
Abstract
The influence of complications and comorbidities on the outcome of patients with traumatic spinal cord injury after early surgery is unclear. The aim of the current study was to analyze the influence of previous comorbidities and common complications on motor function outcome of patients with traumatic spinal cord injury if early surgery was performed. All patients with a traumatic spinal cord injury who were initially surgically treated in our hospital in the period from January 2008 to December 2013 were included in this study. Epidemiological data and previous comorbidities (cardiovascular, pulmonary, metabolic, spinal) were documented. A neurological assessment was performed using the American Spinal Injury Association (ASIA) score. Retrospectively, patients' personal data (age, gender, comorbidities) and clinical data (complications, ASIA score, motor function) were analyzed statistically. A total of 133 patients met the inclusion criteria. The level of spinal cord injury ranged from C3 to L4. Motor function was improved from 51.5 ± 24.8 to 60.1 ± 25.0 (improvement: 25.7%). The most common complications were urinary tract infection and pneumonia. There is a significant relationship between a lack of previous spinal comorbidities and a better outcome in terms of motor function. No other comorbidities or complications showed any effect on motor function outcome. The current study shows that motor function was able to be improved in patients who were given early surgery after a traumatic spinal cord injury. Common complications as well as previous cardiovascular, pulmonary, and metabolic comorbidities do not impair motor function outcome. The final motor function score is reduced if patients have previous spinal comorbidities.
Introduction
A
Current literature shows that an early operative treatment of these patients within 12 h improves neurological outcome. 3 Further, the complication rate increases if surgery is performed later. 4 Therefore, early surgical treatment is outlined as best medical practice in a summary of a series of systematic reviews, 5 and is recommended by current guidelines. 6 However, prospective randomized controlled trials on that topic are not currently available.
Current guidelines on acute trauma care recommend the treatment of patients with traumatic spinal cord injury in specialized centers. 7,8 Here, interdisciplinary treatment is able to be administered, and the length of stay in the hospital is able to be reduced. 9 The frequency of common complications when treating patients with spinal cord injuries such as pneumonia, urinary tract infection (UTI), 10 thrombosis, and embolism 11 is lower in specialized centers. 9
The aim of the current study was to analyze the influence of previous comorbidities and common complications on the motor function outcome of patients with traumatic spinal cord injury if early surgery was performed.
Methods
The current study was approved by the ethical committee in charge (Ethics Committee of the State Medical Association Rhineland-Palatinate, Mainz, Germany).
All patients with an acute traumatic spinal cord injury who were initially surgically treated in our level I trauma center, which is also a specialized treatment center for spinal cord injuries, in the time period from January 2008 to December 2013 were included in this retrospective cohort study. To obtain a more homogenous cohort of patients, those with nontraumatic spinal cord injuries and all patients who had been initially treated in other hospitals were excluded from the current study. Patients with previous neurological deficits and all patients treated conservatively were also excluded from this study.
The epidemiological data of the patients were documented as a standard procedure in our trauma center. Further, previous comorbidities were documented as mentioned by the patient at any time point during hospital stay or as found in former medical documentation. The initial neurological assessment was performed during emergency room treatment according to the established so-called American Spinal Injury Association (ASIA) score 12 (International Standards for Neurological Classification of Spinal Cord Injury). The final ASIA score was calculated during the last 3 days of the patients' hospital stay. The vital capacity was initially determined on the intensive care unit in the first few days after surgery using a spirometer (Spirotest, Riester, Jungingen, Germany). The final vital capacity was measured during the last 3 days of the patients' hospital stay using the same method.
Retrospectively, patients' personal data (age, gender, comorbidities), clinical data (level of spinal cord injury, pathology of spinal cord injury, concomitant injuries), as well as diagnostic data (ASIA score, lung function) and complications that occurred during the patients' stay at our hospital were analyzed anonymously. The improvement of motor function was calculated based on the ASIA score as described earlier
13
:
The outcome was calculated separately for the three different categories – motor function, light touch, and pin prick discrimination – in every patient. Anal sensory score measurements were not analyzed, because prognostic relevance is questionable. 14
Statistical analysis
Statistical data analysis was performed using SPSS Statistics 22.0 (IBM Corp, Armonk, NY). In the case of metric variables, the results are described using distributional parameters such as arithmetic means, standard deviations, and ranges. The results concerning categorical variables are given as absolute and relative frequencies. An analysis of associations was performed using Mann–Whitney U test or Fisher's exact test. In all significance tests for associations a p value <0.05 was considered to be statistically significant.
Results
In the period from January 2008 to December 2013, a total of 133 patients (male: 104; female: 29) met the inclusion criteria. The mean age of the patients was 50.5 ± 21.2 years (range: 13.0–97.0 years). Patients had various comorbidities previous to traumatic spinal cord injury as listed in Table 1.
Except spinal tumors.
COPD, chronic obstructive pulmonary disease.
The main trauma mechanisms were falls from a height of ≤3 m (n = 49; 36.9%) followed by falls from a height >3 m (n = 37; 27.8%) and road traffic accidents involving motorbikes (n = 20; 15.0%) or cars (n = 16; 12.0%). Different pathologies that hich cause spinal cord injury were provoked by these trauma mechanisms (Fig. 1). Spinal cord injury was classified complete in 55 patients (44.0%) and incomplete in 78 patients (56.0%). Most spinal cord injuries (60 cases) were located in the cervical spine, whereas the level of spinal cord injury ranged from C3 to L4 (Fig. 2A).
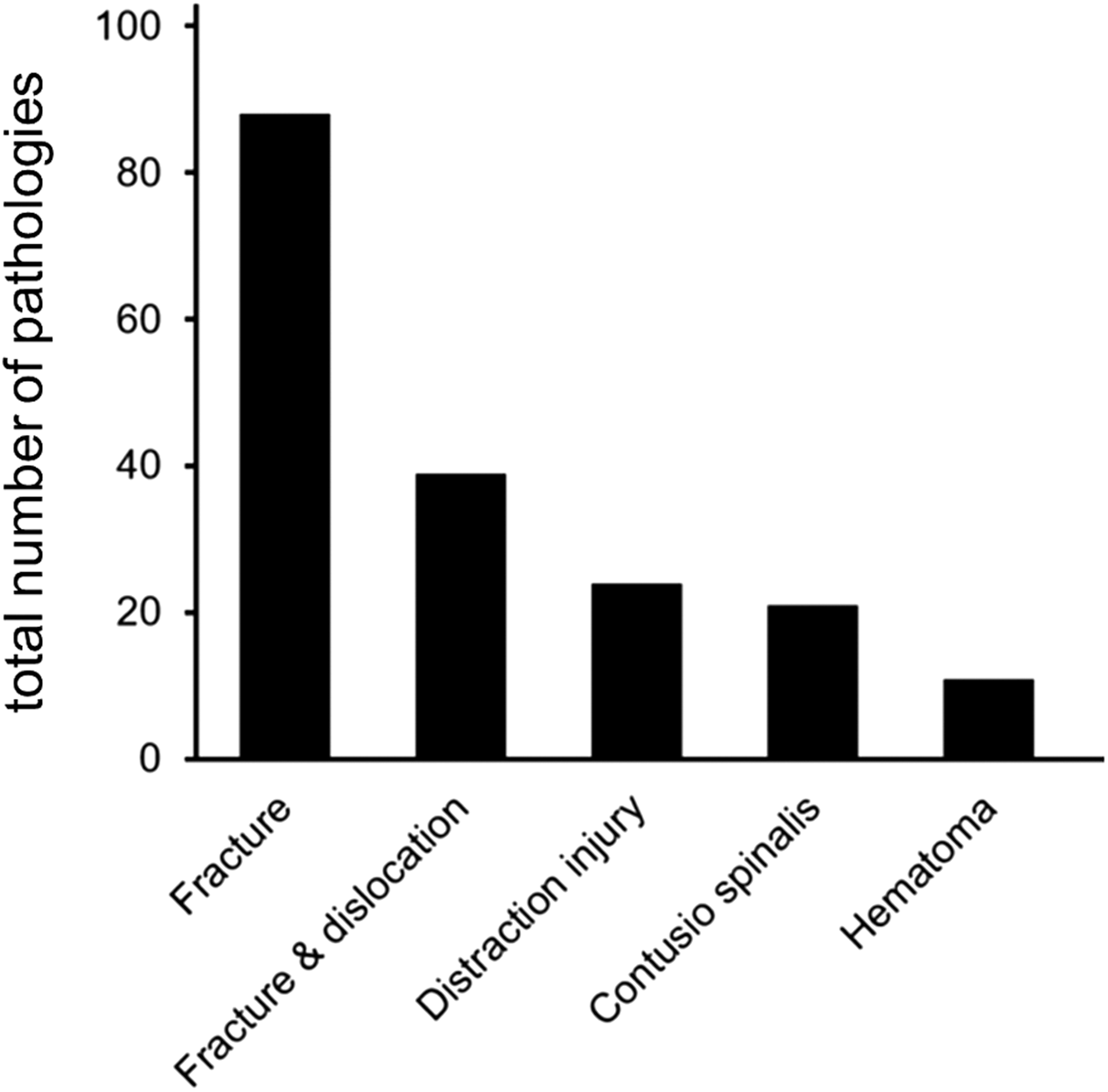
Number of pathologies leading to traumatic spinal cord injury.
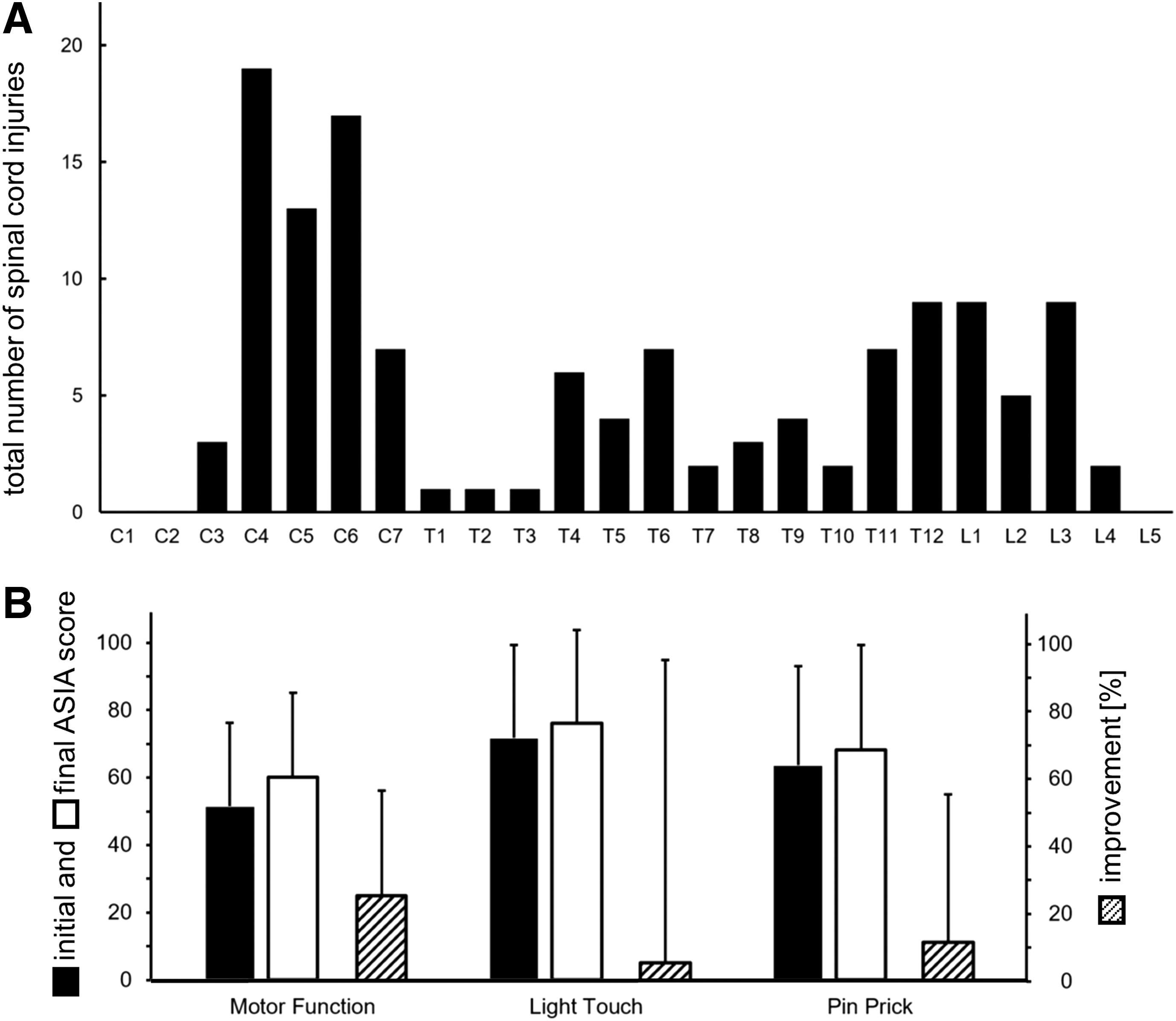
Number of spinal cord injuries at various levels
The initial mean motor function was 51.5 ± 24.8 (Fig. 2B), and the initial vital capacity was 1.44 ± 0.87 L. As a standard procedure, we aim to perform earliest surgical spinal stabilization and decompression by laminectomy after the patient's vital signs are stabilized. In 25 out of the 133 patients included in this study, early surgery within 12 h after arriving in our emergency room was not possible because of insufficient circulation and/or increased intracranial pressure. A total of 108 patients could be prepared for early surgery. The mean time between the patient arriving in our emergency room and start of surgery was 4.2 ± 3.9 h (n = 108). Overall mean time (n = 133) to surgery was 22.1 ± 56.6 h (range: 0.8–362.5 h). In addition to the dorsal spinal stabilization an additional laminectomy was performed in 90 cases.
A further analysis of the two subgroups (108 patients with immediate surgery vs. 25 patients with delayed surgery) compared the groups in terms of distribution of age, gender, level of injury, and previous comorbidities. The difference in these parameters was not significant between the two groups. However, the 25 patients who only could be prepared for delayed surgery had significantly more severe concomitant injuries, such as traumatic brain injury, as well as multiple fractures (long bones, pelvis), hematothorax, or blunt abdominal trauma causing hemorrhagic shock.
After an initial stay at our intensive care unit as recommended by current guidelines, 6 all patients were transferred to a highly specialized station for patients with spinal cord injury in the Department of Paraplegiology where interdisciplinary treatment and rehabilitation was performed. The mean overall stay in our hospital was 122.8 ± 100.4 days (range: 2.0–744.3 days).
The most common complications were UTIs (n = 77; 57.9%) and pneumonia (n = 41; 30.8%; Fig. 3). The pathogens that most frequently cause these infectious complications are listed in Table 2. There was no significant association between occurrence of any complication listed in Figure 3 and the level of spinal cord injury or previous existing comorbidities.
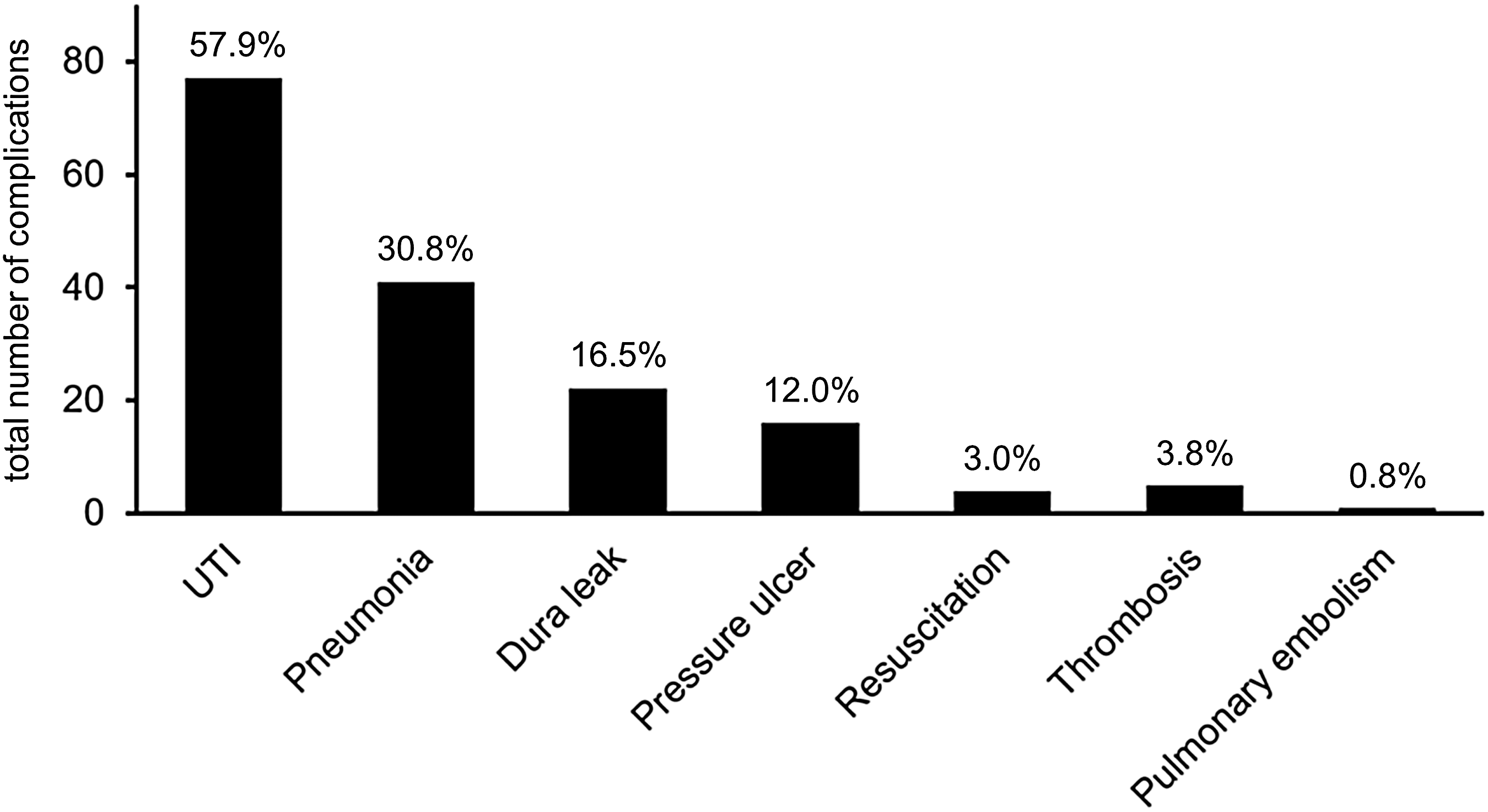
Number of most common complications after traumatic spinal cord injury.
A dura leak was seen in 22 (16.5%) cases. The frequency of dura leaks was highest in the lumbar (n = 8; 30.8%) and thoracic (n = 12; 25.5%) regions. Only two dura leaks were seen in the cervical spine (3.3%). Most of the dura leaks were treated by sealing with a fibrinogen/thrombin patch (TachoSil, Baxter, USA; n = 12; 54.5%), suturing the dura (n = 8; 36.4%), or reconstruction with a patch from the femoral fascia lata in one case.
On discharge from hospital, the mean motor function was scored 60.1 ± 25.0 (Fig. 2B). Therefore, mean improvement during hospital stay was best for motor function (25.7%) compared with the mean improvement of light touch (5.5%) and pin prick (12.0%) testing (Fig. 2B). Motor function improvement was best if traumatic spinal cord injury occurred in the lumbar region (37.9 ± 31.6%) (Table 3) or in the cervical region (30.3 ± 31.1%) (Table 3). In 69.2% and 26.7% of patients who had a traumatic spinal cord injury in the lumbar spine or in the cervical spine, respectively, the ability to walk was achieved at discharge from hospital (Table 3). Therefore, 41 patients were able to walk at the end of their hospital stay (Table 3). A total of 27 of these patients needed a walking aid (Table 3).The final mean vital capacity was 2.30 ± 0.86 L.
Further statistical analysis showed that there was a significant (p < 0.05) relationship between a lack of previous comorbidities of the spine and a better outcome in terms of motor function (Table 4). No other comorbidities or complications showed any effect on motor function outcome (Table 4).
Except spinal tumors
UTI, urinary tract infection.
Discussion
In the current study, the main trauma mechanisms leading to a traumatic spinal cord injury were falls from different heights. Road traffic accidents involving motorbikes or cars are less common as a cause of traumatic spinal cord injuries as confirmed by a United States multicenter study including 315 patients. 10 Most spinal cord injuries occurred in the cervical spine as previously described in an analysis based on the database of the German Trauma Registry. 2
As a standard procedure, we attempt to provide surgical treatment of patients with traumatic spinal cord injury by the means of dorsal stabilization and decompression as early as possible. This approach is recommended by current literature, 3 –5 even though the first prospective controlled multicenter trial on this topic is still underway. 15 The current study showed that 25 patients could only be prepared for delayed surgery. The reasons for delayed surgery were severe concomitant injuries making a patient's status unstable, and thus causing early decompression to aggravate the acute life-threatening situation.
The most frequent complications in patients who underwent early surgical treatment, which have been documented in the current study, were UTIs, pneumonia, and pressure ulcers. These complications are common in traumatic spinal cord injury care. 10 Our complication rate of UTIs is higher than data from another center that specialized in the treatment of spinal cord injury. 10 This may be explained by our regular screening procedure for pathogens in the urine. Contamination of >100,000 colony-forming units per mL is deemed to be an UTI. Not all of these patients have to be treated by administration of medication. The complication rates for pneumonia and pressure ulcers analyzed in the current study are in the same range as reported previously. 10 Maung and coworkers could show that the occurrence of venous thromboembolism after spinal cord injury is correlated to the level of injury, 11 and is highest in the upper thoracic region and lowest in the upper cervical region. However, in the current study there was no association between the level of spinal cord injury and the occurrence of any complication.
In 16.5% of the patients, a dura leak was identified. This high frequency of dura leakages after traumatic spinal cord injury is confirmed by another current study that found dural tears in 13.2% of the cases. 16 In the current study, the risk for a dura leak was highest if the injury was located in the lumbar region of the spine as described previously. 17 Most of the identified dura leaks could be sealed by a fibrinogen/thrombin patch. This technique has been described previously for spinal dura leaks 18 as well as after craniotomy. 19 No further complications of this procedure were documented in our study. However, if the damage of the dura increases, suture or even reconstructions have to be performed in single cases.
Directly following traumatic spinal cord injury, neurological deterioration may occur for several reasons. Many parameters such as growing hematoma, ongoing ischemia or hypoxia, or electrolyte shifts, as well as formation of free radicals and inflammatory mediators 20 contribute to the neurological outcome at this initial time period. According to the literature, the overall outcome for patients with spinal cord injury is significantly improved by rehabilitation. 21 Improvement in motor function during the rehabilitation process seems to be of major import for patients with spinal cord injury. In the current study, motor function shows the best improvement during the patient's stay in hospital. Motor function improvement was best if spinal cord injury was located in the lumbar level. A majority of these patients were able to walk after rehabilitation even if every second patient needed a walking aid. Sensory function as demonstrated by light touch and pin prick testing did not increase that much. We therefore focused on motor function for further analysis of the influence of comorbidities and complications, even if subjective quality of life was not directly associated with motor function. 21
The literature refers to the impairment of the neurological outcome if infectious complications such as UTIs and pneumonia occur. 22 These findings were not able to be supported by the current study, because no relationship between any complications and a reduced improvement in motor function outcome could be detected. Complications such as thrombosis and pulmonary embolism were rare in the current study as described previously. 11 Therefore, correlation analysis was not possible for these complications.
Patients with traumatic spinal cord injury who had previous spinal comorbidities such as ankylosing spondylitis, herniated discs, or spinal stenosis have significantly reduced improvement in motor function during their stay in hospital according to the current study. Unfortunately, developing subpopulations based on the different entities of spinal comorbidity for further analysis was not possible because of the overall group size (14 patients with spinal comorbidities). Because pathophysiological associations between previous spinal comorbidities and final motor function after rehabilitation remain unclear, further prospective studies must analyze this relation. Such a continuative analysis was not possible in the current retrospective study, because comorbidities were only documented from the patients' medical history and not verified on a further diagnostic level. Therefore, the exact location of the spinal pathology (level and site), or the severity (grading, scoring) as well as previous therapies outside our hospital (conservative or surgical) could not be sufficiently determined.
Therefore, the current study is limited to some extent because of its retrospective design. Further, the monocentric setting of the study allowed us to have a more homogenous group of patients according to early surgical treatment; on the other hand, however, the number of patients to be included in the analysis was restricted. Therefore, transferring the findings to other settings and populations should be performed carefully.
Conclusion
In conclusion, the current retrospective analysis shows that motor function improvement was 25.7% in patients who received early surgery after a traumatic spinal cord injury. Common complications such as UTIs and pneumonia as well as previous cardiovascular, pulmonary, and metabolic comorbidities do not impair the motor function outcome. The final motor function score is reduced if patients have previous spinal comorbidities such as ankylosing spondylitis, herniated discs, or spinal stenosis.
Footnotes
Acknowledgements
The authors thank Johannes Gladitz for his statistical expertise, Claudia Thompson for her orthographical revision of the manuscript, and Albert Besseling for his management of the ASIA scores database.
Author Disclosure Statement
No competing financial interests exist.