
Abstract
Traumatic brain injury (TBI) frequently triggers a disruption of cerebral autoregulation. The cerebral perfusion pressure (CPP) at which autoregulation is optimal (“CPPopt”) varies between individuals, and can be calculated based on fluctuations between arterial blood pressure and intracranial pressure. This review assesses the effect of individualizing CPP targets to pressure reactivity index (a measure of autoregulation) in patients with TBI. Cochrane Central Register of Controlled Trials, MEDLINE®, Embase, and Cumulative Index of Nursing and Allied Health Literature were searched in March 2015 for studies assessing the effect of targeting CPPopt in TBI. We included all studies that assessed the impact of targeting CPPopt on outcomes including mortality, neurological outcome, and physiological changes. Risk of bias was assessed using the RTI Item Bank and evidence quality was considered using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria. Eight cohort studies (based on six distinct data sets) assessing the association between CPPopt and mortality, Glasgow Outcome Scale and physiological measures in TBI were included. The quality of evidence was deemed very low based on the GRADE criteria. Although the data suggest an association between variation from CPPopt and poor clinical outcome at 6 months, the quality of evidence prevents firm conclusions, particularly regarding causality, from being drawn. Available data suggest that targeting CPPopt might represent a technique to improve outcomes following TBI, but currently there is insufficient high-quality data to support a recommendation for use in clinical practice. Further prospective, randomized controlled studies should be undertaken to clarify its role in the acute management of TBI.
Introduction
T
Following TBI, maintenance of appropriate cerebral blood flow is imperative to mitigate against the relative adverse effects of ischemia and hyperemia. In healthy states, the cerebral vasculature compensates for variations in systemic blood pressure and cerebral metabolic requirements with judicious alterations of blood vessel diameter, which is known as autoregulation. 2 In injured brains, this autoregulation can be impaired, and observational studies have demonstrated a relationship between loss of autoregulation and poor outcome. 3 –6
In patients with poor intracranial compliance, changes in cerebral blood volume, as dictated by vessel diameter, are expressed as variations in intracranial pressure (ICP). By analyzing the dynamic relationship between mean arterial pressure (MAP) and ICP over a given time period (the length may be chosen arbitrarily, but it should be substantially longer than the respiratory and pulse period), an appreciation of cerebrovascular pressure reactivity can be gained, providing information about the integrity of autoregulation. 7 Perhaps the best known calculated index of cerebral autoregulation is the pressure reactivity index (PRx), which is the correlation coefficient between ICP and arterial pressure using 10 sec-averaged samples as data points and calculating correlation coefficients using a 5 min data window.
Measurement of PRx allows an assessment of the effect of various therapeutic maneuvers on autoregulation. Changes in cerebral perfusion pressure (CPP), 8 temperature, 9 and respiration 10 modulate autoregulation, as does the use of certain anesthetic agents. 11,12
Investigation into the effect of CPP on autoregulation has led to the discovery that the CPP at which autoregulation is best preserved (“optimal CPP” or “CPPopt”) varies both among individuals, and throughout time in an individual patient. 13 Certain neurocritical care units utilize CPPopt techniques as an adjunct to standard care, in order to tailor CPP targets to each patient. To date, however, there are no systematic reviews assessing its clinical utility.
The objective of this systematic review is to determine the effect on mortality and functional recovery of individualizing CPP targets to optimal PRx, compared with standard CPP targets in patients with moderate to severe TBI.
Methods
This review was conducted and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement.
14
Details of the protocol for this systematic review were registered on PROSPERO (registration number CRD42014013048) and can be accessed at
The review is being prepared as part of the CENTER-TBI project, a large European research project that aims to improve the care for patients with TBI. 1,15,16
Information sources
Using the National Health Service (NHS) Library Healthcare Database search engine, the following databases were searched up to March 2015: Cochrane Central Register of Controlled Trials, MEDLINE®, Embase, and Cumulative Index of Nursing and Allied Health Literature. There were no language or date restrictions, and we included studies irrespective of publication status. The search strategy was developed in consultation with a search expert using the following combination of subject headings and keywords: (
Gray literature, ongoing trials, and conference abstracts were searched for via The ClinicalTrials.gov registry, Google Scholar, and abstracts from neurocritical care and international neurotrauma conferences. Reference lists from included studies and other pertinent articles were screened, and citation tracking of included studies (via Scopus) was conducted. Experts leading research into cerebrovascular reactivity were consulted to identify any unpublished data.
Study selection
We included randomized controlled trials (RCTs), quasi-RCTs, controlled clinical trials (CCTs), and observational studies with a control group (i.e., cohort studies and case–control studies) that investigated the effect on one or more of our relevant outcomes of targeting CPPopt in patients with moderate to severe TBI. These outcomes included: mortality, functional outcomes (e.g., Glasgow Outcome Scale [GOS]), and physiological measures (such as brain tissue oximetry). Although we recognize the limitations of including observational studies in a systematic review of intervention effectiveness, an anticipated lack of controlled trials necessitated this decision in order to comprehensively evaluate the available data. We included all age groups and any methods for calculating CPPopt. Studies not measuring any of our prespecified outcomes were excluded.
The first author (E.N.) screened all search results on citation, and removed clearly irrelevant articles. Two authors (E.N., V.N.) then independently screened the remaining citations and abstracts identified to determine their eligibility for inclusion. Agreed citations were retrieved in full text and reviewed by the two authors independently; any disagreement was resolved by discussion until consensus was reached.
Data collection and assessment of risk of bias
Two authors (E.N., C.M.) independently assessed the risk of bias of included studies; disagreement was resolved by discussion until consensus was reached. Data extraction was conducted by E.N. and corroborated by C.M. The following data were extracted from the studies: study characteristics (including site and year), study participants (e.g., number, age, severity), method for calculating CPPopt, and clinical outcomes.
Where dichotomous data were available, we presented it as risk ratios (RR) with p values. Continuous data were presented in the form that they appeared in in the original publication.
Risk of bias was assessed using the RTI item bank. 18 The RTI item bank assesses risk of bias based on 12 domains. Each domain is rated as having low, high, or unclear risk of bias, according to specific criteria.
Data synthesis
To synthesize the data, we grouped studies by outcome, and considered the results of each study contributing to that outcome. Because of the heterogeneity of design and outcome measures, we report the results in a narrative manner, rather than performing meta-analysis. Where studies used shared or overlapping data sets, this is highlighted. The risk of bias of included studies was used to inform an assessment of the quality of the evidence contributing to each outcome, as per the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach. 19 According to the GRADE approach, observational research is considered to be low-quality evidence that may be downgraded further (or in rare instances upgraded) according to specific criteria.
Two authors (E.N., A.J.S.) independently applied the GRADE criteria for each outcome and reached agreement through discussion (Table S1) (see online supplementary material at
Results
Study selection
A total of 2022 de-duplicated citations were identified, with 74 titles included on citation and abstract, and 22 retrieved in full text. Of these, 12 studies did not address the relationship between CPPopt and a clinically relevant outcome, and two abstracts
20,21
reported the same data as full text reports;
22,23
therefore, these were also excluded (Table S2) (see online supplementary material at
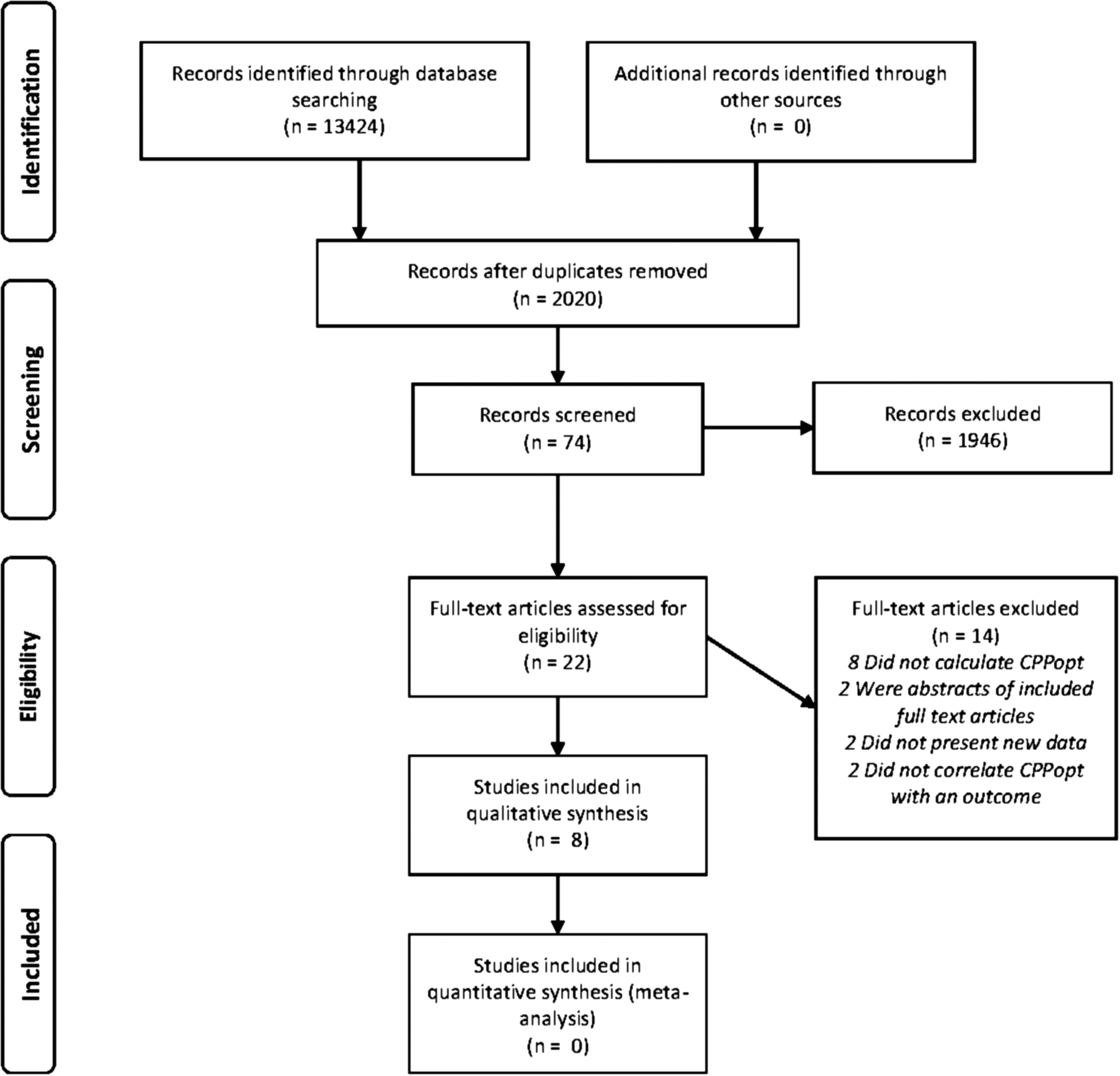
Flow diagram of study selection process. CPPopt, optimal cerebral perfusion pressure.
Study characteristics
We included eight study reports, assessing the effect of CPPopt in 972 patients with moderate to severe TBI (Table 1). One study group (Cambridge, UK) published three articles using overlapping, but not identical, data sets. 22,24,25 Because of overlap of patients in these three studies, we collated them as the “Cambridge Cohort.” Therefore, there were six entirely distinct data sets. All studies took place in academic neuroscience centers in high-income countries. No studies assessed the use of CPPopt in children. All studies used a cohort design, with six studies retrospectively analyzing prospectively gathered observational data. 22 –27 The remaining two were prospective studies; one assessed the feasibility of adhering to a CPPopt-guided protocol, 28 and the other assessed the effects of targeting CPPopt on the partial pressure of brain tissue oxygen (PbrO2). 29 No study directly compared a CPPopt-guided protocol with standard CPP targets.
CPPopt, optimal cerebral perfusion pressure; DATCAR (LAx), dynamic adaptive target of active cerebral autoregulation (low-resolution autoregulation index); GOS, Glasgow Outcome Scale; ICM+ PRx, cerebrovascular pressure reactivity index calculated by ICM+ software, L-PRx, NOS, not otherwise specified; NR, not recorded, PbrO2, pressure of brain tissue oxygen; Retro. Ax of prosp, data, retrospective analysis of prospectively collected data
Seven of the studies produced CPPopt data using ICM+ software, which analyzes high-frequency ICP/CPP data to calculate an optimal individualised CPP target, based on the PRx values seen over a range of CPP levels. (
Six studies reported outcome data for mortality at 6 months, 22 –27 five reported GOS at 6 months, 22,24,25,27,28 one reported functional outcome (assessment tool not detailed) at 6 months 26 and one reported PbrO2. 29
All studies were funded by nongovernmental sources. Five studies were coauthored by the creators of ICM+ software, who have a financial interest in a part of the licensing fee. 22,24,25,27,28
Risk of bias
Given the inherent paucity of data presented in abstract-only publications, these were considered have an unclear risk of bias. 24,26 Broadly, the remaining studies were judged as having high risk of bias (Table 2) . The main source of bias arose because of a failure to account for confounding factors in the analysis, such as intercurrent sepsis and severity of injury. 22,25,27,28 One study performed multivariate analysis, thus addressing this to some degree, 23 and one described physiological data only; therefore, these were deemed at low risk. 29 All data gathered were observational, and, therefore, were only able to describe associations rather than apportion causality.
U, unclear.
Mortality
All six studies assessing mortality reported an increased risk with variance from CPPopt, particularly when managed below CPPopt. 22 –27 This was displayed in differing ways across the studies: Aries and coworkers (Cambridge cohort) 22 and Colton and coworkers 26 (Table 3) described reduced mortality rates in those managed within 5 mm Hg of CPPopt (RR 0.28, p = 0.01522 and RR 0.42, p = not recorded [NR] 26 ); Lang and Smielewski (Cambridge Cohort) and Steiner reported a decrease in mortality in those managed above CPPopt (no effect size stated, p < 0.01; 24,25 RR 0.17, p = NR 27 ); and Depreitere showed that survivors spent longer within 5 mm Hg of CPPopt than nonsurvivors (25.6% vs. 19.6% p = 0.01). 23 The difference between actual CPP and CPPopt was an independent predictor of survival when using the Corticoid Randomisation After Significant Head injury (CRASH) outcome prediction model variables of age, Glasgow Coma Scale, pupil reactivity, and presence of extracranial injury as covariates for a multivariate logistic regression (p = 0.017). 23 Lang also reported that 72% of nonsurvivors were managed with CPP < CPPopt (p = NR). 25
CPP, cerebral perfusion pressure; CPPopt, optimal cerebral perfusion pressure; ΔCPP-CPPopt, difference between actual CPP and CPPopt; GOS, Glasgow Outcome Sale; NOS, not otherwise specified, PbrO2, partial pressure of brain tissue oxygen; RR, relative risk.
According to the GRADE criteria however, the quality of this evidence was judged as very low (downgraded for a failure to address potential confounding factors across most studies, and a lack of comparison to standard management); therefore, our confidence in the effect estimate is limited, and firm conclusions on the effect of CPPopt on mortality cannot be drawn.
Neurological outcome
All six studies assessing neurological outcome identified worsening in neurological outcome with variance from CPPopt, particularly when managed above CPPopt (Table 3). 22,24 –28 It should be noted that the commonly used definition of “poor outcome” (GOS 1–3) incorporates death, and, therefore, some of the following results composite disability and death.
In Aries and coworkers (Cambridge cohort), a good outcome (GOS 4–5) at 6 months was more frequent in those with median CPP within 5 mm Hg of CPPopt; (RR 1.65, p ≤ 0.001). Severe disability (GOS 3) was particularly likely in patients with median CPP >5 mm Hg above CPPopt (RR 1.88, p ≤ 0.001). 22 This pattern was reflected in the study by Colton and coworkers, in which risk of poor neurological outcome was higher in those with median CPP >10 mm Hg away from CPPopt (RR 2.14, p = NR). 26 As the neurological outcome scale used is not specified, the findings cannot be directly compared with those of Aries and coworkers. 22
Lang and Smielewski (Cambridge cohort) found that CPP above CPPopt was associated with increased disability in their data set, but did not publish the effect size (p = 0.005, 25 p ≤ 0.02527). Conversely, Dias and coworkers found that patients with poor outcome (GOS ≤3) were managed with CPP lower than CPPopt (−6.6 mm Hg vs. −1.0 mm Hg, p = 0.004). 28 Note here the inclusion of GOS 1 (dead); the authors did not specify the proportion in the poor outcome group who died.
Lastly, Steiner and coworkers reported that the correlation between the difference of mean CPP and CPPopt (meanCPP-CPPopt) with GOS was highly significant (r = −0.51, p < 0.001), showing that the further from CPPopt a patient was managed, the worse the outcome. This correlation existed for those patients managed below CPPopt (r = 0.53, p < 0.001) and for those managed above CPPopt (r = −0.40, p ≤ 0.05). 27 Again it should be noted that GOS of 1 was included here, and that the overall picture was of increased mortality below CPPopt, and increased disability above it.
The pattern described in these studies suggests that the CPPopt is the point at which CPP is high enough to maximize likelihood of survival, while minimizing the detrimental effects of cerebral hyperaemia.
We judged the quality of this evidence to be very low (downgraded again for a failure to address potential confounding factors across most studies, and a lack of comparison to standard management), and, therefore, firm conclusions cannot be drawn.
Physiological outcomes
One study assessed the relationship between CPPopt and a physiological outcome. Jaeger and coworkers found a significant correlation between CPPopt and the PbrO2 change point (CPPPbrO2), the level at which PbrO2 no longer rises in a pressure-passive manner alongside CPP (r = 0.79, p < 0.001). Up to and including CPPopt, the CPP and PbrO2 correlated (r = 0.51, p < 0.001), whereas no such correlation existed above CPPopt (r = 0.03, p = 0.67), displaying that brain oxygenation improved up to the point of CPPopt, but no further (Table 3). 29
Once more the quality of this evidence was rated as very low (downgraded as the physiological changes represent only a surrogate for clinical outcome, and sample size was very small); therefore, firm conclusions cannot be drawn.
Discussion
We found eight studies, based on six distinct data sets, assessing the effect of optimizing CPP targets to PRx. Six of these addressed mortality risk, 22 –27 six addressed disability 22,24 –28 and one addressed PbrO2. 27 Six studies were retrospective observational trials, 22 –27 whereas the remaining two were undertaken prospectively. 28,29
All studies that assessed neurological outcome suggested an association between proximity of actual CPP to CPPopt and improved outcome. 22 –28 One center reported a pattern of increased mortality when actual CPP was lower than CPPopt, and increased disability when actual CPP was above CPPopt. 22,24,25,27 One study displayed an association between CPPopt and the point at which increases in CPP cease to improve brain tissue oxygenation. 29
However, because of the very low quality of the evidence (predominantly through a failure to address the impact of confounding factors that might associate variance from CPPopt and the measured outcomes; e.g., shock, and a lack of comparison to standard practice), the results must be interpreted with caution. The nature of very low-quality evidence is such that future, robust experimental studies may strengthen but, equally, may contradict these findings. As such, we are unable to draw any firm conclusions about the effect of optimizing CPP targets to PRx on any outcomes.
Additionally, targeting PbrO2 thresholds have not been unequivocally shown to improve clinical outcomes, and, therefore, extrapolating the association between CPPopt and CPPPbrO2 to infer a clinically significant effect is as yet unjustified. The other outcomes measures investigated, however, were well validated and clinically relevant.
Overall, there is an absence of prospective, controlled trials addressing the utility of targeting CPPopt. In this review, all studies were observational, and described associations based on variance from CPPopt, rather than comparing a CPPopt-based strategy to usual practice. They could, therefore, only hope to demonstrate association rather than causality; confounding factors, such as shock, could well create such an association between poor outcome and variance from CPPopt, and were not sufficiently accounted for. However, the risk that this confound was a major cause of the observed association with outcome is mitigated by the finding of poorer outcomes when CPP was greater than CPPopt.
To the best of our knowledge, this is the first systematic review published on this topic. Most evidence up to this point has addressed the effect of targeting universal CPP thresholds for all patients. The most frequently utilized practice guidelines amalgamating this evidence are those published by the Brain Trauma Foundation, 30 which recognizes the limited evidence available, and suggests a CPP range between 50 and 70 mm Hg, to balance between the risks of cerebral ischemia and the cardiorespiratory complications of induced hypertension. The idea that CPP thresholds may vary between individuals is mentioned, but there is no suggestion as to how this might be applied to clinical practice.
The strengths of this review are that we followed best practice in systematic review methods, 14 including a rigorous search of published and unpublished material, and two authors extracted and appraised the data. One notable source of potential bias in the review process is that the majority of the studies were published by the Cambridge group who devised, and have a financial interest in, the ICM+ software. Those studies that were performed entirely independently of any members of the Cambridge cohort, 23,26,29 and those using alternative techniques 23,26 reported similar results to those of the Cambridge group, which is encouraging against bias; however, this potential conflict of interest should be borne in mind by the readership. Additionally, the inclusion of the authors of the Cambridge cohort studies in our review team might introduce bias, although they were not involved in the risk of bias, data synthesis, or GRADE ratings of this review.
The published data suggest a positive association between proximity of CPP to CPPopt and clinical outcome, although the poor quality of the evidence prevents firm conclusions from being drawn. Evolving methods are allowing for CPPopt recommendations to be made by applying relatively simple software to data that are routinely gathered, providing the potential for a very cost-effective intervention to be used by even small centers (one could foresee online access for occasional users). An increasing number of neurocritical care units are adopting the technology, and current data lend some support toward its use.
There is not currently enough high-quality evidence to make recommendations for implementing a CPPopt-based strategy over the usual CPP targets suggested by the Brain Trauma Foundation. To truly identify the impact of a CPPopt-based strategy, well designed prospective RCTs comparing the standard CPP recommendations to CPPopt targeting must be undertaken. These should address clinically meaningful outcomes such as mortality, GOS, and neuropsychological measures, and should include rigorous reporting of confounding factors such as baseline severity, additional injuries, and complications during admission. Recommendations for improving the quality of TBI trials have been published as part of the International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT) Project. 31
Footnotes
Acknowledgment
This work was performed in the context of CENTER-TBI (Comparative European Neurotrauma Effectiveness Research in Traumatic Brain Injury), supported by the Framework 7 program of the European Union (Grant number: 602150-2). David Menon is supported by a Senior Investigator Award from the National Institute for Health Research (UK).
Author Disclosure Statement
The software for brain monitoring ICM+ (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.