
Abstract
Although most patients recover fully following mild traumatic brain injury (mTBI), a minority (15–25%) of all patients develop persistent post-traumatic complaints (PTC) that interfere with the resumption of previous activities. An early identification of patients who are at risk for PTC is currently performed by measuring the number of complaints in the acute phase. However, only part of this group will actually develop persisting complaints, stressing the need for studies on additional risk factors. This study aimed to compare this group of patients with many complaints with patients with few and no complaints to identify potential additional discriminating characteristics and to evaluate which of these factors have the most predictive value for being at risk. We evaluated coping style, presence of psychiatric history, injury characteristics, mood-related symptoms, and post-traumatic stress. We included 820 patients (Glasgow Coma Scale [GCS] score 13–15) admitted to three level-1 trauma centers as part of the UPFRONT-study. At 2 weeks after injury, 60% reported three or more complaints (PTC-high), 25% reported few complaints (PTC-low), and 15% reported no complaints (PTC-zero). Results showed that PTC-high consisted of more females (78% vs. 73% and 52%, p < 0.001), were more likely to have a psychiatric history (7% vs. 2% and 5%), and had a higher number of reported depression (22% vs. 6% and 3%, p < 0.001), anxiety (25% vs. 7% and 5%), and post-traumatic stress (37% vs. 27% and 19%, p < 0.001) than the PTC-low and PTC-zero groups. We conclude that in addition to reported complaints, psychological factors such as coping style, depression, anxiety, and post-traumatic stress symptoms had the highest predictive value and should be taken into account in the identification of at-risk patients for future treatment studies.
Introduction
T
What causes PTC to persist in some patients remains the subject of debate, as does the name for such symptoms. Although they have been referred to as post-concussional syndrome (PCS) for many years, the World Health Organization (WHO) cautioned against this, stating that association was not proof of causation. In this study, we therefore utilize PTC to describe the patients with persistent symptoms. 5,6 With regard to the causal mechanism, recent studies suggest that from the acute phase on, there is a complex interplay of neurogenic, psychological, and social factors such as the injury itself, life stressors, and pre-morbid health status. 5,7,8 Currently, there is consensus on some factors that are used to identify patients in the acute phase who are at risk for long-term problems. 2 Especially, a high number and severity of early reported complaints is thought to predict persistent PTC. 9,10 However, the number of patients who report three or more complaints early after injury is high, 10 and only a portion of these patients will develop persistent PTC. Therefore, investigating additional characteristics of the at-risk group of patients reporting a high number of complaints in the acute phase might enhance a more accurate prediction of which patients will actually develop PTC. Until now, relatively few studies have focused on these additional characteristics. Investigating which particular characteristics distinguish this at-risk group from the patients who report little or no complaints could offer valuable insight into potential additional risk factors and points of focus for prevention.
Several studies have found that patients with high numbers of reported complaints in the acute phase have pre-morbid psychological or early emotional factors in common that are likely to play a role in the exacerbation or maintenance of complaints over time. For instance, patients' psychiatric history, 2 pre-morbid coping style, 11 and the presence of depression or anxiety in the early stage after trauma 3 were identified as important factors. In particular, the stress response and experienced anxiety in the acute phase after trauma have been found to be predictive of the subsequent development of post-traumatic stress disorder (PTSD) and thus of a poor outcome. 12,13 In a recent study, Lagarde and colleagues 14 argue that the persistent symptoms may in fact be a part of the hyperarousal dimension of PTSD. Considering the fact that there may be a combination of (pre-morbid) psychological and emotional factors responsible for a worse outcome besides acute reported complaints, 15,16 a relevant question is whether patients with a high amount of complaints in the acute phase differ from patients with a low number or no complaints with regard to psychiatric history, the presence of acute stress, and the presence of depression and/or anxiety.
The aim of this study is therefore to describe the characteristics of an mTBI patient group at risk, based on the fact that the patients have a high number of complaints in the acute stage, for developing persistent complaints in the long term. To find other discriminating characteristics, these patients will be compared with mTBI patients with few complaints, and patients with no complaints at all. We will investigate whether these three groups differ on pre-morbid personality characteristics (i.e., coping style, presence of psychiatric history), on injury-related characteristics (i.e., GCS score, computed tomography [CT]-scan abnormalities), and on mood-related symptoms (i.e., PTSD, anxiety, and depression). Moreover, we will investigate which of these factors contribute most to the prediction of being at risk. This study might provide valuable information for identifying possible combinations of risk factors that may lead to a better prediction and subsequent follow-up of mTBI patients at risk for an unfavorable outcome. Moreover, insight into the differences between patients without complaints and with few complaints may provide clear starting points for early intervention or treatment programs.
Methods
Design and setting
This prospective follow-up study is part of a larger ongoing prospective cohort study on outcome in mTBI (the UPFRONT-study) that started in January 2013. The UPFRONT-study is being conducted in three level-1 trauma centers: University Medical Center Groningen (UMCG), St. Elisabeth Hospital Tilburg (EZH), and theMedisch Spectrum Twente (MST) in the Netherlands. Patients included in the study filled out questionnaires at 2 weeks after the injury. Demographic variables, injury characteristics, and psychiatric history (having received psychological or psychiatric treatment) were obtained from the hospital records. The Injury Severity Score (ISS) was determined based on these records. 17 On admission, Glasgow Coma Scale (GCS) scores were determined as part of the neurological examination. A CT scan of the brain was performed on admission and CT abnormalities were defined by the Marshall score (category 1 = no abnormalities, categories 2–6 = abnormalities). 18
Participants
In the current study, 820 patients 16 years and older with mTBI admitted to the emergency departments (EDs) of the UMCG, MST, and EZH between January 2013 and January 2015 were included. According to the recommended guidelines of the European Federation of the Neurological Societies (EFNS) task force, mTBI was defined as a blunt impact to the head with sudden acceleration, deceleration, or rotation resulting in a GCS score of 13 to 15 on presentation at the ED, post-traumatic amnesia (PTA) lasting <24 h, and/or loss of consciousness lasting <30 min. 19 Patients were excluded if they suffered from chronic alcohol and/or drug abuse, major psychiatric disorders, neurological disorders, or major learning disabilities. Patients who were not fluent in Dutch or had no permanent home address were also excluded due to anticipated follow-up difficulties.
Measures
Post-traumatic complaints
The Head Injury Symptom Checklist (HISC) is derived from the Rivermead Post-concussion Symptoms Questionnaire (RPQ) 16 and contains the 21 most commonly described post-concussive symptoms. A pre-injury and a current symptom level are indicated by the patient. Values range from 0 to 2 (0 = never, 1 = sometimes, 2 = often). Both the total amount of complaints (0–21) and the severity of complaints (0–42) can be determined. Three groups were made based on the number and nature of reported complaints. The no complaints group consists of the patients who reported 0 complaints. The many complaints group consists of patients who had 3 or more complaints, of which at least one was either in the cognitive- or socio-emotional domain. The few complaints group consists of the patients with 1 or 2 complaints, or more but in the physical domain only.
Coping style
The Utrechtse Coping Lijst (UCL) was used to measure pre-morbid coping style. 20 Coping refers to the efforts made to minimize the impact of stressful events. The UCL is a 47-items questionnaire with seven subscales that represent different coping styles: Problem solving, Self-distraction, Avoidance, Social support, Withdrawal, Expression of emotions, and Positive reframing. Scores on each subscale range from a very low use of that coping style to very high use compared with an age- and gender-matched norm group (range 1–5). For analyses, we dichotomized the values in a high (range 4–5) and low use of the coping style (1–2).
Post-traumatic stress
The Impact of Event Scale (IES) is a self-report measure of post-traumatic stress. 21 The IES consists of 15 statements, with scores ranging from 0 to 5 and a maximum score of 75. Seven items on the scale concern “intrusion,” which is described as strong waves of emotion toward the event. The other eight items are directed at symptoms of “avoidance,” staying away from reminders of the event. For the current study, the Dutch version of the IES was used. 22
Depression and anxiety
The presence or absence of depression and/or anxiety was assessed by means of the Hospital Anxiety and Depression Scale (HADS). 23 The HADS is a 14-item questionnaire, containing two subscales, the depression scale (HADS-D) and anxiety scale (HADS-A) of seven items each. Items are rated on a scale from 0 to 3. A cut-off score of ≥8 is recommended for establishing the presence of both depression and anxiety. 24
Statistical analysis
The data were analyzed with SPSS 22.0 (IBM Corp., Armonk, NY). 25 Differences in patient demographics and injury characteristics between the three groups were tested using the χ2 test (two-tailed) for categorical data, multivariate analyses of variance (MANOVA) for parametric data, and the Kruskall-Wallis test for non-parametric data. Post hoc comparisons were performed under the Bonferroni criterion. A binomial logistic regression was performed to determine which variables had the strongest contribution to the prediction of whether patients had many complaints or not. Alpha was set at 0.05, two-sided.
Results
Demographic and clinical characteristics
A total of 820 mTBI patients completed the 2 weeks of measurement. Of these 820 patients, 122 patients (15%) reported having no complaints at all (group 1: PTC-zero), 205 patients (25%) reported few complaints (group 2: PTC-low), and 493 patients (60%) reported three or more complaints with at least one in the cognitive and/or emotional domain (group 3: PTC-high). The number of reported complaints differed significantly between these groups (p < 0.001). Post hoc analysis (Bonferroni adjusted) showed significant differences between all three groups (all p < 0.001), with, as expected, patients reporting significantly more complaints in each consecutive group (1 < 2 <3).
Table 1 shows a comparison of the three complaint groups. Groups differed with respect to gender, psychiatric history, and several injury-related variables such as GCS score, the rate and days of hospital admission, and the presence of CT abnormalities. Post hoc analyses showed that PTC-high contained more females than PTC-zero and PTC-low (51.9% vs. 73.2%, p < 0.001 and 51.9% vs. 77.9%, p < 0.001, respectively). A psychiatric history was more common in PTC-high (4.5%) than PTC-low (2.4%, p = 0.032) and PTC-zero (0%, p = 0.019).
Mean (±SD), range; all others = number (%)
CT, computed tomography; GSC, Glasgow Coma Scale; ISS, Injury Severity Score; mTBI, mild traumatic brain injury; SD, standard deviation.
With regard to the measures of injury severity no difference in trauma severity (ISS) was present between the three complaint groups. There was a very small but significant difference in GCS scores between patients in PTC-high and PTC-low, with patients in PTC-high scoring lower then PTC-low (14.5 vs. 14.6, p = 0.012, without any significant difference existing between PTC-high and PTC-zero. Patients in PTC-high were more often admitted to the hospital than PTC-low (64.1% vs. 57.6%, p = 0.05) and PTC-zero (64.1% vs. 51.6%, p = 0.041). Significantly more patients in PTC-high had CT abnormalities when compared with patients in PTC-zero (19.1% vs. 6.6%, p = 0.002). No differences were found between groups with regard to age, educational level, and the presence of an alcohol intoxication at the time of injury.
Coping, mood, and impact of events
Table 2 shows the scores on the depression and anxiety scale of the HADS and the scores on the IES for the total mTBI group and the three complaint groups. Because age and level of education did not differ between groups, there was no need for controlling for these variables. Significant differences were found between the three groups for all variables. Post hoc analyses showed that patients in PTC-high scored higher on HADS-D and HADS-A and IES compared with the patients in PTC-zero (p < 0.001) and PTC-low (p < 0.001).

Number (%)
HADS, Hospital Anxiety and Depression Scale; IES, Impact of Event Scale; mTBI, mild traumatic brain injury; PTC, post-traumatic complaints; PTSD, post-traumatic stress disorder.
Figure 1A depicts the percentage of patients scoring low versus high on the active coping style and Figure 1B depicts the percentage of patients scoring low versus high on the passive coping style. With regard to a low and high use of an active and passive coping style, significant differences between groups were found for both coping styles. Surprisingly, a higher percentage of patients in PTC-high have a high use of an active coping style. However, this difference was not significant between groups. In PTC-high, more patients scored high on passive coping when compared with PTC-zero, in which a large proportion of patients scored low on passive coping (χ = 7, 7, p = 0.006).
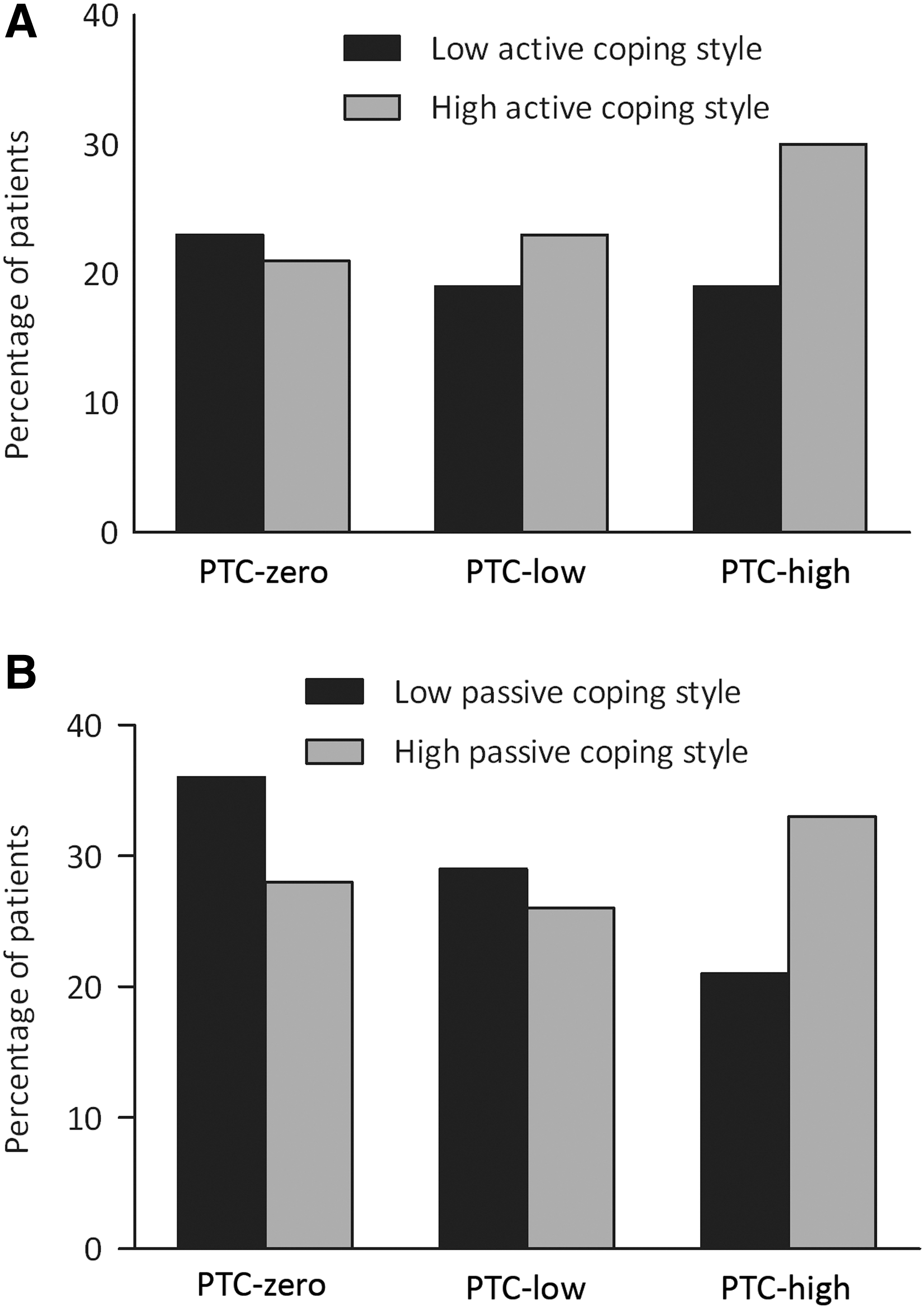
Percentage of patients per group scoring high versus low on the active coping style
Likelihood of being at risk
Table 3 shows the results of the binomial logistic regression analysis that inspected the effects of several factors on the likelihood of having many complaints (PTC-zero and PTC-low vs. PTC-high). The logistic regression model was significant, χ2(9) = 63.20, p < 0.0001. The model correctly classified 61.6% of cases. Sensitivity was 81.3% and specificity was 49.9%. Of the nine predictor variables, six were significant: sex, anxiety, depression, PTSD, active coping style, and passive coping style (as shown in Table 3). Females had 2.68 times higher odds to be in PTC-high. Patients with anxiety had 3.46 times higher odds, with depression 2.63 higher odds and with PTSD-related complaints 1.76 higher odds of ending up in PTC-high. A higher use of an active coping style was also associated with a higher likelihood of being in PTC-high. A higher use of a passive coping style was associated with a reduced likelihood of being in PTC-high. Given that PTC-high had more patients with a high-use passive coping style when compared with PTC-zero, this was not expected.
Note: Sex is for females compared to males
Discussion
Many studies have attempted to identify in the acute phase the minority of mTBI patients that are at risk for developing long-lasting PTC and consequently for a negative outcome. 26,27 The current criterion for identifying the at-risk patients is commonly based on a high number and a high severity of complaints in the acute phase, which is also used as an inclusion criterion in experimental intervention studies. 5 However, not much is known about other factors that distinguish the at-risk patients from the patients with an expected favorable outcome in the acute phase. In this study, we aimed to describe the characteristics of an at-risk group with many complaints, compare them with patients without and with few complaints, and investigate their predictive value. Several differences were found in pre-morbid and injury-related characteristics between these groups. We also found that the at-risk group had a higher number of reported depression, anxiety, and post-traumatic stress. Moreover, the at-risk group had higher levels of an active and a passive coping style. Further evaluation of these differences shows us that these differences were consistently present between the many complaints group on the one hand and the non- or few complaints group on the other, suggesting that the latter two groups were fairly similar.
In our study, we found that at 2-weeks post-injury, a large percentage (60%) of all patients reported three or more complaints of which at least one was of a cognitive or emotional nature, 25% of all patients reported one or two complaints (or of a physical nature solely), and 15% reported having no complaints at all. This is consistent with a recent study by Matuseviciene and colleagues, 10 in which it is described that in the acute phase, 56% of patients reported three or more complaints. 28,29 Considering the large number of patients (60%) that report many complaints and a much smaller percentage of patients (15–25%) 4 that actually suffer from persistent PTC, the necessity to find additional risk factors becomes even more apparent. Our results show interesting overall differences between these three complaint groups on demographics and injury-related characteristics, with regard to sex, GCS score, hospital admission, CT abnormalities, and the presence of a psychiatric history. With regard to mood and coping we found differences between the complaints group on levels of anxiety and depression, PTSD complaints, and active and passive coping style. Further evaluation of these factors in a prediction model showed that especially sex, anxiety, depression, PTSD, and active and passive coping were important predictive factors for having many complaints.
Female patients had a higher chance of having more complaints, which is consistent with findings that women report more complaints then men following mTBI 4,30 and have a higher risk of poor outcome. 26,31 Although it did not reach significance as a predictive factor due to small numbers, we found that patients who reported many complaints were more likely to have a psychiatric history. This is in accordance with findings of different studies, 2,32 that found a psychiatric history to be independently associated with the persistence of complaints. When looking at injury-related characteristics, we found that patients with many complaints had a higher hospital admission rate, a higher percentage of CT abnormalities, and a lower GCS score. However, no differences were found between groups on the ISS, and considering the small difference and effect size of the GCS score (14.6 vs. 14.5, r = 0.12) it is unlikely that there were clinically relevant differences between groups with regard to severity of injury. Moreover, none of the injury severity variables were significant in the prediction model. These findings are in accordance with other studies that find traditional indicators of severity contribute little if anything to the persistence of post-concussive complaints. 31,33
Especially interesting in this matter, is that the at-risk group had a disproportionately high number of patients scoring above cut-off on depression and anxiety scales and post-traumatic stress symptoms when compared with the patients with few and without complaints. Moreover, these were all found to be significant predictors of many complaints. 3,12,13 These findings can be interpreted in the light of recently published research that suggests that PTC are unrelated to injury severity but may actually be an expression of injury-induced mental distress, related to mood disorders and/or PTSD. 14 Given the often life-threatening circumstances of mTBI, PTSD following mTBI is the most expected of anxiety sequelae. Prevalence rates of PTSD following mTBI are varying, and range from 20% 34 to 84%. 35 Harvey and Bryant 13 found that the majority (80%) of patients that have high scores on post-traumatic stress in an early stage will develop PTSD in a later stage. Many patients with anxiety also deal with depression, and high rates of comorbidity (33–65%) 36 have been reported. It has been frequently found that mood disorders have a negative influence on cognitive functioning. 37 Consequently, the presence of mood disorders might be a determining factor in the persistence of complaints over time.
We also found that between groups, patients with many complaints more often showed a high use of a passive coping style in comparison with patients without complaints. The use of an inadequate, passive coping style has been linked to depression 40 and an increased risk for developing acute stress symptoms, 38 and has been put forward in several studies as a risk factor for the development of persistent complaints. 39,40 However, in contradiction with our findings in group differences, a high use of passive coping style lowered the likelihood of many complaints in our prediction model. This can be explained by the fact that there is a unavoidable coherence between passive coping and some predictors (i.e., depression, anxiety, and PTSD). With regard to active coping, we found that patients with many complaints had a higher use of this style in comparison with patients without complaints. A high use of an active coping style was also a significant predictor of more complaints. Although the correlations between active coping style and a better outcome have been found to be moderate to weak, 40,41 an active coping style seems intuitively associated with a more positive outcome. However, our finding could be explained by the fact that the use of an active coping style has also been found to be contra-productive in the acute phase and associated with poor outcome. 42,43 When in the early stage of recovery, patients with an active coping style could be at risk of over-exerting themselves, instead of allowing a paced and gradual resumption of activities. Findings such as these show that there may be other characteristics that can help to further specify the at-risk group and identify the at-risk patients more accurately.
Although this study provides valuable insights in patients at risk for persistent PTC, some limitations need to be addressed. First, our study included patients at the ED where the acute setting and high turnover times often interfere with data collection. This has inevitably led to a substantial number of not-included patients resulting in a potential selection bias. Second, this study relied on self-report measures of pre- and post-injury symptoms, and it is known that many patients misperceive their pre-injury functioning as better than the average population. This so called good-old-days-bias could have caused an over-estimation of the number of complaints. 44 Finally, our study investigated group differences between different complaint groups, and although we have identified valuable potential risk-factors and their predictive value this is only a first step toward a better identification of at-risk patients in the acute phase. Further investigation using a longitudinal approach to investigate these factors on long-term outcome is necessary to determine the actual predictive value.
In summary, the group of patients with many complaints shortly after injury seems to be characteristically different from the patients without and with few complaints, and is highly likely to contain those patients who are at risk for suffering from long-term PTC and a negative outcome. The results of our study further show that not injury-related characteristics, but psychological factors are most predictive of having many complaints. That these factors could lead to persistent PTC is underlined by recent articles that describe the relations between persistent PTC, coping, mood disorders, and PTSD. Therefore, based on the results of this study, we argue that for the selection of at-risk patients for future intervention studies, signs of depression, anxiety, and acute stress symptoms as well as coping style should be taken into account, in addition to the number of complaints. Anxiety- and PTSD-related complaints following mTBI have been proven to be successfully treatable with cognitive behavioral therapy, 12 which also addresses maladaptive coping styles. Identification and subsequent treatment of these patients could therefore lead to a significant decrease in the number of mTBI patients that suffer from complaints in the longer term.
Footnotes
Author Disclosure Statement
No competing financial interests exist.