervical spinal cord injury, inertial SDH, and DAI indicator lesions. However, both tangential impacts resulted in spinal cord injury and inertial SDH. Five of six run-over cases resulted in DAI indicator lesions.
Discussion
This study provides a picture of the head and neck injuries sustained by fatally injured helmeted motorcycle riders when subject to specific types of head impact, confirming the prevalence of BSF and intracranial lesions despite helmet protection. Cases described in the present study are comparable to the 81 AISHead2+ cases detailed by Richter and associates 2 (primarily Munich-based cases that were 95% fatal and with a mean vehicle impact speed of 73.7 km/h) and show a consistent distribution of head injuries. The fact that similar injuries continue to be observed even in more recent crash investigations highlights the need for further investigation of how they are being sustained and emphasizes the importance of this study. The present study is also able to distinguish between neurotrauma associated with remote fractures and inertial brain injury, both classified as indirect force lesions by Richter and associates 2 despite distinctly different injury mechanisms. Description of the specific impact types and the resulting injury outcomes provided in this study are required for development of new impact procedures to improve helmet effectiveness.
Remote contact BSF was the most commonly observed injury in the cases examined (31 cases) and regularly associated with focal contusions and lacerations of the brain and brainstem (22 cases). The primary impact types leading to BSF identified in this study correspond to the main mechanisms documented in the literature. In some cases, local fractures of the facial bones, the vault, or the occiput propagated to the skull base. Straight-edge and flat impacts within the area of impact attenuation that resulted in BSF are consistent with cadaver experiments that showed, in padded superior-inferior impacts to the head and neck complex, the skull base and neck was most susceptible to injury rather than the point of impact. 17 Most frequently, BSF was sustained in impacts to the face (13 cases), an insult also replicated in experimental cadaver studies 18 with documented implications for brainstem injury. 19 BSF poses a difficult challenge for prevention through helmet protection and the frequency of this injury in severely injured helmeted riders is reason for further investigation.
The previously observed high frequency of brain lesions in helmeted riders 2 has meant that brain injury risk reduction for helmeted motorcyclists has received considerable attention. Researchers have proposed new test methods for oblique, or tangential, impacts 20,21 given the majority of helmet impact damage results from this type of impact 22 resulting in the emergence of novel helmet designs. 23 –25 Cases of primarily tangential impact damage in the present study (two cases) both resulted in inertial intracranial injury (Table 4); however, tangential impact was rarely the predominant impact. Even in the tangential impact cases, it was difficult to determine the amount of radially directed force on the helmet and head because the outer surface of the protective liner could not be inspected. Inertial brain injuries were sustained in a number of other load conditions including run-over, facial, and occipital impacts. The high proportion of inertial brain injury in run-over cases (five of six), many without other head or neck injury (four cases), suggests the brain may be vulnerable to multiple impact complex motion events. Given the overall high frequency of inertial brain injury (49%) and the primary impact types seen in this study, effective helmet assessment requires the use of specific brain injury mechanism related criteria, not only for tangential impacts but also complex motion events, and facial and occipital impacts.
Facial impacts were identified by this study as a common loading condition resulting in serious head and neck injury to helmeted motorcycle riders. Despite previous studies also indicating that facial impacts are both frequent 2,26 and injurious, 22 impact testing is not required for this region of the helmet in major international standards. The present study showed that protection from facial impacts is complex due to the various types of injuries that can result. Even with full-face helmet protection, facial impacts can result in BSF, with or without facial fractures. Facial impact can also produce inertial SDH and diffuse brain injury in the absence of fracture, although most brain injury occurred with skull fractures or neck injuries suggesting helmet impacts of a certain severity are more likely to result in brain injury. Facial impact protection represents an area where helmets may be improved and the results of this study indicate that assessment of helmet protection requires the use of more than a single injury criterion and, most likely, should incorporate the injury mechanisms for the facial bones, skull, brain, and cervical spine.
The main impact attenuation test in AS/NZS 1698, as with many other international motorcycle helmet standards, involves dropping an instrumented rigid headform, fitted with the test helmet, onto a rigid anvil. Peak linear acceleration of the headform center of gravity must be below a certain value for helmet compliance. This impact test was developed in the 1960s 27 based on the earliest and most widely used biomechanical head injury tolerance data that formed the Wayne State University Concussion Tolerance Curve (WSUCTC). 28 Despite the name, the WSUCTC primarily used the level of linear acceleration required to produce a linear skull fracture in an adult cadaver. The fact that no local skull fractures in the present study were sustained in impacts similar to those required by AS/NZS 1698 demonstrates the success of this impact test. Compliant motorcycle helmets are essentially designed for a specific load condition (impact within required coverage area) and limit the headform response (peak linear acceleration) below the level of tissue failure (skull fracture threshold). This study provides necessary information for developing new experimental procedures for other injurious impact conditions.
The limitations of this study are as follows. As has been discussed, this study made use of petechial hemorrhages as an indicator of DAI. Identification of DAI and staining procedures have improved since the data used for this study were collected, with the use of beta amyloid precursor protein (βAPP) 29 staining able to detect axonal injury in cases of only 35-min survival. 30 As a result, DAI may be more prevalent than reported in this study given the methods used and a majority of riders with a short survival time (Table 2). Further, a small number of fatal crashes were used in this analysis. The context of fatal crashes needs to be remembered, making up only 2% of all motorcycle crashes in New South Wales in 2013. 31 These crashes are the most severe and in some cases no amount of improved helmet protection would affect the fatal outcome. Finally, the cases used in this analysis were collected between 1983 and 1994. Since then, many factors have changed including road conditions and rider attitudes and behaviors, among others. Importantly however, the impact tests required by the applicable motorcycle helmet standard have not changed, nor have the primary construction materials that offer the injury risk reduction provided by helmets. The fact that similar head injuries continue to be observed in more contemporary crash investigation studies of helmeted riders 2 also indicates the outcomes of this study are still relevant today.
Conclusion
The case-by-case analysis employed in this study details particular impact configurations experienced in real crashes that resulted in head and neck injuries to helmeted riders. The observed injury profiles indicate the success of the motorcycle helmet standard drop test in preventing local skull fractures in similar impacts. However, serious head and neck injuries such as BSF and inertial brain lesions persist despite helmet protection and are sustained in many impact types that are not assessed in current major motorcycle helmet standards, in particular facial impacts. This study provides the necessary information for guiding future development of experimental helmet test methods aimed at increasing the capabilities of motorcycle helmets in preventing serious head and neck injury in crashes.
Footnotes
Acknowledgments
The authors would like to acknowledge the library and research staff at the University of Adelaide Centre for Automotive Safety Research for their help with reinspection of the case helmets and files.
Author Disclosure Statement
No competing financial interests exist.