
Abstract
Major goals of rehabilitation and health interventions in people with spinal cord injury (SCI) are to improve functional independence, increase social participation, and enhance quality of life (QOL). Determining functional areas perceived by consumers as most important can assist in research prioritization, planning for delivery of health services, and policy development. Five high priority areas of functioning for the SCI population (arm/hand use, walking, bladder/bowel control, sexual function, and relief of pain) were chosen to determine the preferences for these five attributes. A discrete choice experiment was conducted involving 151 persons with SCI sampled from Australia and the United States of America. Consistent with prior research, arm/hand function had the highest preference, with odds ratios of subjects being 44–76% more likely to choose arm/hand function over the other four functions. Preference for normal arm/hand function was found to be significantly more preferred by the group with paraplegia compared with those with tetraplegia; that is, retaining and not trading off existing arm/hand function for other improved functions. There were no significant differences found in preferences between bladder/bowel function and walking or elimination of pain, although walking was preferred in earlier (≤ 10) post-injury years and pain amelioration became more important with a longer duration (>10 years) post-injury. Sexual function had the lowest preference when traded against the other four functions. Understanding the functional preferences of persons with SCI will help to inform future research design, as well as enabling successful translation of research into practice and health policy, meeting the needs of people with SCI.
Introduction
S
Given the importance of optimizing QOL following SCI, it is essential that the areas perceived as most important, by individuals living with SCI, to achieving a high QOL with social participation, are determined. 6 Dijkers 7 categorized QOL into three groups, as follows: 1) subjective well-being, 2) achievements, and 3) utility. Subjective QOL refers to people's satisfaction with various life domains, such as health; relationships; and emotional, social, and physical function, including happiness/satisfaction with their living situation and finances. 8 Determining priorities for individuals with SCI can be established by examining factors such as the individual's needs and wants, and the perceived importance of various life domains. 6,7 This information can inform the choice of research priorities that will ultimately lead to improved QOL for the person with SCI.
Involving consumer participation in decision making has increasingly been shown to be an important strategy for improving health outcomes in people living with chronic disease. 9 Increased attention has been given to the inclusion of a “client-centred assessment and treatment” framework into healthcare, whereby the patient's perspective and input is incorporated into the decision-making process. 10,11 It has been shown that persons are more likely to be proactive in their health management if they are involved with the therapeutic process, leading to benefits such as increased satisfaction and engagement, as well as improved cognitive and affective outcomes. 9,12,13 In addition, prioritizing areas to be researched has become an area of interest because of high demand for evidence-based resources, combined with limited research resources. 14,15
Given the challenges faced by people with SCI and limited resources, research prioritization will arguably allow resources to be focused on research areas of greatest demand and benefit. 16 This is important in order to avoid mismatches in health research priorities between consumers and professionals, which may result where there is limited input and participation from consumers. 6,16,17 For example, following acute SCI, muscle paresis or paralysis is the most obvious impairment and often the first focus of questioning by patient and family about predicted future functioning. Further, the need for assisted mobility, such as use of a wheelchair, may be seen as representative of being disabled to the outside world because the ability to ambulate over various terrains is an important factor in being able to engage with one's environment. 11 With this perspective in mind, it is a common belief that loss of the ability to walk is the chief concern for people with SCI. Perhaps as a consequence, a major emphasis of medical research in SCI has focused on recovery of walking function, with prime importance given to finding a “cure” for paralysis. 18 However, walking is not necessarily viewed by the majority of people with SCI as the most important functional priority, nor the most desirable to regain. 18 Previous research has clearly shown that recovery of arm and hand function was perceived to be the highest priority for people with tetraplegia, whereas improvement of sexual function was most important for those with paraplegia. 18 In a systematic review of 11 studies investigating functional priorities, Simpson and colleagues 6 found that bowel/bladder function, upper and lower extremity function, and sexual function comprised the domains ranked in the top 25% of what were perceived as the most important priorities for functional recovery by the SCI population in general. However, most studies employed ranking methodology to determine priorities. 6 For example, functions were ranked in order of their importance for the participants to regain. Although this provided an improved understanding of perceived functional priorities for consumers with SCI, ranking of the priority of different health functions does not fully capture an individual's valuation (of the functions), because valuation will depend not only on the characteristics of an attribute (e.g., arm function), but also on its quality/levels (impaired vs. normal). 19 Although ranking methodology provides a valid order for priorities, the relative difference in weights between the prioritized health functions could have been either very small or very large. 20
Discrete choice experiment/model (DCE) is an attribute-based measure of benefits that considers both attributes and levels, which can be applied to determining functional priorities, and hence overcomes limitations of ranking data. DCE is a valid and reliable approach that has been used to quantify patient preferences in healthcare, 21,22 and is a commonly used strategy in health economics research. 23 DCE is a quantitative technique used to elicit individual preferences, and data gathered employing DCE provides information on how individuals value the selected attributes through their stated choice over different hypothetical alternatives. 24 This model is based on economic theory that assumes that people have clear preferences for goods or services and are able to choose one type of good or service in preference to another. In doing so, individuals will make trade-offs between attributes and provide information with regard to their relative preference for certain attributes. 22 Economic theory assumes that individuals make rational consumption choices when they are faced with limited resources. That is, from among the options, the consumer will attempt to pick the best one, and “utility” is the measure used to demonstrate the level of satisfaction with various combinations of consumer goods and/or services. Therefore, the term “utilities” is synonymous with preferences, with more preferable outcomes associated with greater utility. 25
The current study aimed to determine priorities (or preferences) for key functions/attributes of people with SCI through using a discrete choice model. The DCE was designed to obtain information from people living with chronic SCI on functions/attributes perceived to be important, utilizing a hypothetical scenario of undergoing treatment for their SCI. The background scenario made clear that from the treatment, the outcome alternatives may have either a positive or negative effect, influencing the person's choices. The choices made by the participants provides a database from which their priority choices of a range of functions/attributes can be determined, as well as providing information regarding their preference for one function relative to another. The study also explored whether cultural differences existed between samples from Australia and the United States of America in their preferences for the functions/attributes. In addition, the influence of demographic and injury characteristics was examined.
Methods
Participants
Participants included 151 adults with SCI (104 male; 47 female) having a mean age of 48.3 (SD = 13.2) years. Of these, 79 participants had paraplegia and 72 participants had tetraplegia. Seventy-eight had incomplete lesions with preservation of sacral sensation, determined by using four previously validated questions by Harvey and colleagues. 26 Participants in Australia were recruited through advertising in support group newsletters and organization web sites, including Spinal Cord Injuries Australia (SCIA), Spinal Cord Injuries Network (SCIN), and Wheelchair Sports NSW, as well as through word of mouth throughout the SCI community. Participants were also recruited from the United States through e-mailing information via the Miami Project research volunteer registry. The study therefore included data from both Australian (n = 72) and United States (n = 79) populations. All participants had to complete a survey consisting of discrete choice scenarios (20 choice sets) along with demographic and injury-related questions. The majority completed the survey online and were only admitted into the study after they gave consent. Individuals were given the option of participating anonymously. The study was approved by the University of Sydney Human Research Ethics Committee.
Demographics
There were a total of 89 respondents from Australia, of which 17 responses were unusable as a result of being incomplete and/or the respondent not wishing to continue participation. From this group of incomplete surveys, demographic data were obtained, but DCE data were not completed. Comparison of the demographic variables between the completed surveys and the 17 incomplete surveys were examined using independent t test and contingency table analysis (χ2 test), depending upon the variable's type of measurement. There were a total of 91 respondents from the United States, from whom 12 responses were unusable because they were incomplete and/or respondents no longer wished to take part in the study. From the United States sample, DCE data were collected, but no demographic and injury information was obtained, because of the order in which demographic information was recorded in this sample.
Demographic information from all completed surveys including age, sex, level of education, and employment are shown in Table 1. The demographic variables between the samples from Australia and the United States were compared using independent t test or contingency table analysis (χ2 test).
Discrete choice survey design
In this study a self-administered discrete choice survey was employed. In designing the survey, published guidelines for conducting DCEs in health research were followed, 21,27 specifically a stepped approach previously described by Ryan and Farrar 28 in their guideline article.
Step 1: Identifying the characteristics (attributes)
Attributes for the study were functions known to affect persons with SCI. In identifying the attributes for this survey, past literature was relied upon. The functions reported as priorities by the largest number of studies were the following: bowel/bladder (n = 9), sexual function (n = 7), upper extremity function (arm/hand) (n = 6), and pain (n = 5). 6 Walking was also added into the model, as it remains an area of great interest, and was identified by a panel of neuroprosthesis consumers to be the ultimate goal. 29 Decreased mobility has been rated as the most difficult consequence to deal with after injury. 30 Based on the above analysis of the literature, the five functions/attributes included in the study were: 1) arm function/hand grasp, 2) walking, 3) bladder and bowel function, 4) sexual function, and 5) presence of persistent pain.
Step 2: Assigning levels to the attributes
The next step was to identify the range of variability or levels for each choice attribute. Each of the five attributes was then further assigned two plausible levels, the values of which are detailed in Table 2. The levels were kept to a minimum to improve comprehension and reduce cognitive overload.
Step 3: Choice of scenarios (alternatives)
The survey included a preamble with relevant contextual information, an explanation of each function and its levels, and a hypothetical background scenario. In the hypothetical background scenario, participants were asked to imagine that they were undergoing a new treatment for their SCI. The scenario described how this treatment would lead to four possible alternatives or scenarios and that the alternatives would either have a positive or a negative effect on their functions/attributes. The participants were instructed to read each alternative in its entirety, as some functions had a positive outcome, whereas others had a negative outcome. The alternatives always involved the same five functions/attributes. See Figure 1 for an example of a choice set.
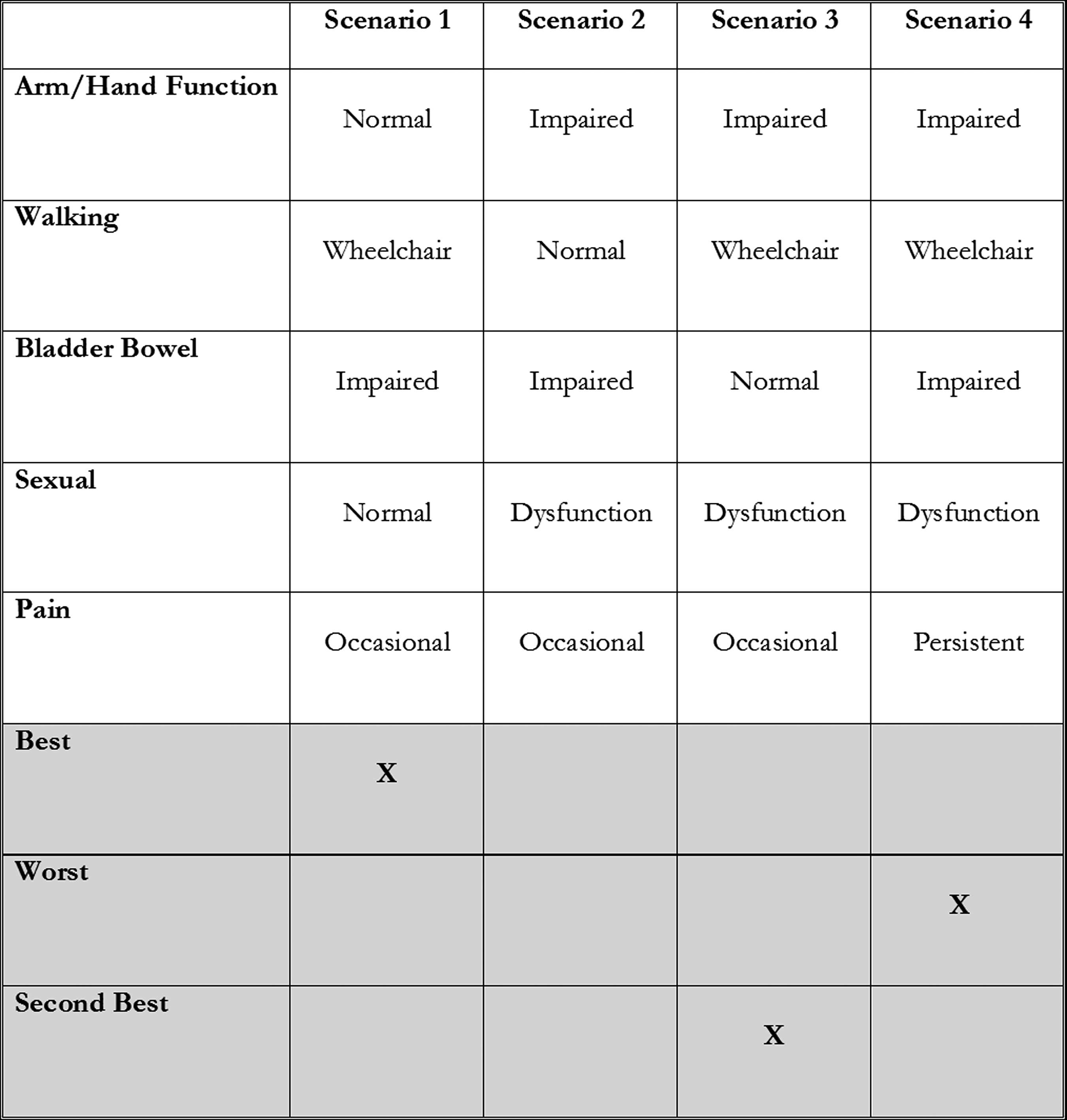
Choice set sample from the discrete choice experiment (DCE) survey.
Step 4: Establishing preferences
For this survey, the response mechanism for obtaining the preferences was a best–worst case three scenario; 31,32 that is, information on the first preference (choosing “best” alternative) as well as full ranking data (choosing “worst” as well as “next best” alternative) was obtained. An example of the choice set is shown in Figure 1. As each alternative did not have a specific label tied to it, the experimental design for this DCE was considered unlabelled.
Data model and statistical analysis
For the survey, a fractional factorial orthogonal choice design was created. An orthogonal design ensures that there is level balance for each attribute; that is, that all levels of each attribute will be evenly distributed over all choice tasks and represented in the same frequency, and that no attribute level combination will exhibit any positively or negatively correlated pattern. A full factorial design occurs when all possible combinations of attribute and levels are generated; however, this will lead to a large number of choice sets and subsequently become too tedious for the respondent. Therefore, a fractional factorial design was used, as this is a subset of choice tasks from the full factorial design, aimed to reduce the number of choice tasks that the respondent needs to answer, and is one that retains an orthogonal structure. 23 This is the most widely used type of design for DCEs. 33 The final design of four alternatives, five attributes with two levels, was evaluated over 20 different choice sets.
Regression techniques were used to analyze responses. 28 For this study, the DCE data were analyzed using the multinomial logit model (MNL) to determine best choices. In this model, we assumed no linear relationship between the different levels of the attributes and that all attributes had independent effects on preferences. Utility was measured as U nj = V nj + ɛ nj where n represents the decision maker and j represents the alternatives. The decision maker would obtain a certain level of utility from each alternative. 34 U nj represents the latent utility of attributes in the choice set with V nj being the systematic and explainable component, specified as a function of the attributes from the different function priority alternatives. ɛ nj is the random (unexplainable) component representing the factors that affect the utility but are not included in V nj . It was assumed that an individual will choose the alternative that maximizes utility among all alternatives in a choice set. 34
On this basis, we estimated the following model for the DCE:
The constant term β0 is the alternative-specific constant. The alternative-specific constant captures the average effect on utility from all the factors that are not included in the model, and serves a similar function to the constant in a regression model. It has been included as the unobserved portion of the utility (ɛnj) and has a zero mean by construction. 34 β1-β5 are coefficients of the attributes indicating the relative weight that individuals place on a certain attribute (see Table 2). An attribute with a two sided p value <0.05 was considered to be an important function to the decision maker.
In the MNL regression analysis, the magnitude of the b coefficients and odds ratio (OR), show the change in utility (satisfaction) associated with change in level (e.g., impaired vs. normal) of each of the attributes. The sign on the b coefficients indicates the direction of preference for each attribute. For example, a positive b coefficient or OR >1 indicates that as the level increases (“normal”) so does the likelihood of respondents choosing it; whereas a negative b coefficient or OR <1, implies that as the level of the attribute decreases (“impaired”), the likelihood of respondents choosing it decreases. 22 We hypothesized that respondents would prefer a return to normal functioning for all five functions/attributes and that the resulting b coefficient would be positive. The sign of the b coefficients estimated from the regression model was compared with these “a priori” hypotheses, in order to ensure that the model was internally valid.
The DCE was analysed using NLOGIT Version 4.0. To determine the overall preferences of the entire sample, a full aggregated model of the DCE was conducted. In addition, to determine whether the two cultural groups (from Australia and the United States) differed in their preferences, segmented models of the two samples were also modelled. Z tests were performed to test for significant differences (p < 0.05) between the two groups. To test how preferences varied according to the respondents' demographic and injury characteristics, these were added as covariates, and interacted with the attributes.
Results
There were no differences in the demographic variables of age, sex, education, level of injury, extent of impairment (completeness of injury), or post-injury years (p > 0.05) between the completed survey group and those who dropped out. However, the employment variable was significantly different between the two groups (p < 0.05) in that there was a larger proportion of employed participants in the dropout group. There were also no significant differences between the groups from Australia and the United States for any of the sociodemographic characteristics (p > 0.05). The samples, therefore, were combined, and the entire sample was used in the DCE analyses.
The final sample consisted of 151 participants. Table 3 shows the MNL model results for the DCE data set. All five alternatives, as hypothesized, returned a positive b coefficient, indicating that the respondents were favoring a return to normal function over the alternative of impaired function. All five functions were statistically significant, suggesting a high degree of substitution between the alternatives, indicating that participants were more likely to trade between the five functions rather than a situation in which only one function was always preferred. 35
To test the trade-offs that the respondents were willing to make between the functions of interest (e.g., arm/hand function versus bladder/bowel function), an OR was calculated to determine how much more likely a function/attribute will be chosen over the other. There were five functions/attributes, and testing for preference for each attribute relative to the other attributes made 10 combinations possible. Table 4 presents the results of the ORs for trade-offs between different functions/attributes. Table 4 shows that there were increased odds for choosing arm/hand function (between 44% and 76% more likely) over any of the other functions/attributes, resulting in arm/hand being the highest preference and the least likely one to be traded off. The next highest function favored was bladder/bowel function, with increased odds of 2–22% over the remaining functions/attributes. However, the preference between choosing bladder/bowel function over walking and bladder/bowel function over the pain attribute were not significantly different. The preference for choosing between the attributes of walking or pain reduction was also not significantly different. Sexual function was most likely to be traded off against all the other functions, showing that it was the least preferred attribute.
p value <0.001.
NS, not significant.
Given that there were no significant demographic differences between the samples, segmented DCE models from the two cultural groups were examined to test whether cultural differences affected the preferences. Table 5 shows that the sample from the United States displayed a higher preference for return to normal functioning in arm/hand, walking, and bladder/bowel control (p < 0.05) than the Australian sample. There were no differences between the two groups in terms of sexual function and pain attribute (see Table 5). The order of preference for the five functions/attributes also differed slightly between the two groups. After arm/hand function, the United States sample chose walking as second preference over bladder/bowel function, pain amelioration, and sexual function, whereas after arm/hand function the Australian sample chose bladder/bowel function and reduction in pain over walking and sexual function.
To test for the effects of demographic and injury characteristics on preferences for different attributes, sex, level and extent of neurological impairment, and time post-injury were interacted with the five attributes in the analysis. Figure 2 shows the OR of each function/attribute being preferred by males versus females. Compared with females, males had a significantly stronger preference in choosing normal sexual function over sexual dysfunction. Females had a significantly stronger preference in choosing the other four functions; that is, a return to normal arm/hand function, walking ability, bladder/bowel function, and only occasional aches and pain. Figure 3 shows the OR of each of the functions being preferred by the group with paraplegia versus that with tetraplegia. Compared with the group with paraplegia, participants with tetraplegia had a significantly stronger preference in choosing occasional pain over the presence of persistent pain. The paraplegia group had a significantly stronger preference for retaining normal arm/hand function and gaining ability to walk compared with the group with tetraplegia. Preference for choosing normal bladder/bowel function and normal sexual function were not different between the two groups. Similarly, in participants with complete versus incomplete lesions, arm/hand, bladder/bowel, and sexual function were not significantly preferred by one group or the other; however, the choices of walking and ameliorated pain were more strongly preferred by people with an incomplete impairment (see Fig. 4). Figure 5 shows the interaction effects of time post-injury, grouped as ≤10 years versus >10 years post-injury, on the five attributes. Two significant interactions were found, these being for time post-injury with walking ability and with pain amelioration. Return to normal walking function was found to be more important to those persons who were ≤10 years post-injury. In contrast, the choice of having only occasional pain over experiencing persistent neuropathic type pain becomes more preferred over time; that is, in people who are >10 years post-injury.
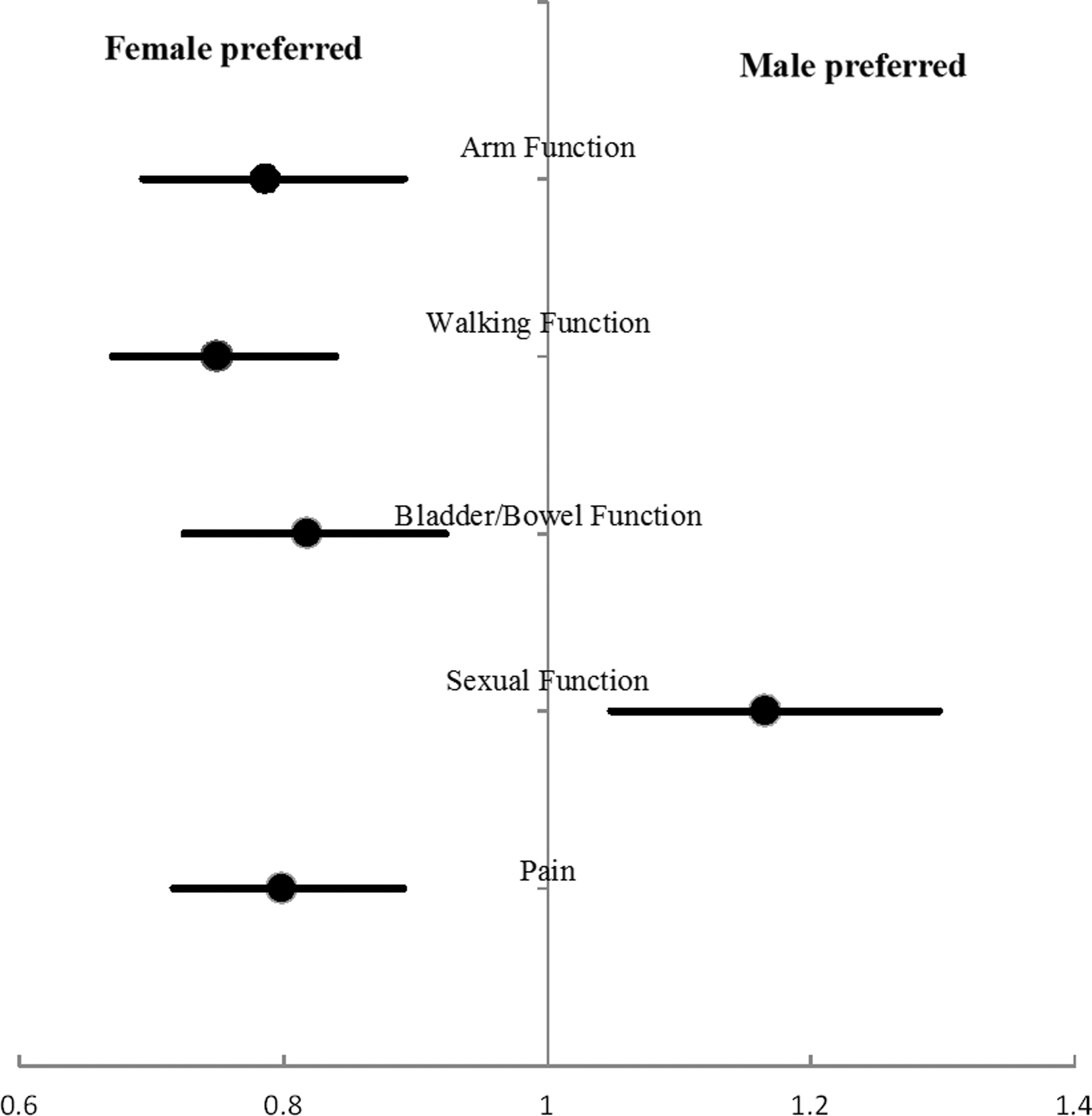
Odds ratios showing preferences of females versus males for each priority function/attribute.
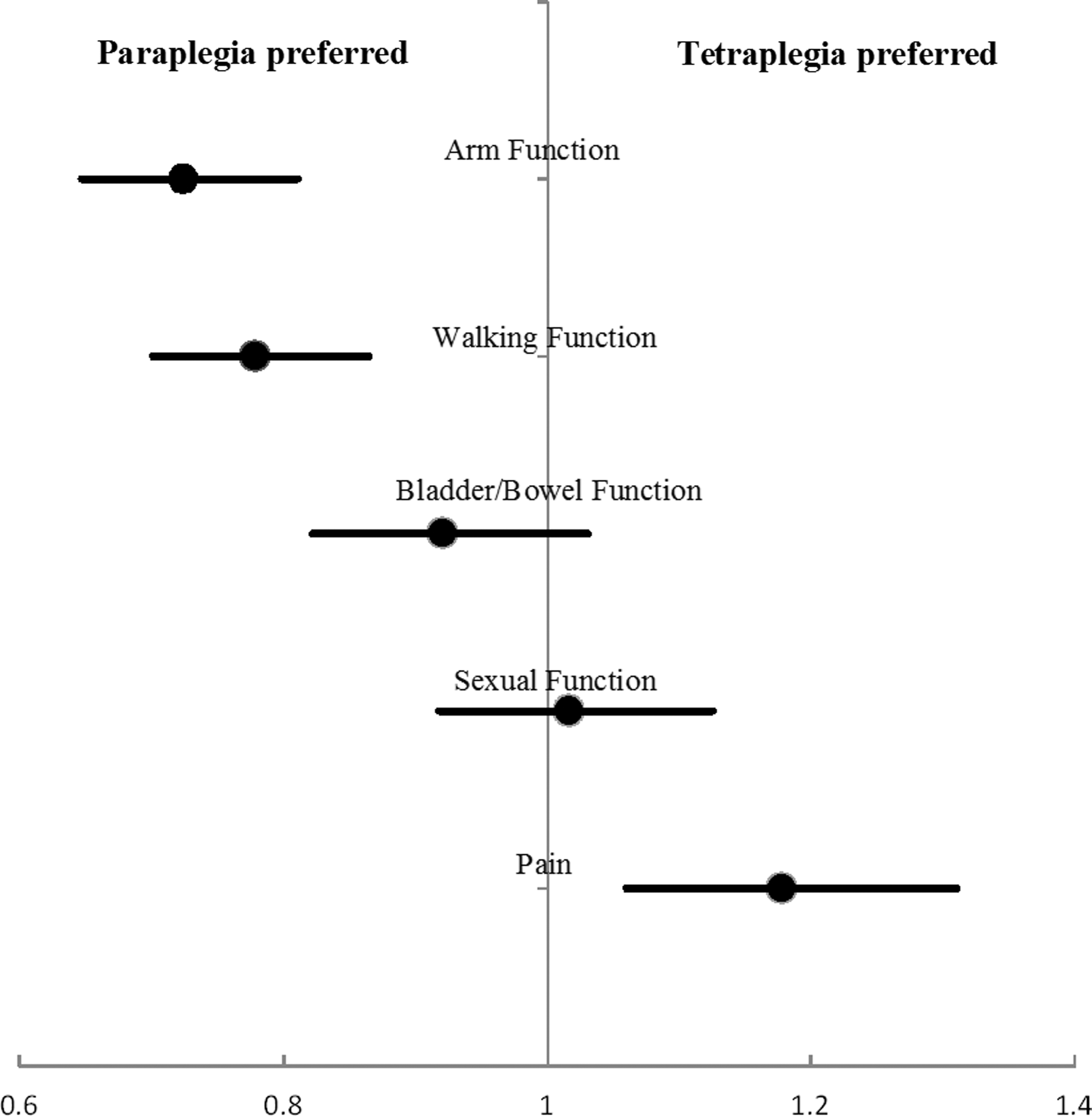
Odds ratios showing preferences of subgroups with paraplegia versus those with tetraplegia for each priority function/attribute.
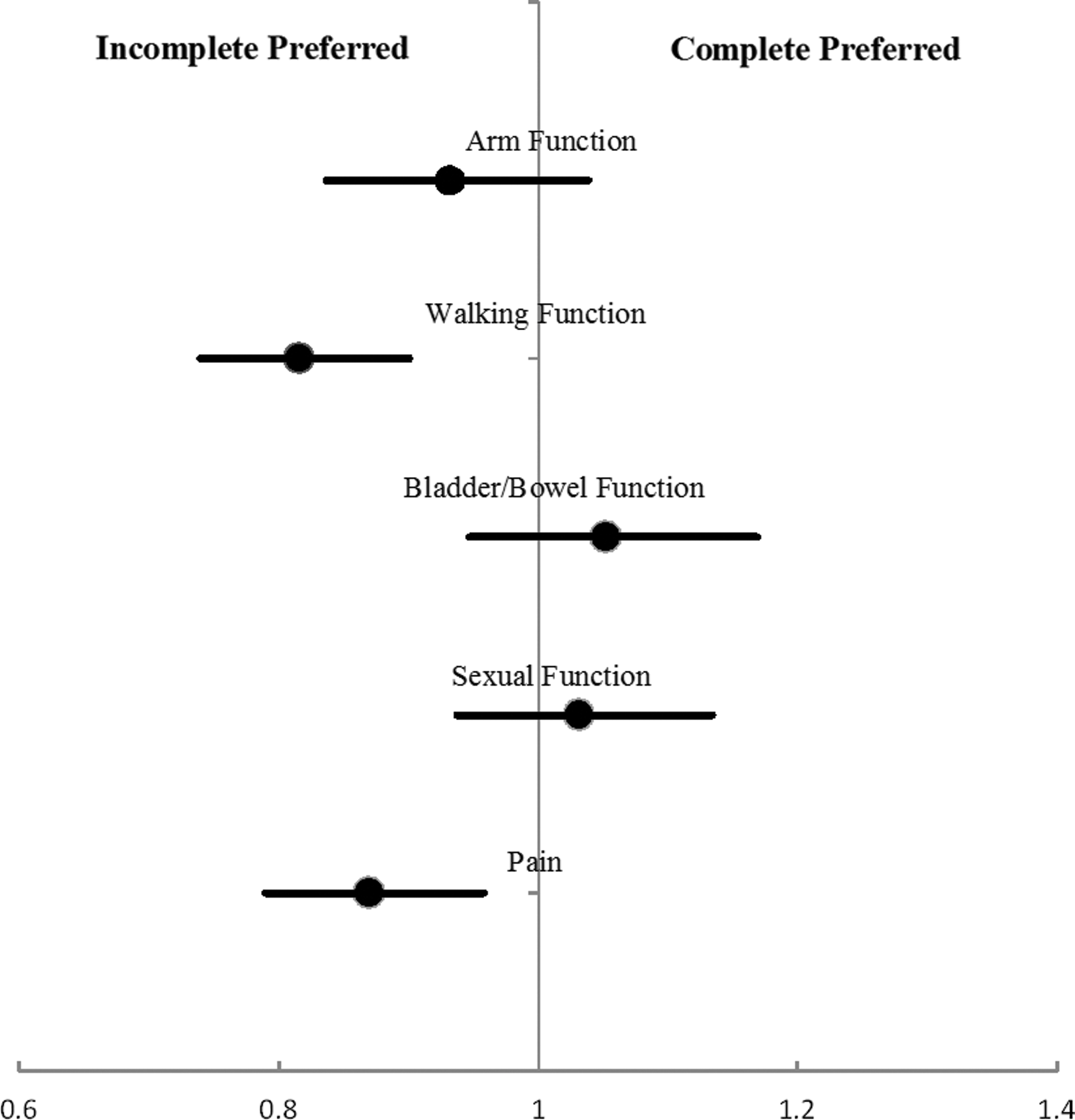
Odds ratios showing preferences of subgroups with incomplete versus those with complete lesions for each priority function/attribute.
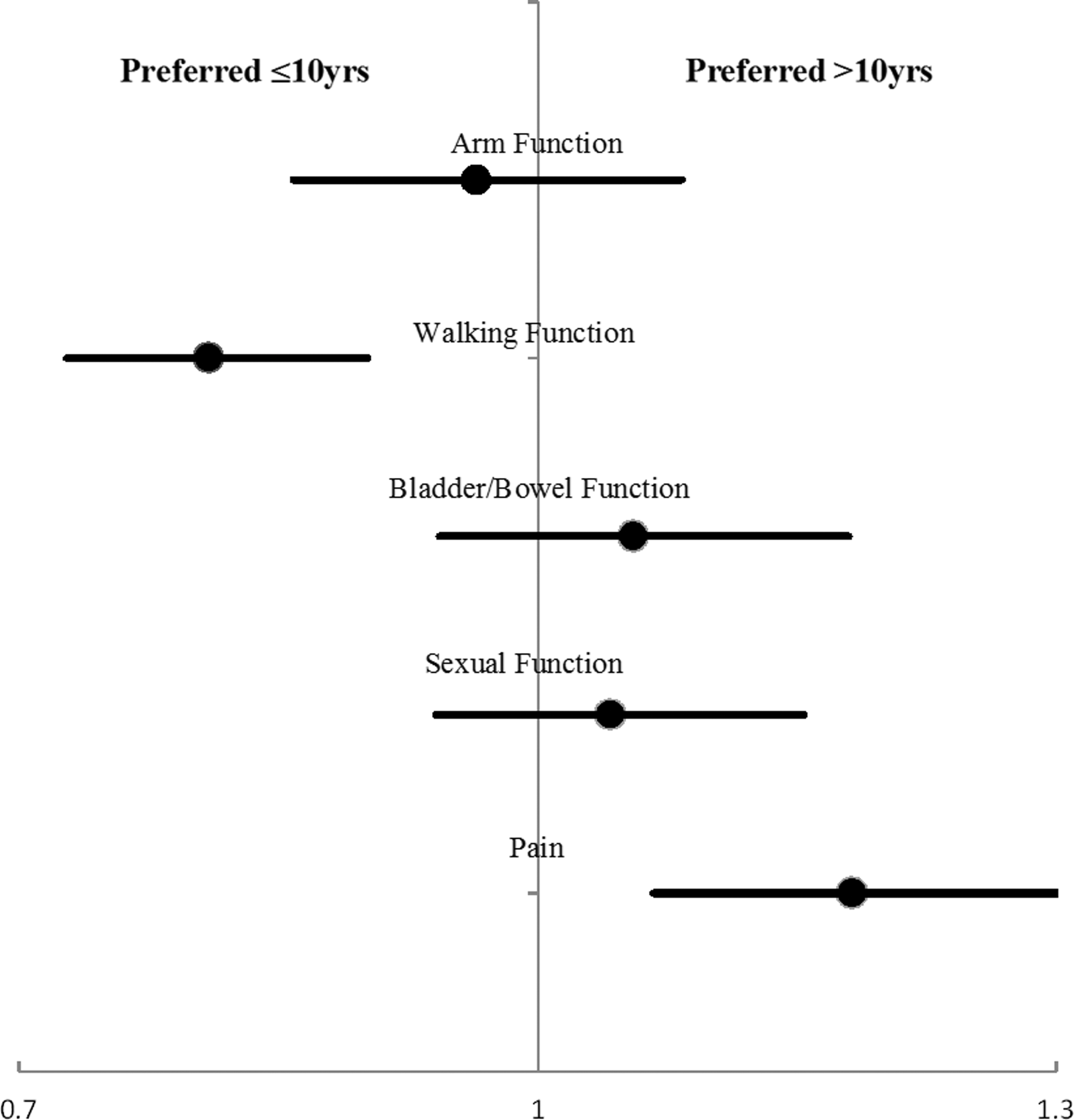
Odds ratios showing preferences based on time living with spinal cord injury (SCI) for each priority function/attribute.
Discussion
DCEs are a commonly used instrument in health economics research, and this approach has been applied to research concerning the valuation of healthcare programs and policies, diabetes care, patient choice for end-stage kidney disease, and colorectal cancer screening. 22 –24,36 In this article, preferences for five priority areas of healthy functioning (arm/hand use, ability to walk, bladder/bowel control, sexual function, and absence of pain) known to have an important influence on the QOL and participation of the SCI population, were determined using a DCE strategy. One advantage of using this method over ranking is that both an order of importance as well as the relative value of each function/attribute can be determined. This study established that all five of the functions/attributes employed in the study were viewed as important, because all five attributes were statistically significant in the DCE model, indicating a high degree of substitution or trading between the preference of normal function over impaired function. 35 This confirmed past literature that studied priority functions important for persons with SCI, 6,20,30,37,38 For example, Simpson and colleagues 6 concluded that bowel, bladder, sexual, and motor functions (the latter comprising arm/hand function and walking) were high priority. Although pain was not included in many of the studies reviewed, it was also identified as important when it was incorporated. 6 Chronic pain is common, occurring in approximately two thirds of people with SCI, with approximately one third reporting pain intensity to be severe or excruciating, 39 often persisting despite a wide range of treatment strategies, including pharmacological, physical, and complementary therapies. 40 Pain is also consistently rated by people with SCI as one of the most difficult problems to manage, despite the presence of various other consequences that interfere with daily life. 41
To gauge a preference for one function or attribute over another, the OR of each priority was compared against the other. From this, normal arm/hand function was most preferred, with the odds of choosing arm/hand function being the greatest relative to the other four functions/attributes. Similarly, other studies have found arm/hand function to be perceived as the highest priority, with one study showing that 42% of SCI persons with tetraplegia chose to restore arm function first, followed by restoration of bowel function as the next highest priority in 24% of the group. 42 Likewise, 75% of participants with tetraplegia rated restoring arm/hand function as very important for improvement of QOL in a study examining the interest in participants for using assistive technologies and brain computer-interfaces to improve lost function. 43
The loss of arm/hand function has been described as one of the most significant and devastating losses an individual can experience following SCI, because the use of the upper extremities is critical for completing basic activities of daily living, such as self-feeding, dressing, bathing and toileting, as well as meeting mobility needs. 20, 44 Surprisingly, despite the importance of possessing good arm and hand function for independence in everyday living it appears that many with tetraplegia may be unaware of what reconstructive surgery may offer, with only 39% of 137 people with tetraplegia surveyed being told that tendon transfer surgery was an option. 45 Upper-extremity reconstructive procedures have been well described and continuously improved upon for >40 years, 46 and it is estimated that at least 65% of persons with tetraplegia can benefit from reconstructive surgery. 42,46,47 However, Anderson and colleagues 45 found <10% of individuals with tetraplegia surveyed will have traditionally undergone these procedures, 45 possibly for various reasons including lack of information, hope for natural recovery, perceived invasiveness, negative perceptions, and a 3 month period of increased dependence during postoperative recovery. Given that arm/hand function has been consistently chosen as the function that people with tetraplegia view as most important, the mismatch in this health priority area between what research informs us that consumers demand and what service providers deliver needs to be addressed. The recent advent of nerve transfer procedures to augment tendon transfers and other techniques, 48 including report of a triple nerve transfer successfully reconstructing elbow extension, key pinch, grasp, and release simultaneously, 49 offer great promise and may help in the future to increase significantly the early uptake of surgical reconstruction.
The neurological level of injury (paraplegia or tetraplegia) and lesion completeness (incomplete or complete impairment) are strong indicators for the level of functioning and independence of the person with SCI. 37,50 Prior studies have examined the effect of neurological level on choices of preferred function, with Anderson 18 having reported that regaining arm/hand function was of highest priority for people with tetraplegia, whereas restoring sexual function was most important for people with paraplegia. In this current study, for persons with paraplegia versus tetraplegia, desire for restored bladder/bowel and sexual function was not significantly different between the two groups. Similarly, the extent of impairment (i.e., complete vs. incomplete lesion) had no significant effect on choices made for arm/hand, bladder/bowel, and sexual function. The health priority to manage pain was significantly preferred by the group with tetraplegia compared with those with paraplegia, and also more strongly preferred in the group with incomplete lesions. Interestingly, unlike the findings of other studies, the group with paraplegia showed greater preference for arm/hand function in comparison with the tetraplegia group. One possible reason for this finding may be the manner in which the DCE questions were phrased. In order for participants to be able to place a value on each of the functions/attributes, it is necessary to use levels (such as normal vs. impaired function) from which to choose not only attributes to gain, but ones to trade against that they may lose. As a consequence of this design, the possible loss of arm/hand function for the group with paraplegia was perhaps so highly concerning that it was rated highest and least likely to be traded. Previous studies have generally asked participants to rank or choose the function they would like to regain to most improve their QOL, and employing ranking limits the ability to capture the importance of not losing existing arm or hand function, such as could occur in a person with paraplegia through development of syringomyelia, compressive neuropathy, or a rotator cuff tear with shoulder degeneration from chronic upper limb overuse.
Walking was preferred more in those with paraplegia, as well as in those with incomplete lesions. Widerström-Noga and colleagues 41 reported that a large majority (62.6%) of their respondents found that “decreased ability to walk or move” was very hard to deal with, although this did not seem to be different between those with paraplegia and those with tetraplegia in their participants. This study found similar findings to those of Anderson, 18 whereby regaining of walking was ranked slightly higher by people with paraplegia (15.9%) than by those with tetraplegia (7.8%).
After arm/hand function, the next priority identified by the respondents in this present study was restoring bladder/bowel function. This was similar to Snoek and colleagues, 20 who reported that from a sample of 567 SCI persons with tetraplegia, 75% indicated that improvement in bowel and bladder function would enhance their QOL, which was the same percentage as for return of arm/hand function. Bladder and bowel problems have often been found to be major concerns, and were the most frequent complaints experienced in 60–70% of persons with SCI, 38 who reported problems that included urinary tract infections (46%), urinary incontinence (38%), constipation (32%), fecal incontinence (31%), diarrhea (20%), and lack of bladder/bowel regulation (40–50%), all of which restrict participation and independence. However, in the same study, Bloemen-Vrencken and colleagues 38 also reported that pain was the most disabling condition in both daily and social activities for 454 persons with SCI.
In this present study, although overall there were no significant differences found in preferences between bladder/bowel function and walking or absence of pain, both pain and walking function interacted significantly with time since injury. With a longer duration post-injury (>10 years), walking was perceived to become a less important preference, whereas the elimination of persistent pain became more important. Similarly, Anderson 18 showed elimination of pain as being more important with increased time post-injury, reporting that eliminating pain was not a priority for individuals with either tetraplegia or paraplegia injured for <3 years, but that it became increasingly important for improving QOL after 3 years. In addition, the prevalence of pain tends to increase over time. 39 Perhaps in the earlier years of adjustment following injury, walking for mobility may be more relevant to not being seen as “disabled” to the outside world. 11 Of interest also was the finding that walking was more greatly preferred in the sample from the United States compared with the Australian sample, which may reflect the greater proportion of people from the United States with paraplegia and incomplete lesions, but could also relate to cultural differences in the way people view disability, as well as other sociodemographic and environmental factors.
Kennedy and colleagues 51 reported sexual function to be the area of greatest unmet need for persons with SCI in a large community sample across four European countries. Somewhat surprisingly then in this study, sexual function, although important, was shown to have the lowest preference relative to the other four functions/attributes and was the most likely to be traded off. The order of priority of health functions is similar to that in the study by Wagner and colleagues, 42 who found the following in order of priority: upper extremity (arm/hand), bladder, lower extremity (walking), and sexual function (the latter being from 4% of their respondents). In this present study, return to normal sexual functioning was significantly more greatly preferred by the male participants than the female participants, which differed somewhat from the study by Anderson, 18 in which regaining sexual function was slightly more important for females than males with paraplegia (30.4% vs. 23.1%). Other studies have reported that problems with reduced sexual satisfaction occur more often in men than in women with SCI. 38,52 There may be various reasons to explain perceived differences between males and females about sex after injury, including changes in sensation, arousal, and orgasm; reduced desire; emphasis on intimacy instead of penile–vaginal intercourse; altered sexual repertoire and positioning; concerns about bladder and bowel accidents; body image/self-esteem; and concerns about satisfying one's partner. 53,54
This is the first study to use the DCE technique in people with SCI, being designed to elicit priorities for five areas of healthy functioning (arm/hand function, walking, bladder/bowel control, sexual function, and absence of pain). This technique has an advantage over a simple ranking method of quantifying the relative value, as well as order of importance of each function/attribute, which may differ not only between individuals with SCI, but change within the same individual over their life span. However, limitations in using DCE exist. For example, it is more time consuming and is a cognitively exacting technique, reflected by the 16% non-completion/dropout rate in the current study, which may possibly have contributed to bias in the results. In addition, unlike rankings, there is a limit to the number of attributes that could be tested.
Anderson 18 and Whalley-Hammell 55 have previously highlighted concerns about the mismatch between the priorities of people with SCI and the focus and interests of SCI researchers. For the successful translation of research into practice and health policy in which the needs of people with SCI are met, it is critical that the focus for future research with its inherent resource limitations be informed by the priorities and domains of importance for individuals with SCI. The DCE technique employed in this study offers a way to sensitively discriminate between attributes and explore their complex interactions with other personal, injury-related, and temporal factors in people with SCI. This may help to determine future research priorities, better define meaningful person-centered outcomes, and refine recruitment strategies/sample stratification. In addition, the importance of discussing possible loss of function when asking people to prioritize gain of function has been clearly shown in this study, with the DCE technique offering a way in the future to identify how much loss, if any, is acceptable, which can help inform safety assessments in interventional studies.
Footnotes
Acknowledgments
This project was supported by the Australian Rotary Health Scholarship. The authors thank Dr. Luke Greenacre and John Rose for their advice on the choice modeling technique. We are grateful for the time and effort the participants took to fill out the questionnaires.
Author Disclosure Statement
No competing financial interests exist.