
Abstract
In patients in the chronic phase after recurrent mild traumatic brain injury (mTBI), alterations in gamma-aminobutyric acid (GABA) concentration and receptor activity have been reported, possibly mediating subtle but persistent cognitive deficits and increased rate of dementia in older age. We evaluated whether anodal transcranial direct current stimulation (atDCS) over the primary motor cortex reduces GABA concentration and GABAB receptor activity in patients with recurrent mTBI. Seventeen patients (mean age 25, two women) in the chronic phase after recurrent mTBI and 22 healthy control subjects (mean age 26, two women) were included. All participants received comprehensive cognitive testing and detailed questionnaires on post-concussive symptoms at baseline. Subsequently, they participated in four experimental sessions, consisting of either magnetic resonance spectroscopy (MRS)/atDCS/MRS, transcranial magnetic stimulation (TMS)/atDCS/TMS, MRS/sham/MRS, or TMS/sham/TMS to determine GABA concentration (from MRS) and GABAB receptor activity (from TMS) after atDCS and after sham stimulation. Patients with mTBI scored significantly lower on verbal fluency tasks compared with healthy control subjects. GABA concentration at baseline was associated with the number of mTBI, although no group differences in GABA concentration and GABAB receptor activity were found. Moreover, no effects of atDCS on GABA concentration and receptor activity were seen in patients with mTBI or healthy control subjects. GABA concentration may increase with the number of mTBI, but atDCS did not modulate GABA concentration and receptor activity, as has been reported previously. Specifics of experimental design and analysis, but also characteristics of the respective samples, may account for these differential findings, and should be addressed in future larger studies.
Introduction
T
Patients with mTBI generally reveal no overt structural brain lesion on routine magnetic resonance imaging (MRI) or computed tomography scans. After a single mTBI, most patients report full recovery regarding clinical and cognitive symptoms within days or weeks. A minority of patients complains about persistent symptoms over months and years. 3 This so called post-concussion syndrome comprises physical (e.g., headaches, dizziness, fatigue), cognitive (e.g., reduced concentration, memory dysfunction) and/or emotional (e.g., depression, anxiety) symptoms. 4 Further, slight changes in cognitive ability may persist, as determined by cognitive tests. 5 In particular, episodic memory, working memory, attention and executive functioning have been reported to be reduced in these patients. 6
In addition, recurrent mTBI may be associated with symptom severity, 7 increased recovery time, 8 increased susceptibility to sustain further mTBI, 8 and higher risk for an earlier onset of Alzheimer's disease (AD); 9 although not all studies could confirm these findings. 10 –13 Note, though, that an association between recurrent mTBI and low cognitive performance may also be based on severity of post-concussive symptoms as such. Further, pre-injury characteristics such as alcohol abuse and psychiatric history might predispose long-term post-concussive symptoms and cognitive deficits. 14 In sum, recurrent mTBI may not be a benign condition, but the issue is still discussed controversially, and the mechanisms underlying the proposed association need to be elucidated in more detail.
Because clinical MRI generally reveals no overt brain lesions, microstructural and neurochemical changes have been proposed to account for slight but persistent deficits in this population. On a structural level, diffusion tensor imaging has been used as a measure of white matter integrity. 15 Studies here revealed alterations regarding fiber integrity in the corpus callosum of patients with mTBI 16 –18 and moderate TBI, 17 –19 possibly because of demyelination in response to the brain injury. 15
Neurochemical changes after mTBI have been analyzed by MR spectroscopy (MRS) and non-invasive brain stimulation (NIBS). Regarding MRS, studies postulated a tight link between cognitive impairments in patients with mTBI and metabolite alterations. 20 Here, alterations in total choline, N-acetylaspartate + N-acetylaspartylglutamate, creatine + phosphocreatine and glutamate + glutamine concentrations have been evaluated, 21 but recent technological advances also allow an in vivo detection of gamma-aminobutyric acid (GABA), 22,23 a promising indicator for metabolic disruption after mTBI. 22,23 Although alterations in GABA concentrations after TBI were demonstrated in animal studies, 22,24 MRS-studies in human beings failed to show differences in GABA concentrations between patients with mTBI and healthy control subjects. 23 In contrast, NIBS studies concentrated on changes in GABA receptor activity in human motor cortex.
Here, transcranial magnetic stimulation (TMS) protocols such as long-interval intracortical inhibition (LICI) and corticomotor silent period (CSP) have been used to evaluate GABAB receptor activity. 25 Recent TMS studies revealed alterations of these parameters in athletes with recurrent mTBI compared with healthy control subjects. A majority of these studies showed enhanced LICI 23,26 –28 and prolonged CSP durations 23,26,27,29,30 indicating higher activity in the GABAB receptor system 29 and thus intracortical inhibition-excitation imbalance. 31 In these patients, a higher GABAB receptor activity has been linked to decreased long-term potentiation (LTP)-like plasticity and motor learning. 28
Because an association between anodal tDCS (atDCS) and a reduction in GABA concentration was shown in several previous reports, 32 –35 atDCS as an easy-to-use and safe tool 36 –38 could be a promising treatment for patients with diseases with pathologically high cerebral GABA concentration, such as mTBI. 31 Also, recent reports demonstrate that atDCS reduces GABAB-mediated inhibition, indicated by shortened CSP duration after atDCS. 39 tDCS is able to modulate metabolite concentration in a polarity-specific manner 35 : atDCS increases cortical excitability, possibly mediated by a decrease in GABA concentration, 32 –35 cathodal tDCS (ctDCS) inhibits cortical excitability, possibly mediated by a reduction in glutamate concentration. 32,34,35
The aim of this study was therefore twofold: first, to evaluate differences in cognition, GABA concentration, and receptor activity between healthy control subjects and patients in the chronic phase after recurrent mTBI, hypothesizing that the patient group would score significantly lower in the cognitive test battery and show higher mean GABA concentration and longer mean CSP duration than healthy controls, indicating increased GABAB receptor activity; second, to evaluate the impact of atDCS over left primary motor cortex (M1) on GABA concentration and GABAB receptor activity in these groups. Here, we hypothesized that atDCS would reduce GABA concentration and GABAB receptor activity in both groups, with a potentially stronger decrease in patients.
Methods
Participants
In total, 17 patients with mTBI (24.2 ± 2.8 years (mean ± standard deviation [SD]), 15.4 ± 2 years of education, 2 women, 2 left-handed) were recruited from local sports clubs in Berlin and intranet advertisements on the website of the Charité University Hospital Berlin (Table 1). For diagnosis of individual mTBI, a standardized questionnaire was used. Diagnosis of mTBI required reporting of either confusion for less than 24 h and/or loss of consciousness for less than 30 min after head injury (American Academy of Neurology Practice, 1997).
mTBI, mild traumatic brain injury.
The patients with mTBI had to report sustaining at least two mTBIs (number of TBIs: 3.1 ± 1.6, range 2–7; time since last TBI in month 21.2 ± 13.5, range 7–54, patients with mTBI) taking place at least 6 months before study enrollment. None of the patients was involved in litigation over any TBI. As a control group, 22 group-wise matched (age, years of education, sex) persons (26.1 ± 5.4; 15.3 ± 1.8 years of education, 2 women, 2 left-handed) without a history of (m)TBI were recruited from the same local sports clubs or via intranet advertisements on the website of the Charité. All subjects had already been participating in an earlier study of our group. 40
All subjects fulfilled the following inclusion criteria: (1) normal findings on neurological examination; (2) no intake of medication that influences the central nervous system; (3) no signs of severe cognitive deficits (Mini Mental State Examination ≥26) 41 ; (4) no signs of relevant depression (Beck Depression Inventory ≤12). 42 Exclusion criteria comprised: (1) history of moderate or severe TBI (all groups) or history of mild TBI (control group); (2) epilepsy; (3) history of alcohol and/or substance abuse; and (4) attentional deficits.
The study was approved by the local ethics committee of the Charité University Hospital in Berlin, Germany. It was performed in accordance with the Declaration of Helsinki. All participants provided written informed consent.
Study outline
After enrollment, all subjects underwent medical examination, baseline cognitive testing, and completed a detailed questionnaire on Pittsburgh Steelers Post-Concussion Scale (PSPS) (Fig. 1). Subsequently, they participated in two separate experimental sessions (MRS; TMS), each of which comprised an atDCS and a sham condition; order of atDCS versus sham and MRS versus TMS was randomized between subjects.

Study outline. See main text for details. mTBI, mild traumatic brain injury; MMSE, Mini Mental Status Examination; PSPS, Pittsburgh Steelers Post-Concussion Scale; t0, pre-interventional measurements; MRS, magnetic resonance spectroscopy; TMS, transcranial magnetic stimulation; atDCS, anodal transcranial direct current stimulation; t1, post-interventional measurements.
Before (t0) and directly after 20 min stimulation (t1) (atDCS or sham), the respective measurement (MRS or TMS) was conducted. This procedure was chosen in line with previous studies that reported an increase in cortical excitability 43 and decrease of GABA concentration. 32
Baseline
Post-concussive symptoms
Post-concussive symptoms in the patients with mTBI and healthy control subjects were assessed by a German version based on a standardized questionnaire PSPS. 44 The PSPS aims to detect somatic (balance problems, nausea, headache), neuropsychiatric (irritability, sadness, nervousness, fatigue, trouble falling asleep), and cognitive symptoms (difficulties in concentrating, difficulties in remembering) that may occur after mTBI. The PSPS was completed by both groups, because there has been evidence that post-concussion–like symptoms are also reported by healthy subjects and are correlated with self-reported depressive symptoms. 45
Cognitive testing
A set of standardized cognitive tests was conducted to detect deficits in domains previously reported as impaired after mTBI. 40,46 –49 For verbal episodic memory, the German version of the Auditory Verbal Learning Test (AVLT) 50 was used to assess verbal learning ability (sum of trials 1–5 of word list learning; AVLT, sum 1–5) and retrieval from verbal memory, as tested by a delayed recall task 30 min later.
Processing speed was assessed with the Trail Making test (TMT) A and B. For TMT-A, participants were instructed to connect a set of 25 numbers as fast and as accurately as possible, for part B (TMT-B) to alternate between connecting numbers and letters as fast and as accurately as possible. Verbal fluency was assessed with the Regensburger Verbal Fluency Test, using “S” words and “G/R” words (alternating) for phonemic fluency, “food” and “clothes/flowers” (alternating) for category fluency.
For the Rey-Osterrieth Complex Figure Test, participants were asked to reproduce a complicated line drawing task, first by copying the figure freehand (recognition), and after a delay of 30 min, drawing it from memory (recall). This task examines visuospatial skills and episodic memory in the visuospatial domain. Digit span forward and backward (as taken from the Revised Wechsler Memory Scale) was used to assess working memory performance.
To control for participants' compliance and validity of performance, the reliable digit span (RDS) was calculated following Meyers. 51 None of the participants scored below the cutoff score (RDS ≤6 or RDS ≤7); see Schroeder and associates 52 for cutoff scores. Cognitive testing was administered in all but one patient with mTBI because he was a non-native German speaker. TMS and MRS data (see below) of this subject were included in all analyses. All cognitive tests were performed by a medical student who was trained by the lead neuropsychologist of the Neurology Department before the study.
Intervention
All subjects received separate TMS and MRS protocols. Within each of these protocols, subjects received atDCS on one day, sham stimulation on a different day (at least 7 days apart). Order of MRS and TMS sessions as well as order of atDCS versus sham within each session (MRS, TMS) was randomized between subjects. MRS and TMS were conducted consecutively and performed before (t0) and after (t1) atDCS and sham condition (Fig. 1). To exclude carryover effects, all measurements were separated by at least 1 week.
Stimulation
A constant direct current of 1 mA over M1 was applied using an MRI-compatible stimulator (DC-Stimulator Plus,® NeuroConn, Ilmenau, Germany). The anode sheathed with a 5 cm × 7 cm saline-soaked sponge was positioned over M1 using C3 of the 10–20 electrode system. 53 For reference electrode, a 10 cm × 10 cm saline-soaked sponge was used and placed over the right supraorbital region. The larger size of the reference electrode (cathode) was chosen to render the stimulation over the respective area functionally inefficient. 54,55
This setup is widely used in neurophysiological and clinical studies in both healthy subjects and patients. 32,56,57 The electrode positioning was verified using MR images (see below) in every participant. In both stimulation and sham condition, the current was gradually increased to 1 mA in the first 10 sec. For sham condition, the current was turned off after 30 sec and for atDCS condition after 20 min.
MRI and MRS
All anatomical T1-images (both groups) and fluid-attenuated inversion recovery-images (mTBI group) were evaluated by a board-certified neuroradiologist. No structural lesions were noted on visual inspection.
MR data acquisition
All MR images and spectra were collected on a 3 T Verio system (Siemens Healthcare, Erlangen, Germany) using a 32-channel receive-only head coil. Transmission of radiofrequency (RF) was performed with the body coil of the scanner. For planning and analysis purposes, anatomical images were acquired using a three-dimensional magnetization prepared gradient-echo sequence (MPRAGE) with an isotropic resolution of 1.0 mm, a repetition time (TR) of 2.3 sec, an echo time (TE) of 3.03 msec, an inversion time (TI) of 900 msec, and a flip angle of 9° degrees. A volume of interest (VOI = 22 × 22 × 22 mm3) was positioned in the left motor cortex, such that the motor hand area was encompassed (Fig. 2). 58 The transmitter RF voltage was calibrated for the individual OI, and first- and second-order shims were adjusted using FAST(EST)MAP. 59,60
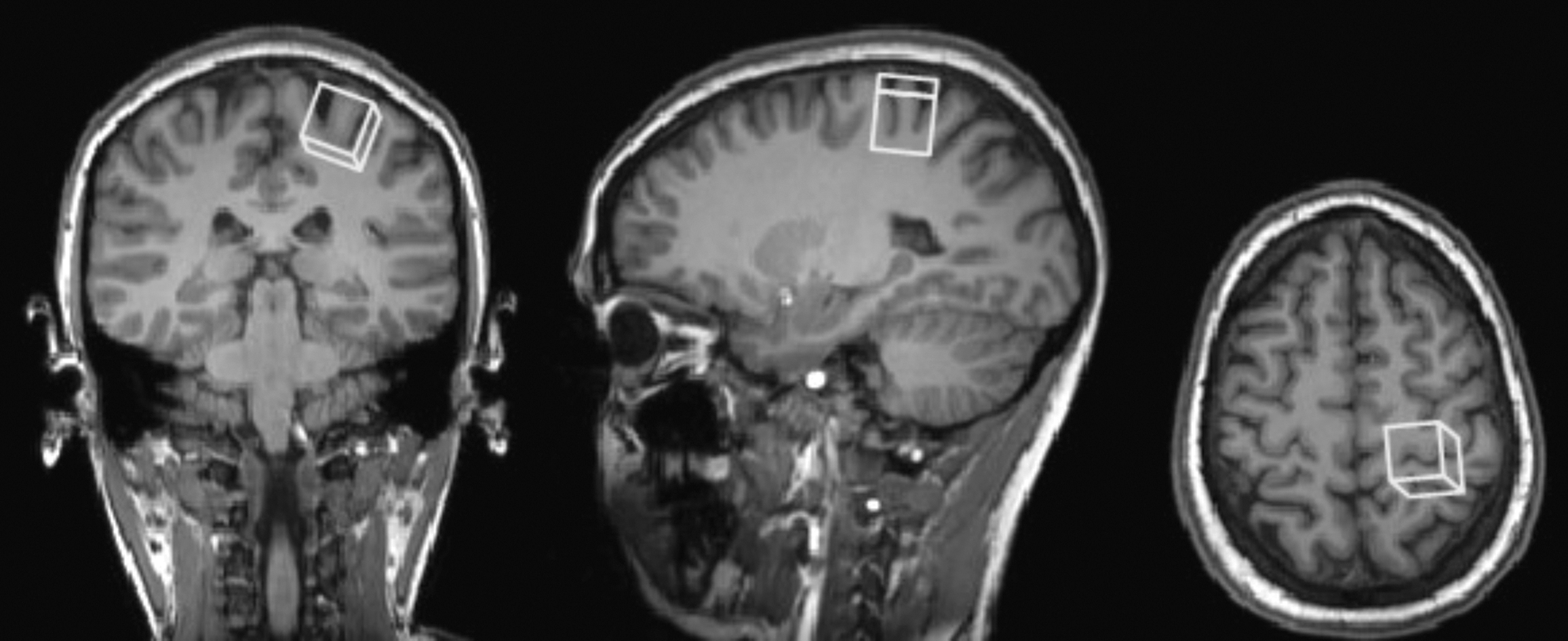
Location of voxel of interest in left motor cortex.
Single volume MR spectra were acquired using the spin echo full intensity acquired localized (SPECIAL) sequence with the following scan parameters: TR/TE = 3000/8.5 msec, number of averages (NA) = 256, spectral width = 2000 Hz, and Tacq = 1024 msec. 61,62 The implementation of the sequence included a scheme of variable power RF pulses with optimized relaxation delays (VAPOR) water suppression and outer volume saturation (OVS). 63 OVS was performed using six outer volume suppression slices placed around the spectroscopic VOI to saturate outside spins. An unsuppressed water signal was subsequently recorded (NA = 8) for eddy current correction and GABA quantification. MR spectra were measured before and after atDCS stimulation using identical settings.
After the onset of stimulation, resting state fMRI was performed using an echo planar imaging (EPI) sequence with 35 AC-PC oriented slices of 4 mm thickness, TR = 2.3 sec, TE = 30 msec, field of view = 192 × 192 mm2, matrix = 64 × 64, flip angle 90 degrees, acceleration factor 2. Scan time of the EPI scan was 5:52 min. It was followed by 5 min of rest (no data acquisition, but continuous stimulation) before the stimulation period was concluded with a second fMRI data acquisition.
MR data analysis and quantification
Before GABA quantification, MR signals from all 32 channels were weighted, combined, corrected for frequency drifts, and averaged using an in-house software package written in Matlab (The Mathworks Inc., Natick; MA). The resulting spectra were then analyzed using LCModel 64 with a simulated basis set containing 20 metabolites, using the water signal from the VOI as an internal reference. The resulting GABA amplitudes were corrected for relaxation using relaxation times at 3 T. 65,66
In addition, in vivo concentrations were adjusted for the amount of cerebrospinal fluid (CSF) in the selected VOI by segmenting the MPRAGE images using statistical parametric mapping (SPM8). Pixels in the VOI were then classified according to their probability calculated by SPM8 to belong to one of the tissue types: CSF, gray matter, or white matter. Note that errors in CSF estimation caused by the small chemical displacement of the metabolites and imperfections of RF pulse profiles were neglected, because the CSF fraction in the selected VOI was very small.
TMS
TMS was delivered through a figure-of-eight shaped coil (9 cm outer diameter of each wing) that was connected to a Magstim 200 stimulator (Magstim, Whitland, Dyfed, UK). Participants were sitting comfortably in a reclining chair. The coil was held tangential to the scalp with the handle pointing backward at an angle of 45 degrees to the interhemispheric fissure. The optimal position (“hot spot”) of the coil was the cortical representation area of the abductor pollicis brevis muscle of the contralateral hand. On the hot spot, a moderately suprathreshold stimulation intensity was leading to visible abduction of the respective muscle of the contralateral hand. The hot spot was then marked with a waterproof pen on the scalp of the subject.
Motor evoked potentials (MEP) of the respective muscle were recorded via surface electromyographic (EMG) activity using Ag/AgCl surface electrodes in a belly-tendon-montage. Raw MEP signals were amplified and digitized and then stored on a laboratory computer for later offline analysis. The bandpass filter was 5 Hz to 5 kHz (Digitimer). Data were digitized at an analog-to-digital rate of 5 kHz.
Resting motor threshold (rMT)
At the hot spot, rMT was defined as the stimulus intensity (in % of maximum stimulator output) that was required to produce an MEP of the respective muscle of at least 50 μV in at least 5 of 10 consecutive trials. 67
CSP
CSP duration was calculated at two TMS intensities. Ten single-pulse stimulations for each of the two TMS intensities (120% and 130% of rMT) were applied to the hot spot. Participants maintained a voluntary isometric contraction of the respective muscle at approximately 20% of their maximum EMG amplitude as determined during a maximum voluntary contraction by providing visual feedback from the surface EMG on a computer screen.
The CSP duration was defined as the time elapsing from the onset of the MEP until the reversion of voluntary tonic EMG activity. Detection of onsets and offsets was made with an in-house written automatic tool.
Statistical analysis
Normal distribution (histogram check, skewness value <|1|) was ascertained for all variables before using parametric tests.
Baseline
Post-concussive symptoms
To analyze group specific differences on the PSPS, the Student's t test for independent samples was computed.
Cognitive data
To allow for direct comparison of performance in different cognitive domains, single-test Z-scores (mean score of 0 and SD of 1) were generated using the formula:
Xmean and SD here refer to the healthy control subjects. This approach enabled direct comparison of performance in different cognitive domains. Z-scores were also used to compute Student's t tests for independent samples to analyze group specific differences in the cognitive profiles.
GABA concentration and TMS data
Measurements at t0 (GABA, TMS) were calculated by averaging the individual data across both t0 atDCS and sham condition. A paired samples t test was conducted to look for differences in t0 measurements between atDCS and sham condition. Group differences in MRS-derived GABA concentration and TMS-derived CSP duration were tested with the Student's t tests for independent samples. An outlier detection for rMT values (raw data) was performed following the method by Hoaglin and colleagues 68,69 to control for outlier effects on TMS data.
Intervention
To examine the effect of the condition (atDCS vs. sham) on the GABA concentration and TMS data, repeated measures analysis of variance (RM ANOVA) was conducted with factors TIME (before vs. after atDCS or sham) and CONDITION (atDCS vs. sham). Moreover, the between-subject factor GROUP was included in the model to analyze the effect of mTBI.
Explorative analyses
Spearman rank-order correlations were used to assess the relationship between baseline GABA concentration (mean) and baseline CSP duration (mean) versus number of mTBI, post-concussive symptoms, and time elapsed since the last injury. Further, the relationship between baseline MRS-derived GABA concentration (mean) and baseline CSP data (mean) and verbal fluency was assessed using the Pearson correlation. Correction for multiple analyses was applied.
For all statistical analyses, SPSS Statistics 22.0 (IBM Corporation, Armonk, NY) was used. The alpha value was set to 0.05.
Results
Baseline
Post-concussive symptoms
Average PSPS scores of patients with mTBI were 11.8 (SD = 12.8) and of healthy controls were 9.3 (SD = 14.7). Although the patient group showed generally higher PSPS scores, the difference between patient group and healthy subjects was not significant (t(37) = 0.58, p = 0.57).
Cognitive testing
As indicated by negative Z-values, the mTBI group performed trend-wise lower in most cognitive tests (Fig. 3). Student's t tests revealed significant differences between groups in verbal fluency tasks (uncorrected) (Table 2).
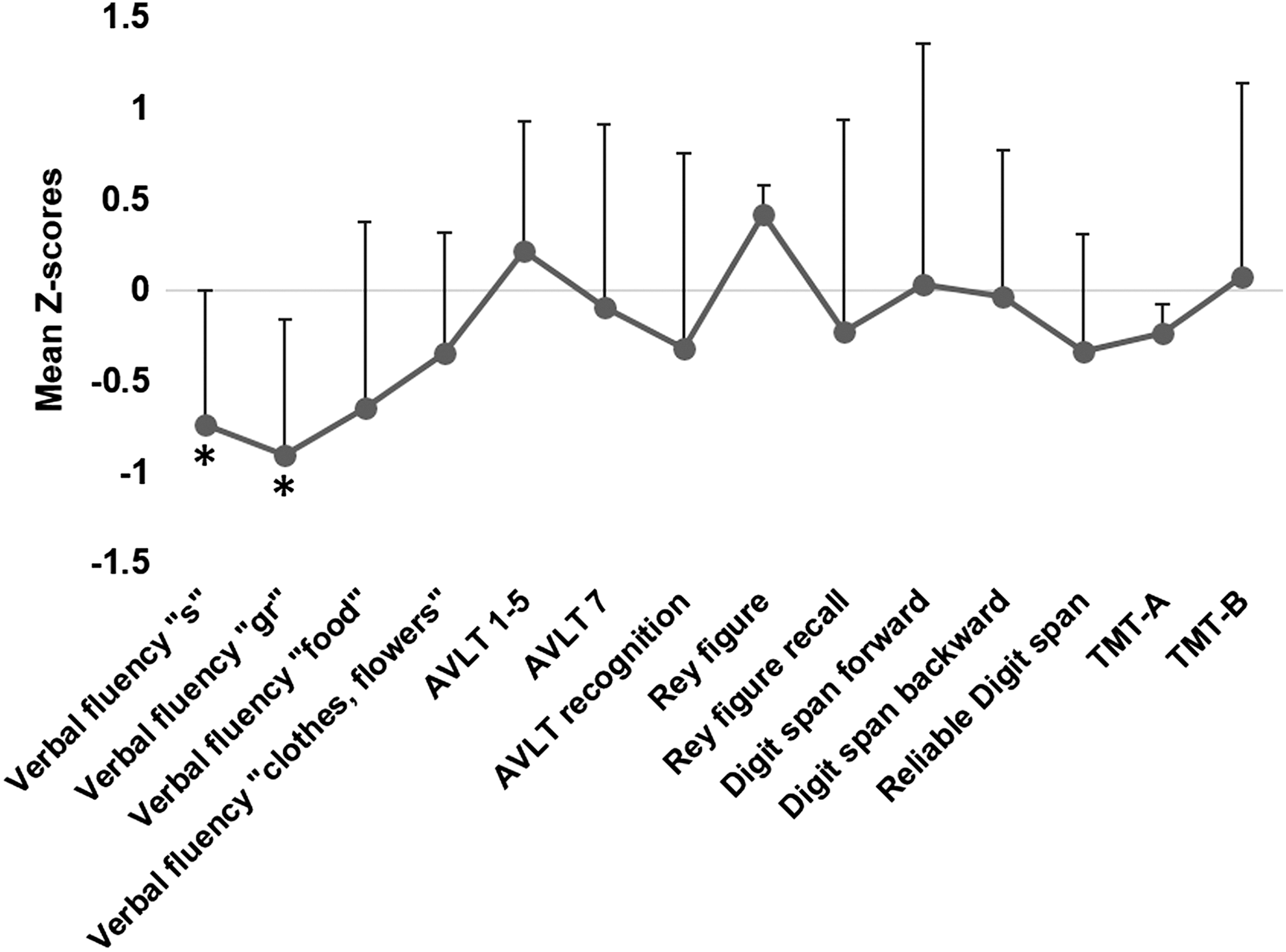
Cognitive profile of patients with mTBI. Mean Z-scores (error bar +1 standard deviation) of cognitive tests for patients with mTBI. AVLT, Auditory Verbal Learning Test; TMT-A/B, Trail Making Test A/B.
mTBI, mild traumatic brain injury; MMSE, Mini Mental Status Examination; BDI, Beck Depression Inventory; PSPS, Pittsburgh Steelers Post-Concussion Scale; TMT-A/B, Trail Making Test A/B; AVLT, Auditory Verbal Learning Test; RWT, Regensburger Verbal Fluency Test; GABA, gamma-aminobytric acid; t0, pre-interventional measurements; atDCS, anodal transcranial direct current stimulation; rMT, resting motor threshold; CSP, corticomotor silent period.
GABA concentration
Average GABA concentration across all participants was 1.51 mmol/L (SD = 0.32) in the t0 atDCS condition and 1.46 mmol/L (SD = 0.42) in the t0 sham condition. The difference was not significant (t(38) = 0.71, p = 0.48). Similarly, the GABA concentrations in control subjects (mean = 1.51 mmol/L, SD = 0.24) versus patients with mTBI (mean = 1.45 mmol/L, SD = 0.23) were not significantly different (t (37) = −0.75, p = 0.46; cf. Table 2).
TMS data (CSP)
No outliers regarding rMT values were found. Mean rMT across all participants was 39.4 (% of maximum stimulator output) (SD = 6.8) and 39.3 (% of maximum stimulator output) (SD = 6.0) at t0 atDCS and t0 sham, respectively, without significant difference (t(32) = 0.20, p = 0.53), and 40.4 (% of maximum stimulator output) (SD = 7.5) and 38.9 (% of maximum stimulator output) (SD = 5.0) for patients with mTBI and healthy control subjects, respectively, over all baseline rMT measurements at t0. The latter difference was not significant (t(33) = 0.69, p = 0.52).
Average CSP durations across all participants were 0.15 sec (SD = 0.03) and 0.14 sec (SD = 0.03) at t0 atDCS and t0 sham, respectively, without significant difference (t(34) = 0.63, p = 0.53), and 0.15 sec (SD = 0.02) versus 0.14 sec (SD = 0.03) for patients with mTBI and healthy control subjects, respectively, over all baseline CSP measurements at t0. As before, the latter difference was not significant (t(33) = 0.06, p = 0.95; Table 2).
Intervention
GABA concentration
Group specific effect of atDCS on GABA concentration
A 2 × 2 (TIME × CONDITION) RM ANOVA with the between-subject factor GROUP revealed no significant main effects for TIME (λ = 0.99, F(37,37) = 0.02, p = 0.88) and CONDITION (λ = 0.98, F(37,37) = 0.7, p = 0.41) on the GABA concentration (Table 3). In addition, no significant effect of the between-subjects factor GROUP was found (F(1,37) = 0.04, p = 0.84) (Table 3).
mTBI, mild traumatic brain injury; SE, standard error; GABA, gamma-aminobutyric acid; CSP, corticomotor silent period.
TMS data (CSP)
Group specific effect of atDCS on CSP duration
A 2 × 2 (TIME × CONDITION) RM ANOVA with the between-subject factor GROUP revealed a significant main effect for TIME (λ = 0.19, F(33,33) = 7.93, p = 0.008) on CSP duration. No significant main effect for the factor CONDITION (λ = 0.01, F(33,33) = 0.24, p = 0.63) was found (Table 3). In addition, no significant effect for the between-subjects factor GROUP was found (F(1,33) = 0.24, p = 0.63) (Table 3).
Explorative analyses
Correlation between baseline parameters (MRS, TMS) and cognition
We noted (for mTBI only) a significant positive association between number of mTBI and baseline GABA concentration (r = 0.57, p = 0.016 [uncorrected]) that remained significant after Bonferroni correction (number of comparisons = 3, critical p = 0.0167) (Fig. 4). For a detailed overview, see Table 4.

Associations between gamma-aminobutyric acid (GABA) concentration and number of mild traumatic brain injuries (mTBI). Corr, correlation; Md, median.
TBI, traumatic brain injury; GABA, gamma-aminobutyric acid; CSP, corticomotor silent period.
Bivariate Pearson correlation for verbal fluency (s and gr words) and baseline GABA and CSP.
Discussion
Patients after recurrent mTBI showed slight deteriorations in cognitive abilities, reaching significance for verbal fluency, as already reported in a previous study by our group. 40 Within the patient group, a significant association between higher GABA concentration and higher number of mTBI was noted. No significant differences in GABA concentration in M1 and in GABAB receptor activity, as indicated by CSP duration, between patients with mTBI and healthy control subjects were found at baseline, however. Moreover, atDCS did not significantly alter GABA concentration or GABAB receptor activity in either of the groups.
GABA concentration and GABAB receptor activity in mTBI
In recent years, cognitive sequelae after recurrent mTBI have been described in young and old patients. 70 –73 For example, patients scored significantly lower in verbal fluency tasks. 70,71 This slight deterioration in cognitive abilities in the first years after mTBI may be based on direct structural and functional deficits from recurrent mTBI, including lower cortical thickness within the right temporal lobe and left insula, 40 decreased cellular integrity, particularly in the corpus callosum, 74 and decreased functional connectivity within the motor-striatal network in patients with mTBI compared with healthy control subjects. 75
In older age, these structural and functional changes may lower the threshold for developing mild cognitive decline and AD. This hypothesis is supported by epidemiological studies that reported a correlation between history of mTBI and an earlier onset of AD, 9 indicating a reduction of individual cognitive reserve ability (for review, see Moretti and coworkers 76 ). A mechanism underlying this association may be a decreased ability to induce neuroplasticity via training, an alteration that can already be found in patients at a younger age. Here, lower ability to induce LTP-like cortical plasticity in patients after recurrent mTBI has been documented, possibly because of chronically increased GABAB receptor activity in these patients. 27,29,73 This hypothesis is supported by studies in animals demonstrating that chronic elevation of GABA has an adverse effect on memory functions in rats. 77,78
Evidence for an increased synthesis of GABA in the acute phase after TBI only stems from animal studies so far that noted increases in GABA concentration. 77,79 In humans, only two studies assessed GABA concentration (Tremblay and associates, 23 present study), both in the chronic phase after recurrent mTBI (36.1 ± 24.7 [SD] months after last mTBI in Tremblay and associates 23 ; 21.2 ± 13.5 [SD] months in the present study). Both studies noted subtle changes in GABA concentration, albeit only in exploratory analyses. A lack of differential findings for GABA concentration between groups in the present study may also occur because of a lack of significant differences in the PSPS questionnaire between groups, which has also been indicated by Tremblay and associates, 23 who did not find altered GABA concentration in participants with asymptomatic concussions.
In line with Tremblay and colleagues, 23 Powers and coworkers, 80 and Chistyakov and associates, 30 the present study revealed no baseline differences in GABAB receptor activity, as determined by CSP duration. Other studies found decreased CSP duration 81 or increased CSP duration. 26,27,29,73 These inconsistent results may be because of the impact of sample characteristics, such as age, sports practiced by participants, number of mTBI, injury, and symptom severity and type of injury, as well as time since last mTBI. 26 –30,73,80,81
A consistent pattern of any of these characteristics did not emerge so far, however. For example, even within the group of studies on chronic mTBIs, increases, 26 –29,73 decreases, 30 and, as in the present study, no alterations in CSP duration/GABAB receptor activity 23 were detected. Future studies assessing GABA concentration and GABAB receptor activity repeatedly after mTBI—i.e., in the acute, subacute, and chronic phase after the traumatic event—might be able to shed more light on the issue of time-dependent changes in GABA-related parameters.
Impact of atDCS on GABA concentration and GABAB receptor activity
Previous reports suggested an effect of atDCS on GABA concentration and GABAB receptor activity. 32,33,35 More specifically, a significant reduction in GABA concentration 33,35 and a significant decrease of GABAB receptor activity 39 in M1 after atDCS in healthy participants has been found. Other studies, however, could not confirm these findings and reported no effect of atDCS on GABAB receptor activity. 82 A crucial factor may be the high inter-individual variability in the responsiveness to tDCS, which has been emphasized by a variety of recent reports. 83,84 We observed no atDCS-induced modulation of GABA concentration and GABAB receptor activity. Note, however, that atDCS has been shown repeatedly to modulate GABAA receptor activity—i.e., decrease of short-interval intracortical inhibition, 34,81,85 a parameter that was not evaluated in the present study.
Given that in the present study more than twice as many healthy subjects were examined as Stagg and colleagues 35 did, it is unlikely that our study was underpowered to detect atDCS-induced changes in GABA concentration. Of note, GABA concentration in Stagg and colleagues 35 was assessed with a different MRS method—MEscher-Garwood-Point RESolved Spectroscopy (MEGA-PRESS) 34,35,86,87 versus SPECIAL sequence in the present study. The SPECIAL sequence with very short echo time is less selective for GABA but has a higher signal-to-noise ratio than MEGA-PRESS. 88 Both sequences are established methods, however, to quantify the identical biochemical species in a given area of the brain, and within their respective uncertainties, both will provide consistent results. Accordingly, a large study showed positive linear association (correlation = 0.58, p < 0.05) between results obtained for GABA from the two sequences. 88,89
Further differences between Stagg and associates 35 and the present study include the duration of tDCS, with 10 min of stimulation in Stagg and associates 35 versus 20 min in our study. While it seems unlikely that longer stimulation diminishes atDCS-induced GABA concentration shifts, no reports have yet directly compared the impact of stimulation duration on MRS-derived metabolite levels.
Note, however, that most rehabilitation studies use at least 20 min of tDCS to improve motor performance, 53,90,91 a mechanism that was proposed to rely on changes in GABA concentration. 92 Also, the size of the reference electrode in our study differed from that of Stagg and coworkers. 34,35,86,92 The setup used in the current study is widely used in neurophysiological and clinical studies in both healthy subjects and patients and yields (for anodal stimulation) an up-regulation of cortical excitability 93 and down-regulation of GABA concentration. 32 Further studies that compare different stimulation protocols and different MRS sequences are necessary to resolve these open issues.
Limitations and strengths
Several limitations should be considered when interpreting the present findings. First, relying on self-reports concerning number of mTBI and symptoms might over- or underestimate mTBIs. Standardized and validated questionnaires were used, however, which is the current standard procedure in mTBI research. 7,9,23,28,47,81,94 –99 Second, controls were recruited from the same sports teams; thus, sub-concussive events, which were not detected by our questionnaire, may have led to metabolite alterations, 100 and thus diluted differences between groups. The advantage of choosing individuals from the same sports club was that baseline differences between groups, except for history of mTBI, were minimized. Future studies should address this question by additionally including a control group that does not participate in contact sports.
Third, the questionnaire PSPS used in the present study assessed whether participants showed symptoms in the last month and did not specifically account for deterioration of any pre-existing symptoms after mTBI, which makes it difficult to differentiate between symptoms from the concussion and pre-existing symptoms that are also frequently found in the general population—e.g., sleep disturbances, irritability, or sadness. Nevertheless, the PSPS questionnaire and its variations are widely used in clinical studies 44,101 and national football leagues 102,103 to monitor symptoms. Strengths of this study include the comprehensive assessment of both GABA concentration and receptor activity and the impact of atDCS on these measures in both healthy control subjects and in patients in the chronic phase after recurrent mTBI.
Conclusion
The present examination did not detect significant differences in GABA concentration or GABA receptor activity between patients after recurrent mTBI and healthy control subjects, although an association between higher GABA concentration and higher number of mTBI within the patient group was noted. Moreover, no modulation of GABA concentration or receptor activity by atDCS was detected, in contrast to several previous studies. Specifics of experimental design and analysis but also characteristics of the respective samples may account for these differential findings and should be addressed in future larger studies. Given the high prevalence of mTBI and previous reports on an association with higher incidence of AD, additional techniques to improve neuroplasticity should be investigated, including repetitive TMS, 31,104 pharmacologic treatments, 105 and regular physical activity. 106
Footnotes
Acknowledgments
This work was supported by grants from the Deutsche Forschungsgemeinschaft (AF: 379-10/1; 379-11/1; DFG-Exc-257), Bundesministerium für Bildung und Forschung (AF: 01EO0801, 01GQ1424A, 01GQ1420B). JL is participant in the Charité Clinical Scientist Program funded by the Charité Universitätsmedizin Berlin and the Berlin Institute of Health.
Author Disclosure Statement
No competing financial interests exist.