
Abstract
Spinal cord injury caused by stab wounds (SCISW) results from a partial or complete transection of the cord, and presents opportunities for interventional research. It is recognized that there is low incidence, but little is known about the natural history or the patient's suitability for long-term clinical outcome studies. This study aims to provide population-based evidence of the demographics of SCISW, and highlight the issues regarding the potential for future research. The database of the Queen Elizabeth National Spinal Injuries Unit (QENSIU), the sole center for treating SCI in Scotland, was reviewed between 1994 and 2013 to ascertain the incidence, demographics, functional recovery, and mortality rates for new SCISW. During this 20 year period, 35 patients with SCISW were admitted (97.1% male, mean age 30.0 years); 31.4% had a cervical injury, 60.0% had a thoracic injury, and 8.6% had a lumbar injury. All had a neurological examination, with 42.9% diagnosed as motor complete on admission and 77.1% discharged as motor incomplete. A total of 70.4% of patients with an American Spinal Injury Association Impairment Scale (AIS) level of A to C on admission had an improved AIS level on discharge. Nine (25.7%) patients have died since discharge, with mean life expectancy for these patients being 9.1 years after injury (20–65 years of age). Patients had higher levels of comorbidities, substance abuse, secondary events, and poor compliance compared with the general SCI population, which may have contributed to the high mortality rate observed post-discharge. The low incidence, heterogeneous nature, spontaneous recovery rate, and problematic follow-up makes those with penetrating stab injuries of the spinal cord a challenging patient group for SCI research.
Introduction
A
The aim of this study was to provide population-based evidence of the incidence, demographics, functional recovery, morbidity, and mortality rates of patients with an SCISW, assisting in the planning of future research pathways for spinal cord repair and regeneration.
Methods
Study setting
The Queen Elizabeth National Spinal Injuries Unit (QENSIU) was built in 1993 to be the sole provider of initial treatment, rehabilitation and lifelong care for patients with an SCI >12 years of age in Scotland; a devolved region of the United Kingdom National Health Service. It is the hub of a managed clinical network funded by NHS Scotland. The unit provides care for a population of 5,300,000, and admits all patients who sustain traumatic spinal cord injury (TSCI). The etiology, gender, age, injury level, medical history, and degree of functional impairment of all new admissions are entered into the QENSIU database and have been published previously. 5 The database does not include deaths caused by SCI before admission, but contains information on all new SCIs being treated and rehabilitated in Scotland, enabling a population-based review of SCISW.
Scotland has a post-industrial mixed economy, and despite a high income per capita, has large health and socioeconomic variation. 6 There is a tradition of knife crime, but strict gun laws are in place. 7
The National Services Division of the Scottish Government granted approval for the collection and evaluation of data within the database.
Analysis
Patients admitted between January 1, 1994 and December 31, 2013 were included in this study if they were assigned with the International Statistical Classification of Diseases and Related Health Problems, Ninth Revision (ICD-9) diagnostic codes 806 (vertebral fracture with SCI) and 952 (SCI), 8 with the etiology of injury being a stab wound (Fig. 1).

Radiograph showing the blade of a knife embedded in the thoracic region of the spinal cord of a 28-year-old male. This stab wound resulted in the patient being discharged from the hospital with an injury level of T7 and American Spinal Injury Association Impairment Scale (AIS) score of A.
The neurological level of injury and degree of impairment after SCI was defined according to the International Neurological Classification of Spinal Injury using the American Spinal Injury Association Impairment Scale (AIS). 9 Admission and discharge AIS scores were assessed by SCI specialists who latterly completed an International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI) Instructional Course and an ISNCSCI Assessors Training Course for research purposes. No patients with an AIS score of E on admission; that is, stab wound with normal function, were admitted during the course of the study.
The QENSIU medical records, current family physician, and the National Patient Administration system were consulted as to the health of the subjects on the November 1, 2015.
Statistical analysis
Incidence data are presented as the mean and standard deviation over a 5 year time block, as well as the mean values over the 20 year study duration. 10 Crude annual incidence rates were calculated using the midyear population estimate for each year. 11 Annual incidence of homicide, nonsexual crimes of violence, and crimes of possession of an offensive weapon in Scotland were obtained for the years 1994–2013 from data published by the Scottish government, 12 –15 and annual incidence of crimes of public possession of a bladed weapon were obtained for the years 2004– 2013 from these figures. 12 All analysis was performed using MATLAB (version R2013a, MathWorks, USA).
Results
Incidence of SCISW
Between 1994 and 2013, 35 patients were admitted to the QENSIU with an SCISW, accounting for 2.1% of the 1638 TSCI admissions over this period. All SCISW were caused by assault. The mean annual incidence was 1.8 admissions per year (Table 1), corresponding to an annual incidence rate of 0.4 incidents per million population. A marked decrease in the incidence of SCISW was observed over the study duration (Fig. 2), and subsequently, no patients were admitted to the QENSIU with an SCISW between December 2010 and October 2015.

Results are presented as average values over a 5 year period, as well as over the entire study duration, with standard deviation shown in parentheses. Note that incidence of crimes of possession of a bladed weapon are only available from 2004 on.
Incidence of personal violence in Scotland
The incidence of homicide and nonsexual crimes of violence in Scotland remained relatively stable over the first 15 years of the study, whereas crimes for possession of an offensive weapon were 50% greater between 2004 and 2009 than between 1994 and 1998 (Table 1). There was a marked decrease in the mean annual incidence of homicide (29.5%) (Fig. 2), nonsexual crimes of violence (31.6%), possession of an offensive weapon (43.4%), and public possession of a bladed weapon (30.5%) in the final 5 years of the study, compared with the previous 5 years.
Gender and age at injury
Of the 35 patients admitted with an SCISW, 34 (97.1%) were male. The average age at injury was 30.0 years (± 11.6 years [range: 16–55 years]).
Nature of injury and management
The neurological deficit was associated in 11 (31.4%) patients with an injury at the cervical level of the spinal cord, in 21 (60.0%) it was associated with an injury at the thoracic level, and in 3 (8.6%) it was associated with an injury at the lumbar level (Fig. 3). Three (8.6%) patients, who had sustained injuries at C1/2, C3/4 and T8/9, required mechanical ventilation for a period of 290, 14, and 14 days, respectively.
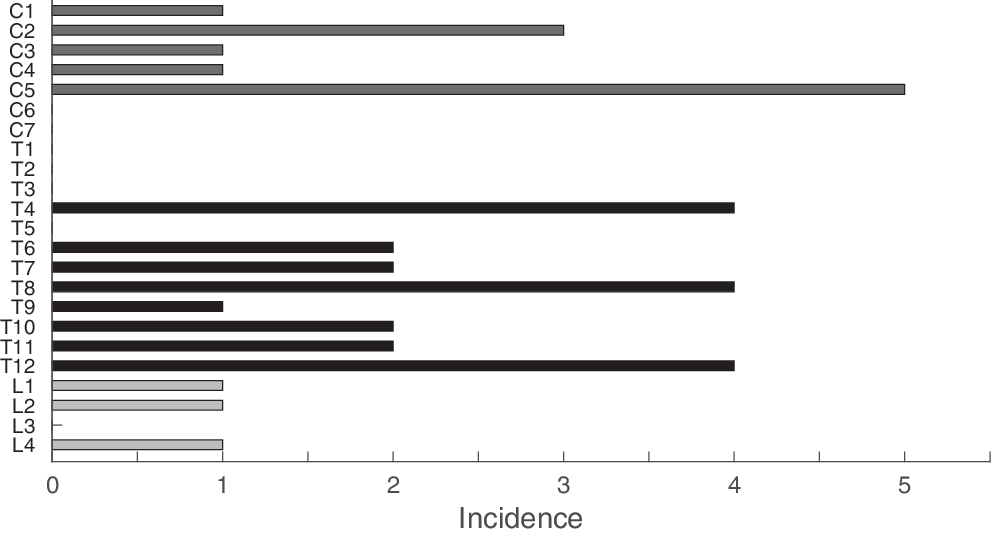
Injury level of 35 patients with a new spinal cord injury caused by stab wound in Scotland between 1994 and 2013. Injuries to the lumbar region are shown in light gray, the thoracic region is shown in black, and injuries to the cervical region are shown in dark gray.
Anatomically, 15 (42.9%) patients sustained a single stab wound and 20 (57.1%) patients sustained multiple wounds. There were a total of 96 incised wounds. The 12 single neck wounds resulted in 11 cases of neurological injury. The 18 chest wounds in 10 patients resulted in five deficits. None of the head (8 wounds in 7 patients), abdomen (12 wounds in 8 patients), or limb (10 wounds in 8 patients) wounds caused spinal cord damage; however, there was one femoral nerve transection. The 24 patients with back wounds (5 multiple) resulted in 19 cases of paralysis.
Thirty-four (97.1%) patients with SWSCI had primary closure and one a delayed closure because of late presentation. Eleven (31.4%) patients required a chest drain, with two thoracotomies and two laparotomies were performed (liver laceration: mesenteric artery division). Surgical explorations of the spine were required in six (17.1%) patients because of hematoma or a retained foreign body. There were three cerebrospinal fluid (CSF) leaks and one infection reported. All limb wounds and fractures (two total) had primary closure or fixation.
Extent and outcome of paralysis
All patients had an AIS assessment at both admission and discharge. On admission 15 (42.9%) had a motor complete injury (AIS A or B), whereas the remaining 20 patients (57.1%) were motor incomplete (AIS score C or D).
Of the 27 patients who had an AIS score of A to C on admission, 19 (70.4%) had an improved AIS score on discharge (Table 2). Eight (22.9%) patients were motor and sensory complete (AIS A) on admission, with three (37.5%) having an improved AIS score on discharge. Seven (20.0%) patients were motor complete and sensory incomplete on admission (AIS B), with six (85.7%) of these patients motor incomplete on discharge.
A, no motor function or sensation; B, no motor function with sensation; C, severely compromised motor function with sensation; D, slightly compromised motor function with sensation.
All patients underwent standard rehabilitation for their neurological level and severity of injury. Steroid administration was not routinely advised at the time of the study for penetrating injuries. Three patients (2 AIS A, 1 AIS D) had steroids administered, prior to admission to the unit, with no improvement in their AIS score at discharge.
Morbidity, mortality, and outcome
By November 1, 2015, 9 (25.7%) of the 35 patients had died, with an average life expectancy from injury of 9.1 years (± 5.7 years, range 0.8–16.7 years). The current life expectancy for a male in Scotland is 77 years. 11 The mean age at death for the SCISW patients was significantly lower, at 44.8 years. None of the deaths occurred during initial admission, and none are believed to be a direct consequence of SCI. The cause of death was available for six of the nine patients. Two patients died from an overdose, the other four patients died from pneumonia, bowel obstruction leading to abdominal sepsis, acute pancreatitis, and sudden cardiac death, respectively
Prior to their injury, 2 (5.7%) of the 35 patients were known to be smokers, 11 (31.4%) had a drug addiction, 4 (11.4%) were alcohol dependent, and 3 (8.6%) had hepatitis C. Of the 26 patients alive on November 1, 2015, 14 (53.8%) were smokers, 11 (42.3%) had a significant history of depression, 9 (34.6%) had a drug addiction, 7 (26.9%) were alcohol dependent, and 6 (23.1%) had hepatitis C. Despite national outreach clinics and a liaison nursing service, 14 patients (53.9%) had been lost to follow-up, 5 (19.2%) had attended all follow-up appointments since discharge, 6 (23.1%) had not attended the hospital for any appointments for >6 years, and 2 patients were in prison (7.7%). In 2014, these patients only attended 40 of 127 (31.5%) scheduled hospital appointments (range: 15–100%).
Discussion
This population-based study shows that SCISW has a low incidence, occurs primarily in young males, leads to greater spontaneous functional recovery, and has a higher morbidity and mortality rate than that of the general SCI population.
Incidence
There were 35 cases of SCISW in Scotland between 1994 and 2013, representing ∼2% of all TSCIs in Scotland over this period. 5 This rate is higher than in the United States (0.3%) 2 and Europe (1.1%), 16 but is much lower than in South Africa, where SCISW has been reported to be responsible for 26% of all TSCIs. 17 The variation in the proportion of TSCIs caused by SCISW will relate to cultural, economic, and political differences in combination with the availability of weapons. In the United States, gunshot wounds were reported to be the cause of 5.8% of TSCIs between 1997 and 2012. 18 By comparison, in Scotland there were only 10 patients with TSCIs caused by gunshot wounds admitted between 1994 and 2013, accounting for 0.6% of all TSCI admissions. 5 Of these injuries, five were assaults (two of which were caused abroad), two were self-inflicted (one accidental and one deliberate self-harm), and three were caused during acts of war.
In 79% of cases of SCISW in Scotland, the patient lived in the Greater Glasgow area. This area, which has a population of 1,200,000 (accounting for less than a quarter of the Scottish population) has been ranked as the United Kingdom's most violent area, 19 with a homicide rate between 2009 and 2013 of 1.5 per 100,000 people, 14 compared with 1.0 across the United Kingdom as a whole. 20 However, unlike in the United States, where firearms were responsible for ∼70% of homicides in 2010, 21 firearms were only associated with 4.4% of homicides in Scotland between 2004 and 2013. 14 Instead, Glasgow has been notorious for knife crime, with 48.1% of homicides in 2010 committed using a knife, down from 58% in 2008. 7 This may be the reason for the large proportion of SCISW observed in this area.
Annual incidences of homicide, nonsexual crimes of violence, and crimes of possession of both a bladed and offensive weapon all decreased in the last 5 years of the study compared with the previous 5 years, with smaller reductions in both homicide and violent crime also observed in the penultimate 5 years of the study. 12,14 The reduction in homicide, assaults, and stabbings are likely linked to knife amnesties (1993 and 2006) and increased penalties for those caught carrying a knife, which were implemented in 2007. 22 Similar reductions have been subsequently reported elsewhere in the United Kingdom. 23
Gender and age at injury
The population of Scotland in 2011 was 48.5% male and 51.5% female. 11 The proportion of males sustaining an SCISW (97.1%), is disproportionate and is additionally far greater than the proportion of males in the general Scottish TSCI population (75.2% over the same period), 5 and is a consistent feature of all SCISW studies. 17,24 –27
The average age at injury for SCISW (30.0 years), was 17.2 years lower than that of the general TSCI population in Scotland, who had an average age at injury of 47.2 years over the same period. 5 Young males have an increased likelihood of being involved in episodes of violence and the age is mirrored in fatal stabbings, 28 nonfatal stabbings, 29 general assault, 30 and SCISW. 17,24 –27
Nature of injury
The site of injury varies in general assault, 29 fatal stabbings, 28 and SCISW. In this study, the majority of SCISWs (60%) occurred in the thoracic region of the spinal cord (from wounds in the back) a finding that has also been reported by Lipschitz 27 (74% thoracic, 18% cervical) and Peacock and coworkers 26 (64% thoracic: 30% cervical: 6% lumbar). The pattern of injury and low incidence of lumbar injuries relates to the target areas in stabbing attacks with both the cervical and thoracic regions (front and back) within the natural reach of the attacker. 31 The spinal cord is vulnerable in the posterior triangle of the neck with the major vessels, trachea, and esophagus more accessible via the anterior triangle. There were no SCISWs between C6 and T3, and it is probable that this area is less accessible and that anterior penetrative injuries in this area lead to high levels of mortality because of vascular injury or injury to the trachea. 32
Extent and outcome of paralysis
The proportion of motor complete injuries (AIS A or B) caused by SCISW in Scotland between 1994 and 2013 (42.9%) agrees with rates reported in the United States (37%) 24 and Iran (43%), 25 and is approximately equal to the rate in the general Scottish TSCI population over the same period (39.7%). 5 The proportion of patients with an AIS A injury (23.5%) mirrors the findings of Peacock and coworkers 26 who found that in South Africa 21% of patients with an SCISW had a motor and sensory complete injury. The conversion rate of motor complete to motor incomplete injuries over time reported here (46.6%) agrees with a study in Iran, where 40% of patients who were motor complete on admission had improved function at discharge. 25
That 70.4% of patients had an improved AIS score on discharge agrees with Velmahos and coworkers, 17 who found that 61% of patients in South Africa made significant recovery, characterized as the ability to walk unaided or with crutches. This is significantly higher than the rate of recovery for the general TSCI population. Marino and coworkers 33 found that of the 1626 patients with an AIS score of A to C on admission to Model Centres in the United States, an average of 39.9% of patients had an improved AIS score on discharge. This is also better than the recovery after gunshot wounds (32%) and road traffic collisions (44%). 17 The finding that three out of eight (37.5%) patients who had an AIS score of A on admission were discharged with an improved AIS score is greater than the rate reported in the general TSCI population, with Marino and coworkers 33 finding that of 981 patients admitted to Model Centres in the United States with an AIS level of A on admission, only 11% were discharged with an improved AIS score. The superior functional recovery observed in patients with SCISW has important implications in long-term follow-up studies.
Morbidity, mortality, and outcome
Strauss and coworkers 34 predicted that a 25-year-old male patient with the most severe TSCI (C1–3, AIS A), who survived the first 3 years post-injury, would have a life expectancy of 25 years post-injury. However, for the nine patients who had died since discharge in this study, the life expectancy was only 9.1 years. This suggests that there are other medicosocio and economic factors responsible for the early deaths of these patients with SCISW. 34 Tetrault and Courtois 35 reported that pre-accident, 32% to 35% of patients with a TSCI had been using illegal drugs, and Young and coworkers 36 reported that 21% of patients with a TSCI were alcohol dependant. It was found that in Scotland, pre-stabbing, 31.4% of the SCISW population had been using illegal drugs, and 11.4% were alcohol dependant, increasing to 34.6% and 26.9% post-stabbing, respectively.
In this group of SCISW patients, 42.3% had moderate to severe depression, compared with the 25% found by Williams and coworkers 37 in patients with TSCI. The reduced life expectancy, high level of comorbidities, and poor follow-up attendance after SCISW suggests that long-term outcome studies with this population may be challenging to achieve.
Relevance and limitations
Human models for research in SCI are challenging, and a partial or full transection of the spinal cord with a minimum shear or compression element offers advantages. There has been recent focus on the use of a combinational therapy involving cellular and structural implants plus rehabilitation to induce neural repair following a transection, such as that caused by a stab wound. 3,4
The SCISW population represents a small proportion of those with TSCIs. They are generally of a young age, with a reduced life expectancy and lifestyle options that may interfere with long-term compliance in rehabilitation, follow-up, and research review. The patients also demonstrate a higher level of spontaneous functional recovery post-injury compared with the general TSCI population. These findings suggest that this patient group will present particular challenges for experimental research.
A limitation of this study is the small sample size, caused by the infrequent nature of SCISW. Long-term multi-center studies may enable a more detailed analysis of the demographics and functional recovery of patients with an SCISW. A further limitation is that MRI/CT scans were not available for every participant. Although imaging has historically played only a small role in interpreting neurological deficit and functional recovery after SCISW, this lack of imaging meant that it was not possible to compare initial or longitudinal changes in the spinal cord to neurological deficit or functional recovery.
Conclusion
This study demonstrates that SCISW in Scotland occur primarily in young males. The incidence rate is low, and is currently decreasing in this region. Spontaneous functional recovery following SCISW appears better than that for the general SCI population. There is a high mortality rate post-discharge, unrelated to the SCI, with a poor life expectancy for these patients compared with their peer groups. The patient group also has a range of comorbidities, including high levels of drug and alcohol dependence, and has poor rates of attendance at hospital follow-up. Although partial or full transection may provide a useful model for spinal cord repair, patients with an SCI from a stab injury may be a particularly challenging group for experimental research studies.
Footnotes
Acknowledgments
The authors thank Dr. Alan McLean, Matthew Fraser, Ana Bewick, and the QENSIU staff for maintaining the database, and Dr. Jim Guest for comments on the initial manuscript.
Author Disclosure Statement
No competing financial interests exist.