
Abstract
Neurologic impairment after spinal cord injury (SCI) is currently measured and classified by functional examination. Biological markers that objectively classify injury severity and predict outcome would greatly facilitate efforts to evaluate acute SCI therapies. The purpose of this study was to determine how well inflammatory and structural proteins within the cerebrospinal fluid (CSF) of acute traumatic SCI patients predicted American Spinal Injury Association Impairment Scale (AIS) grade conversion and motor score improvement over 6 months. Fifty acute SCI patients (29 AIS A, 9 AIS B, 12 AIS C; 32 cervical, 18 thoracic) were enrolled and CSF obtained through lumbar intrathecal catheters to analyze interleukin (IL)-6, IL-8, monocyte chemotactic protein (MCP)-1, tau, S100β, and glial fibrillary acidic protein (GFAP) at 24 h post-injury. The levels of IL-6, tau, S100β, and GFAP were significantly different between patients with baseline AIS grades of A, B, or C. The levels of all proteins (IL-6, IL-8, MCP-1, tau, S100β, and GFAP) were significantly different between those who improved an AIS grade over 6 months and those who did not improve. Linear discriminant analysis modeling was 83% accurate in predicting AIS conversion. For AIS A patients, the concentrations of proteins such as IL-6 and S100β correlated with conversion to AIS B or C. Motor score improvement also was strongly correlated with the 24-h post-injury CSF levels of all six biomarkers. The analysis of CSF can provide valuable biological information about injury severity and recovery potential after acute SCI. Such biological markers may be valuable tools for stratifying individuals in acute clinical trials where variability in spontaneous recovery requires large recruitment cohorts for sufficient power.
Introduction
E
Past and current clinical trials of therapeutic interventions for acute SCI have revealed that the evaluation of a novel treatment for this indication is an immense challenge, and that demonstrating the promotion of neurologic recovery exceeding that which occurs spontaneously is extremely difficult. 8,9 At the heart of this challenge is our singular reliance upon the functional neurologic examination in the clinical evaluation of novel therapies. The International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) examination is an excellent tool that allows for the standardized assessment of neurologic function. 10,11 While the American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade is currently the gold standard for stratifying injury severity and predicting outcome, it clearly has its limitations when applied to clinical trials.
First, the baseline examination is often difficult if not impossible to validly conduct in the acute SCI setting. 12,13 This renders many individuals simply ineligible for enrollment in clinical trials because they cannot be stratified appropriately into the study. Second, even when a baseline examination can be conducted according to ISNCSCI standards and an AIS grade can be assigned at an early time-point post-injury, the variability in spontaneous recovery within each AIS grade is very high. This necessitates a large number of patients to be enrolled in order to have sufficient power to detect a treatment effect in efficacy studies. 14 Third, in small, early stage clinical trials, it can be very difficult (if not impossible) to distinguish treatment effect from spontaneous neurologic recovery using the ISNCSCI examination as the sole measurement of outcome. Without other outcome measures to provide a “signal of efficacy,” such early trials may be poorly informative for the crucial decision to proceed with a large-scale clinical trial.
In an attempt to more objectively classify injury severity and better predict outcome, we and others have been interested in the use of proteins within the cerebrospinal fluid (CSF) as neurochemical biomarkers of SCI. 15,16 In our previous work, we studied the CSF of 27 individuals with acute SCI and identified a series of inflammatory markers (interleukin [IL]-6, IL-8, and monocyte chemotactic protein [MCP]-1) and structural proteins (tau, S100β, and glial fibrillary acidic protein [GFAP]) that appeared promising as neurochemical biomarkers of injury severity. 17 This represented our first experience with this prospective observational clinical trial and the largest available series of acute SCI patients with CSF samples obtained over multiple days. The limitation of this study was that in this small series of patients, it was not possible to distinguish between cervical and thoracic SCI (which we anticipate would behave differently) and it was difficult (albeit not impossible) to actually predict neurologic recovery.
We have continued to recruit acute SCI individuals into a prospective observational clinical trial of CSF collection and CSF pressure monitoring. Here, we extend our findings from 2010 by reporting on the analysis of CSF from the first 50 acute SCI patients enrolled at a single institution. Specifically, the purpose of this study is to analyze CSF biomarkers at the 24 h post-injury time-point to determine if they are able to: 1) distinguish between baseline AIS grades; 2) predict AIS conversion; and 3) predict motor score recovery in cervical and thoracic SCI at 6 months post-injury.
Methods
Clinical trial enrollment
Individuals sustaining an acute SCI were enrolled into this prospective observational study if they met the following inclusion criteria: 1) AIS grade A, B, or C SCI upon presentation; 2) spinal bony injury between C0 and L1 inclusive; 3) the ability to insert a lumbar catheter within 48 h of injury ; and 4) the ability to provide a valid, reliable neurologic examination. Patients were excluded if they had concomitant head injuries, concomitant major trauma to the chest, pelvis, or extremities that required invasive intervention (e.g., internal or external fixation), or were too sedated or intoxicated to provide a valid neurologic examination. While the inability to provide a neurologic examination was a significant impediment to recruitment, a valid baseline examination was felt to be critical for the establishment of a neurologic “phenotype” to compare against the biomarkers. The clinical trial protocol for conducting this prospective observational study at this single institution was approved by our local institutional review board (#H10-01091); a subsequent multi-center extension of this study is registered with
CSF collection and processing
Once enrolled in the study, an intrathecal catheter (PERIFIX® Custom Epidural Anesthesia Kit; B. Braun Medical Inc., Bethlehem, PA) was inserted in the lumbar spine at L2/3 or L3/4 using a standard aseptic technique. The catheter was advanced 15–20 cm from the entry point on the skin surface and kept in place for 72 to 120 h. The catheters were inserted prior to surgery with the patient log-rolled to the right side and the spinal column protected in a neutral position by a physician.
CSF samples of 3–4 mL were drawn at the time of catheter insertion and then in the subsequent post-operative period approximately three times each day (discarding the first 1 mL of CSF aspirated from the line). Sample processing occurred immediately at the patient's bedside by the research study nursing team. The CSF sample was centrifuged at 1000 rcf for 10 min, and the supernatant then dispersed into 200 μL aliquots and immediately frozen in an ethanol–dry ice bath and stored at −80°C.
Biochemical analysis
Concentrations of inflammatory markers in CSF were evaluated using Bio-Plex (Bio-Rad, Hercules, CA) multiplex magnetic bead-based antibody detection assay. A total of 30 cytokines, chemokines, and growth factors were evaluated simultaneously in human CSF using a commercially available human 25-plex kit (LHC-0009; Invitrogen, Carlsbad, CA) and five additional single-plex kits (LHC-7071, LHG-0021, LHC-7041; LHG-0111). This assay allowed the detection of tumor necrosis factor (TNF)-α, TNF-R1, IL-1β, IL-2, IL-2R, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12p40, IL-13, IL-15, IL-17, inducible protein (IP)-10 , MCP-1, interferon (IFN)-α, IFN-γ, eotaxin, granulocyte-macrophage colony-stimulating factor , MIG, macrophage inflammatory protein (MIP)-1α, MIP-1β, and RANTES, IL-16, brain-derived neurotrophic factor, fibroblast growth factor-basic, glial cell–derived neurotrophic factor, and vascular endothelial growth factor. As only IL-6, IL-8, TNF-R1, MCP-1, and IP-10 levels were within detection limit of the assay, further analysis was done using a custom 5-plex kit (LHC-0061, LHC-0081, LHC3021, LHC-1011, LHC-1081). Beads were read on the Bio-Plex suspension array system (Bio-Rad), and the data were analyzed using Bio-Plex Manager software. CSF levels of total tau (T-tau; KHB0042, Invitrogen), S100β (RD192090100R; Biovendor, Modrice, Czech Republic) and GFAP (RD192072200R; Biovendor) were determined using specific commercially available enzyme-linked immunoassorbent assay (ELISA) kits. For each of these individual ELISAs, the assay sensitivities for tau, S100β, and GFAP was 10 pg/mL, 15 pg/mL, and 0.045 ng/mL, respectively. The intra-assay coefficients of variation (CV) were less than 5.9, 3.8, and 6.4%, and inter-assay CVs were less than 9.0, 10.1, and 6.1 for tau, S100β, and GFAP respectively. Concentration levels were determined based on a standard curve generated on each plate using the manufacturer-supplied reagents. For each analyte, the samples were assayed in duplicate and the average concentrations were used for statistical analysis.
Neurologic evaluation
The severity of neurologic impairment was graded according to ISNCSCI standards of neurologic testing, with motor scores recorded separately in the upper and lower extremities. All baseline testing and the assigning of the baseline AIS grade (A, B, or C) was conducted by research study nurses (who received extensive training in how to conduct the ISNCSCI examination and calculate the AIS) to confirm the initial examination of the patients, which often was conducted by the house staff. Follow-up ISNCSCI motor assessments were conducted at 6 months post-injury.
Statistical analysis
For all data analyses, we utilized the CSF concentrations from the 24 h post-injury data collection time-point (27.4 ± 8.6 h; mean ± standard deviation [SD]). The distribution of data was checked using Kolmogorov-Smirnov, Shapiro-Wilks and Q-Q plots. The log10-transformation was used to normalize the raw CSF concentrations. Parametric tests were used if the data were normally distributed and non-parametric tests were used if either the data were not normally distributed or for subgroup analyses with small sample sizes. Chi-square or Fisher's exact test were used for categorical data. Comparisons between two groups were analyzed using independent t-tests with Levene's test to assess the equality of variance. A one-way between-subjects analysis of variance (ANOVA) was conducted when there were three or more groups. Post hoc comparisons using the Duncan test were used to detect any differences between subgroups following the ANOVA tests. Mann-Whitney U and Kruskal-Wallis tests were used to compare the groups if the data were not normally distributed.
After the bivariate analyses to distinguish among AIS grades, linear discriminant analysis (LDA) was used (objective 1). 18 To predict AIS conversion (objective 2), LDA was used to combine the markers into an Inflammatory index and a Structural index to create a composite score. This composite score was included in the logistic regression and LDA analyses to identify who would and would not convert. These analyses were conducted within clinically meaningful subsamples (e.g., cervical vs. thoracic, complete vs. incomplete injury). Goodness of fit was assessed using the Hosmer-Lemeshow test for the logistic regressions and by conducting a “leave-one-out” cross-validation for LDA. Receiving operating characteristics curves were produced to compare which biomarkers were most accurate in predicting neurological improvement (converters vs. non-converters).
To understand the association between biomarkers and change in motor score (objective 3) Pearson and Spearman correlation coefficients were used to assess the relationship between variables if the data were normally or non-normally distributed, respectively. Diagnostic performance of each biomarker was assessed using the area under the curve (AUC) and their p values. Multiple linear regression and locally weighted regression (Lowess) also were applied to simultaneously visualize their main and interaction effect for selected biomarkers.
A p value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS (version 23), R × 64 (version 3.1) and Matlab (version R2014b).
Results
A total of 50 consecutive patients suffering acute traumatic SCI were recruited at our single, provincial referral center between March 2006 and August 2011. This included 32 cervical and 18 thoracic SCI patients whose basic demographics and neurologic assessments at baseline and 6 months follow-up are listed in Table 1. Of the 50 patients, 39 (78%) were male and the average age was 41.9 ± 14.9 years (mean ± SD). Follow-up for neurologic assessment at 6-month post-injury was achieved in 48 of 50 patients (a 96% follow-up rate). One patient with a cervical SCI died and another with a cervical SCI moved to a different province and was lost to follow-up.
Of the 50 subjects recruited, there were 29 AIS A, 12 AIS B, and 9 AIS C at baseline. There were 39 males, and the average age was 42.1 years. 32 were cervical-level injuries.
AIS, American Spinal Injury Association Impairment Scale; UEMS, Upper Extremity Motor Score; LEMS, Lower Extremity Motor Score; MS, motor score; N/A, not assessed.
Objective 1
Are the CSF biomarkers significantly different between patients with different baseline AIS grades?
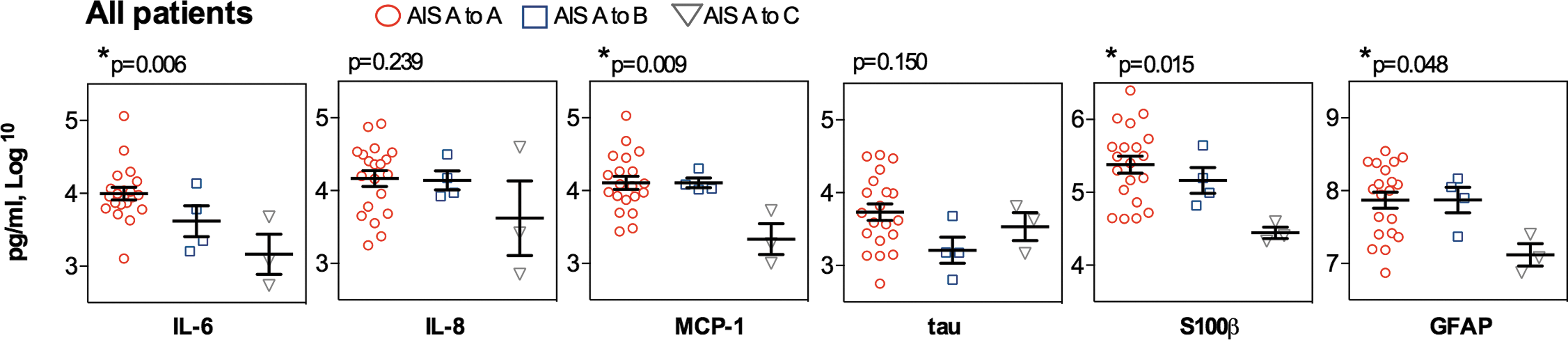
The first question we addressed is how different the CSF proteins at 24 h post-injury were between the different AIS grades (Fig. 1). After first confirming normality (Kolmogorov-Smirnov), a one-way ANOVA confirmed statistically significant between-group differences between AIS A, B, and C for IL-6, tau, S100β, and GFAP in all 50 patients (p < 0.001 for each biomarker; Fig. 1A). The differences in log10 concentrations of 1 or 2 between AIS grades represents absolute differences of 10 to 20 times, suggesting that the levels of these biomarkes were indeed quite different between the different injury severities. Between-group differences for IL-8 and MCP-1 were not statistically different, although there was a trend for IL-8 (p = 0.051). The between-group differences for IL-6, IL-8, tau, S100β, and GFAP were statistically significant when comparing the cervical AIS A versus B versus C patients, while in the comparison of thoracic AIS A versus B versus C cohorts, the IL-6 and GFAP levels were significantly different (Fig. 1B, 1C).
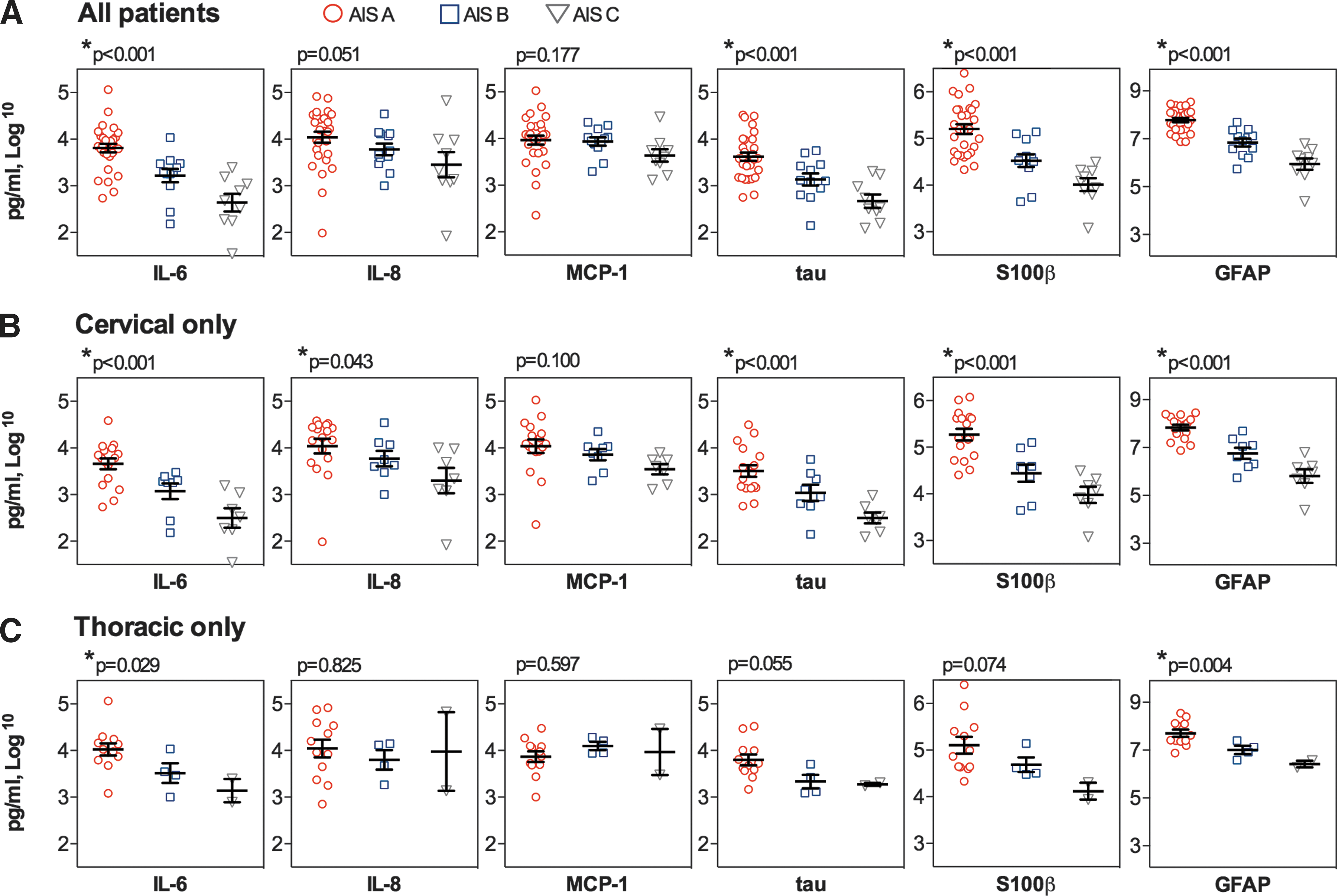
Log10-transformed cerebrospinal fluid biomarker concentrations (pg/mL) between patients of different American Spinal Injury Association Impairment Scale (AIS) grades. Analyses are separated in:
Can the baseline AIS grade be classified by the 24 h post-injury CSF concentrations of these biomarkers?
Based on the significant differences between AIS A, B, and C patients for the 24-h post-injury CSF concentrations (shown in Fig. 1), we used discriminant function analysis to establish a prediction model for classifying baseline injury severity. Based on two canonical discriminant functions using the CSF levels of IL-6, IL-8, MCP-1, tau, S100β, and GFAP, the model had an 84% accuracy at classifying the correct AIS grade for all 50 patients (Fig. 2A). Using a separate leave-out-one cross-validation model, the accuracy for classifying the correct AIS grade was 76.0%. For the cervical patients (n = 32), the model included the CSF levels of all six proteins and had an accuracy of 81.3%, with a cross-validation model accuracy of 68.8% (Fig. 2B). Finally, for the thoracic patients (n = 18), the model included only IL-6, tau, S100β, and GFAP and had an accuracy of 83.3%, with a cross-validation accuracy of 66.7% (Fig. 2C). The relative contribution of each CSF protein in each of the discriminant functions is included in Figure 2. LDA coefficient was used to calculated the discriminant score (Function 1 and 2) for a given patient. The data was first standardized and then applied in the equation. Associated equations for Function 1 and 2 (for patients) are:
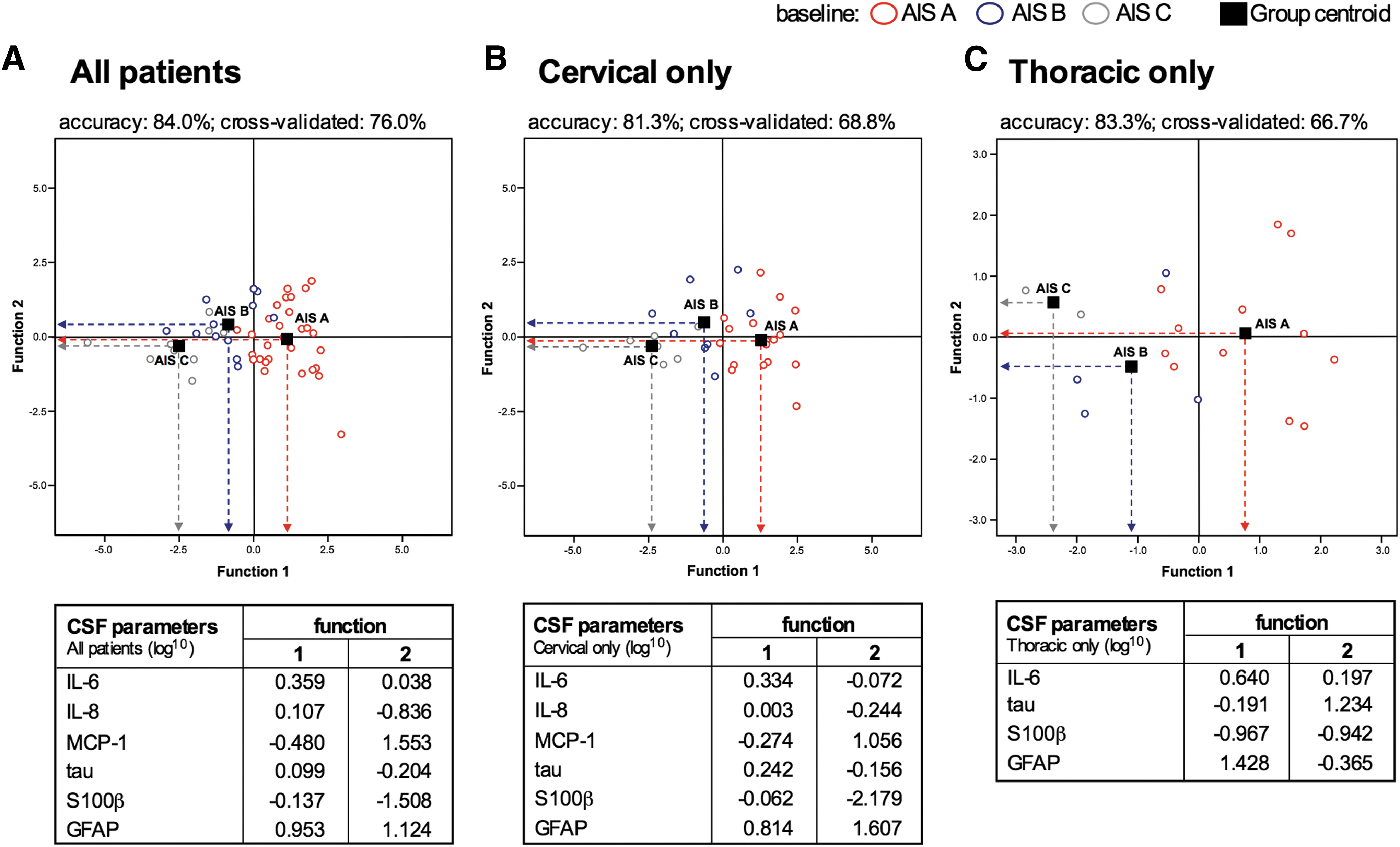
Projection plot of two canonical discriminant functions for prediction of initial baseline American Spinal Injury Association Impairment Scale (AIS) grade using interleukin (IL)-6, IL-8, monocyte chemotactic protein (MCP)-1, tau, S100β, and glial fibrillary acidic protein (GFAP). Analyses are separated in:
The results showed that the most significant variables that play the principal role in distinguishing between AIS grades are comprised of GFAP (for Function 1) and MCP-1 and S100β (for Function 2).
Objective 2
Can AIS grade conversion be predicted using CSF biomarkers?
Here, we determined whether the CSF biomarker concentrations at 24 h post-injury were different between those who experienced AIS grade conversion/improvement at 6 months versus those who did not. No patient experienced a conversion due to deterioration of neurologic function. Two of the initial 50 patients were lost to follow-up (both suffered cervical AIS A injuries), and therefore this question was addressed with the analysis of 48 patients. For the cohort of 48 patients, the IL-6, IL-8, MCP-1, tau, S100β, and GFAP levels were significantly different between those who remained the same versus those who converted (Fig. 3A). These differences were statistically significant for all proteins in the cervical SCI patients (Fig. 3B). For the thoracic patients, only IL-6 and S100β were significantly different (p = 0.038 and p = 0.02, respectively; Fig. 3C).
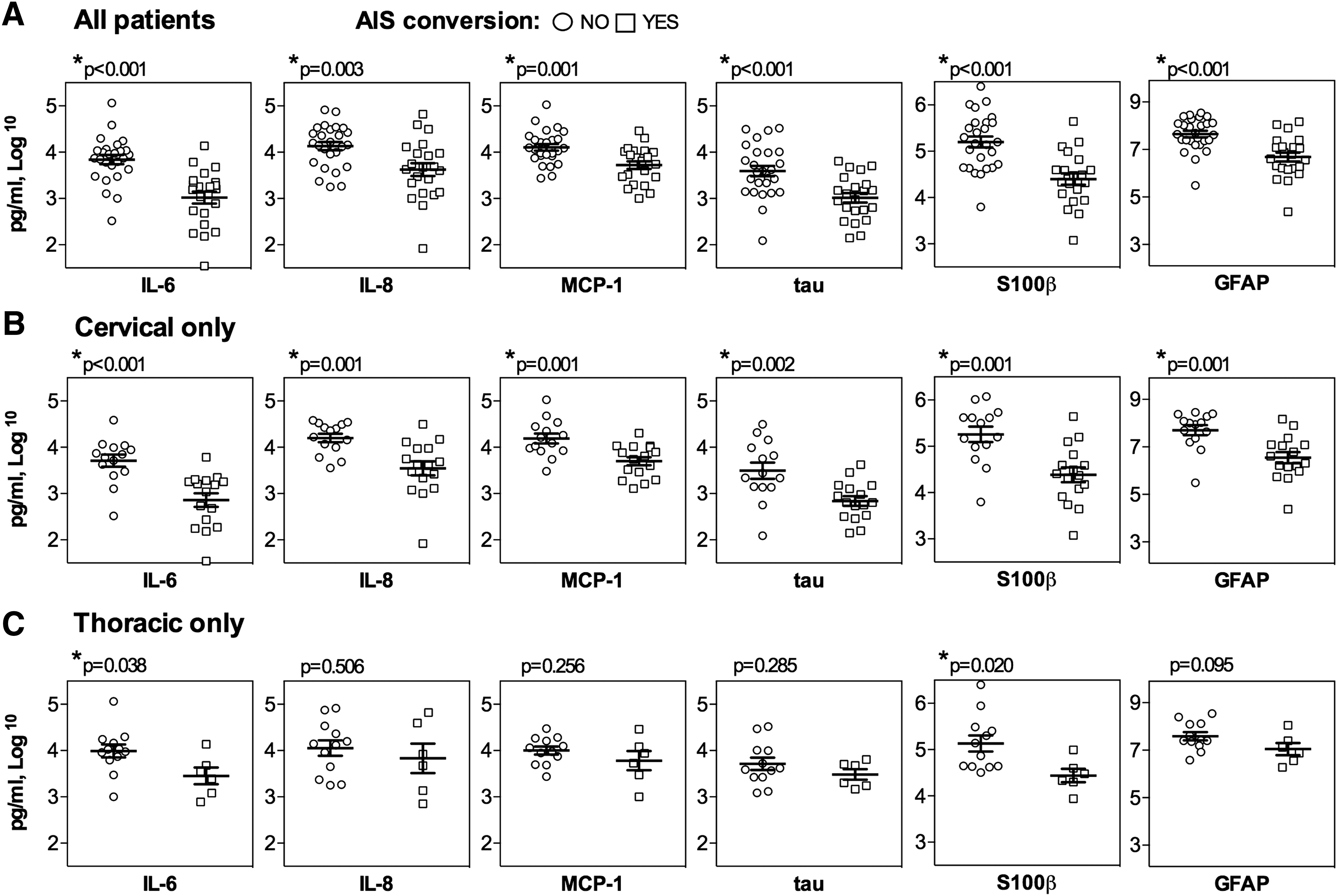
Log10-transformed cerebrospinal fluid (CSF) concentrations (pg/mL) of biomarkers between spinal cord injury (SCI) patients who experienced American Spinal Injury Association Impairment Scale (AIS) grade conversion/improvement over the first 6 months, compared to those who did not. Analyses are separated in:
We then conducted a discriminant analysis to separate the biomarkers into inflammatory markers (IL-6, IL-8, and MCP-1) and structural markers (tau, S100β, and GFAP), and then established a linear discriminant analysis using the inflammatory and structural components to predict conversion (either yes or no; Table 2). In all patients (n = 48), the model had an 83.3% accuracy at predicting conversion. The accuracy of the model was 86.7% in the cervical SCI cohort and 94.4% in the thoracic, suggesting that the biomarkers were better at predicting conversion in thoracic SCI than in cervical SCI. However, in the leave-out-one cross-validation analyses, the biomarkers had the same accuracy for predicting conversion in the cervical SCI cohort (86.7%), while this accuracy dropped to 77.8% for the thoracic, suggesting that the biomarkers are more robust predictors in the cervical SCI patients.
The model consisted of a set of “inflammatory markers” which included interleukin (IL)-6, IL-8, and monocyte chemotactic protein 1, and a set of “structural markers,” which included tau, S100β, and glial fibrillary acidic protein. Note that the prediction was strongest (by considering its higher performance in full data and cross-validation) in the cervical patients. A “leave-one-out” cross-validation demonstrated that there was nearly identical prediction accuracy in the entire cohort (n = 48) and in the cervical patients (n = 30).
AIS, American Spinal Injury Association Impairment Scale.
For each set of inflammatory markers and structural markers, the AUC for predicting AIS conversion was computed illustrated in Figure 4. Both sets of markers were able to significantly discriminate between the converters and non-converters. When considering all patients, the AUC was slightly higher for the inflammatory markers index than the structural markers index (0.883 ± 0.052 vs 0.857 ± 0.055). Additionally, the AUC was computed for predicting AIS conversion in cervical and thoracic SCI. For the cervical SCI patients (n = 30), the AUC was 0.924 ± 0.052 and 0.857 ± 0.075 for the inflammatory and structural markers, respectively. For the thoracic SCI patients (n = 18), the AUC was 0.833 ± 0.120 and 0.861 ± 0.096 for the inflammatory and structural markers, respectively. This indicates that in general, the biomarkers are somewhat better at predicting AIS conversion after cervical SCI, compared with thoracic SCI, although the analysis of thoracic SCI may be limited by the smaller number of patients (n = 18), compared with cervical SCI (n = 30).
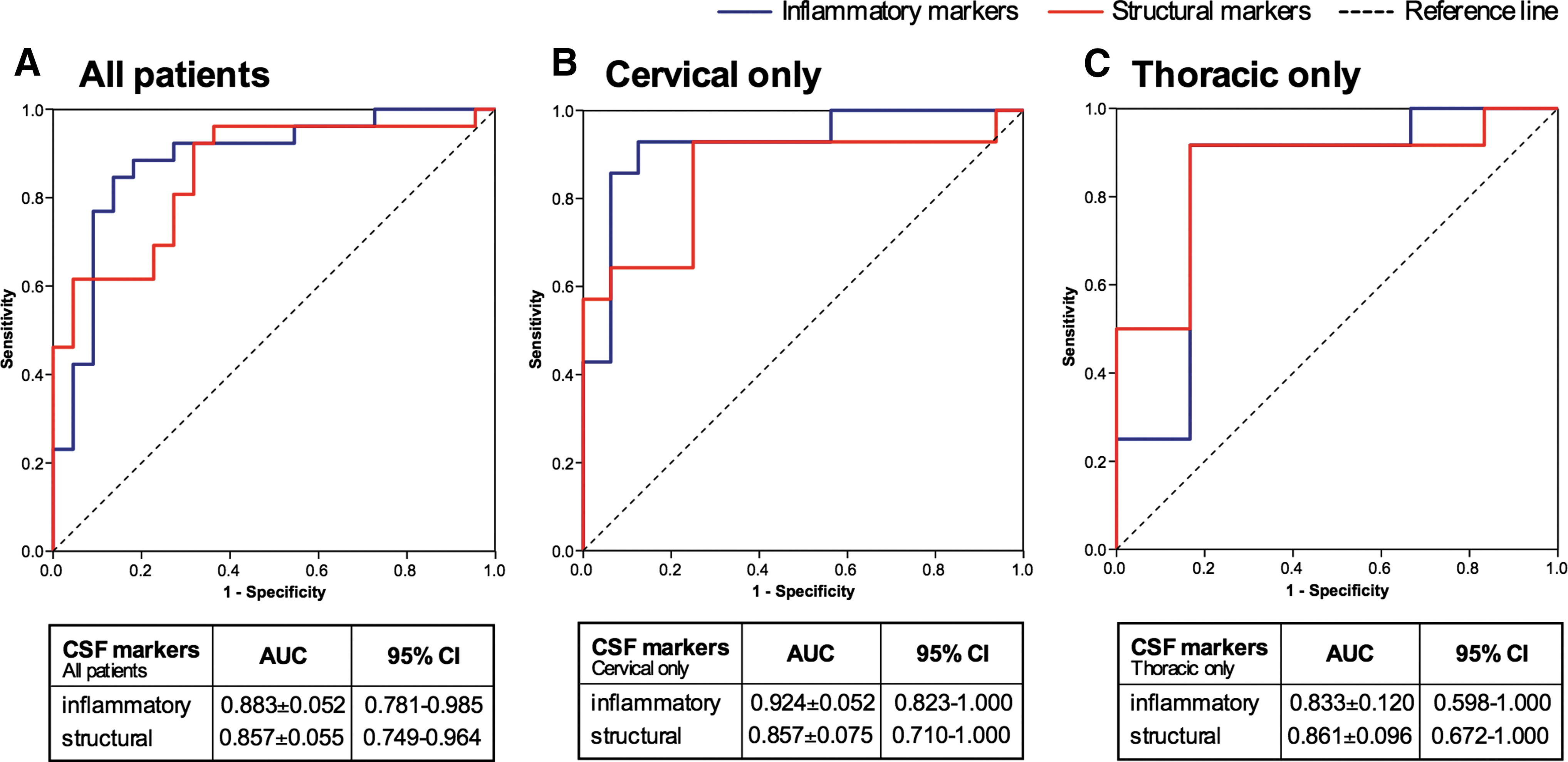
Receiving operating characteristic (ROC) curve analysis of inflammatory and structural cerebrospinal fluid (CSF) biomarkers for the prediction of American Spinal Injury Association Impairment Scale (AIS) conversion. Analyses are separated in:
Can conversion in AIS A patients be distinguished using the biomarkers?
We explored the prediction of AIS grade conversion even further in the 29 AIS A patients specifically. This group of patients likely represents a particularly challenging cohort in clinical trials because of the potential heterogeneity in the extent to which the spinal cord is traumatized by the initial mechanical impact. For example, let us assume that there is a certain extent of mechanical trauma that needs to be imparted to the spinal cord to produce a complete, AIS A injury. One individual might sustain this extent of mechanical trauma by falling off of a ladder, for example. But another individual might sustain five times this extent of mechanical trauma in a high speed rollover motor vehicle accident. Neurologically, these two individuals would both present as AIS A complete SCI, but one (the first) is quite likely to have a less severe biological injury and theoretically a higher chance for conversion than the other. We asked if the biomarkers might be able to predict AIS conversion for those who were deemed AIS A. The log concentrations of the biomarkers for those AIS A patient who did convert versus those who converted to AIS B or AIS C convert are shown in Figure 5.
Log10-transformed cerebrospinal fluid concentrations (pg/mL) of biomarkers between American Spinal Injury Association Impairment Scale (AIS) A patients who demonstrated neurological improvement to AIS B or C over the first 6 months, compared with those who remained AIS A. Between-group analysis of variance revealed significant differences for interleukin (IL)-6, monocyte chemotactic protein (MCP)-1, S100β, and glial fibrillary acidic protein (GFAP), demonstrating that some of the heterogeneity within this single AIS A grade may be explained biologically. Vertical lines indicate the mean value ± standard error of the mean. *p < 0.05 significantly different between groups. Color image is available online at
Objective 3
Can ASIA motor score improvement be predicted using CSF biomarkers?
Acknowledging that AIS conversion is a gross measure of neurologic recovery, clinical trials of novel neurorestorative agents are increasingly utilizing improvements in motor score (MS) at 6 months post-injury as an outcome measure, accepting that the majority of motor recovery occurs during this period. 19,20 Hence, we sought to determine if motor score recovery over 6 months could be predicted by the biomarkers, and which ones. Because MS recovery may be related to segmental or distant recovery, we divided this analysis into cervical and thoracic. Using Spearman correlation coefficients, we found that the relationship between individual biomarkers and total MS recovery was indeed statistically significant in cervical SCI. This statistically significant relationship held true for upper and lower extremity motor recovery (not shown). The change in MS is plotted against the log concentrations of each biomarker (Fig. 6). We found similar statistically significant relationships between IL-6, S100β, and GFAP in the thoracic SCI patients.
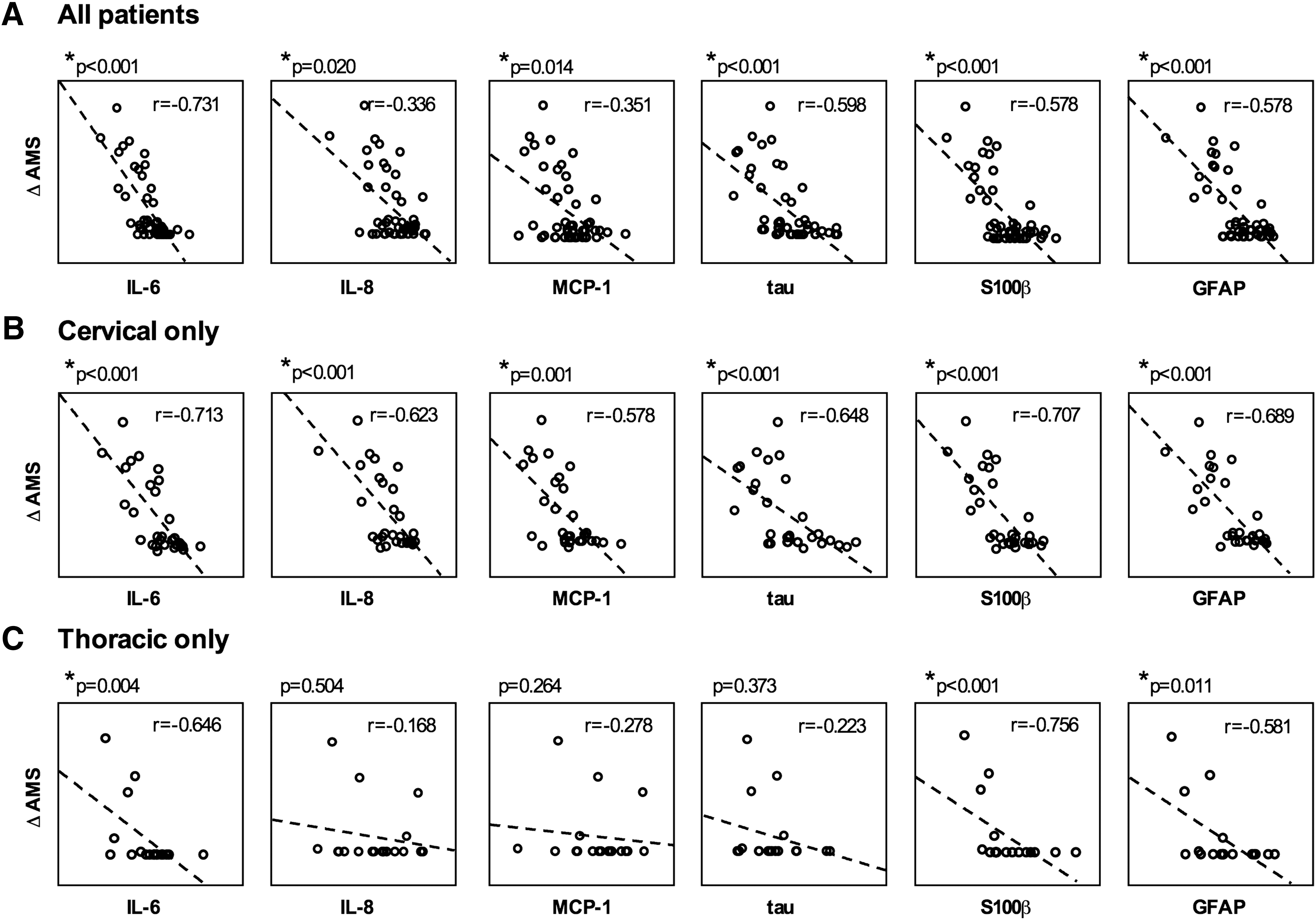
The relationship between cerebrospinal fluid biomarker concentrations and the improvement in motor score (ΔMS) over the first 6 months. Analyses are separated in: (A) all patients (n = 48); (B) cervical patients only (n = 30); and (C) thoracic patients only (n = 18). For the cervical spinal cord injury (SCI) patients, the ΔMS represents change in both upper and lower extremity motor scores over the first 6 months, while for the thoracic SCI patients the ΔMS represents the change in lower extremity motor scores. Our data showed a statistically significant correlation between ΔMS and interleukin (IL)-6, IL-8, monocyte chemotactic protein (MCP)-1, tau, S100β, and glial fibrillary acidic protein (GFAP) concentration, which was especially strong for the cervical SCI patients, with correlation coefficient values for the different proteins ranging from −0.578 to −0.713. Black dots indicate data of individual patients. The dashed lines indicate the identity function and r denotes the Spearman's correlation coefficient. *p < 0.05 significantly different between groups.
An additional way to address this question would be to try to use specific biomarkers to determine if individuals have a poor likelihood of achieving significant motor recovery. For example, if administered a novel therapeutic intervention and measuring change in MS, it would be useful in interpreting such changes if one could stratify the likelihood of such improvement occurring spontaneously. We did this using Lowess modeling (Fig. 7) to demonstrate that a combination of the log concentrations of IL-6 and S100β was particularly effective at showing which individuals did not achieve significant MS recovery. This suggests the possibility of using these biomarkers in the stratification of individuals for clinical trials that measure 6-month MS recovery as an outcome measure.
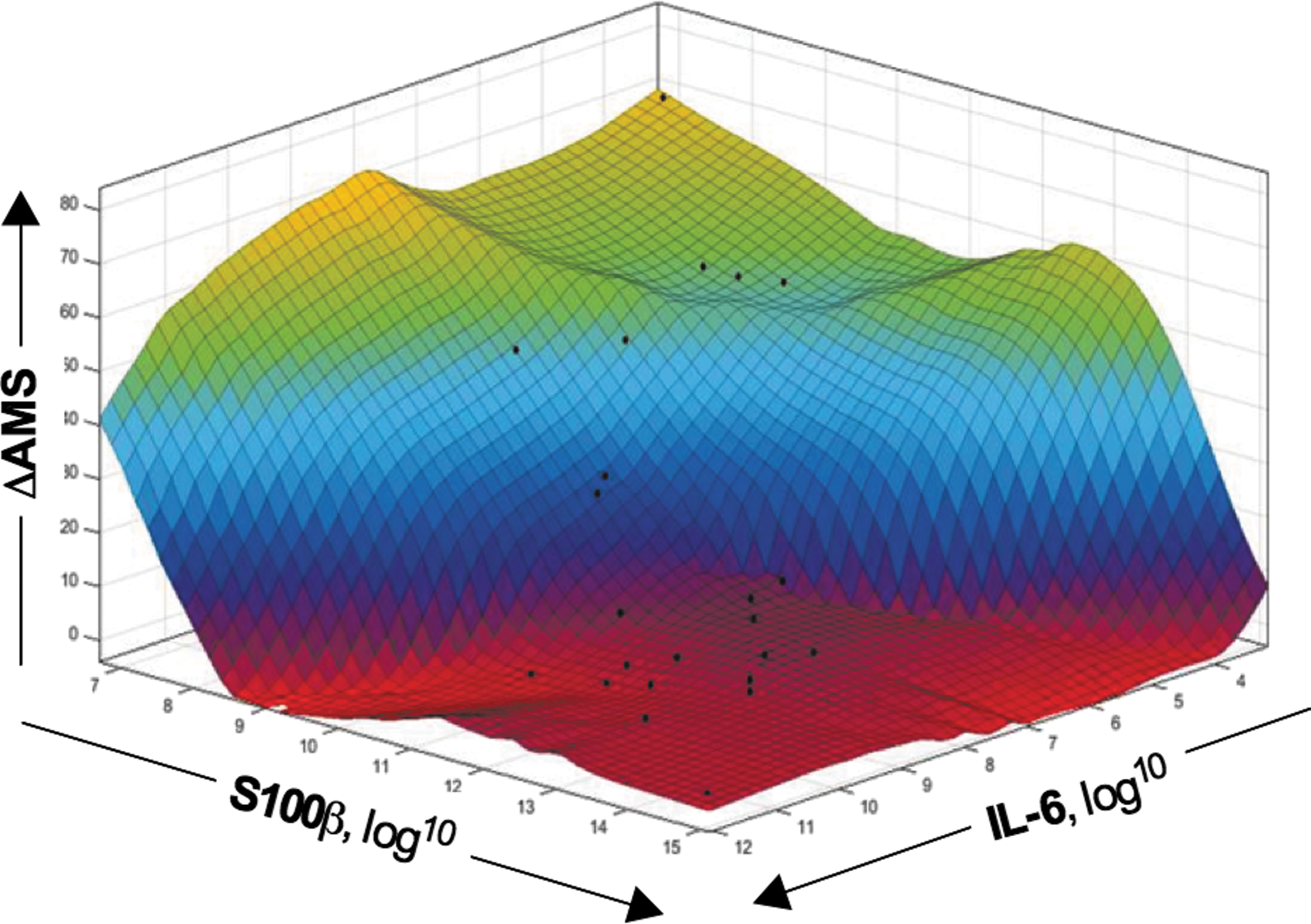
Three-dimensional color image of Lowess-smoothed surface plot of the change in American Spinal Injury Association Impairment Scale (AIS) motor score (ΔMS) by cerebrospinal fluid (CSF) concentration of interleukin (IL)-6 and S100β (polynomial: Linear, Span: 35, Robust: Bisquare, Center and scale). Estimated relationship between the log10-transformed IL-6 and S100β concentration (pg/mL) in CSF (horizontal axes) and the change in AIS motor score improvement (ΔMS) over the first 6 months (on a linear scale on the vertical axis). The red to green color scale represents low to high changes in ΔMS, respectively. Our data show that CSF concentrations of IL-6 and S100β could identify which spinal cord injury patients achieved significant motor score recovery over time (green/yellow color) and those who did not (red color). The individual black dots represent the raw data. Color image is available online at
Discussion
In summary, we report that concentrations of inflammatory and structural proteins within the CSF of acute SCI patients 24-h post injury are distinct between different injury severities (AIS A, B, and C), and that these early biological responses can be utilized to predict AIS conversion and motor score recovery at 6 months post-injury. We also report that even within patients with AIS A injuries, the concentrations of CSF biomarkers differ between those who will and will not convert to AIS B or C injuries. We also observed that the biomarker prediction of recovery is more accurate in cervical SCI patients, compared with thoracic injury patients. This work extends our previous work, which first introduced the concept of using these CSF proteins at this time-point post-injury as biomarkers of injury severity and predictors of recovery.
The importance of the baseline neurologic assessment and classification of injury severity
In the initial management of acute traumatic SCI, the baseline classification of neurologic impairment as AIS A, B, C, or D is a fundamental component of the early assessment. Clinicians instinctively prognosticate the neurologic outcome of the acute SCI patient after this initial assignment of neurologic impairment. This prognostication is obviously important in the early communication with the patient and his/her family, and can influence management decisions. For example, in an international survey of more than 900 spine surgeons, the percentage of respondents who would rush an incomplete cervical SCI patient to the operating theater for surgical decompression within 6 hours was much higher than the percentage who would do so for an otherwise identical cervical SCI patient with complete quadriplegia (72.9% vs. 46.2%). 21 Whether rational or not, this strong inclination to more expeditiously operate on the incomplete SCI reflects clinical sentiment around the prognostic implications of this baseline neurologic assessment. Similarly, the distinction between complete and differing levels of incomplete SCI is used to prognosticate functional outcome in the more chronic rehabilitation setting. 22 –27
Despite this, one could take the counter argument that the baseline neurologic assessment is not essential to the early clinical management: The timing of surgical decompression (if it is performed at all) and the extent of rehabilitation may be heavily influenced by many other factors unrelated to the initial neurologic assessment, such as other associated injuries or co-morbidities and the availability of resources and facilities. However, where such a baseline assessment is indeed critical is in the stratification of acute SCI patients within clinical trials.
27,28
In this regard, the challenges associated with the baseline neurologic assessment have enormous implications on the translation of novel therapies or interventions for human SCI. The inability to even conduct such a baseline neurologic assessment in intoxicated or pharmacologically sedated individuals or those suffering from traumatic brain injury is an impediment in virtually all prospective clinical studies. As we have previously shown, this can be a problem in, conservatively, one-third of acute SCI patients arriving in the emergency department.
13
Without a baseline neurologic assessment, such individuals cannot be included in acute clinical trials, thereby reducing the eligible pool of recruitable patients at any given institution. Such a reduction in recruitable patients has most certainly had an impact on the execution of acute SCI clinical trials that have begun in the last 5 years, including the trials of riluzole (
Potential biomarkers of injury severity: IL-6, tau, S100β, and GFAP
In this study, we observed significant differences between the AIS A, B, and C patients in their 24 h log concentration of IL-6, tau, S100β, and GFAP. These differences were significant in both the cervical and the thoracic injuries. Interestingly, IL-8 and MCP-1 were not significantly different between the AIS grades, which is in contrast to our previous reporting on the first 27 patients. 29 This would suggest that when examined within a larger cohort of patients, the cytokines IL-8 and MCP-1 are less robust as biomarkers of injury severity than IL-6. We found IL-6 to be a particularly strong biomarker of injury severity, which fittingly also turned out to be a strong predictor of neurologic recovery with respect to AIS conversion and motor score recovery. IL-6 is a pro-inflammatory cytokine that also has been evaluated as a potential biomarker in the setting of acute neurologic injury by other investigators. In a study of seven acute SCI patients, Tsai and colleagues reported that the CSF levels of IL-6 and IL-8 were elevated in patients with complete SCI. 30 The IL-6 messenger RNA and protein were significantly increased within the spinal cord in an injury severity–dependent fashion using a rodent thoracic weight-drop experimental model. 31 In patients with spinal cord paralysis secondary to transverse myelitis, Kaplin and colleagues demonstrated a more than 250-fold increase in CSF IL-6 concentrations, compared with control patients. 32 They also found a strong correlation between IL-6 concentrations and the clinical severity of paralysis. A recent report of 114 severe traumatic brain injury (TBI) patients demonstrated that increased levels of IL-6 over time in serial CSF samples were associated with poor outcomes on Glasgow Coma Scale. 33
Aside from the inflammatory cytokines, GFAP, S100β, and tau are structural biomarkers that were distinct between AIS grades in our current study, in keeping with our initial reported results. 29 Each of these three proteins also have been studied by other investigators as potential biomarkers of acute neurologic injury. 34 GFAP is an intermediate filament protein within astroglial cells. GFAP levels within the CSF of patients undergoing thoracoabdominal aortic aneurysm (TAAA) surgery were more than 500 times higher in patients who suffered ischemic paralysis, compared with those who did not undergo TAAA surgery. 35 In a recent study of 35 acute SCI patients, GFAP levels in the blood were found to be higher in AIS A and B patients, compared with AIS C or D patients. 36 The S100 proteins are calcium binding proteins found in astroglial and Schwann cells. S100β has been reported by many investigators as a potential CSF and serum biomarker of traumatic and ischemic spinal cord injury and also traumatic brain injury. In the experimental setting, animal SCI studies have reported increased S100β levels after injury. 37 –39 In the aforementioned TAAA study, CSF level of S100β also were elevated in addition to GFAP in those who sustained ischemic spinal cord damage. 35 In clinical TBI, unfavorable outcomes were seen in patients with elevated CSF levels of S100β, which also correlated with elevated intracranial pressure. 40
Finally, tau is a microtubule binding protein highly enriched in neurons. Roerig and colleagues reported that CSF levels of tau were significantly elevated in a series of 51 dogs with traumatic paraplegia caused by thoracolumbar or cervical intervertebral disc herniation. 41 CSF levels of tau also were reported to be significantly elevated in human patients suffering ischemic SCI during TAAA repair. 42 In the setting of diffuse axonal brain injury, CSF tau levels have been shown to increase 500- to 1000-fold at 1 h post-injury to 40,000-fold at 24 h post-injury. 43,44 Our current findings with regard to the utility of GFAP, S100β, and tau as biomarkers of injury severity in acute human traumatic SCI is consistent with this body of literature on GFAP, S100β, and tau spanning both human and animal studies in acute traumatic SCI in addition to ischemic SCI and traumatic brain injury.
The prediction of neurologic recovery with biomarkers
As pointed out in the introduction, the conducting of clinical trials would certainly be facilitated by being able to stratify an acute SCI patient's injury severity with an objectively measured biomarker. However, arguably the greatest utility of biomarkers in acute clinical trials would be in the improved prediction of neurologic recovery. The early assignment of neurologic impairment as AIS A, B, or C unfortunately leaves much uncertainty about the final neurologic outcome due to variability in spontaneous neurologic outcome. This was highlighted by Fawcett and colleagues in their seminal review of the variability in neurologic recovery in the patients enrolled in the Sygen trial. 28 Conversion rates for individuals deemed to have complete spinal cord injuries have ranged from 4 to 25%, 19,20,45 –48 and the historical conversion rate for complete SCI has been estimated to be less than 10%. 28 However, the time of initial assessment for many of these studies was days to weeks post-injury, 49 and it is well understood that the earlier the baseline neurologic assessment and assignment of “completeness” is conducted the more variability there is in subsequent neurologic recovery. This fact was evident in the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS) that evaluated surgical decompression in more than 300 acute cervical SCI patients. In this study, with the baseline neurologic assessment occurring early (at least within 24 h of injury, and in some cases, merely a few hours post-injury) the conversion rates for AIS A individuals were 43.2% for those decompressed early (<24 h) and 37.0% for those decompressed late (>24 h). STASCIS highlights the fact that even in the most homogeneous group of individuals with complete SCI, predicting their outcome when assessing them early is extremely challenging.
In this regard, the biomarkers may play an important role in facilitating clinical trials. We found that AIS conversion could be predicted well with the combination of inflammatory and structural biomarkers. Indeed, we found that the CSF biomarkers were best at predicting who would not convert, especially for those with cervical SCI. In the future, such CSF biomarkers could be utilized in a clinical trial to identify those individuals who had a low chance of spontaneous recovery. This would help investigators interpret neurologic recovery in the context of a therapeutic intervention (which is often impossible to interpret in small, early stage clinical trials). We would contend that this is particularly relevant for the AIS A patients. Conceptually, because there is no neurologic impairment that is more severe than AIS A, this AIS grade includes individuals with a wide spectrum of injuries—some sustained in high speed rollover motor vehicle accidents and some sustained in falls or sporting accidents. This would, in theory, generate some AIS A injuries that are more severe (and less likely to convert) than other AIS injuries. Our sub-analysis of AIS A patients suggests that the biomarkers IL-6, GFAP, and S100β may indeed help to distinguish these gradations in injury severity amongst the AIS A grading (Fig. 5). Establishing robust models to predict conversion specifically in AIS A patients will require further study, and our conclusions are tempered by the fact that there were only seven conversions in the cohort of 29 AIS A patients. Nonetheless, we are encouraged by demonstrating the proof of principle that biological features within the CSF may help to discern some of the heterogeneity of human SCI that currently is unaccounted for within the AIS grading system.
Along the same lines, we also found that all of the CSF biomarkers were significantly related to MS recovery over the 6 months in cervical SCI patients (Fig. 6). This is particularly relevant given the trend for acute clinical trials to include only cervical SCI patients. There are many well-documented reasons for excluding thoracic SCI patients from such trials, especially given the challenges of observing/measuring segmental motor recovery. But again, there is considerable variability in spontaneous motor recovery as per the MS, which necessitates large cohorts of patients to be recruited if MS recovery is to be used as a primary outcome measure. 28 We observed that combinations of IL-6 and S100β could be used to model spontaneous MS recovery, and in particular identify those individuals who have a low likelihood of motor improvement (the red “valley” on the Lowess plot; Fig. 7). Having this information again could be helpful in interpreting motor recovery in a small, early stage clinical trial. For example, if an individual with a C6 AIS A injury were to improve 12 motor points after being administered a novel therapy in a phase II clinical trial, a CSF biomarker instrument that included IL-6 and S100β could potentially provide insights as to how likely such recovery is attributable to the therapy versus to spontaneous recovery. It is interesting to us that our CSF biomarker data is consistent with what is well-recognized in the field: that thoracic SCI is a different entity from cervical SCI and that MS recovery in thoracic SCI patients is difficult to predict given that so many do not recover any motor points (as noted in Fig. 7, where so many of the thoracic SCI patients have a ΔMS of 0.)
We also acknowledge that our inclusion of patients with bony spinal injuries extending down to L1 potentially creates the confounding variable of including patients with cauda equina injuries, and that a more “pure” spinal cord injury study would limit the inclusion to a neurologic injury level of T12. 50 Our patient cohort included three individuals with L1 injuries (coincidentally, distributed evenly amongst AIS A, B, and C). Our assessment of their magnetic resonance imaging (MRI) scans indicated that these injuries were at or above the conus, and based on our previous work demonstrating no statistically significant difference in motor recovery between pure spinal cord injuries and conus medullaris injuries (as defined either by MRI or by bony spinal level), we felt that including such patients would not deter from the overall analysis. 51 Certainly, with further recruitment and a larger patient cohort, it would be interesting to analyze whether these thoracolumbar junction injuries are distinct in their biochemical profile from more rostral cord injuries.
This study is the largest to date of acute human SCI patients in which CSF samples at a specific time-point post-injury (24 h) were evaluated for neurochemical biomarkers of injury. Our 96% clinical follow-up at 6 months reflects our acknowledgment of how valuable these patients and their samples are, and our concerted efforts to achieve clinical follow-up in a patient population that is notoriously hard to follow-up (and that sometimes requires traveling out to distant communities for clinical assessment). We acknowledge, of course, that we are neither the first nor the only group to have an interest in establishing biomarkers or other clinical methods for better predicting neurologic outcome and facilitating clinical trials. With respect to neurochemical markers, Yokobori and colleagues have reported on CSF levels of ubiquitin B-terminal hydrolase-L1, spectrin breakdown products, and GFAP in a cohort of seven acute SCI patients. 16 Pouw and colleagues (in collaboration with our center) have examined CSF GFAP, neuron specific enolase, S100β, tau, and neurofilament heavy chain in acute SCI patients. 52 While we contributed CSF samples for this study, large differences in the timing with which the CSF samples were drawn resulted in considerable variability in the early concentrations, and hence it is difficult to compare these results with our current results where the CSF samples were consistently taken close to the 24 h post-injury time-point. Kuhle and colleagues recently reported on the longitudinal measurement of serum neurofilament light chain (NFL) in acute SCI patients who were part of a prospective randomized controlled trial of minocycline conducted at the University of Calgary. 53 This study reported that serum NFL levels were closely related to injury severity and neurologic outcome, and were decreased in patients treated with minocycline, which nicely demonstrates that neurochemical biomarkers also may be useful as surrogate biological outcome measures in small clinical trials.
These studies illustrate the point that there are certainly other protein candidates besides those that we report on here that are potentially useful biomarkers of injury. Ultimately, a “biomarker signature” that consists of different proteins and biomolecules may be optimal. We are currently engaged in studies that employ proteomic, metabolomic, lipidomic, and genomic platforms for further biomarker discovery in our human SCI patients. Also, the study by Kuhle and colleagues on serum NFL does raise an important point about the use of CSF and serum for studying neurochemical biomarkers of SCI. While the CSF undoubtedly provides the most representative picture of central nervous system injury, there is little argument that blood sampling would be a far more convenient and feasible in an acute clinical trial setting. In our previous work, we evaluated the serum in nine acute SCI patients and found that the concentrations of proteins such as IL-6, GFAP, and S100β were in some cases many orders of magnitude lower in the blood than in CSF. 29 This is, however, not to say that biomarkers within blood may not correlate with injury severity or predict outcome, as Kuhle and colleagues have demonstrated. We also are currently conducting these biochemical analyses on the serum samples of these patients for whom we have already measured the CSF, and will be better able to interpret how the CSF concentrations are reflected in blood. As pointed out by Woodcock and Morganti-Kossman, the challenge in establishing useful biomarkers in blood for acute neurologic conditions is related to the fact that systemic responses to trauma may obscure the specific responses to neurologic injury, and for some neurochemical markers, the extravasation from the injured central nervous system into the bloodstream may be more reflective of blood–brain barrier disruption than actual injury severity. 54
Alongside the discussion of neurochemical biomarkers of SCI, it should be noted that extensive work also has been done in MRI in an effort to establish imaging biomarkers to classify injury severity and predict outcome. 55 –59 Parameters such as the maximal canal compromise, maximum spinal cord compression, presence of hemorrhage, and extent of spinal cord edema may be helpful in predicting neurologic recovery. Also, novel sub-analyses of the neurological impairment in acute SCI patients may help to delineate some of the early heterogeneity and better predict motor recovery.
Dvorak and colleagues, for example, reviewed more than 800 patients in the Rick Hansen SCI Registry and in reporting on the differences in motor recovery achieved by AIS A, B, and C cervical and thoracic injuries, they highlighted for the first time the distinction between high and low cervical SCI and the need to balance these populations in clinical trials. 60 Tanadini and colleagues have analyzed neurologic recovery patterns in complete and incomplete cervical SCI patients within the European Multicenter Study about Spinal Cord Injury database. 61,62 Using unbiased recursive partitioning, they have established conditional inference trees that can subdivide patients based on early upper extremity motor scores into more homogeneous groups with regard to motor recovery. All of these are worthwhile and necessary efforts to better understand the heterogeneity of acute SCI and improve our ability to conduct clinical trials. Ultimately, some combination of clinical features, MRI parameters, and biological markers may prove to be most effective at predicting neurologic recovery. Wilson and colleagues demonstrated this concept with the establishment of a clinical prediction rule that utilized both clinical and MRI information to predict Functional Independence Measure motor score at 1 year follow-up. 63 In keeping with this, one of our ongoing initiatives is to examine the utility of combining clinical and MRI features with our CSF biomarkers in the prediction of neurologic recovery.
The patient cohort that we report on here represents all individuals that were recruited at our single center prior to the launch of a multi-center initiative to collect CSF samples from acute SCI patients, titled the Canadian Multicenter CSF Pressure and Biomarker study (
Footnotes
Acknowledgments
The authors acknowledge the funding support of the Canadian Institutes for Health Research, Michael Smith Foundation for Health Research, the Vancouver Coastal Health Research Institute, the Craig H. Neilsen Foundation, and the Paralyzed Veterans of America. The authors also gratefully acknowledge the support provided by the staff of the Vancouver Spine Research Program, including Allan Aludino, Leilani Reichl, and Andrew Pennington.
Author Disclosure Statement
No competing financial interests exist.