
Abstract
Glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) have been studied as potential biomarkers of mild traumatic brain injury (mTBI). We report the levels of GFAP and UCH-L1 in patients with acute orthopedic injuries without central nervous system involvement, and relate them to the type of extracranial injury, head magnetic resonance imaging (MRI) findings, and levels of GFAP and UCH-L1 in patients with CT-negative mTBI. Serum UCH-L1 and GFAP were longitudinally measured from 73 patients with acute orthopedic injury on arrival and on days 1, 2, 3, 7 after admission, and on the follow-up visit 3–10 months after the injury. The injury types were recorded, and 71% patients underwent also head MRI. The results were compared with those found in patients with CT-negative mTBI (n = 93). The levels of GFAP were higher in patients with acute orthopedic trauma than in patients with CT-negative mTBI (p = 0.026) on arrival; however, no differences were found on the following days. The levels of UCH-L1 were not significantly different between these two groups at any measured point of time. Levels of GFAP and UCH-L1 were not able to distinguish patients with CT-negative mTBI from patients with orthopedic trauma. Patients with orthopedic trauma and high levels of UCH-L1 or GFAP values may be falsely diagnosed as having a concomitant mTBI, predisposing them to unwarranted diagnostics and unnecessary brain imaging. This casts a significant doubt on the diagnostic value of GFAP and UCH-L1 in cases with mTBI.
Introduction
M
Several groups have reported that central nervous system (CNS) derived blood-based biomarkers have been able to predict intracranial lesions, and that they may help in diagnosis and in avoiding unnecessary CT scans. 6 –10 The association of glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) with visible CT pathologies has raised a special interest.
GFAP is a cytoskeletal monomeric filament protein present in astrocytes located both in white and gray brain matter. 11 It has been suggested that GFAP has good sensitivity and specificity for intracranial findings of TBI, 10 and it is considered to be a better marker for a focal than for a diffuse injury. 6,12 Two groups reported that serum levels of GFAP were increased in those patients with clinically diagnosed mTBI with abnormal CT compared with those patients with mTBI with normal CT. 7,13 They also found that GFAP levels were higher in patients with axonal injury on MRI 13 and in patients, who required neurosurgical interventions. 7 It had been reported earlier that GFAP was not affected by extracranial fractures, 14 and that it was possible to distinguish both patients with mTBIs and moderate TBI (moTBI) from healthy controls and from patients with orthopedic injury without a TBI. 7
UCH-L1 is involved in both adding and removing ubiquitin from proteins, which are set for internal metabolism within cells. 15,16 UCH-L1 is considered a suitable counterpart for GFAP in TBI diagnostics, as it is produced by different cell types, and UCH-L1 is found to be more abundant after diffuse than after focal injury. 6 In patients with mTBI, serum UCH-L1 levels were increased in comparison with healthy controls and non-brain-injured orthopedic patients, 8 and UCH-L1 was able to discriminate between CT-positive and CT-negative mTBI 8 and between healthy controls and full spectrum TBI patients. 9 However, there are also contradictory results in which UCH-L1 levels were unable to distinguish healthy controls from patients with mTBI when analyzed with two different immunoassays. 17
However, GFAP and UCH-L1 are also found outside the CNS, 18,19 and variable serum levels of GFAP and UCH-L1 have been observed in non-brain-injured patients in previous TBI studies. 7,8,20,21 Based on the present knowledge, the specificity of GFAP and UCH-L1 in mTBI diagnostics remains uncertain. Multiple studies have suggested that GFAP and UCH-L1 could be sensitive and specific markers of the existence and severity of brain injury in trauma, especially in case of moTBI, severe TBI (sTBI), and complex mTBI. 9,14,22 –24 However, the published studies include generally healthy individuals or a small number of orthopedic trauma patients as controls, and comparison studies with CT-negative mTBI patients are few in number. In order to further explore the performance of GFAP and UCH-L1 in discriminating patients with orthopedic trauma and CT-negative mTBI, we assessed GFAP and UCH-L1 in patients with acute orthopedic injuries without CNS involvement and related them to the type of extracranial injury, head MRI findings, and GFAP and UCH-L1 levels in patients with CT-negative mTBI in relatively large precisely characterized populations.
Methods
Study population
This prospective two-center study was part of the EU-funded TBIcare project (Evidence-based Diagnostic and Treatment Planning Solution for Traumatic Brain Injuries) project. In that project, we recruited patients with TBI of all severities as well as a control group of patients with acute orthopedic injuries at the Turku University Hospital (Finland) and at the Addenbrooke's Hospital Cambridge (United Kingdom). The analysis in this study included all 73 patients with acute orthopedic trauma and those 93 patients with mTBI who had no pathological brain parenchymal findings on head CT. Three patients with skull base fracture, but concomitant negative parenchymal findings, were included in mTBI group.
Inclusion criteria for the orthopedic group were age ≥16 years, and acute orthopedic nontrivial injury or injuries without any signs of acute CNS involvement. Exclusion criteria were any suspicion of an acute TBI (injury signs in the head, any suspicion of TBI signs at the time of injury, symptoms suggesting a possible TBI), previous TBIs or brain diseases, polytrauma needing intensive care, or trivial injuries not needing acute measures or follow-up. mTBI was diagnosed if the patient had sustained a brain injury that fulfilled the American Congress of Rehabilitation Medicine (ACRM) criteria for TBI 25 and that patient's lowest recorded Glasgow Coma Score (GCS) was ≥13. However, patients with GCS of 13 and deteriorating or patients with GCS of 13 and concomitant multitrauma needing intensive care were excluded from the mTBI group. If there was any suspicion that the signs of TBI could be caused by confounders (inebriation, medications) the patient was not included.
One patient with an orthopedic injury was sedated with propofol because of an orthopedic operation before the blood samples were obtained, whereas other patients did not receive anesthetics before the initial sample was obtained. None of those who had high GFAP and/or UCH-L1 levels underwent general anesthesia.
The study protocol was approved by the ethical review board of Hospital District of South-West Finland, the Cambridgeshire 2 Research Ethics, and the Norfolk Research Ethics Committee.
All patients were given necessary information about the study in both oral and written form, and written informed consent was obtained.
Analysis of GFAP and UCH-L1
Blood samples for GFAP and UCH-L1 were collected upon arrival and on days 1, 2, 3, and 7 (when available) after the admission, and on the follow-up visit 3–10 months after the injury. We did not recruit patients during the night. In case a patient was recruited >24 h after admission, samples were considered taken on day 1 after the injury. It was possible to obtain longitudinal samples from several patients with mTBI because they were admitted as a result of prolonged symptoms. The samples were centrifuged for 10 min at 10,000 rpm at 4°C, and the serum was immediately frozen at −70°C for further analysis.
Proteomic analyses were conducted at Randox Laboratories Ltd (Crumlin, County Antrim, United Kingdom) with Randox Biochip technology, which is a solid-state device containing an array of discrete test regions of immobilized antibodies specific to different cerebral immunoassays. The samples were prepared singly. Increased levels in a specimen led to increased binding of antibody labeled with horseradish peroxidase and, therefore, an increase in the chemiluminescent signal emitted. The light signal generated from each of the test regions on a biochip was detected with digital imaging technology and compared with that from a stored calibration curve. The concentration of analyst present in the sample was calculated from the calibration curve. The Evidence Investigator Cerebral Custom Array IV (Randox Laboratories Ltd) was used to quantitatively test for UCH-L1 and GFAP simultaneously.
The lower limits of quantification were 0.3 ng/mL and 0.16 ng/mL, and the upper limits were 50 ng/mL and 100 ng/mL for UCH-L1 and GFAP, respectively. For the UCH-L1 assay, coefficient of variation was 6–7% and for GFAP assay it was 3–4%. The samples with no detectable biomarker levels were assigned a value of zero.
MRI
Most patients with orthopedic trauma (n = 52/73) underwent head MRI during the first 4 weeks after their injury as part of the study protocol as well as at the follow-up visit 3–10 months after the injury. The included 3T MRI sequences were T13D, T2, fluid-attenuated inversion recovery (FLAIR), susceptibility-weighted imaging (SWI), diffusion-weighted imaging (DWI), and diffusion tensor imaging (DTI).
Statistical analyses
The normality of UCH-L1, GFAP, age, and injury severity score were assessed using Kolmogorov–Smirnov test and by visually inspecting histograms. Nonparametric methods were used in the further analyses, because these variables were not normally distributed. Differences in background variables between patients with orthopedic injury and patients with mTBI were studied using the Mann–Whitney U test for age and injury severity score and the χ2 test for gender. Spearman correlation coefficient was used to assess the correlation between GFAP and UCH-L1 on different days in patients with orthopedic injury. Association of the biomarkers on arrival and background variables were assessed using Spearman correlation coefficients (age, injury severity score) and Mann–Whitney U test (gender).
Given that we wished to explore the ability of these protein biomarkers to distinguish CT-negative mTBI from extracranial injury, we chose not to define diagnostic thresholds based on values from healthy subjects, but rather on values obtained in patients with extracranial orthopedic injuries. The cutoff value for an individual biomarker was set at the 95th percentile, which is determined theoretically based on a previous publication 26 in order to provide a basis to undertake more detailed exploratory analysis in subjects with high levels of UCH-L1 and GFAP in the orthopedic injury population.
MRI findings were also studied in the orthopedic injury population. MRI findings were categorized as MRI not done, normal MRI findings, and abnormal MRI findings. Differences in the biomarkers among these categories were studied with the Kruskal–Wallis test. Mann–Whitney U test was used to study differences in GFAP and UCH-L1 values between patients with orthopedic injuries and patients with mTBI. Ability of the biomarkers to differentiate these two patient groups was evaluated using the receiver operating characteristics curve (ROC) and the area under the ROC curve (AUC). Levels of UCH-L1 and GFAP on arrival were compared with levels on day 1 and follow-up with Wilcoxon signed rank test. Differences in biomarker levels among patients with orthopedic injuries, patients with CT-negative mTBI and concomitant orthopedic injuries, and patients with isolated CT-negative mTBI were studied using the Kruskal–Wallis test. Data were analyzed using IBM SPSS Statistics 22 (IBM Corp, New York) and Matlab R2012b (MathWorks, Natick, MA).
Results
The demographic features, mechanisms of injuries, injury severity scores, 29 and injury types of the two study groups are shown in Table 1. The mean age of the patients with orthopedic injury was 46.7 ± 18.3 years and the majority was female (55%). In patients with orthopedic injury, the most common injuries were ankle fractures 29% (n = 21), upper or lower extremity soft tissue contusions and bruises 14% (n = 10), and wrist fractures 10% (n = 7). The mean age of the patients with CT-negative mTBI was 42.1 ± 18.6 years and the majority was male (63%). In the mTBI group, 43 patients (47%) had a concomitant orthopedic injury.
Percentages of the injuries are in parentheses; values are expressed as mean ± standard deviation or number of subjects (percentage of subjects); percentages do not sum up to 100% because some subjects had several mechanisms or several extracerebral injuries.
Orthopedic, patients with orthopedic injury; mTBI, patients with mild traumatic brain injury
Levels of UCH-L1 and GFAP
Most of the patients with orthopedic injury had GFAP and UCH-L1 levels available on arrival, on the following day and at the follow-up visit.
Figure 1 presents biomarker levels on different days in patients with orthopedic trauma. Figure 2 shows scatter plots of UCH-L1 and GFAP and Spearman correlation coefficients between the biomarkers in the same subjects. Multiple subjects had identical values of UCH-L1 and GFAP; therefore, the number of plotted dots in the panels of Figure 2 seems to be smaller than the number of subjects. Significant correlations between UCH-L1 and GFAP levels were found upon arrival (Spearman ρ 0.739, p < 0.001), on day 1 (Spearman ρ 0.544, p = 0.004), and at the follow-up visit (Spearman ρ 0.382, p = 0.007). Figures S1 and S2 show relations between the biomarkers and gender, age, and injury severity score in patients with orthopedic injury and patients with CT-negative mTBI on arrival day (see online supplementary material at
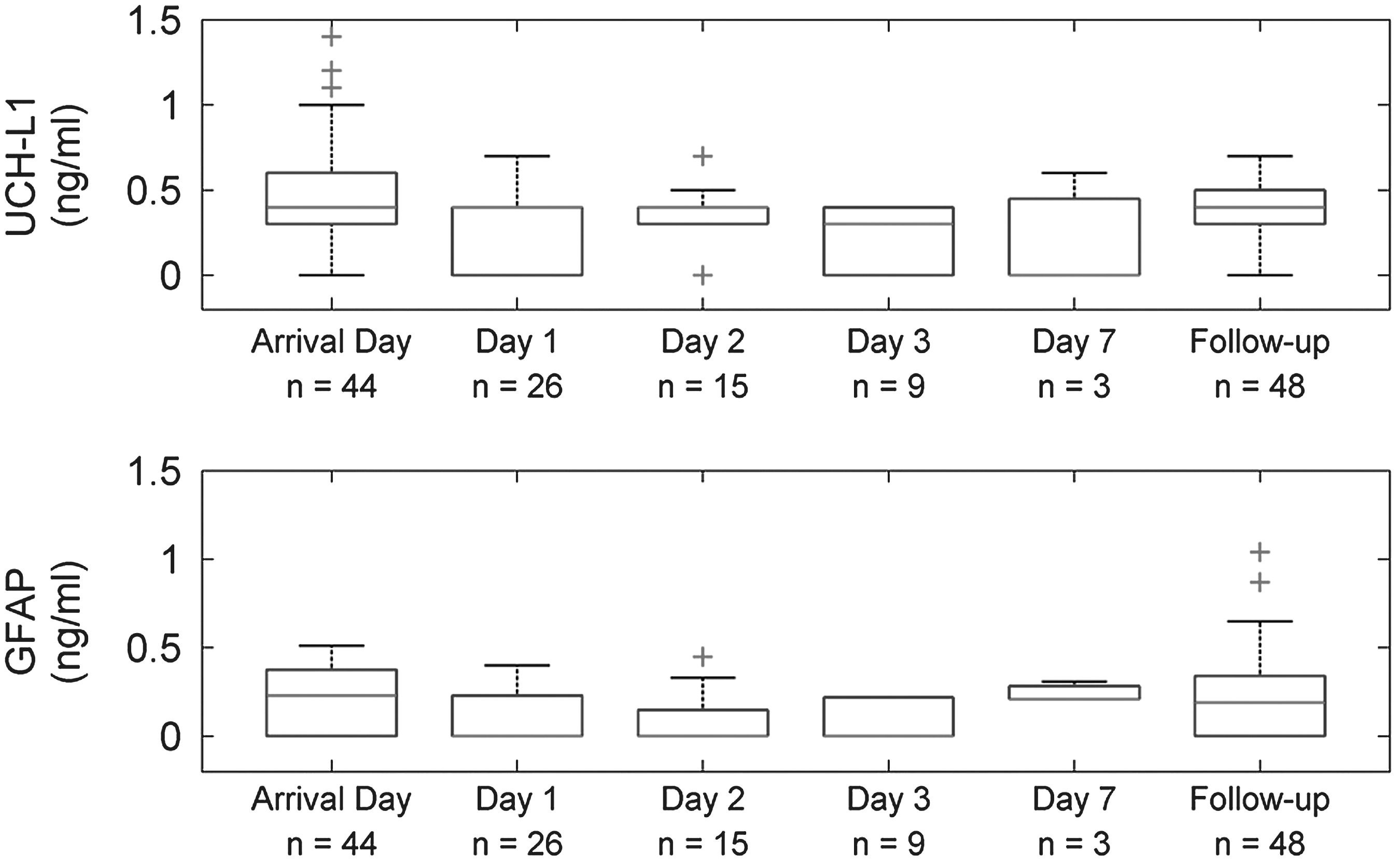
Levels of ubiquitin C-terminal hydrolase-L1 (UCH-L1) and glial fibrillary acidic protein (GFAP) on different days in patients with orthopedic trauma (y-axis zoomed). Box plots represent medians in nanograms per milliliter and interquartile ranges.
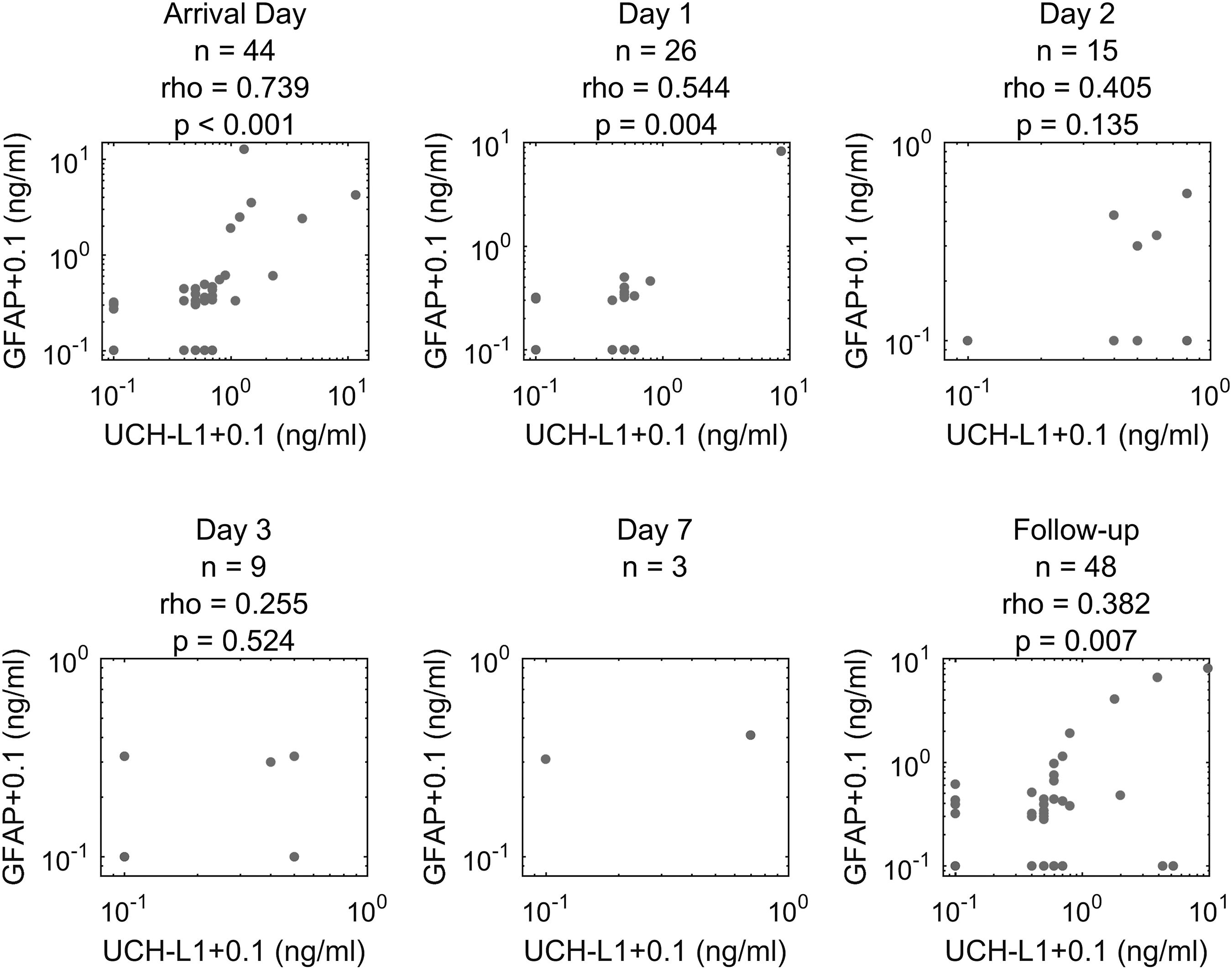
Spearman correlations coefficients (ρ) between ubiquitin C-terminal hydrolase-L1 (UCH-L1) and glial fibrillary acidic protein (GFAP) levels in patients with orthopedic trauma on different days. p, p value of rho; n, number of subjects.
Table 2 shows in more detail the biomarker levels of those patients with orthopedic injuries who presented with GFAP or UCH-L1 levels in the 95th percentile (n = 6, 8%, UCH-L1 ≥ 2.74 ng/mL or GFAP ≥3.61 ng/mL) along with details of their demographics, comorbidities, current and previous injuries, and MRI findings. All patients were female and had injuries in the extremities. Four out of six subjects (67%) showed levels for both GFAP and UCH-L1 in the 95th percentile. Five out of six patients (83%) had fractures in the distal part of the extremities, whereas one patient had only superficial injuries of the extremities. Of those six patients who showed high levels during the first post-injury week, five (83%) showed an elevated level of either one or both biomarkers also at the follow-up visit (Table 2).
Values are presented as nanograms per milliliter. T13D, T2, fluid-attenuated inversion recovery (FLAIR), susceptibility-weighted imaging (SWI), diffusion-weighted imaging (DWI), and diffusion tensor imaging (DTI) sequences were utilized and used to confirm the absence of brain pathology. Patients with particular biomarkers with high levels at the follow-up visit and during the hospital stay have shaded background.
GFAP, glial fibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase-L1.
Within the CT-negative mTBI group, only one patient showed biomarker levels that were in the 95th percentile defined in the orthopedic controls (UCH-L1 ≥ 2.74 ng/mL or GFAP ≥3.61 ng/mL). This patient was a previously healthy 21-year-old male who did not have extracranial injuries. His UCH-L1 level was 3.50 ng/mL and his GFAP level was 0 ng/mL on arrival day, whereas the corresponding levels were 0.80 ng/mL and 1.31 ng/mL on the follow-up visit. Those three patients who had a skull base fracture without intracranial abnormalities did not have biomarker values differing from other patients with mTBI.
MRI findings
In patients with orthopedic trauma, 52 patients (71%) underwent MRI imaging of the head. Thirty patients (58%) had normal findings, the rest showing nonspecific ischemic-degenerative changes or other insignificant abnormalities, and in one case an old contusion was suspected. None was found to have any imaging changes compatible with an acute TBI. Four out of six patients (67%) with levels of UCH-L1 or GFAP in the 95th percentile underwent head MRI, and their findings were normal. The only patient with mTBI, whose UCH-L1 level was in the 95th percentile on arrival, had normal head MRI.
Table 3 presents the MRI findings in the patients with orthopedic injuries. Table 4 shows levels of UCH-L1 and GFAP in three MRI finding classes in the population of the orthopedic patients: MRI not done, normal MRI findings, and abnormal MRI findings. Levels of UCH-L1 and GFAP did not differ significantly among the three classes.
T13D, T2, fluid-attenuated inversion recovery (FLAIR), susceptibility-weighted imaging (SWI), diffusion-weighted imaging (DWI), and diffusion tensor imaging (DTI) sequences were utilized and used to confirm the absence of brain pathology.
Values are presented as median in nanograms per milliliter (25th percentile; 75th percentile; 95th percentile); p value from Kruskal–Wallis test. Days 3 and 7 are not presented because of the low number of samples.
GFAP, glial fibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase-L1.
Comparison between patients with orthopedic trauma and those with CT-negative mTBI
The levels of GFAP were higher in patients with orthopedic trauma than in patients with CT-negative mTBI on arrival day (p = 0.026); however, there were no difference on the following days (Fig. 3). The levels of UCH-L1 were not significantly different between patients with CT-negative mTBI and patients with orthopedic injury. As a result of this, GFAP levels on arrival day were able to modestly discriminate the patient groups in receiver operating characteristic analysis (AUC = 0.629, 95% CI 0.514, 0.731) (Fig. 4 and Table 5).
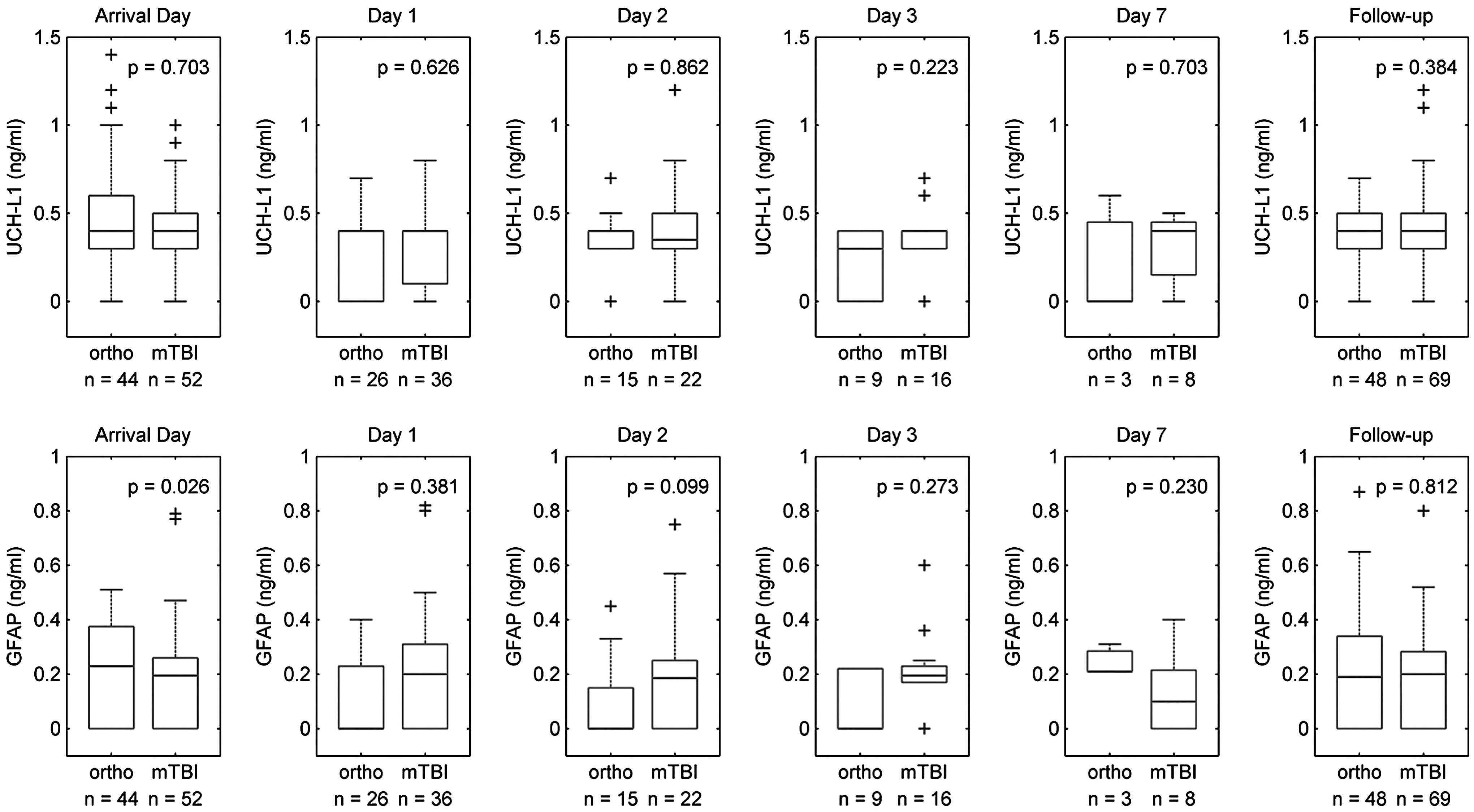
Levels of glial fibrillary acidic protein (GFAP) and ubiquitin C-terminal hydrolase-L1 (UCH-L1) in patients with orthopedic injury (ortho) and CT-negative mild traumatic brain injury (mTBI). Box plots represent medians in nanograms per milliliter and interquartile ranges.
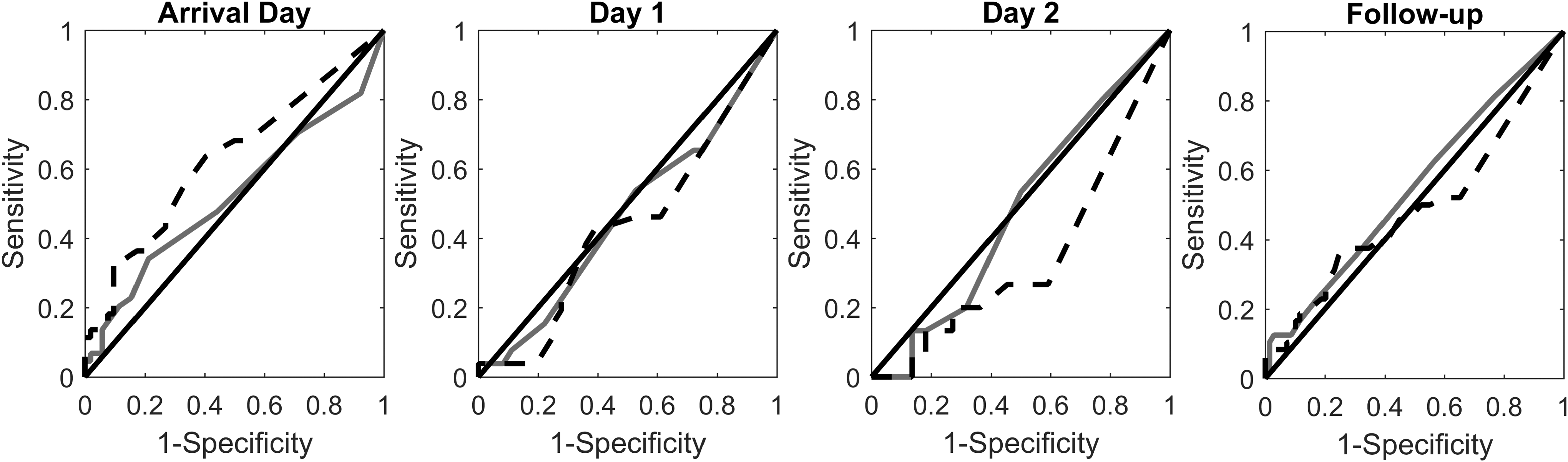
Receiver operating characteristic curves for distinguishing orthopedic patients from patients with CT-negative mild traumatic brain injury Days 3 and 7 are not shown due to the sample size. GFAP, dashed line; UCH-L1, solid line. For numeral values see Table 5.
Days 3 and 7 are not shown because of the small sample size. Significant AUC in bold.
GFAP, glial fibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase-L1; AUC, area under the receiver operating characteristic curve; CI, confidence interval; n (ortho), number of orthopedic patients; n (mTBI), number of patients with CT-negative mild traumatic brain injury.
Table 6 shows differences in UCH-L1 and GFAP levels over time. Levels of UCH-L1 were significantly lower on day 1 and follow-up than on arrival day in patients with CT-negative mTBI, whereas significant differences in the levels of GFAP were not observed. There were no significant differences over time in the levels of GFAP and UCH-L1 in patients with orthopedic injury, Figure 5 presents changes in levels of UCH-L1 and GFAP between arrival and follow-up in CT-negative mTBI and orthopedic injury populations. There were no statistically significant differences in levels of GFAP and UCH-L1 among patients with orthopedic injuries, patients with CT-negative mTBI and concomitant orthopedic injuries, and patients with isolated CT-negative mTBI (Fig. S3) (see online supplementary material at
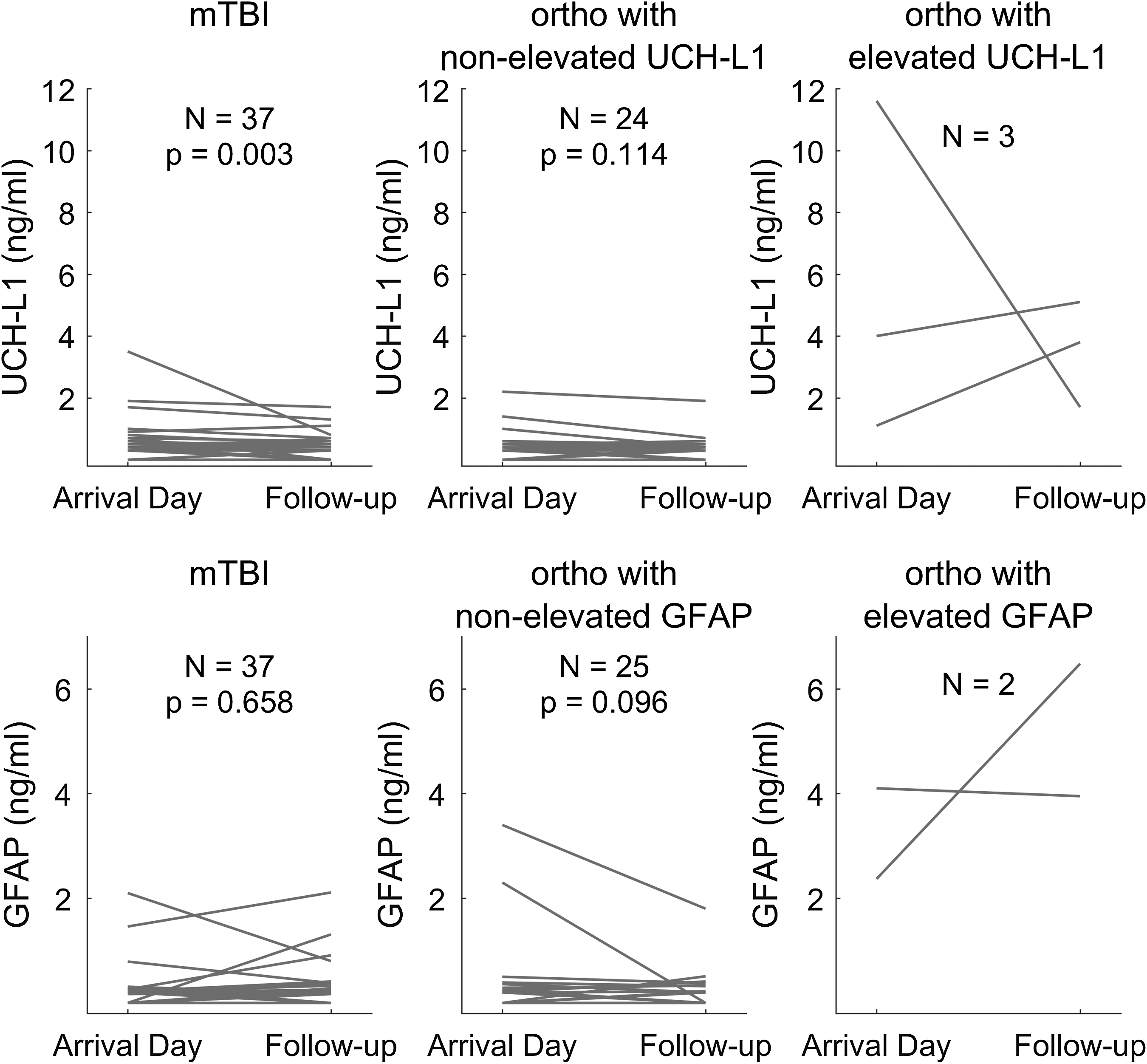
Changes in levels of biomarkers between the arrival and the follow-up in patients with CT-negative mild traumatic brain injury (mTBI), orthopedic injury, and with non-elevated (below the 95th percentile) (ortho with non-elevated) and elevated biomarker levels (in the 95th percentile) (ortho with elevated).
The table shows changes in UCH-L1 and GFAP levels between arrival day and day 1 and arrival day and follow-up visit.
n, number of subjects with proteomics levels at both time points; p values from Wilcoxon signed rank test.
p < 0.05. Other value are expressed as median (25th; 75th percentile).
GFAP, glial fibrillary acidic protein; UCH-L1, ubiquitin C-terminal hydrolase-L1; mTBI, mild traumatic brain injury.
Discussion
This prospective, observational, two-center study assessed the serum levels of GFAP and UCH-L1 in patients with acute orthopedic injury and compared the results with those from patients with CT-negative mTBI. Our main finding was that the levels of these biomarkers were unable, in a clinically relevant sense, to separate these groups and thus provide any diagnostic benefit for the common problem of determining whether a patient with acute injury has a concomitant TBI or not. Additionally, the levels of the biomarkers were not able to discriminate patients with orthopedic injuries, patients with CT-negative mTBI and concomitant orthopedic injuries, and patients with isolated CT-negative mTBI. Another main finding was that in patients with orthopedic injury, high levels of these biomarkers tended to persist between the acute phase and follow-up visit several months later, suggesting that some people have clearly higher levels than others, irrespective of any injury. All the patients with orthopedic injury who had biomarker levels in the 95th percentile were females with injuries in the extremities. Of 52 patients with orthopedic injuries who underwent MRI imaging of the head, 30 patients had normal findings, whereas the rest showed nonspecific ischemic-degenerative changes or other insignificant abnormalities. None of these findings were suggestive of an acute TBI, which was carefully excluded clinically as well. Additionally, the only patient with CT-negative mTBI and high biomarker value had normal MRI findings.
There are many previous studies that have explored the correlation of GFAP and UCH-L1 levels with different severity classes of TBIs, although the validation in mTBI is incomplete, as the controls have generally been healthy volunteers, and when non-CNS trauma controls have been used, numbers have been small and patients have been poorly characterized, and the comparison has generally been with moTBI and sTBI rather than with mTBI, which is the real diagnostic differentiation we are seeking in the current study. Several studies have explored the potential of GFAP and UCH-L1 in the diagnostics and outcome prediction of TBI with promising results. 7,8,24,28,29 In some studies, which have included orthopedic injury patients without TBI, low but measurable levels of GFAP 7,21,30,31 and UCH-L1 8,21,22,29 have been detected in these patients. In two studies, the levels of GFAP 7 and UCH-L1 8 were higher in patients with orthopedic trauma than in uninjured controls, and there were significant differences between the uninjured controls and all other groups, including orthopedic controls and different severities of TBI. 7,8 Papa and coworkers reported that GFAP breakdown product levels were significantly higher in patients with CT-positive findings than those with CT-negative finding irrespective of orthopedic injury, mTBI, or moTBI. Further, they reported that patients with CT-negative mTBI and moTBI had significantly higher levels of GFAP breakdown product levels than patients with orthopedic injury, although they did not provide median and p values. 7 Another study by the same group investigating the performance of UCH-L1 in patients from the same centers reported that UCH-L1 levels in patients with CT-negative TBI (mTBI and moTBI) had higher levels of UCH-L1 than trauma controls with a negative CT (p = 0.057). 8 These findings are inconsistent with our current results. However, another earlier study reported that UCH-L1 levels could not distinguish uninjured controls from patients with mTBI when analyzed with two different immunoassays. 17 In a recent publication, Papa and coworkers reported very promising results regarding performance of GFAP and UCH-L1 in discrimination of patients with orthopedic injuries and patients with CT-negative and CT-positive mTBI and moTBI. 21 The study differs from our current study in terms of the TBI populations, but in some of their orthopedic trauma controls, Papa and colleagues detected high UCH-L1 levels (range 0.045–4.241 ng/mL), which is parallel with our findings.
We used a different assay than that used by these authors, which may make cross- study comparisons (e.g., our controls with those from other studies) difficult. However, the key findings of our analysis should not be affected, as it relies on within-study comparisons performed using a single analytic platform. We found that in patients with orthopedic trauma, there were significant correlations between GFAP and UCH-L1 levels on arrival day, day 1, and the follow-up visit. The only significant difference in the biomarker levels over time was observed in patients with CT-negative mTBI: the levels of UCH-L1 were significantly lower on day 1 and follow-up than on arrival day. Our results suggest that the relatively high levels of GFAP and UCH-L1 found in some of the patients with orthopedic trauma are not related to their acute injury, because the injuries were very heterogeneous and the levels were still elevated during the outcome visit several months after the injury. Excluding the recent article by Papa and coworkers, 21 the other aforementioned groups did not measure GFAP and UCH-L1 levels of patients with orthopedic trauma at different time points, and they did not assess their correlations.
An interesting finding is that all the patients with orthopedic injury who had GFAP and UCH-L1 levels in the 95th percentile were females, and most of them had persistently high biomarker values on the follow-up visit. On arrival, female patients with orthopedic injury had significantly higher levels of UCH-L1 than male patients. The reason for this difference remains unexplained. However, when both genders were analyzed together, patients with orthopedic injury had higher GFAP levels than patients with mTBI, whereas no statistical difference was observed in UCH-L1 levels on arrival.
Both GFAP and UCH-L1 were originally presumed to be specific to the CNS, but subsequently, GFAP has been detected also in non-glial and non-CNS cells, such as Schwann cells, 32 chondrocytes, 33 fibroblasts, 33 myoepithelial cells, 34 lymphocytes, 35 and liver stellate cells, 36,37 whereas expression of UCH-L1 outside the CNS has been reported in cells of the testis, ovaries, and kidney, 15,19 Based on studies on knockout mice, UCH-L1 appears to have an integral role in the structure and function of the neuromuscular junction. 38 Despite this, GFAP and UCH-L1 have generally been considered specific for TBI in terms of TBI diagnostics. 7 –9,31 The most studied astroglial TBI biomarker S100β is a Ca2+-binding protein that regulates intracellular levels of calcium in glia and oligodendrocytes. 39 S100β remains a promising diagnostic tool for TBI, as it has excellent negative predictive value for pathological intracranial CT findings; 40 however, its lack of specificity to intracranial injuries has caused concerns. 41 –43 Like GFAP and UCH-L1, expression of S100β has been detected outside of the CNS, such as in adipocytes and chondrocytes; 39 however, it has been reported to be inferior in detecting intracranial injuries in comparison with GFAP in patients with mTBI 9 and sTBI, 8,22 and in multitrauma patients with TBI. 23
Even though GFAP and UCH-L1 may mostly be of CNS origin, they are not TBI specific. Elevated levels of GFAP and UCH-L1 have been reported after seizures 44,45 and stroke. 46 High plasma levels of GFAP have been associated with neuroepithelial tumors, such gliomas 47 and ependymomas. 48 However, in a recent study, Kiviniemi and coworkers investigated the association of GFAP with prognostic markers in patients with high-grade gliomas. In their healthy control population, all subjects but one had unmeasurable GFAP levels (detection limit 0.014 ng/mL). This subject had substantially higher level of GFAP than the median level of patients with high-grade glioma. 20
We recently reported that in a TBI population of all severities, UCH-L1 and GFAP levels were able to discriminate patients with unfavorable outcome (Glasgow Outcome Scale 1–3) from patients with favorable outcome (Glasgow outcome scale 4–5). In that study, the cutoff value of UCH-L1 for unfavorable outcome was 1.03 ng/mL, 49 whereas a cutoff value of 1.89 ng/mL has been reported to predict in-hospital mortality in another study. 6 Similarly, we reported a cutoff value of GFAP for unfavorable outcome at 1.26 ng/mL, 49 whereas values >1.5 ng/mL were reported to be predictive of mortality by another group. 50 The median levels of UCH-L1 and GFAP in our orthopedic injury population are relatively comparable with those reported earlier by Papa and coworkers. 7,8 Intriguingly, the circulating levels obtained in our study are consistent with those from the aforementioned research. Therefore, our results show that patients with acute orthopedic injury may often show levels of GFAP and UCH-L1 that overlap with those obtained from patients with mTBI and, if these biomarkers are used as a diagnostic tool, they may predispose these patients to unwarranted diagnostics and recurrent head imaging. This article does not address the role of these biomarkers in assessing different subgroups of patients with mTBI or more severe TBI.
All patients with levels of UCH-L1 and GFAP in the 95th percentile, who had MRI available (67%), had normal imaging findings. None of these patients had history of epilepsy or seizures related to their current injuries and none them had intracranial tumors. Based on this finding, it seems obvious that elevated levels of these biomarkers do not reflect any acute brain condition in these patients. This raises three possible explanations and interferences.
First, a potential extracerebral origin for these elevations might be supported by the results from previous studies indicating that the levels of GFAP 7 and UCH-L1 8 were higher in patients with orthopedic injuries than in healthy controls. Hainfellner and coworkers reported staining of chondrocytes and fibroblasts with anti-GFAP antibodies in epiglottis and ligamentum flavum in vitro. 35 Fellenberg and coworkers reported that UCH-L1 was richly expressed in bone marrow-derived mesenchymal cell samples, 51 and Hsu and coworkers were able to detect UCH-L1 in skin fibroblasts of patients with spinal muscular atrophy in vitro. 52 Therefore, one potential explanation for our current results is the expression of GFAP and UCH-L1 in chondrocytes and fibroblasts of extremity joint cartilage and bone marrow, which results in serum elevation of GFAP and UCH-L1 in peripheral blood after traumatic fractures. This explanation can be brought further by a possibility of traumatic peripheral neuropathy, because GFAP and UCH-L1 may be expressed in Schwann cells and the neuromuscular junction. 32,38 Regrettably, we have no clinical data available on possible development of symptoms of neuropathy, and electrophysiological tests were not undertaken in these patients, which is why this explanation remains theoretical.
Second, some orthopedic patients might have had a concomitant mTBI by current definitions that remained undetected. However, this is very unlikely, as none of these patients had a history suggesting any TBI; that is, all diagnostic criteria for a TBI were lacking, as was any suspicion of the presence of these criteria. In addition, none of the controls showed external signs of head or neck injury, showed any symptoms suggesting a possible concussion, or were involved in a high-energy trauma. Also their MRI showed no acute changes, even in patients with elevated biomarkers. Further, as the controls were recruited in the study, they were carefully interviewed about the details of their injury and their histories were reviewed.
Third, some of the orthopedic patients had a nontraumatic CNS insult caused by the consequences of peripheral trauma; for example, the cytokine and neurohumoral storm associated with their orthopedic injury. It has been previously reported that orthopedic injuries may result in elevated proinflammatory interleukin-1β and interleukin-8 production, leading to CNS inflammation response. 53,54
Because in both the orthopedic injury and mTBI groups several subjects continued to show elevated levels several months after the injury – substantially later than could be explained with the half-life of these biomarkers in blood – it seems more likely that the individual high levels seen in our study are not related to these patients' acute injuries.
Even though these data provide new insights concerning biochemical diagnostic challenges in diagnostics of CT-negative mTBI, and demonstrate for the first time that some patients seem to exhibit high levels of GFAP and UCH-L1 irrespective of any injury that tends to persist, the authors recognize that there are limitations to this study. In this study, levels of biomarkers were not compared with those of healthy controls, which would have given more information about possible differences between uninjured patients and studied populations. Another limitation is that we have used custom arrays in assessments of biomarkers, and, therefore, the manufacturer has not been able to provide values for the lower limit of detection. Further, we did not recruit patients during the night, which is why some of the first samples are taken on day 1. On the other hand, many patients with milder injuries do not seek medical attention immediately, but only after a variable delay.
Our main finding was that GFAP and UCH-L1 are not specific biomarkers for mTBI, and that their levels are not clinically relevantly able to discriminate patients with CT-negative mTBI and patients with acute orthopedic trauma. Many patients with orthopedic injury had higher biomarker levels than patients with CT-negative mTBI. The source of high GFAP and UCH-L1 levels in these patients remains unknown, but persistent elevation several months after the injury suggests a source that is not related to the injury. Our results cast a significant doubt on the diagnostic value of these biomarkers in the differential diagnostics of CT-negative mTBI.
Footnotes
Acknowledgments
This work was partially funded by the European Commission under the 7th Framework Programme (FP7-270259-TBIcare), personal Government's Special Financial Transfer tied to academic research in Health Sciences (J.P.P. and R.S.K.T.), personal EVO funding and grant from Maire Taponen Foundation (J.P.P.), Health Foundation/Academy of Medical Sciences Clinician Scientist Fellowship (V.N.), National Institute for Health Research (NIHR) Research Fellowship (P.J.H.) The authors thank research nurses Patricia Bertenyi and Satu Timlin for their valuable contribution to this study.
Author Disclosure Statement
Jussi P. Posti has no financial disclosures. He has received financial support in the form of a congress fee and travel expenses paid by Skulle Implants Ltd.; Iftakher Hossain has no financial disclosures; Riikka S.K. Takala has no financial disclosures. She has received speakers' fees from Abbott, Fresenius-Kabi, and UCB Pharma Finland Ltd. and conference funding from Pfizer, and is a stockholder of Orion Plc.; Hilkka Liedes has no financial disclosures; Virginia Newcombe has no financial disclosures; Joanne Outtrim has no financial disclosures; Ari J. Katila has no financial disclosures; Janek Frantzén has no financial disclosures; Henna Ala-Seppälä has no financial disclosures; Jonathan P. Coles has no financial disclosures; Anna Kyllönen has no financial disclosures; Henna-Riikka Maanpää has no financial disclosures; Jussi Tallus has no financial disclosures; Peter J. Hutchinson is a director of Technicam and supported by an NIHR Research Professorship and the NIHR Cambridge Biomedical Research Centre; Mark van Gils has no financial disclosures; David K. Menon has no financial disclosures; Olli Tenovuo has no financial disclosures. He has received a speaker fee from Orion Corporation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.