
Abstract
The Neuromuscular Recovery Scale (NRS) is a tool for measuring functional recovery in spinal cord injured (SCI) persons based on tasks that test pre-injury functional capability. The NRS has been shown to be a valid, reliable, and responsive instrument for measuring functional recovery. The NRS has been updated to include three items measuring upper extremity function, and a new scoring mechanism has been defined. The purpose of this prospective, observational study was to explore the properties of the expanded NRS, introduce and evaluate the new scoring method, and to examine the score's relationship with other SCI outcome measures. The NRS and seven other SCI outcome measures were assessed at enrollment and after every 20 locomotor training sessions in 64 participants of the NeuroRecovery Network (NRN) of the Christopher and Dana Reeve Foundation (CDRF). The NRS exhibited a dominant first principal component that correlated strongly with the new NRS score, as well as a potential secondary component discriminating upper extremity function. The new NRS score and its empirical subscales were generally well-correlated with International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI) motor scores and other established SCI functional measures, but exhibited substantial variability at their boundary values. The NRS score was more strongly correlated with other SCI functional measures than ISNCSCI motor scores were. The new NRS score was most responsive to change brought on by locomotor training. The expanded NRS appears to be a valuable tool in measuring functional recovery from SCI; further evaluation of its psychometric properties is warranted.
Introduction
P
The sensitivity and responsiveness of ISNCSCI motor scores to the complexities of paralysis within an American Spinal Injury Association Impairment Scale (AIS) classification and in response to activity-based therapy in chronic patients are limited, however. Other SCI outcome measures such as the Functional Independence Measure (FIM) and the Spinal Cord Independence Measure (SCIM) to date have focused on the assessment of a patient's ability to perform a task using his or her remaining functional capacity. 7,8 Thus, improvements on scales like these do not necessarily reflect neurological improvement and may actually measure compensated improvement to a greater extent.
The Neuromuscular Recovery Scale (NRS) was developed within the NeuroRecovery Network (NRN) to provide a novel measurement tool addressing specifically the recovery of the neurological state post-traumatic SCI and establish a classification scale focused on uncompensated task-specific recovery that can be used in clinical and research settings. 9,10 The original NRS evaluated 11 motor tasks involving the trunk and lower extremities, and an ordinal summary measure—referred to as the NRS Phase—has been shown to differentiate individuals into distinct functional performance groups that exhibit substantially reduced variability in commonly used outcome measures. Psychometric testing has established the validity, 11 test-retest reliability, 12 and inter-rater reliability 13 of the NRS, and it has been shown to be able to detect change from enrollment to discharge in a standardized activity-based therapy program. 9,14
The developers of the NRS have noted limitations of the scale. The functional classification provided by the NRS does not encompass the full spectrum of recovery, both at the item level and the summary score level. Specifically, each item of the NRS corresponds to a functional task, which was graded on a 10-point ordinal scale (see Appendix 1; see online supplementary material at
A related limitation of the NRS is the absence of tasks evaluating upper extremity function, because only trunk and lower extremity tasks are evaluated. It is generally understood that a normal functioning pelvis/trunk (postural control) is the foundation for both upper limb and lower limb function. Ultimately, without a normal functioning pelvis, the lower extremities for gait and upper extremities cannot perform tasks in a normal fashion. 15 Thus, the addition of items testing function in the upper extremities would expand the NRS into a measure that assesses three components of normative function: the trunk/pelvis, the upper extremities, and the lower extremities.
In partial response to these limitations, a new version of the NRS has been developed, reflecting several changes to the scale. Three items evaluating upper extremity function have been added to the NRS, and one item measuring treadmill performance has been removed. The ordinal grading scales for each NRS item have been expanded to better capture the full recovery spectrum for each task, and a new summary measure, referred to as the NRS Score, has been introduced. A noted deficiency in the development of the NRS has been the lack of use among patients with American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade A and B injuries. The purpose of this study was to introduce the upper extremity dimension of the NRS, examine relationships among the three NRS dimensions (treadmill, lower extremity, upper extremity), extend the use of the NRS to persons with AIS grade A and B injuries, introduce and examine the NRS Score, and further compare the NRS to ISNCSCI examination data and other existing outcome measures.
Methods
Participants
We examined 152 participants with complete or incomplete SCI who completed at least 20 sessions of a locomotor training (LT) program across six outpatient rehabilitation centers in the Christopher and Dana Reeve Foundation NRN: Frazier Rehab Institute, Louisville, KY; Kessler Institute for Rehabilitation and Kessler Foundation, West Orange, NJ; Magee Rehabilitation Hospital, Philadelphia, PA; The Ohio State University Medical Center, Columbus, OH; Shepherd Center, Atlanta, GA; and The Institute for Rehabilitation and Research, Houston, TX. All participants met the following inclusion criteria: (1) no-progressive spinal cord lesion above T11, AIS A, B, C, or D; (2) no current participation in an inpatient rehabilitation program; (3) medical referral by an NRN physician; (4) capacity to generate a lower limb reciprocal alternating flexion/extension stepping pattern in the step training environment using body weight support on a treadmill with manual facilitation; (5) ability to wean off of antispasticity medication under the direction of an NRN physician.
All participants took part in the NRN's standardized LT protocol. This protocol has been described in detail previously, 16 so we briefly summarize the protocol here. A LT session consists of 60 min of total weight bearing time with at least 20 min of step retraining in the treadmill and body weight support environment with manual assistance available. 10 An additional 15 to 30 min of over-ground activities occur after the treadmill training, with a focus of translating skills to the home and community environments.
The frequency and intensity of training sessions are varied based on patient need and capability; nearly all patients undergo 3–5 training sessions per week. Comprehensive patient evaluations occur approximately every 20 training sessions, and during these evaluations, the outcomes that are considered in this article are measured.
NRS
The original version of the NRS was developed between 2000 and 2008 by clinicians and researchers in the NRN. The NRS was originally developed as a classification tool in which patients were categorized into one of four classes of neuromuscular recovery after SCI, called Phases, based on their ability to perform specific motor tasks at a pre-injury level. 9,10,14 The Phases of recovery were enumerated so that Phase 1 represents the lowest degree of functional recovery and Phase 4 represents full recovery of pre-injury functional capacity. Incremental improvements in function were marked by alphabetized sub-Phases within Phases 1 through 4—e.g., Phases 1A, 1B, 1C, 2A, etc. The initial version of the NRS 9 consisted of 11 motor tasks that were evaluated in the over ground and body weight supported treadmill environments, with each task focusing on trunk and lower extremity function.
The NRS has since been extended in three ways. The first change to the NRS was the inclusion of three upper extremity items as a means of assessing the recovery of upper extremity function in persons with tetraplegia. These three upper extremity items are the (1) forward reach and grasp, (2) door open and pull, and (3) overhead press. These tasks are intended to simulate functional tasks involving the upper extremities in a person's daily life. In addition, an existing NRS item measuring performance on the treadmill—Stand Retraining—was removed from the scale. The second change made to the NRS was the addition of three sub-Phases to Phase 4—4A, 4B, and 4C—for all NRS items to fully capture the recovery of patients at the high end of the recovery spectrum.
The third change was the introduction of a new summary measure for the NRS, called the NRS Score and defined as the simple sum of the scores from each of the 13 NRS items, where item scores ranged from 1–12: 1 corresponding to Phase 1A and 12 corresponding to Phase 4C. The NRS Score is distinct from the existing NRS summary measure, the NRS Phase, which is calculated according to a previously published algorithm based on the NRS item exhibiting lowest function.
9,10,14
The procedures for assessing and scoring all 13 items of this extended NRS are detailed in an appendix to this article; Appendix 1 (see online supplementary material at
With these updates, the current version of the NRS can be empirically divided into three sets of items—body-weight support treadmill (BWST) items (1–3), trunk and leg (TL) items (4–10), and arm and shoulder (AS) items (11–13). Each of these sets of items can be regarded as an empirical subscale of the NRS, with scores generated as the simple sum of subscale items. An empirically derived subscale consisting of all nontreadmill items was also considered (TL + AS), in an effort to extend the utility of the NRS beyond the treadmill environment. The NRS takes approximately 45 min to administer. Treadmill items require up to four personnel for administration and the remaining trunk, lower limb, and upper extremity items require 1–2 personnel. 12
Additional outcome measures
The ISNCSCI examination is an assessment that is widely used and accepted for classification of the level and completeness of neurological deficit after SCI. 1 This scale assesses dermatomal light touch and pinprick sensation as well as motor strength. The motor strength is assessed in selected muscle groups in the upper and lower extremities, and upper, lower, and total motor scores are used to quantify motor strength (abbreviated UEMS, LEMS, and TMS, respectively). The AIS classification determines the extent of the SCI. The reliability and validity of ISNCSCI motor scores have been thoroughly evaluated, 2 –6 but their responsiveness to activity-based rehabilitation interventions is questionable. 17 The ISNCSCI exam is administered to patients in the NRN on enrollment and at discharge from the program.
Two measures of balance are evaluated at each NRN functional evaluation: the Modified Functional Reach (MFR) test and the Berg Balance Scale (BBS). The MFR evaluates seated balance and has been shown to be a reliable measure of seated balance function. 18,19 The validity and responsiveness of the MFR have yet to be explored in the SCI population, although the standard error of measurement and minimum detectable change of the MFR previously have been estimated. 19
In the NRN implementation of the MFR, the person is seated in a chair with feet supported and back against the back of the chair (10 degrees from vertical). The person raises his/her preferred shoulder to 90 degrees of shoulder flexion, or the acromion is used for point of reference if the person is unable to reach 90 degrees of shoulder flexion. Measurements are taken from a wall-mounted yardstick, to which the arm is held parallel. Two practice trials are allowed, followed by three scored trials. The final score is the maximum of the three scored trials.
The BBS was originally developed to determine fall risk in the elderly population, 20,21 but has since been used in other populations including persons with SCI, 9,14,22 –24 The reliability and validity of the BBS have been previously demonstrated, 25,26 but its responsiveness to activity-based rehabilitation in the SCI population has yet to be evaluated.
The BBS comprises 14 sitting and standing tasks, each of which tests the ability of individuals to maintain position while the limits of base of support are challenged. Each item is scored on a 5-point scale, and items are ordered with increasing level of difficulty. The highest score for each item requires the functional coordination of multiple systems of strength, flexibility, and balance. The summary score for the BBS is defined as the simple sum of the 14 item scores and ranges from 0–56. The summary score was originally interpreted relative to the threshold value 40—scores lower than 40 were indicative of a person at risk for falls. 20,21 The summary score itself has been used in SCI populations as an ordinal measure of balance function. 9,14,22 –24
Two tests of ambulatory function are conducted at NRN functional evaluations the Six Minute Walk Test (6MWT) and the 10 Meter Walk Test (10MWT). The 6MWT is used to measure walking endurance, and its reliability, validity, and responsiveness in the SCI population are well established. 27,28 The procedures for the 6MWT are thoroughly defined elsewhere, and we briefly describe their implementation in the NRN here. A straight path of no less than 100 ft is established with turns specifically placed throughout the path. The person is instructed to walk as far as he/she can in 6 min, and only standardized verbal feedback is permitted. Lower extremity bracing is not permitted, but persons can use an assistive walking device (walker, canes, crutches, etc.) The test ends when 6 min have passed or if the person receives physical assistance or has to sit and rest.
The 10MWT measures gait velocity and has well-established reliability, validity, and responsiveness in the SCI population. 27,28 In its NRN implementation, the person is instructed to walk as fast as possible along a 14 m path. The timing of the walk begins after a 2 m flying start and ends 10 m from the starting point (the 12 m point of the 14 m path) to adjust for acceleration and deceleration effects. As with the 6MWT, standardized verbal feedback is permitted, lower extremity bracing is prohibited, and assistive walking devices are allowed.
Data analysis
Baseline demographic and clinical characteristics were summarized with counts and percentages for categorical data, means and standard deviations for continuous data, and medians and ranges for skewed continuous data. While our data were longitudinal (873 longitudinally collected observations from 152 patients), our goals and hypotheses were largely marginal in scope. Therefore, we used statistical techniques for the marginal analysis of clustered data, of which longitudinal data are a type. The items of the NRS were explored with a marginal principal components analysis conducted via within-cluster resampling. 29 Loading coefficients from the primary principal components and percent variability explained were estimated as the within-cluster resampled averages over 10,000 Monte Carlo loops. Relationships between the NRS score, NRS Phase, NRS empirical subscale scores (BWST, HL, AS, HL+AS), and other continuous functional and clinical measurements were assessed by the calculation of marginal Pearson correlation coefficients for clustered data. 30
Mean NRS scores were compared among groups defined by AIS and neurological level through linear contrasts applied to linear mixed effects models with categorical covariates as fixed effects. The responsiveness of the NRS and other clinical and functional measures to LT were evaluated with the calculation of standardized response means (mean/standard deviation [SD]) of the enrollment and discharge measurements, both for the overall sample and within AIS levels. All analyses were conducted in the open-source R software environment (R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria.
Results
Demographic and clinical characteristics
Our sample was largely male with an average age of 36 years (Table 1). Times since injury were varied and ranged from 0.1–45.2 years. Most injuries were cervical, and there was representation from all AIS levels and the full range of UEMS and LEMS. Injuries were largely traumatic in nature. Enrollment characteristics, including enrollment duration, number of LT sessions received, and the number of functional evaluations conducted, varied widely. The majority of patients were nonambulatory at enrollment.
Values are mean (standard deviation) or median [min, max] for continuous variable and count (%) for categorical. AIS, American Spinal Injury Association (ASIA) Impairment Scale; SCI, spinal cord injury; UEMS, Upper Extremity Motor Score; LEMS, Lower Extremity Motor Score; LT, locomotor training.
Principal components analysis of the NRS
The marginal principal components analysis by within cluster resampling showed that the primary principal component accounted for 65% of the overall scale variability in the NRS, the second component accounted for 17%, while no other component contributed more than 4% of overall scale variability. The contributions of individual NRS items to the first principal component were variable, as exhibited by the loading coefficients that ranged from 0.14 for the Walking item to 0.41 for the Stand item (Table 2). The loading coefficients were all of the same sign indicating that the first principal component was a marker of general functional capacity that discriminated high- and low-functioning patients. The NRS Score, a simple sum of NRS items, correlated nearly perfectly (Pearson correlation = 0.999) with scores from the first principal component (a weighted sum of NRS items with weights given by the loading coefficients), indicating that the NRS Score was a reasonable surrogate for the primary component of variability in the NRS.
PC, principal component; NRS, Neuromuscular Recovery Scale.
The second principal component discriminated patients based on arm and shoulder function. Loading coefficients were large and positive for the newly introduced arm and shoulder items, and small and/or negative for all other items. Thus, patients with high arm and shoulder function but poor trunk and lower limb function would score highest on the second principal component. Patients functioning highly in all NRS items would exhibit lower second principal component scores, because the loading coefficients for the trunk and leg items (1 through 10) were negative. A simple sum of the three arm and shoulder items—the score for the AS subscale of the NRS—was positively correlated with scores from the second principal component (0.65, 95% confidence interval [CI] = [0.57, 0.72]).
NRS Score and NRS Phase
The NRS Score corresponded well with the NRS Phase (Fig. 1). The estimated marginal Pearson correlation between the NRS Score and NRS Phase was 0.90 (0.88, 0.92). Observed NRS Scores ranged from 23–151, nearly covering the available range of 12–156. The NRS Score exhibited substantial variability in NRS Phases 1B through 2C, with SDs of 11 and higher. The average NRS Score over all evaluations was 70 (SD = 31), and average NRS Score increased with NRS Phase. The higher NRS Phases were underutilized, because only 72 of 873 (8%) assessments of the NRS resulted in a NRS Phase of 3A or higher (Fig. 1).
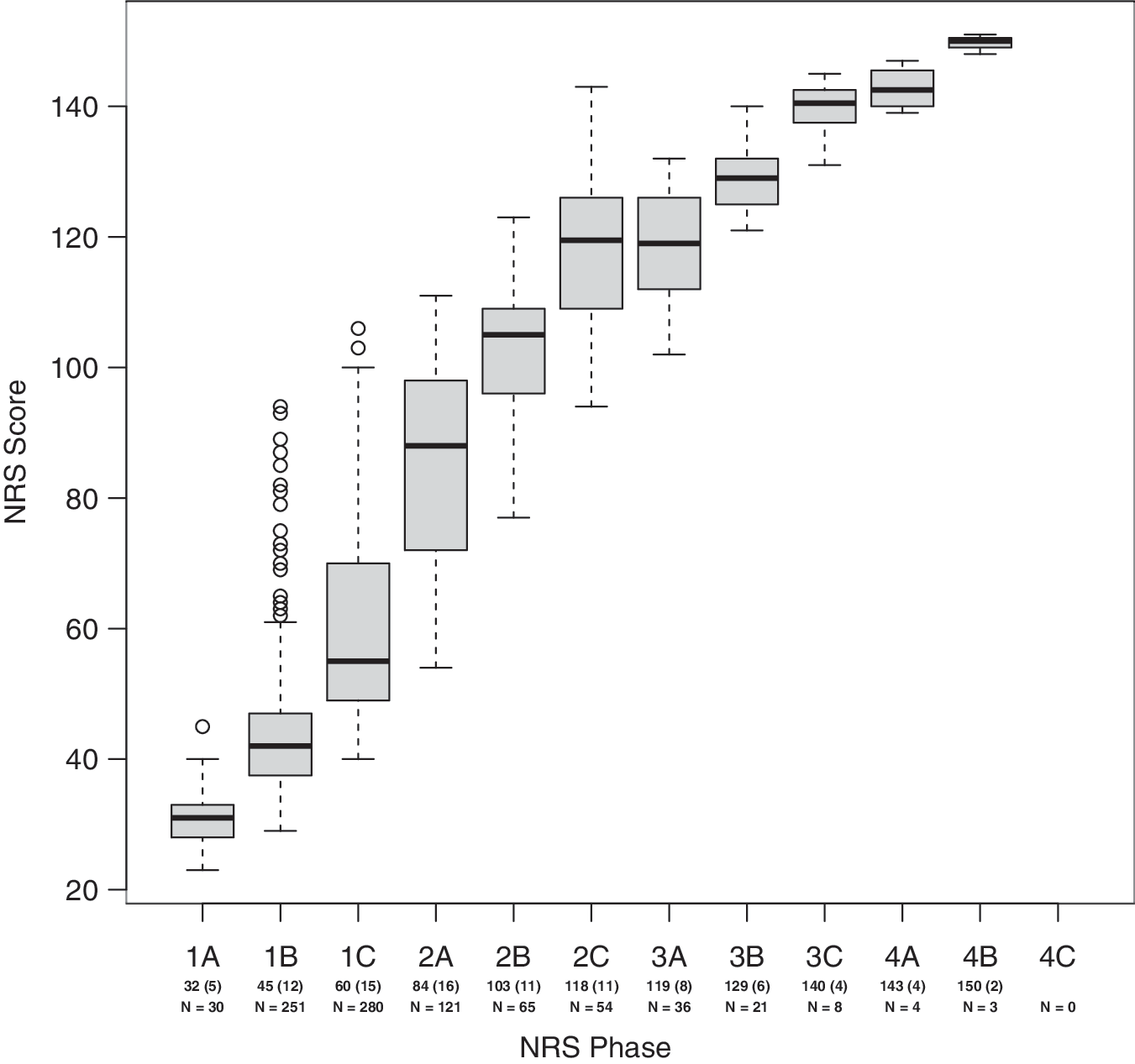
Boxplot of Neuromuscular Recovery Scale (NRS) Score by NRS Phase. Values underneath x-axis labels are mean (standard deviation) for NRS Scores within each NRS Phase and number of observations per NRS Phase level.
NRS Score and ISNCSCI examination data
Average NRS Scores increased with AIS level, with averages (95% CI) of 53 (49, 59) for AIS A patients, 55 (50, 61) for AIS B patients, 67 (63, 72) for AIS C patients, and 88 (83, 92) for AIS D patients. Average scores significantly differed among AIS levels (p < 0.001). Pairwise comparisons showed that average NRS Scores for AIS A and B patients were not significantly different (p = 0.54), while all other pairings (A vs. C and D, B vs. C and D, C vs. D) showed significant differences (p < 0.001). Average NRS scores (95% CI) were 68 (63, 73) for cervical patients and 71 (65, 76) for thoracic patients, and did not significantly differ (p = 0.24). Neurological level of injury, ranked according to position on the spinal cord, significantly but weakly correlated with the NRS Score (Fig. 2, top row; r = 0.18, 95% CI = [0.03, 0.34]).
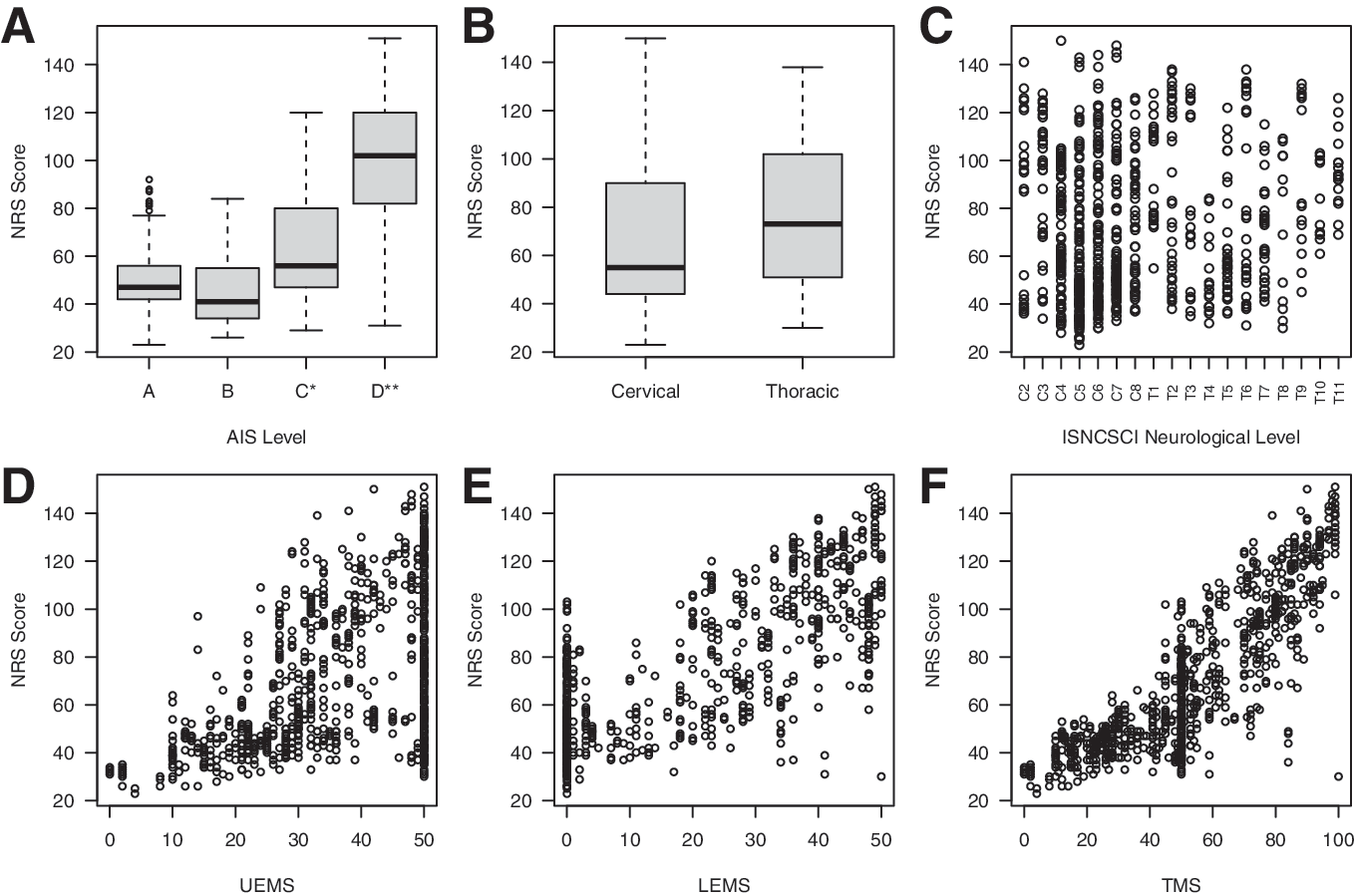
Neuromuscular Recovery Scale (NRS) Score against clinical measures from the International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI) examination. (
The NRS Score was weakly correlated with the ISNCSCI UEMS and strongly correlated with LEMS and TMS (Table 3, Fig. 2). Substantial variability in the NRS Score existed at the boundary values of the UEMS and LEMS (Fig. 2). NRS Scores varied from 23–103 among patients with LEMS of 0, and from 30–151 among patients with UEMS of 50. The NRS Score was uniformly more strongly correlated with the UEMS, LEMS, and TMS than the NRS Phase. Among the NRS Score and its empirical subscale scores, the AS Score was most strongly correlated with the UEMS, the TL Score was most strongly correlated with the LEMS, and the nontreadmill summary score (TL + AS) was most strongly correlated with the TMS.
NRS, Neuromuscular Recovery Scale; ISNCSCI, International Standards for the Neurological Classification of Spinal Cord Injury; BWST, Body-Weight Supported Treadmill; TL, Trunk & Leg; AS, Arm & Shoulder; UEMS, Upper Extremity Motor Score; LEMS, Lower Extremity Motor Score; TMS, Total Motor Score; MFR, Modified Functional Reach; BBS, Berg Balance Scale; 6MW, Minute Walk; 10MW, 10 Meter Walk.
Indicates largest within-row correlation.
Values are marginal Pearson correlation coefficients (95% confidence interval).
The NRS Score was substantially more responsive to LT than the UEMS, LEMS, and TMS, both overall and within groups defined by AIS (Table 4). The standardized response mean (SRM) for the NRS Score was 1.13 in the full sample and 1.03, 1.14, and 1.52 for AIS A/B, C, and D patients, respectively. Improvements in UEMS, LEMS, and TMS were incremental in absolute magnitude and substantially less in relative magnitude than the NRS Score. There was virtually no improvement in UEMS, LEMS, and TMS among AIS A and B patients, and only minimal improvement among AIS D patients. Each of UEMS, LEMS, and TMS exhibited improvement among AIS C patients, but to a much lesser extent than the NRS Score.
AIS, American Spinal Injury Association Impairment Scale; NRS, Neuromuscular Recovery Scale; UEMS, Upper Extremity Motor Score; LEMS, Lower Extremity Motor Score; TMS, Total Motor Score; MFR, Modified Functional Reach; BBS, Berg Balance Scale; 6MW, 6 Minute Walk; NA – SRM not available, because A/B patients were nonambulatory; 10MW, 10 Meter Walk.
Summary statistics are mean (standard deviation) or median [min, max] when data are skewed. Responsiveness statistics are standardized response means (SRM).
NRS Score and other functional measures
The NRS Score correlated strongly with speeds and distance from the two walk tests (6MWT, 10MWT) as well as the tests of standing (BBS) and seated balance (MFR). The NRS Score was more strongly correlated with the MFR and BBS than the NRS Phase (Table 3, Fig. 3) and as or nearly as correlated with the 6MW and 10MW. NRS Scores varied widely near the boundaries of other functional measures. Patients with BBS scores of 7 or lower exhibited NRS Scores ranging from 25–109, while nonambulatory patients exhibited NRS Scores ranging from 23–109 (Fig. 3). Among the full NRS Score and subscales scores, the NRS TL Score was generally most strongly correlated with the functional outcome measures, exhibiting correlations of 0.79 and higher.

Scatterplot of Neuromuscular Recovery Scale NRS Score (left column) and International Standards for the Neurological Classification of Spinal Cord Injury ISNCSCI Total Motor Score (TMS, right column) against Modified Functional Reach (in), Berg Balance Scale score, 6 Minute Walk distance (m), and 10 Meter Walk speed (m/s).
The BWST score was also strongly correlated with the walk tests. The full NRS Score exhibited lower correlations with the outcome measures than the TL and BWST subscale scores, but the differences in correlation were no greater than 0.05. The nontreadmill subscale score (TL + AS) exhibited correlations with functional measures that were in reasonable correspondence with correlations between the full NRS Score and the functional measures. The AS subscale score was statistically significantly but weakly correlated with the five measures of lower body function, exhibiting correlations not exceeding 0.43. Both the NRS Score and the NRS TL Score were more strongly correlated with functional measures than the UEMS, LEMS, and TMS, with the exception of the MFR (Table 3, Fig. 3). Among the ISNCSCI motor scores, the LEMS exhibited the strongest correlation with the functional outcome measures.
Each of the functional outcome measures responded positively on average to LT (Table 4). Because the large majority (77%) of our sample was nonambulatory and most remained nonambulatory, the summary statistics for the walk tests were largely reflective of the zero walk distances and speeds exhibited by nonambulatory patients. The relative magnitudes of change were substantially different among the measures and different within subgroups defined by AIS. The NRS Score was uniformly most responsive to LT, exhibiting SRM that substantially exceeded the SRM of all other functional measures. After the NRS Score, the MFR was generally most responsive overall and among AIS A/B and C patients. The 10MW test was most responsive among all other functional outcome measure among AIS D patients, a largely ambulatory group, although the NRS Score was far more responsive in this group (SRM = 1.52 vs. 0.98).
Discussion
Our results show that the NRS, with the addition of three items measuring AS function, the extension of the scoring rubric to full recovery, and the use of the new NRS Score, improves the estimation of neuromuscular recovery over the wide range of levels and severity of SCI, providing a more sensitive and comprehensive measure for use in the clinic and for research studies for functional recovery after SCI. The NRS Score showed greater sensitivity in measuring functional capacity as demonstrated by the substantial variability at the boundary values of other measures commonly used as end-points for SCI rehabilitation programs.
The NRS Score was more strongly correlated with other SCI functional measures than ISNCSCI motor scores and was the most responsive outcome measure to change brought on by LT, an activity-based therapy, in persons with chronic SCI. The expanded NRS appears to be a valuable and comprehensive tool in measuring functional recovery from SCI in that it can detect significant changes across varied levels and severities of injury.
Changes to the NRS—upper extremity tasks and the NRS Score
The three AS items added to the NRS exhibited two important features described by the results of the marginal principal components analysis. First, each item loaded onto the first marginal principal component along with the original 10 items, indicating that their contribution to measuring functional recovery was in line with contributions of the other 10 items. Second, the AS items were the primary contributors to a second principal component. The contribution of these items was largely to the exclusion of the other 10 NRS items, indicating that the second principal component was primarily related to AS function and that the addition of these three tasks to the NRS provided an additional domain of functional recovery captured by the NRS.
The definition of the NRS Score as the summary measure of overall recovery for the NRS was also justified by the results of our marginal principal components analysis. The first marginal principal component was dominant (65% variance accounted), included all 13 NRS items, and each NRS item contributed positively to the component, suggesting that scores derived from the first marginal principal component were indicative of overall recovery. The NRS Score was a good surrogate for scores generated from the first principal component, exhibiting near perfect correlation with first principal component scores.
The previous summary score for the NRS, the NRS Phase, was defined via a “lagging item” algorithm, in which the lowest scoring task of the NRS either defined the NRS Phase or was the benchmark from which the NRS Phase was defined. The lagging item algorithm for scoring the NRS Phase generally resulted in underutilization of higher subphase categories (3A and higher), while observed NRS Scores ranged over nearly the entire available range of values.
Further, while the NRS Score and NRS Phase were significantly correlated, there was substantial variability within the subphases defined by the NRS Phase, because the NRS Score exhibited ranges of nearly 70 in lower subphases (1B through 2B). This was in correspondence with previously published results for the NRS Phase, because other functional outcome measures were highly variable among Phase 2 individuals. 9 Finally, the NRS Score was uniformly more strongly correlated with existing measures of function than the NRS Phase, indicating that the NRS Score is likely a more suitable summary measure of function than the NRS Phase.
The NRS Score, with contributions from the newly added AS items, was fairly well related to clinical data from the ISNCSCI examination. NRS Scores were significantly different on average among AIS groups and well-correlated with the UEMS, LMS, and TMS. The NRS Score also exhibited strong correlations with other established functional measures of balance and walking capacity, providing an informal external validation of the NRS Score as a summary measure of function. The NRS Score was also more closely related to other measures of function than any of the UEMS, LEMS, and TMS.
The NRS score also mitigates the complex interaction of level and severity of injury that remains a limitation of using INSCSCI examination data such as the AIS classification, UEMS, LEMS, or TMS as recovery measures. This is shown by the wide ranges of NRS values within AIS classifications, levels of injury, and among UEMS, LEMS, and TMS (Fig. 2). For example, NRS Scores ranged from 23–103 among persons with LEMS of 0, and ranged from 30–151 among persons with UEMS of 50. This indicates that the NRS may be more sensitive to overall recovery than other available outcome measures.
NRS as a sensitive, responsive, and flexible measure of recovery from SCI
While the NRS Score was closely related to other measures of functional capacity, the substantial variability it exhibited at or near the boundaries of other measures indicated that the NRS Score may be a more sensitive marker of recovery representing functional differences in patients that are not detected by other functional measures. For example, nonambulatory individuals all have walk speeds of zero, but varied greatly in other domains of functional capability such as balance and upper extremity function. The fact that NRS Scores among nonambulatory persons ranged from 23–109 demonstrates that the NRS Score measures aspects of function not captured by the walk tests (as well as other functional outcome measures).
The NRS Score was clearly the most responsive to LT among all outcome measures we considered, not only for the SCI population in general but also within subgroups defined by injury severity (AIS A/B, C, and D). In fact, the NRS Score was substantially more responsive than measures that would be expected to perform well in specific AIS subgroups. In particular, the NRS Score was more sensitive than balance measures and motor scores among persons with AIS A, B, and C injuries, and was more sensitive than walking measures among AIS D patients, a typically ambulatory population. This provides evidence that the NRS may be an optimal general purpose measure of function useful in studies of persons with SCI and in the clinic, regardless of the individual characteristics (i.e., severity or level) of the injury.
When NRS items were grouped empirically as BWST, TL, and AS and summary scores generated for each, we found that TL scores most closely correlated with existing measures of ambulatory and balance function—i.e., lower extremity function. Correlations between the TL subscore and the other functional measures, however, were not substantially greater than the correlations we observed with the full NRS score.
This result was important in two ways. First, the addition of AS items to the existing lower limb, trunk, and BWST items did not substantially diminish the NRS and its relationships with walking and balance outcome measures. Second, the practicality of the NRS as an outcome measure is in part hampered by the fact that the BWST items require equipment not available to all clinicians. We have provided evidence that the TL and nontreadmill (TL + AS) scores alone are also closely related to existing measures of function, and that either of these subscores can be used as a surrogate NRS Score for clinicians lacking access to BWST systems. When providing LT, however, the BWST items do become important in delivery of the intervention.
Limitations
The analyses we have conducted do not represent a formal psychometric evaluation of the properties of the updated NRS. In particular, the added AS items will require reliability testing and an assessment of the validity of the NRS more formal than a principal components analysis. The responsiveness statistics we have presented are unadjusted for other factors that may account for recovery. The NRN is a diverse SCI population, and there may be other sources of variation left unexplained by our basic analyses of responsiveness. Further analyses evaluating the responsiveness of the NRS are needed. A more advanced examination of these properties of the updated NRS is in progress currently.
Conclusions
Paralysis after SCI results in complex neuromuscular presentations because of wide ranges of severity, level of injury, and available activity-dependent rehabilitation. ISNCSCI motor scores, the most often used primary outcome measure, is limited in capturing these complexities of paralysis and may contribute to the inability of recent clinical trials to demonstrate efficacy even with robust scientific and pre-clinical data. The NRS may overcome many of these limitations because it spans the entirety of severity and focuses on functional tasks. The NSR also may be particularly relevant as other activity-based therapies or combined interventions that target plasticity and recovery are tested and translated into clinical practice, because it provides an improved mechanism to test the efficacy and effectiveness of these interventions.
Footnotes
Acknowledgments
The authors thank the Christopher and Dana Reeve Foundation and all current and past members of the NeuroRecovery Network (NRN). For a list of all NRN team members, please visit:
This work was in part supported by the Centers for Disease Control and Prevention and the Christopher and Dana Reeve Foundation (grant/cooperative agreement U10/CCU220379). This project was supported, in part by grant number 90PR3002, from the U.S. Administration for Community Living, Department of Health and Human Services, Washington, D.C. 20201.
Grantees undertaking projects under government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not, therefore, necessarily represent official Administration for Community Living policy.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.