
Abstract
Health-related quality of life (HRQOL) is an emerging method to quantify the consequences of pediatric mild traumatic brain injury (mTBI)/concussion in both clinical practice and research. However, to utilize HRQOL measurements to their full potential in the context of mTBI/concussion recovery, a better understanding of the typical course of HRQOL after these injuries is needed. The objective of this study was to summarize current knowledge on HRQOL after pediatric mTBI/concussion and identify areas in need of further research. The following databases from their earliest date of coverage through June 1, 2015 were used: MEDLINE®, PubMed, Embase, Scopus, Cumulative Index to Nursing and Allied Health Literature (CINAHL), SPORTDiscus, Cochrane Central Register of Controlled Trials (CENTRAL), Physiotherapy Evidence Database (PEDro), and Child Development and Adolescent Studies (CDAS). Studies must have examined and reported HRQOL in a pediatric population after mTBI/concussion, using a validated HRQOL measurement tool. Eight of 1660 records identified ultimately met inclusion criteria. Comprehensive data were extracted and checked by a second reviewer for accuracy and completeness. There appears to be a small but important subgroup of patients who experience poor HRQOL outcomes up to a year or longer post-injury. Potential predictors of poor HRQOL include older age, lower socioeconomic status, or a history of headaches or trouble sleeping.
Differing definitions of mTBI precluded meta-analysis. HRQOL represents an important outcome measure in mTBI/concussion clinical practice and research. The evidence shows that a small but important proportion of patients have diminished HRQOL up to a year or longer post-injury. Further study on this topic is warranted to determine the typical longitudinal progression of HRQOL after pediatric concussion.
Introduction
Concussion and mild traumatic brain injury
C
Clinical manifestations of concussion/mTBI in pediatric patients are highly variable and include physical, cognitive, sleep, and mood-related symptoms. 5,6 With conservative management and adequate levels of physical and cognitive rest, ∼80–90% of concussed adults will experience neurological recovery within 7–10 days; 3 however, children and adolescents may take longer to recover. 3,7 –9 Some patients will experience persistent symptoms lasting >1–3 months, and will be diagnosed with post-concussion syndrome (PCS). 10 Studies suggest that patients with PCS are at an elevated risk of developing further impairments in physical, psychological, and social functioning including chronic headaches, vestibular dysfunction, aerobic deconditioning, mood disorders, social isolation, and poor academic performance. 11 –13
Defining health-related quality of life (HRQOL)
HRQOL is a multi-disciplinary concept that captures the effect of disease states on a patient's physical, mental, and social well-being, and has emerged as an important patient-reported outcome (PRO). 14,15 Although quality of life and HRQOL are often used interchangeably, HRQOL refers specifically to aspects of life that are directly affected by one's health. 14,15
Measuring HRQOL
Assessment of HRQOL is applicable both to acute and chronic conditions. HRQOL questionnaires can be completed by the patient or by a proxy. HRQOL tools may be generic (i.e., applied to any disease or condition) or disease specific. Generic HRQOL instruments allow for the comparison of HRQOL across multiple, unrelated diseases. Examples of generic HRQOL instruments previously used in pediatric mTBI/concussion include the Pediatric Quality of Life Inventory (PedsQL), 16 the KINDL, 17 and the Child Health Questionnaire (CHQ). 18 Presently, there are no pediatric mTBI/concussion-specific HRQOL instruments available.
It may not be possible for patients to report their own HRQOL; therefore, a proxy, usually a parent or caregiver, may have to complete the assessment. Research demonstrates that children as young as 5 years of age can reliability assess their HRQOL, whereas parents can provide proxy assessments of HRQOL in children as young as 2 years of age with appropriate instruments. 15 A systematic review of pediatric HRQOL studies concluded that while good agreement was observed among pediatric patients and parents for physical HRQOL domains (such as symptoms), agreement was poor for social and emotional HRQOL domains. 19 As such, the authors recommend that both patient and parental assessments of HRQOL should be obtained whenever feasible. 19
HRQOL in pediatric concussion/mTBI
Despite accumulating evidence of impaired HRQOL among children and adolescents following any TBI, 20 there is limited understanding of HRQOL in pediatric patients with mTBI/concussion or PCS specifically. With an increase in the incidence of diagnosed mTBI/concussion 21 and greater understanding of the potential long-term effects of mTBI/concussion, 22 the field has seen an explosion of new research in recent years, and frequent knowledge synthesis efforts are needed to allow researchers and clinicians to stay up to date. Therefore, the objectives of the current study are to present an overview of HRQOL concepts and assessment and to conduct a systematic review of the available studies examining HRQOL in pediatric acute concussion/mTBI and PCS patients.
Methods
Literature search
A systematic search of the literature was performed by a professional health sciences librarian across the following nine databases from their earliest date of coverage through June 1, 2015: MEDLINE®, PubMed, Embase (Ovid), Scopus, Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO), SPORTDiscus (EBSCO), Cochrane Central Register of Controlled Trials (CENTRAL), Physiotherapy Evidence Database (PEDro), and Child Development and Adolescent Studies (CDAS) (EBSCO). Although specific searches varied in keeping with the options available within each database, a combination of controlled vocabulary and key word queries were used whenever possible. Subject headings included:
Inclusion criteria
The following a priori determined inclusion criteria were applied to each potentially relevant study by two reviewers independently. 1) Must have examined and reported the effects of isolated physician-diagnosed concussion or mTBI in a pediatric/adolescent population (< 20 years old). 2) Must have measured two or more HRQOL domains (e.g., physical, cognitive, social, emotional) in the patient after concussion/mTBI using a validated HRQOL measurement tool. The HRQOL scales could have been completed by the patient, the patient's proxy, or both. 3) Must be primary research, excluding case reports, published in a peer-reviewed academic journal or in gray literature (e.g., PhD dissertation). 4) Must be available in English. Studies that did not report results specific to mTBI were excluded.
Studies that met all four inclusion criteria were included. All discrepancies between reviewers were resolved through consensus or by a third reviewer as needed. The reference lists of included studies were reviewed for any additional potentially relevant studies.
Data extraction and assessment of methodological quality
Study data were extracted using a standardized form focusing on study design, study inclusion/exclusion criteria, recruitment method, sample size, participant characteristics, setting (inpatient versus outpatient), mTBI/concussion diagnostic criteria, cause of injury (e.g., sports, motor vehicle, falls), HRQOL measurement tool, time points that HRQOL was assessed, patient versus proxy report, control groups (i.e., baseline, uninjured, non-brain injured), predictors of HRQOL, statistical methods, results, conclusions, study funding, and methodological quality/risk of bias, using the Scottish Intercollegiate Guidelines. 23 A second independent reviewer then verified data extraction forms for accuracy and completeness.
Data analysis
Substantial heterogeneity in timing of HRQOL measurements, HRQOL tools, proxy versus child reporting, and definitions of mTBI/concussion precluded performing a meta-analysis. A descriptive analysis was performed, and the results were summarized narratively.
Results
The search results are outlined in Figure 1. Eight manuscripts, representing five unique studies were included (Table 1). One study was identified as a PhD dissertation and as two journal articles (with one reporting additional time points). 25 –27 Two of the studies were also conducted among the same group of patients, with different data analyses performed in each. 28,29 Reviewing the reference lists of the included manuscripts did not yield any additional studies.
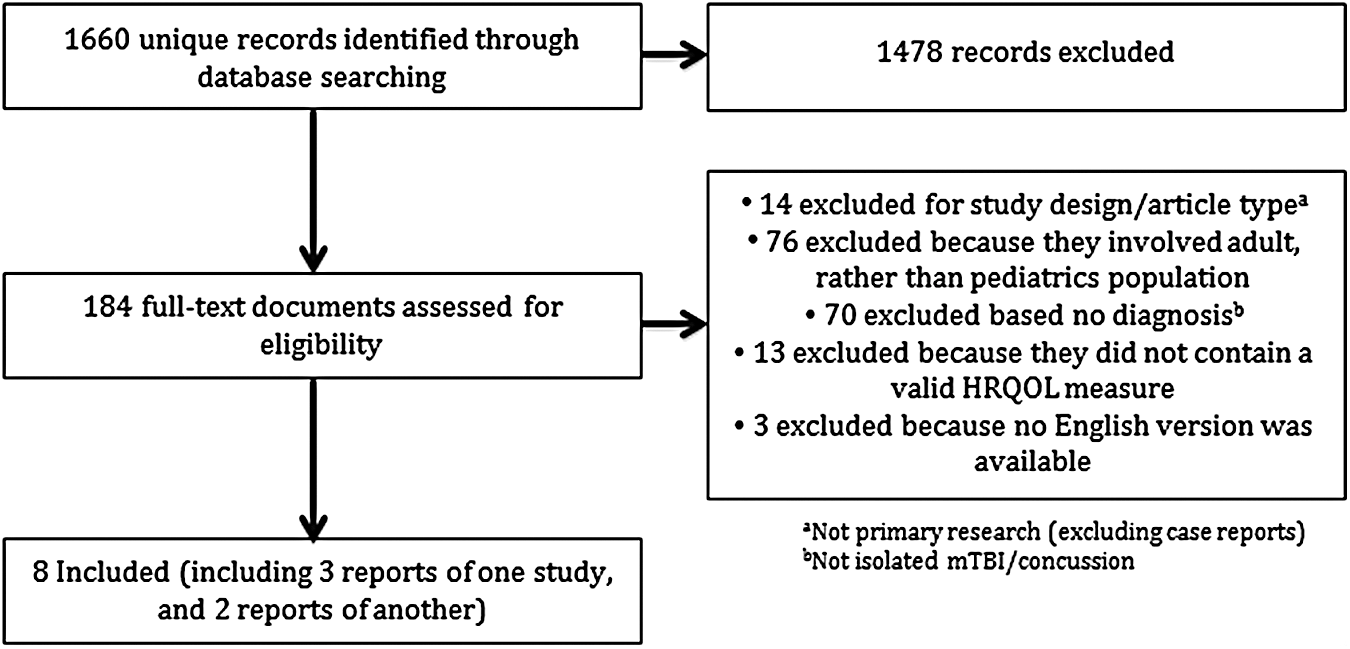
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram outlining the search process and results.
mTBI, mild traumatic brain injury; HRQOL, health-related quality of life; ICD, International Classification of Diseases; GCS, Glasgow Coma Scale; PedsQL, Pediatric Quality of Life Inventory.
Description of included studies
The studies were published between 2008 and 2014. Three were completed in the United States, 25 –30 one in Germany, 31 and one in Australia. 32 Ages of participants ranged from 2 to 17 years, with all studies including both children (≤ 12 years of age) and adolescents (≥ 13 years of age). 25 –32 All studies used the term mTBI; none focused exclusively on concussion. 25 –32 Only one of the five studies compared mTBI patients with uninjured controls, 25 –27 whereas two of the studies compared mTBI patients with patients with mild non-brain injuries. 25 –29 The total number of unique participants with mTBI included in analyses across all studies was 733. 25 –32
The PedsQL 25 –27,30 and CHQ 28,29,32 were each utilized in two studies. One study used the KINDL questionnaire. 31 A description of the different HRQOL measurement tools can be found in Table 2. Four studies used proxy reports exclusively to measure HRQOL in at least some of the children/adolescents. 28 –32 Only one study used both proxy and child-completed HRQOL measures for all participants. 25 –27 Four of the studies asked participants to retrospectively complete HRQOL evaluations to assess their preinjury/baseline status. 25 –30,32 The timing of HRQOL measurements was variable: one study assessed HRQOL at first contact post-injury, 31 one assessed HRQOL at 1 month post injury, 25 –27 three assessed it at 3 months post-injury, 27 –30 one assessed it at 3 months after first contact, 31 two assessed it at 6 months post-injury, 27,32 and three assessed HRQOL at 12 months post-injury. 27 –30
HRQOL, health-related quality of life; PedsQL, Pediatric Quality of Life Inventory.
Proportion of pediatric mTBI patients with poor HRQOL outcomes
Only one study attempted to quantify the proportion of patients who had poor HRQOL outcomes. 30 Zonfrillo and colleagues found that 11.3% of mTBI patients reported a decrease in their PedsQL scores of ≥15 between baseline and 3 months post-injury, and that 12.9% reported a decrease of ≥15 points between baseline and 12 months after injury. 30 The authors used a cutoff of 15 points on the PedsQL as it represents the approximate difference between the mean score for healthy children and that for those with moderately severe chronic health conditions. 30,33,34
Predictors of poor HRQOL outcomes after mTBI
Three studies identified predictors of poor HRQOL in youth after mTBI. 28 –31 Zonfrillo et al found that poor HRQOL was significantly associated with older age, Hispanic ethnicity, less parental education, Medicaid insurance (vs. private insurance), lower levels of household income (< 30,000 vs. >100,000 USD at 3 months and 12 months and 60,000–100,000 vs. >100,000 at 12 months only), and a history of headaches or trouble sleeping. 30 Poor HRQOL was defined as a ≥15 point reduction in PedsQL score from baseline. A significant correlation was found between poor HRQOL scores and poor results on the Strengths and Difficulties Questionnaire (a behavioral screening questionnaire) and the revised Functional Status II questionnaire (a measurement of self-care, mobility, and other functional capabilities) using Spearman or Pearson coefficients (p < 0.001 for both questionnaires at first contact post-injury and 3 months later). 31,35,36 Greater somatic post-concussion symptoms were associated with worse physical HRQOL at both 3 and 12 months post-injury (p = 0.008), and greater somatic and cognitive symptoms were associated with worse psychosocial HRQOL (p = 0.004 for cognitive symptoms, p = 0.035 for somatic symptoms). 28 Similarly, increases in both physical and cognitive symptoms at 3 months post-injury (but not one or the other independently) were associated with diminished physical HRQOL at that time point (mean difference, 17.43; 95% CI, 10.37–24.49) but not at 12 months post-injury. 29 Increases in cognitive symptoms at 3 months post-injury were associated with worse psychosocial HRQOL at both 3 months (mean difference, 6.27; 95% CI, 2.72–9.82) and 12 months (mean difference, 8.36; 95% CI, 4.54–12.18). 29 Symptom increases were in turn more likely in mTBI youth who experienced a loss of consciousness at the time of injury and in youth with abnormalities indicated on magnetic resonance imaging. 29
Comparing mTBI patients with uninjured controls
One small study reported comparisons between youth with mTBI and uninjured controls. 25 –27 They did not find any significant differences in PedsQL scores between the mTBI patients and uninjured controls at any time point. 25 –27
Comparing mTBI with controls with mild non-brain injury
One study reported worse HRQOL outcomes on the PedsQL from mild non-brain injury youth at 1 month post-injury compared with mTBI youth (p = 0.009 for child reports, p = 0.002 for parent reports). 25 –27 The non-brain injury controls were children with nonoperative injuries such as closed fractures, sprains, dislocations, lacerations, bruises, or burns. However, Moran and colleagues reported significantly worse physical HRQOL on the CHQ in mTBI youth at 12 months post-injury compared with patients with orthopedic injuries. 28 Between 1 and 12 months post-injury, the physical HRQOL of children with orthopedic injuries had improved, whereas that of the mTBI patients remained largely unchanged. In this study, orthopedic injury was defined as an upper or lower extremity fracture yielding a score of 1–3 on the Abbreviated Injury Scale, excluding those who had evidence of head trauma or symptoms of concussion. 37
Variance in child versus proxy reports
One study that used collateral reporting from both patient and proxy found a significant difference between the two reports. The children reported lower HRQOL than their proxies estimated in all areas except cognitive functioning. 25,26
Discussion
Although the majority of mTBI patients experience a complete recovery in a relatively short time, there is a small but notable minority who experience prolonged effects. 9,38 The included studies confirm that this is also reflected in HRQOL outcomes in children and youth. Early identification of the subgroup of pediatric mTBI patients who experience poor HRQOL is important so that these outcomes can be mediated as much as possible. Predictors identified in this review include older age and high ratings of post-concussion symptoms, as well as increases in symptoms over time. Clinicians can use HRQOL measurement tools to assess high-risk patients, to ensure that they receive adequate management and follow-up care. By repeatedly measuring HRQOL during the recovery phase, clinicians will be able to monitor improving or declining HRQOL, which may be a global representation of the mTBI recovery process.
Several studies also found that some mTBI patients have compromised HRQOL up to a year or longer post-injury. This prolonged recovery may have implications on academic performance or psychosocial well-being, such as social isolation and increased risk of developing adverse psychiatric outcomes. 39 In addition, schools may have to provide academic accommodations to ensure that these children are able to successfully attend school and complete their work. These potential impacts of prolonged recovery warrant further investigation.
Another important finding identified was a difference between child and proxy reports, in which children reported lower HRQOL than their proxies estimated in all areas except cognitive functioning, a concerning finding given that all but one study relied on parent reports of HRQOL without collateral information from the child. 25 –27 This underappreciation of the impact of concussion/mTBI is likely not limited to parents/guardians, as mTBI is, largely, an invisible injury. These false perceptions may reduce the number of school and sport accommodations, as well as family and peer support, which may further diminish a child's social and emotional well-being. These perceptions, and their effects, represent an area in need of further study.
Although we attempted to characterize the longitudinal progression of HRQOL after mTBI, no typical course could be elucidated from the results. The changes in HRQOL over time were often isolated to individual HRQOL domains and the results were variable among studies. 25 –28,31,32 This may be because of the small number of studies and differences among patient populations resulting from varying definitions of mTBI.
Limitations/Future direction
One limitation of this review is that various definitions of mTBI were used across the studies. These heterogeneous definitions made it challenging to synthesize data from multiple studies and apply the results to clinical situations. For example, it is unknown if the results of this review can be extrapolated to the concussion population, as other clinical entities were included as well. This field would greatly benefit from consistent definitions of mTBI and concussion and a clear distinction between the two entities.
Future studies should appreciate that the proportion of mTBI patients who experience poor outcomes is relatively small, and thus means values could conceal the presence of this important subset of patients. This may explain the lack of significant differences between the mTBI groups and controls. Regardless, a subgroup of patients with poor outcomes appears to exist, and deserves further study to better identify them and provide meaningful intervention.
There was also considerable heterogeneity in the timing of HRQOL measurements and, therefore, we could not identify optimal timing of when HRQOL should be measured or when it should be expected to return to pre-injury scores. The lack of significant differences in HRQOL scores between time points may be explained by the fact that the first HRQOL measurement was ≥1 month post-injury in all studies that reported this information. By 1 month, the majority of mTBI patients may have recovered. 3,9 Future research efforts should attempt to measure HRQOL more acutely, and more frequently throughout the course of mTBI recovery so that the typical progression of HRQOL can be characterized, and patients with lower than expected HRQOL can be managed appropriately.
Conclusion
Pediatric mTBI is a clinical entity with few reliable objective measures to provide insight into a patient's progress, prognosis, and recovery. HRQOL is a validated and relevant, although often undervalued, outcome that can quantify recovery for both clinical and research purposes. Our findings show that there is a subset of mTBI patients who report diminished HRQOL in some domains long after their injury. Careful attention is needed to identify these patients and intervene where possible. In order for HRQOL measures to reach their potential in this application, additional research is needed to better understand the expected progression of HRQOL in the pediatric mTBI/concussion population and to identify clinical predictors and outcomes associated with impaired HRQOL.
Footnotes
Author Disclosure Statement
No competing financial interests exist.