
Abstract
As spinal cord injury (SCI) trials begin to involve subjects with acute cervical SCI, establishing the property of an upper limb outcome measure to detect change over time is critical for its usefulness in clinical trials. The objectives of this study were to define responsiveness, sensitivity, and minimally detectable difference (MDD) of the Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP). An observational, longitudinal study was conducted. International Standards of Neurological Classification of SCI (ISNCSCI), GRASSP, Capabilities of Upper Extremity Questionnaire (CUE-Q), and Spinal Cord Independence Measure (SCIM) were administered 0–10 days, 1, 3, 6, and 12 months post-injury. Standardized Response Means (SRM) for GRASSP and ISNCSCI measures were calculated. Longitudinal construct validity was calculated using Pearson correlation coefficients. Smallest real difference for all subtests was calculated to define the MDD values for all GRASSP subtests. Longitudinal construct validity demonstrated GRASSP and all external measures to be responsive to neurological change for 1 year post-injury. SRM values for the GRASSP subtests ranged from 0.25 to 0.85 units greater than that for ISNCSCI strength and sensation, SCIM-SS, and CUE-Q. MDD values for GRASSP subtests ranged from 2–5 points. GRASSP demonstrates good responsiveness and excellent sensitivity that is superior to ISNCSCI and SCIM III. MDD values are useful in the evaluation of interventions in both clinical and research settings. The responsiveness and sensitivity of GRASSP make it a valuable condition-specific measure in tetraplegia, where changes in upper limb neurological and functional outcomes are essential for evaluating the efficacy of interventions.
Introduction
A
Interventions must induce and demonstrate clinically relevant change in the a priori determined outcome of interest to be deemed efficacious. 4 To accomplish this, outcome measures should be valid and reliable at a single time point in addition to being able to capture changes over time in the intervention versus control groups. This quality domain is referred to as either “sensitivity to change” or “responsiveness.” 7 Minimally detectable difference (MDD) is the difference in a score needed to detect a true clinical change, which is outside of error. The smallest real difference (SRD) calculation is used to define the MDD. 8 These measurement quality domains have important implications for clinical trial design and end-point calculations. Thus, the quality of responsiveness can dictate which measures are useful in the design of a trial. Further, sensitivity helps define which measures are most useful in defining differences between treatment groups. 5,6
An increasingly important factor for SCI trials is that reliable, valid, and responsive outcome measures reduce the sample size needed to demonstrate change. Thus, well-designed and rigorously studied measures can facilitate the success of future SCI trials.
The Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP) was developed as a measure of upper limb impairment specific for traumatic tetraplegia. 9 The five subtests included in the GRASSP are strength, dorsal sensation, palmar sensation, prehension ability, and prehension performance. The quality domains of reliability and validity have been established in a previous cross-sectional study. 10
A multinational, longitudinal study has been conducted to establish the responsiveness of the GRASSP. In this study, we report results on the sample studied in Canada. The general responsiveness has been established in a European cohort. 11 The objective of this study was (1) to define the responsiveness of each GRASSP subtest starting from as early as 10 days post-injury, (2) to determine the minimally detectable difference for each GRASSP subtest, and (3) to confirm that results obtained from the European study remain valid when compared with a Canadian sample. 11
Methods
Study design
A multicenter, observational, longitudinal, cohort study was conducted in Ontario, Canada, which included five centers (seven sites) (Table 1). Ethics board approval was obtained at all sites. Enrollment and follow-up data collection took place between 2009 and 2013. Patients were included if they sustained a traumatic cervical SCI and presented with a minimum motor grade of 1 in the C5 myotome on either the right or left side, or both; were graded as A, B, C, or D on the American Spinal Injury Association Impairment Scale (AIS); were between the ages of 16 and 75; and were able to provide informed consent. Patients were excluded if they had any additional cause of upper limb neurological impairment and/or a moderate to severe brain injury precluding their ability to participate in the assessment battery. To ensure adequate power, a sample size of convenience and feasibility was set at 60 study participants.
AIS, American Spinal Injury Association Impairment Scale; SD, standard deviation; ON, Ontario.
First, it was hypothesized a priori that all GRASSP subtests would be responsive to change across the 1-year time course. Further, the standardized response means (SRM) for the GRASSP strength and sensation subtests were expected to be at least 0.25 units greater than that for the International Standards of Neurological Classification of Spinal Cord Injury (ISNCSCI) upper extremity motor score (UEMS), and ISNCSCI Light Touch Score (ISNCSCI-LT).
Pearson correlation coefficients calculating longitudinal concurrent validity would be used to confirm responsiveness against the measures of change (UEMS, ISNCSCI-LT, Capabilities of Upper Extremity Questionnaire [CUE-Q], Spinal Cord Independence Measure-Self-Care Subscore [SCIM-SS]) with ideal correlations greater than 0.60, at 3 months post-injury and beyond. Second, the GRASSP prehension subscores were expected to have an SRM greater by at least 0.25 units than the SCIM-SS and CUE-Q, allowing it to show a larger effect size in the same sample.
External measures of change
Selection of external measures of change for comparison was based on their use in the field of SCI and/or their established psychometric qualities. GRASSP consists of five subtests for each hand. The subtests scored and discussed in this manuscript are: GRASSP Strength (GR-st), GRASSP Dorsal Sensation (GR-dsen), GRASSP Palmar Sensation (GR-psen), GRASSP Prehension Ability (GR-pa), and GRASSP Prehension Performance (GR-pp). Although GRASSP subtest scores are intended to be applied unilaterally, both right- and left-sided scores were added for this analysis. 9,10
The ISNCSCI provides a sensory and motor level based on the most normal caudal spinal cord level represented by the dermatomes and myotomes tested. The 2003 version of the ISNCSCI was administered. 12 The ISNCSCI was selected for use in the study to define the sample according to an accepted SCI classification method and to define the severity of injury for persons involved in the study. Interrater reliability of ISNCSCI motor and sensory testing has been confirmed to be greater than 0.80 where standardized training has been provided. 12
The SCIM-III is a global measure of function specifically tailored for persons with SCI 13 and was used to define the function and independence of patients in this study. Interrater reliability of the total SCIM-III score is 0.94, and its concurrent validity with the Functional Independence Measure used for other populations in addition to SCI is 0.79. 13 The SCIM total and self-care subscale (SCIM-SS) were used as comparator scores. The SCIM-SS includes items specific to upper limb use and was, therefore, ideal for comparisons with GRASSP subtests. The SCIM subscales are reliable and useful quantitative representations of the specific independence constructs in SCI. 13
CUE-Q is a 32-item questionnaire developed to assess difficulty in performing certain activities with the upper extremities. The CUE-Q was selected as a measure to establish the relationship between impairment and self-perceived upper limb function. Psychometric properties of the CUE-Q have been reported as 0.92 for test-retest reliability and 0.74 for concurrent validity with the Functional Independence Measure. 14
Timing of data collection
Serial testing of study participants was conducted. ISNCSCI and partial GRASSP were administered at 0–10 days (baseline). ISNCSCI, complete GRASSP, CUE-Q, and SCIM were administered at 1, 3, 6, and 12 months post-injury. All assessments were performed by physical therapists or occupational therapists trained to carry out the aforementioned measures. All trained examiners attended and participated in standardized study-related training by one of the lead investigators.
Data analysis
Descriptive statistics were used to analyze the demographic data and all score totals at each time point. Pearson correlation coefficients were calculated at baseline, -month, 3 months, 6 months, and 12 months for the GRASSP subtest scores versus the CUE-Q and SCIM-SS. The strength of association was classified as follows: mild (0.3–0.59), moderate (0.6–0.79), and strong (0.8–1.00). 5 SRMs 4 were calculated for 10 pairs of scores at different time intervals (baseline to 1, 3, 6, 12 months; 1 month to 3, 6, 12 months; 3 months to 6, 12 months; 6 months to 12 months) for ISNCSCI-UEMS, ISNCSCI-LT, GR-st, GR-sen, and GR-pa scores.
SRMs were calculated for six pairs of scores at different time intervals (1 month to 3, 6, 12 months; 3 months to 6, 12 months; 6 months to 12 months) for ISNCSCI-UEMS, ISNCSCI-LT, GRASSP st, GR-dsen, GR-psen, GR-pa, GR-pp, SCIM-SS, and CUE-Q scores. MDD was calculated for each GRASSP subtest score using the SRD method (SRD, 1.96 × √2 ×SEM) from Beckerman and associates. 8 All analyses were conducted using SPSS Version 21.0 (International Business Machines Corp., Boston, Mass)
Results
Sample
Fifty-nine study participants were enrolled. Fifty-three persons had more than one assessment available and thus were eligible to be included in the analysis. Of these 53 participants, at baseline 11 were AIS-A, 5 were AIS-B, 16 were AIS-C, and 21 were AIS-D. Data available for analysis included 46 sets for baseline assessment, 51 sets at 1 month, 38 at 3 months, 43 at 6 months, and 38 at 12 months. Analysis was conducted for the total sample and two subgroups of the total sample (group 1, AIS A and B; group 2, AIS C and D). The sample was stratified on the basis of initial baseline presentation as having either a motor complete (AIS-AB) or motor incomplete (AIS-CD) SCI. General demographics, sample characteristics, and sample contribution per site can be viewed in Table 1. Recovery profiles of this sample have been published previously. 3
Longitudinal validity
Table 2 shows the Pearson correlation coefficients between the GRASSP subtest scores and the measures of change at the 1-, 3-, 6-, and 12-month time points for the whole sample. A correlation coefficient greater than 0.60 is indicative of a moderately strong, positive relationship between the measures of change and GRASSP scores longitudinally. The correlation matrix shows that the GRASSP subtest scores demonstrate moderately strong correlations with the UEMS, SCIM-SS, and CUE-Q across a 1-year time course starting as early as 1 month post-injury. All GRASSP subtests are found to be responsive (able to detect change over time). The magnitude of change remains to be defined, however.
All values are significant with a p value of 0.001.
UEMS, Upper Extremity Motor Score; GR-st, Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP) Strength; GR-sen, GRASSP Sensation; ISNCSCI-LT, International Standards of Neurological Classification of Spinal Cord Injury Light Touch Score; SCIM-SS – Spinal Cord Independence Measure-Self-Care Subscore; CUE-Q, Capabilities of Upper Extremity Questionnaire; GR-pa, GRASSP prehension ability; GR-pp, GRASSP prehension performance.
Responsiveness and sensitivity
Mean differences, standard deviations, and SRM values for all 10 pairs of data can be viewed in Table 3. The sample data are presented as a whole and subgrouped into motor complete and motor incomplete SCI (AB and CD). Figure 1 illustrates the responsiveness of the GRASSP subtests in comparison with the previously described measures of change. The magnitude of the SRM value is also used to determine the sensitivity of each measure when comparing the GRASSP to the measures of change. A greater SRM value indicates greater sensitivity.
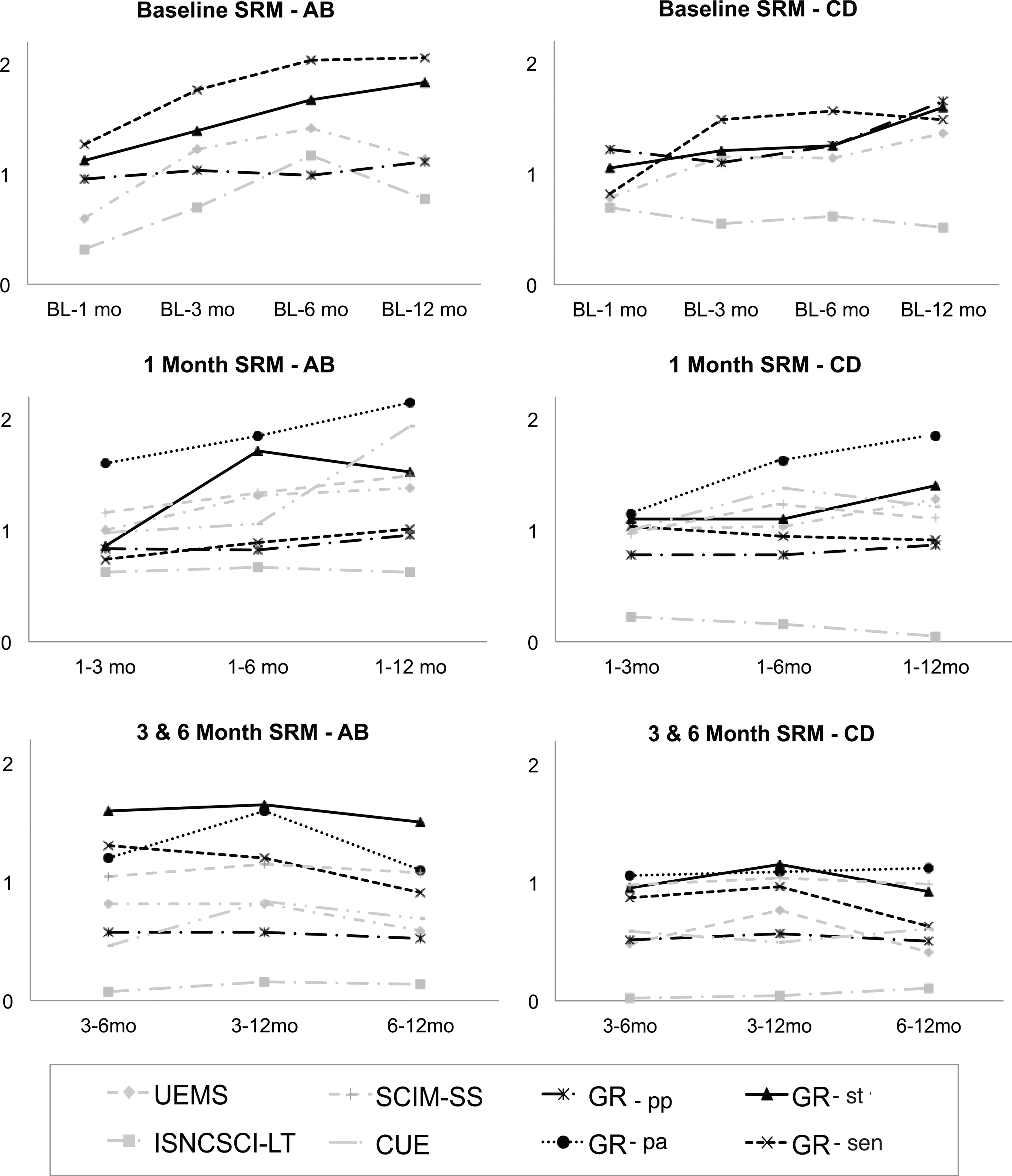
The responsiveness of Graded Redefined Assessment of Strength, Sensibility, and Prehension (GR) subtests—prehension ability, (pa) strength (st), prehension performance (pp), sensation (sen), black graph lines—compared with the measures of change—Upper Extremity Motor Score (UEMS), International Standards of Neurological Classification of Spinal Cord Injury Light Touch Score (ISNCSCI-LT), Capabilities of Upper Extremity (CUE), Spinal Cord Independence Measure-Self-Care Subscore (SCIM-SS), grey graph lines—through incremental time intervals during post-SCI recovery. The y-axis denotes the magnitude of the SRM (standardized response mean), which is used to determine the sensitivity of each measure with a greater value indicating greater sensitivity. Each graph title denotes the starting time point as well as the severity of SCI classified by the American Spinal Injury Association Impairment Scale (AB, motor complete, CD, motor incomplete). The x-axis denotes the specific time intervals of interest in terms of months after SCI.
mo, month; ISNCSCI, International Standards of Neurological Classification of Spinal Cord Injury; UEMS, Upper Extremity Motor Score; BL, baseline; ISNCSCI-LT, Light Touch Score; GR, Graded Redefined Assessment of Strength, Sensibility, and Prehension (GRASSP); GR-st, GRASSP strength; GR-sen, GRASSP sensation; GR-pa, GRASSP prehension ability; GR-pp, GRASSP prehension performance; SCIM-SS, Spinal Cord Independence Measure-Self-Care Subscore; CUE-Q, Capabilities of Upper Extremity Questionnaire;.
MDD calculations for each GRASSP subtest are presented in Table 4. The MDD for both unilateral and bilateral scores of each subtest have been calculated separately.
SEM, standard error of measure; SRD, smallest real difference.
Discussion
This study demonstrates that the GRASSP subtests are responsive and more sensitive than the current gold standard post-tetraplegia upper limb assessments including the ISNCSCI, SCIM III, and CUE-Q in terms of detecting neurological change. It should be noted that the ISNCSCI-LT scores appear to be neither responsive nor reflective of change that occurs over a 1-year time course after SCI. Therefore, the ISNCSCI-LT scores failed to meet the appropriate sensitivity threshold to be used as a measure of change.
Responsiveness
Longitudinal construct validity demonstrated in this sample supports the hypothesis that the GRASSP is responsive to change across the 1-year post-injury time frame. The measures of change selected for comparison in this study were the ISNCSCI, SCIM III, and CUE-Q. Associations between the GRASSP and both impairment and functional measures of change remained moderate to high throughout the recovery period. All measures, including the GRASSP, were responsive to change in the neurological and functional status of the upper limb. This analysis confirms that all selected measures, including the GRASSP, are capable of capturing change over time. The magnitude of change detected by each tool, however, does differ and is defined by the SRM values.
Sensitivity
SRM values were calculated to determine the sensitivity of the scales. The SRM values for each measure were compared with a priori expectations for directionality and magnitude. A larger SRM value indicates greater sensitivity. Differences in the SRM values between the measures were used to determine the sensitivity of the GRASSP subtests and for comparisons against the measures of change. All GRASSP subtests were found to be more sensitive than the comparison measures of change. The GR-st and GR-sen subscales were more sensitive than the ISNCSCI-UEMS and ISNCSCI-LT scales by at least 0.25 units across the 1-year time course.
SRM values were calculated for the whole sample and for both the motor complete and motor incomplete groups separately. These values show a few trends. First, impairment measures for the motor complete group show larger changes than the motor incomplete group across the 1-year time course. In addition, functional measures for the motor incomplete group show larger changes than the sensory incomplete group across the 1-year time course. These findings are consistent with the recovery profiles of the sample when stratified by AIS classification. 9
The motor complete group presents with greater impairment at baseline and shows greater improvements in impairment. The motor incomplete group, however, presents with less impairment at baseline and makes significant functional gains early in the recovery process. The functional gains made by the motor incomplete group during the early part of the 1-year post-injury window are greater than the functional gains made by the motor complete group over the entire year.
The sensitivity of an outcome measure is affected by structural parameters such as the type of scale, the scoring system, and the number of items that either affect signal or noise. 5 A larger number of items tends to improve sensitivity as long as items are not redundant or irrelevant to the disease in question. 4 The increased sensitivity of the GRASSP when compared with more traditional measures, such as the ISNCSCI, provides an opportunity to better differentiate patients in a highly variable cervical SCI population and subsequently use this information in a clinical and scientific capacity. Further, the SRM values established in this study can effectively elucidate the details and recovery profiles of specific disease severities.
The use of multiple assessment measures enhances clinicians' ability to adequately comprehend the spatial and temporal elements of the upper limb recovery profile. Therefore, defining changes in impairment and function for specific subgroups of this highly heterogeneous population becomes feasible.
The MDD was calculated for each subtest of the GRASSP both unilaterally and bilaterally. The MDD is the minimum amount of change in a patient's score that signifies that the change is not the result of measurement error (with 95% certainty). These values are useful for clinicians when administering the GRASSP to determine whether an observed change is a true clinical change or whether it may be attributed to chance.
The MDD values for each of the GRASSP subtests are quite low and far lower than the average amount of change noted over the 1-year time course. This indicates that true clinical change is effortlessly detectable with the GRASSP. The other setting in which the MDD is useful is test selection for less impaired patients. For example, if a patient scores 45 on GR-st unilaterally, a further change of greater than 5 points would be required to confirm a true clinical change in strength. In this case, an alternative GRASSP subtest might be preferentially selected because the GR-st score might not provide the desired sensitivity.
The previous GRASSP responsiveness study completed in Europe yielded similar findings in which GRASSP was found to be more sensitive than the ISNCSCI and SCIM III. 10 This previous study did not define the sensitivity of the GRASSP to detecting change in the first 6 weeks post-injury. Findings from both this and the previous study, however, have demonstrated that the GRASSP is responsive and sensitive in the initial post-injury window as well as throughout the recovery period up to at least 1 year.
Both studies are consistent, with a similar outcome. As such, it is clear that the GRASSP has the potential to provide the field of SCI with a novel tool that demonstrates excellent responsiveness in its ability to detect subtle changes in strength, sensation, and prehension related to injury severity.
Limitations
Development of the GRASSP outcome measure was prompted by the current gaps in upper limb assessment for traumatic tetraplegia. A general concept incorporated into the development of the GRASSP was to enhance the sensitivity of a potential upper limb testing battery. Thus, the elements selected for inclusion in the GRASSP Version 1.0 were deliberately selected for this purpose. The findings of this study confirm that the selected added elements have enhanced our ability to assess the upper limb with greater sensitivity.
This tool has been designed to assess a very specific group of persons with traumatic tetraplegia, with a focus on impairment rather than function or quality of life. The GRASSP has been specifically designed for persons with traumatic cervical SCI from the early acute phase through to the chronic phase. Its applicability in other conditions that may cause upper limb disability remains to be established. GRASSP is also a tool that can only be appropriately applied by or in the presence of an experienced assessor and may therefore not be a measure that can be readily used remotely.
Sensitivity and responsiveness of a measure do not address the relevance of change with regard to reported function and quality of life, but rather define a psychometric property of a tool, which was the focus of our work. We do not report on the clinical relevance of the detected change as it relates to function, but rather we focus on the intrinsic capabilities of the GRASSP to detect and quantify change.
Conclusion
The aim of this study was to report on the responsiveness, sensitivity, and MDD of the GRASSP Version 1.0. GRASSP is responsive to change that occurs as early as 10 days post-injury through to at least 1 year post-injury. The GR-st and GR-sen subtests are more sensitive than the ISNCSCI UEMS and ISNCSCI-LT scores. The GR-pp subtest is more sensitive than the CUE-Q and SCIM-SS. The purpose of developing the GRASSP was to enhance the repertoire of upper limb assessments available for SCI. Development of the GRASSP and establishment of its associated psychometric properties have provided the field with a robust outcome measure that is sensitive to changes in the upper limb post-injury.
This study indicates that the GRASSP is more sensitive to change than existing measures and is specific for changes in the upper limb of traumatic tetraplegia patients, making it an appropriate measure for the study of cervical SCI. The GRASSP is an appropriate and well-designed outcome measure specific for tetraplegia, which should be used as an adjuvant measure in studies that utilize neurological and functional change in the upper limb as an end-point.
Footnotes
Acknowledgment
The authors would like to acknowledge the funding agencies Craig Neilsen Foundation, Canadian Institutes for Health Research, Ontario Neurotrauma Foundation, and Rick Hansen Institute. We would also like to acknowledge support for Dr. Fehlings from the Gerald and Tootsie Halbert Chair in Neural Repair and Regeneration, the DeZwirek Family Foundation and the Sherman Clinical Trials Unit.
Author Disclosure Statement
Kalsi-Ryan, Fehlings, Curt, and Verrier as part of the International Design Team receive royalties from GRASSP sales. Kalsi-Ryan owns Neural Outcomes Consulting, Inc., manufacturer of the GRASSP.