
Abstract
Incomplete spinal cord injuries (iSCI) leave spared synaptic pathways below the level of injury. Intermittent hypoxia (IH) elicits plasticity in the spinal cord and strengthens spared synaptic pathways, expressed as respiratory and somatic functional recovery in experimental animals and humans with iSCI. This study is a randomized, triple-blind, two-arm parallel clinical trial performed in Santiago, Chile. We compared the effects of a 4-week protocol of IH combined with body weight-supported treadmill training (BWSTT), with continuous normoxia (Nx) and BWSTT on 10-meter walk test (10MWT), 6-minute walk test (6MWT), and timed up and go (TUG) test in American Spinal Injury Association C and D individuals with iSCI. Subjects received daily IH (cycling 9%/21% O2 every 1.5 min, 15 cycles/day) or continuous Nx (21% O2) combined with 45 min BWSTT for 5 consecutive days, followed by IH/Nx 3 × per week (3 × wIH/Nx) for 3 additional weeks. Subjects were assessed at day 5, weekly from weeks 2–4, and at a 2-week follow-up. Daily IH plus BWSTT enhanced walking speed, expressed as decreased 10MWT time at day 5 versus baseline (IH: −10.2 ± 3.0 vs. Nx: −1.7 ± 1.7 sec, p = 0.006), and walking endurance expressed as increased 6MWT distance at day 5 versus baseline (IH: 43.0 ± 10.7 vs. Nx: 6.1 ± 3.4 m, p = 0.012), but not TUG time. Further, 3 × wIH maintained the daily IH-induced walking speed, and enhanced the daily IH-induced walking endurance, which is maintained up to the 2-week follow-up. We conclude that daily IH enhances walking recovery in subjects with iSCI, confirming previous findings. Moreover, 3 × wIH prolonged or enhanced daily IH-induced walking speed and endurance improvements, respectively, up to 5 weeks post-daily IH. Repetitive IH may be a safe and effective therapeutic alternative for persons with iSCI.
Introduction
M
Intermittent hypoxia (IH)-induced neuroplasticity has been extensively studied in phrenic motor nuclei (C3–C5) through phrenic nerve recording preparations. 6 Moderate IH (3, 5-min hypoxic episodes; PaO2 35–45 mm Hg; 5-min intervals) elicits phrenic long-term facilitation (pLTF), a prolonged increase in phrenic nerve activity after exposure to IH. 7 IH elicits activation of raphe serotonergic neurons that project to phrenic motor nuclei. Intermittent spinal serotonin release subsequently activates serotonin type 2 (5-HT2) receptors coupled to Gq protein on or near phrenic motor neurons, and initiates intracellular cascades that underlie pLTF. 7 Downstream signaling events include new synthesis of brain-derived neurotrophic factor (BDNF) 8 and activation of its high-affinity receptor tyrosine kinase (TrkB) 8 followed by extracellular signal-regulated kinase (ERK) mitogen-activated protein (MAP) kinase signaling. 9
Experimental studies in rats have demonstrated that repetitive IH is a possible therapeutic approach to restore breathing capacity 10,11 and forelimb function after cervical (C2) spinal hemisections (C2HS). 11 For instance, daily IH (cycling 10.5%/21% O2 every 5 min, 10 cycles/day, 7 days) elicited nearly complete and prolonged (>3 weeks) recovery of forelimb function in the horizontal ladder-walking task in rats with C2HS. This functional improvement was accompanied by increased BDNF and TrkB levels within cervical (C7) motor nuclei innervating the forelimb. 11
In humans with iSCI, exposure to relatively brief sessions of IH has been shown to improve motor function. A randomized crossover study demonstrated that a brief and moderate protocol of IH (cycling 9%/21% O2 every 1 min, 15 cycles/day, 1 day) increased maximal plantar flexion torque by 82% in chronic ASIA D subjects with iSCI. 12 The increased plantar torque was positively correlated with the peak gastrocnemius electromyogram activity and was sustained for more than 90 min. 12 Using a similar protocol of IH, Hayes and associates 13 reported that 5 days of IH plus 30 min of overground walking practice improved walking speed and endurance in persons with chronic iSCI. The effect of longer IH protocols (>5 days) has not been explored.
Experiments in rats suggest that the capacity of IH to induce functional recovery after a spinal injury is highly dependent on time post-injury. 14 –16 For example, IH-induced diaphragm long-term facilitation (diaLTF) was abolished at 2 weeks but was restored at 8 weeks post-C2HS. 16 Similarly, IH (3 episodes 5 min 11% O2 interspersed with 5 min normoxia [Nx]) induced pLTF at 8 weeks but not at 2 weeks post-C2HS. 15 This increasing ability with time post-injury correlated with spontaneous restoration of serotonergic input to the phrenic motor nucleus below the injury. 15 Although it is unclear when serotonergic connections/terminals are restored after SCI in humans, based on animal studies, we speculate that IH may be most effective therapeutically in subjects with chronic iSCI.
Combinatorial therapies, one being an activity-based training, can augment plasticity after iSCI. 17 –20 In a randomized, double-blind, crossover design study, the effect of daily IH (cycling 9%/21% O2, every 1.5 min, 15 cycles/day, 5 days) alone or combined with overground walking practice (30 min/day at maximal exertion) was studied in 19 persons with chronic iSCI. 13 Daily IH alone (n = 9) increased walking speed by 18% 3 days after exposure; whereas daily IH combined with overground walking (n = 10) improved walking endurance. 13
It is not known whether the same effect can be achieved combining IH with a different modality of locomotor training such as body weight-supported treadmill training (BWSTT). A study demonstrated that in persons with chronic iSCI, both overground walking and BWSTT improved walking speed, measured with the 10-meter (10-m) walk test. 21 At a cellular level, both locomotor training and IH increase the expression of BDNF, 8,22,23 a known neurotrophic factor involved in neural protection and plasticity. 24 We propose that BWSTT may serve as a catalyst in tandem with repetitive IH, and when combined, develop a greater walking functional recovery.
The purpose of this study was to compare the effect of a 4-week protocol of IH combined with BWSTT (experimental group) versus continuous Nx with BWSTT (control group) on the 10-m walk test (10MWT), 6-min walk test (6MWT), and timed up and go (TUG) test in chronic ASIA C and D subjects with iSCI. We hypothesized that 5 days of IH (daily IH) and BWSTT elicits a greater walking function than Nx and BWSTT, and that exposure to IH three times per week and BWSTT for 3 additional weeks can maintain the beneficial effect of daily IH.
Methods
Study design
This was a randomized, triple-blind, placebo-controlled, two-arm parallel clinical trial conducted in two sites, including subjects recruited from Instituto Teletón Santiago, Hospital Clínico Mutual de Seguridad, Clínica Los Coihues, and Hospital del Trabajador, in Santiago, Chile. The research sites selected to execute locomotor training were Teletón Institute and Hospital Clínico Mutual de Seguridad, based on the availability of a body weight-supported treadmill system.
The study was conducted in accordance with the Declaration of Helsinki; it was approved by the Institutional Review Boards of participating centers and was registered at ClinicalTrials.gov (NCT02441179). All subjects provided written informed consent before study enrollment.
The overall study and statistical analysis were reported according to Consolidated Standards of reporting Trials 2010 guidelines 25 and Statistical Analyses and Methods in the Published Literature Guidelines, 26 respectively.
Subjects
Men and women with iSCI were eligible for enrollment according to the following inclusion criteria: (1) subjects ≥18 years of age; (2) neurological level C5–T12, classified as ASIA grades C and D; (3) traumatic and nontraumatic, nonprogressive lesions; (4) onset >6 months; (5) ability to ambulate with or without assistive devices; (6) ability to follow verbal or visual commands; and (7) signed informed consent. Exclusion criteria included: (1) unstable orthopedic injuries, (2) osteoporosis with high risk of pathological fracture, (3) cutaneous lesions and/or pressure ulcers, (4) joint contractures, (5) cardiopulmonary conditions, and (6) body weight exceeding 150 kg.
Eligibility of subjects was determined by a rehabilitation physician following inclusion/exclusion criteria. We collected general health and sociodemographic information; none of the subjects reported having a diagnosed cardiopulmonary disease or obstructive sleep apnea. An external independent statistician used a blocked randomization design to assure a balanced distribution of ASIA (C and D), as well as age (≥35 years vs. <35 years) in both groups. The allocation list for the two comparison groups was formed by means of computer-based random numbers in Excel software.
Intervention
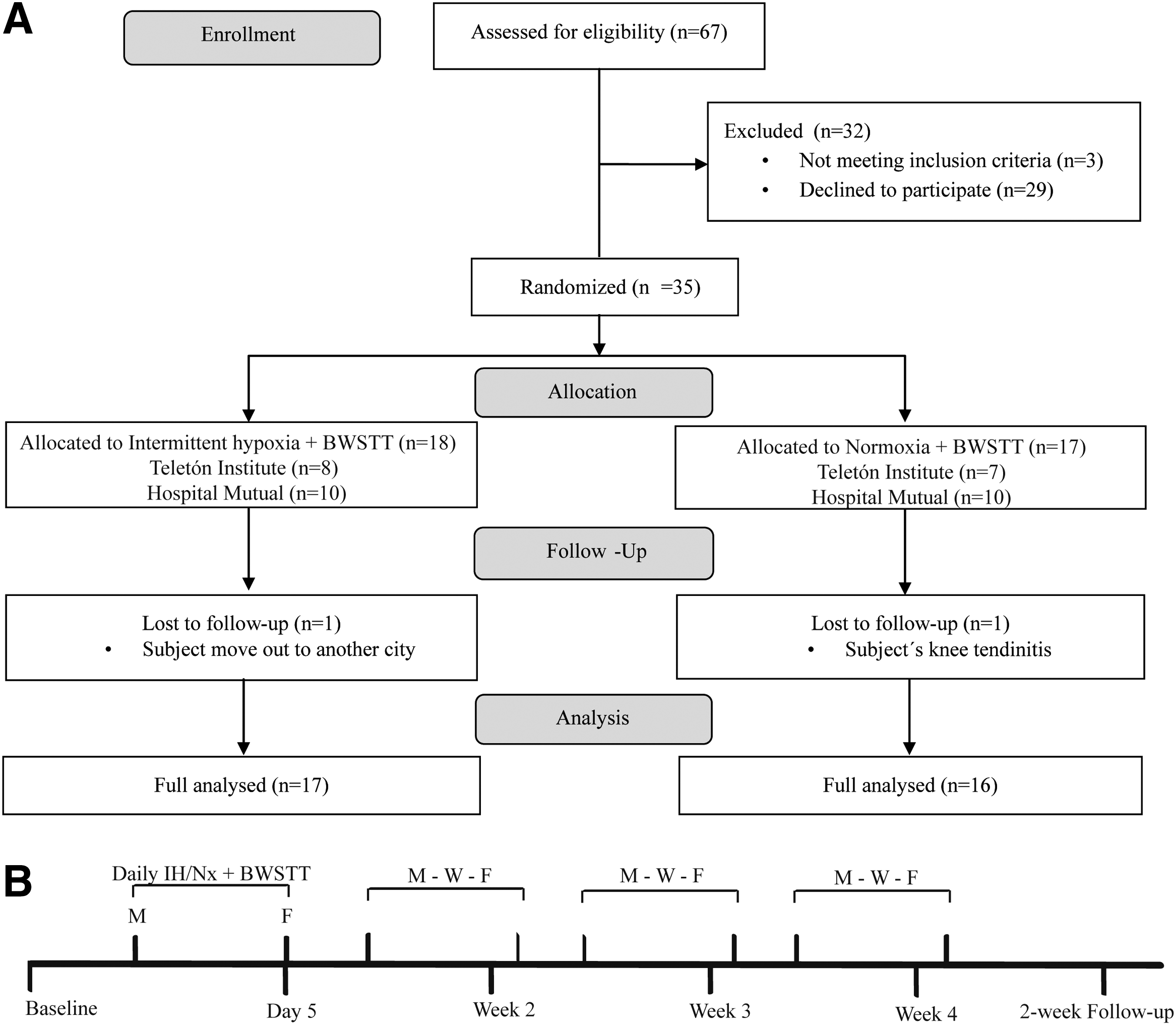
For a two-arm parallel clinical trial, two groups received either the experimental intervention or the control. The experimental group (n = 18) received IH plus BWSTT, and the control group (n = 17) received continuous Nx, (placebo) plus BWSTT (Fig. 1A).
(
The physician administrating the IH/Nx protocol received the group assignments in sealed envelopes. Subjects, physical therapists (assessors), and the statistician were blind to group assignment, constituting a triple-blind study. Intervention allocation was recorded in a password-protected document.
IH/Nx gas delivery
The desirable gas concentration for IH (9% O2) or Nx (21% O2) was provided by pre-calibrated and certified gas cylinders (Indura S.A, Chile). The time of the intervals was automatically controlled by a programmable compact smart relay (Zelio Logic SR2B121BD, Telemecanique, Schneider Electric, France) controlling two solenoid valves (Model 2026BV172T, Jefferson Solenoid Valves, USA).
The inlet of one valve was connected to a gas cylinder (6 m3) containing compressed air; the other valve inlet was connected to a different cylinder (6 m3) filled with a certified gas mixture (Indura S.A., Chile) of 9% O2 in N2. The outlets of the valves were connected together to a single output line, the flow from which was controlled by a flowmeter (2–20 L/min) to maintain a steady flow of 8 L/min. The output line was connected to a humidifier (Hudson RCI® 3230, Teleflex Inc., USA) and then to an oro-nasal mask through one arm of a Y-tube connector. The other arm was connected to a reservoir containing 50 mL of water to exhaust exhaled CO2.
The total duration of the experiment, as well as the duration of each gas exposure in the cycle, was programmed into the smart relay using Zelio Soft 2 (4.5, Schneider Electric, France). The relay and the valves were supplied with a 24 VDC power supply (UNO-2902994, Phoenix Contact, Germany) that was connected to an uninterruptible power supply (OMNIVSINT800, Tripp Lite®, USA). The oxygen content in the output line was measured using an oxygen analyzer (AX300, Teledyne Analytical Instruments, USA) and the blood oxygen saturation with a pulse oximeter to assure that the saturation did not drop below 80% during the hypoxic episodes.
IH protocol
This consists of 90 sec of 9% O2 interspersed with 90 sec of 21% O2, 15 times a day, for 5 consecutive days (daily IH), followed by IH three times per week for 3 additional weeks. Total time was 4 weeks. The oxygen concentration used in this protocol (9% O2) was based on previous experimental animal 10 and human studies. 12,13 The extended timeline (IH three times per week, for 3 additional weeks) was based on a recent study performed in rats with chronic C2HS. 27 Chronic C2HS rats were exposed to a moderate dose of IH (cycling 10.5%/21% O2, every 1.5 min, 10 times a day) for 5 consecutive days (daily IH), followed by IH three times per week for 3 additional weeks.
Daily IH elicited a greater bilateral diaphragm motor (EMG) recovery than control rats exposed to Nx. Further, presentations of IH three times per week maintained the effect of daily IH for 3 additional weeks. 27 Based on these findings, we hypothesized that exposure to IH three times per week may be capable of maintaining the potential walking beneficial effects elicited by daily IH in persons with iSCI.
Placebo protocol
This consisted of continuous Nx n (21% O2) for 45 min for 5 consecutive days followed by three times per week for 3 weeks. Total time was 4 weeks.
BWSTT
Following the IH/Nx protocol, all subjects received BWSTT. Exercise was performed on a custom-built motorized treadmill (Techogym, model Jog Now 500, Italy) and body weight suspension system (Medlinne, model: SA-M274, Chile). Subjects started training with approximately 30% body weight support and a treadmill speed of 0.6 km/h. Manual facilitation was used to assist stepping motion and encourage an upright trunk during walking. Subjects were encouraged to walk at the fastest speed and with the lowest body weight support they could comfortably tolerate.
In summary, two groups of subjects received either IH or Nx (placebo) protocol (45 min), followed by BWSTT (45 min) for a total of 90 min per day for 5 consecutive days followed by IH and BWSTT three times per week for 3 additional weeks. Total time was 4 weeks (Fig.1B).
Primary outcome
10MWT
The 10MWT measures the time (in sec) that it takes a subject to walk 10 m. This scale is validated for subjects with iSCI. 28 It has an excellent test-retest reliability (r = 0.983), 29 as well as intra-rater and inter-rater reliability (r: 0.98 and 0.974, respectively). 30,31 The evaluator asked subjects to walk 10 m as quickly, but safely, as possible. Participants used their regular assistive devices to walk independently.
Secondary outcomes
6MWT
The 6MWT measures the distance (in meters) a subject is able to walk over a 6-min period. 32 This scale is validated for subjects with iSCI 28 with an excellent inter-rater reliability (r: 0.97). 30,32 The length of the corridor was marked every 10 m and turnaround points were marked by a cone. The evaluator asked subjects to walk as far as possible in 6 min. Subjects rested as needed, but they were instructed not to sit.
TUG
The TUG test measures the time (in sec) it takes the subject to stand up from a seated position in a chair, walk 3 m at a comfortable and safe pace, turn, walk back to the chair, and sit down. It is validated in ASIA grades D 33 and has excellent intra-rater (r = 0.979) and inter-rater (r = 0.973) reliability. 30 There is an excellent correlation between TUG and 10MWT (r = 0.89) and between TUG and 6MWT (r = −0.88). 30 Participants were allowed to use assistive devices to walk independently, if needed.
Visual analog scale (VAS)
To assess the influence of the interventions on general pain intensity, participants were asked to rate their current pain immediately before and after the 4-week protocol of IH/Nx plus BWSTT using the VAS scale, 34 ranging from no pain (score 0) to unbearable pain (score 10).
Ashworth Scale (AS)
To assess whether the interventions had a negative effect on the degree of spasticity, participants were evaluated before and after the 4-week protocol of IH/Nx plus BWSTT using the AS 35 ranging from 0 (no increase in muscle tone) to 4 (limb rigid in flexion or extension).
The 10MWT, 6MWT, and TUG measures were assessed before IH/Nx + BWSTT (baseline), after 5 days of daily IH (day 5), weekly from week 2 to 4, and 2 weeks after the completion of the study (2-week follow-up). The AS and VAS measures were assessed before (baseline) and at the end of the 4-week protocol.
Statistical analysis
Sample size
The smallest real minimally clinically important difference (MCID) detected by the 10MWT in subjects with iSCI corresponds to 0.14 m/sec. 29 Considering that the target population included subjects with chronic iSCI, and that the mean change between 3 and 6 months post-injury corresponds to 0.47 m/sec, 29 a 0.4 m/sec was proposed as a clinically significant change, however. Using the DuPont and Plummer test for paired and independent samples, 36 32 subjects (16 subjects per group) were calculated for a two-arm parallel clinical trial with a 0.05 alpha error and 80% power.
Normality and variance
Data from all the outcome measures were not normally distributed (Shapiro-Wilk, p < 0.05). There was equality of variances for groups 1 and 2 (Levene test, p > 0.05).
Outcomes
We used the nonparametric Friedman test with post-hoc Wilcoxon-rank comparisons to examine the effects of repetitive IH combined with BWTSS on walking speed (10WMT), endurance (6WMT), and TUG test among baseline, day 5, weeks 2–4, and a 2-week follow-up. The Kruskal-Wallis test was used to establish between-group comparisons (IH + BWSTT vs. Nx + BWSTT) at all time points.
SPSS Statistics (IBM Inc., Armonk, NY, version 20.0) was used for statistical analyses. Results were reported as mean differences (relative to baseline) ± standard error. Age was reported as mean ± standard deviation. Statistical differences were considered at p < 0.05.
Results
Subject's eligibility
The research databases of Hospital Mutual de Seguridad, Instituto Teletón, Clínica los Coihues, and Hospital del Trabajador were screened for possible candidates. In total, 67 entries were found to approximately match inclusion and exclusion criteria. These subjects were contacted and invited for screening on site. Of 67 subjects contacted, only 38 accepted the invitation. The reasons reported by the subjects for declining to participate in the study included: (1) lack of employer's permission, (2) a tight work schedule, (3) lack of transportation, (4) lack of family support, and (4) lack of interest in the therapy. Of 38 subjects, 3 could not be included because they had brain trauma history and unknown cognitive deficits.
Thus, 35 subjects were enrolled and randomly assigned to group 1 (IH plus BWSTT, n = 18) or group 2 (Nx plus BWSTT, n = 17). Of 35 subjects, 33 completed the entire protocol and all the assessments. One subject from the IH + BWSTT group dropped out during the trial to move to another city, and another subject from the control group dropped out of the trial because of a chronic knee tendinitis that prevented him from continuing with the training (Fig. 1A).
Characteristic of subjects
Characteristics of the participants are displayed in Table 1. Most of the subjects were male (n = 31). The mean age was 41 (17) and 42 (17) years for groups 1 and 2, respectively. There was a balanced distribution of ASIA C and D subjects in group 1 (6 ASIA C, 12 ASIA D) and group 2 (7 ASIA C, 10 ASIA D). Most subjects were more than 2 years post-injury (n = 25). The shortest time post-injury was 13 months, and the longest was 13 years.
ASIA, American Spinal Cord Injury Association Impairment Scale; SD, standard deviation.
Intervention: Group 1, intermittent hypoxia plus body weight-supported treadmill training (BWSTT). Group 2, normoxia (placebo) plus BWSTT.
Participants were asked to maintain their regular medication scheme and to inform the team of any discomfort or change they may experience. Participants were allowed to wear their regular ankle-foot orthosis during all training sessions and their usual walking devices during the walking assessments. None of the subjects were receiving physical therapy or any other therapy at the beginning of the protocol, and they were advised not to perform additional training at home during the execution of the study. We incorporated subjects’ family members early on the study, who served as facilitators to assure good attendance at the sessions and to prevent additional training of participants at home.
Safety
The IH/Nx exposure and training program were well tolerated by all subjects. We monitored for incidence of headaches, nausea/vomiting, lightheadedness, respiratory distress, cyanosis, and autonomic dysreflexia before and after exposure to IH/Nx and locomotor training. No incidents or unwanted side effects were reported by the subjects.
The AS and the VAS were assessed before and after the 4-week IH/Nx plus BWSTT protocol (Table 2) to determine whether the interventions had a negative effect in the degree of spasticity or pain perception of the participants. The percentage of participants showing a greater AS score (i.e., greater spasticity) at the end of the 4-week protocol was not significantly different between groups (Pearson chi-square test, p = 0.57). Similarly, there was no significant difference in pain perception between groups (Pearson chi-square test, p = 0.14).
IH, intermittent hypoxia; BWSTT, body weight-supported treadmill training; Nx = normoxia.
There were no significant differences in spasticity or pain perception between groups after a 4-week protocol.
Arterial oxygen saturation (%) was monitored continuously with a pulse oximeter attached to a fingertip, with the monitor shielded from participants. The oxygen concentration during the hypoxic episodes was tightly controlled by certification of the gas mixture (Indura S.A.), which ranged from 8.8–9.2% O2. In addition, a gas analyzer located in the output line was used to register the O2 delivered to the subjects, which ranged from 8.7–9.4% during the hypoxic exposures. The pulse oxygen saturation dropped to 80–83% during the hypoxia episodes and remained unchanged in the normoxic group.
Repetitive IH combined with BWSTT enhanced walking speed
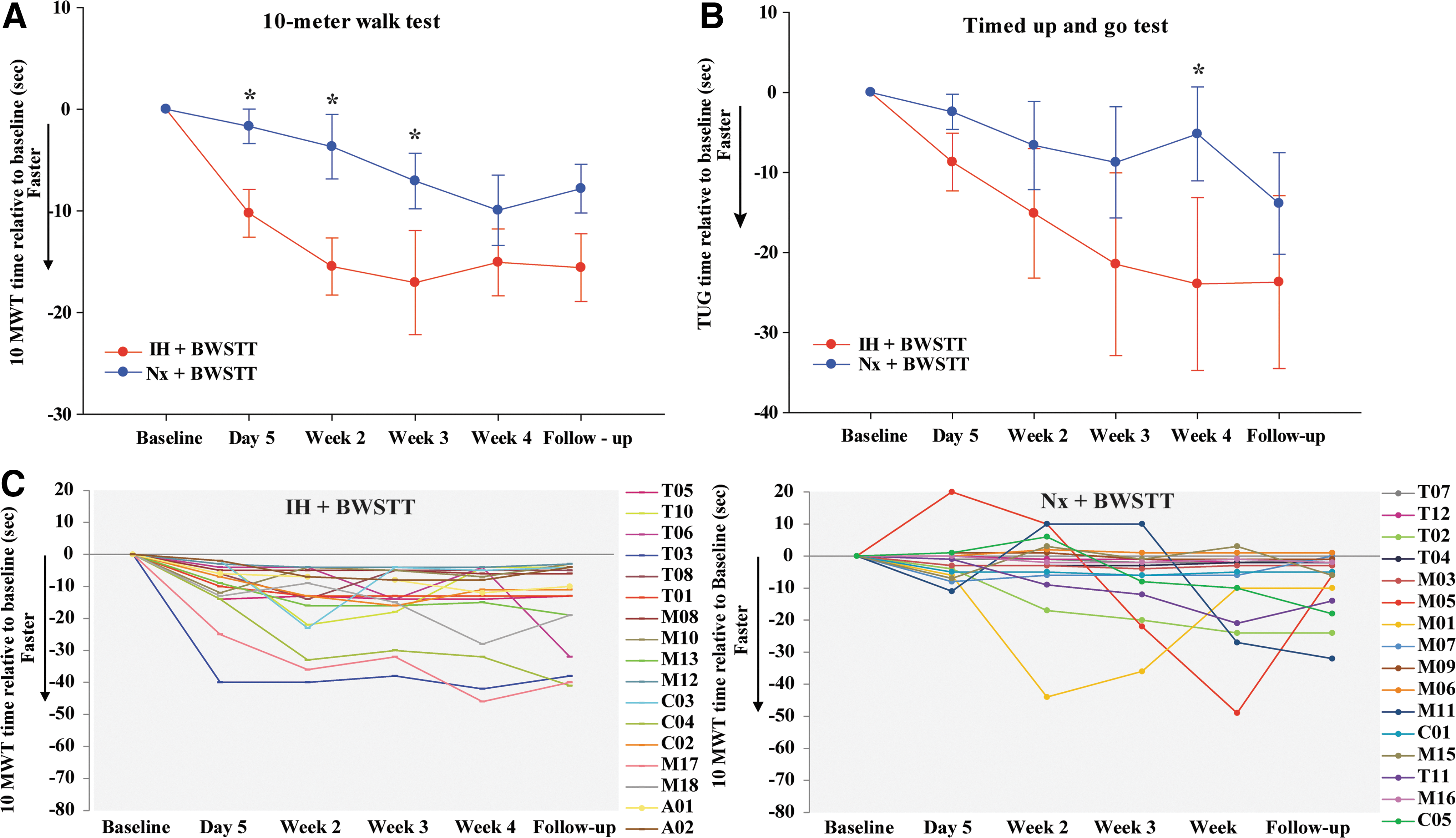
The 10MWT was assessed before IH/Nx plus BWSTT (baseline), 5 days after daily IH (day 5), weekly (weeks 2–4), and 2 weeks after the completion of the study (follow-up) (Fig. 2A, C). There were no significant differences in baseline mean (Student t test, p = 0.46) and variance (Levene test, p = 0.08) of walking speed between groups.
Changes in 10-Meter Walk Test (10MWT) time (
Between-group comparisons showed that the IH group had a greater walking speed than the control group, expressed as a decrease in 10MWT time versus baseline at 5 days after the interventions (IH: −10.2 ± 3.0 vs. Nx: −1.8 ± 1.7 sec, p = 0.006, Fig. 2A). This trend was maintained at week 2 (IH: −15.5 ± 4.8 vs. Nx: −3.7 ± 3.3 sec, p = 0.04) and week 3 (IH: −17.1 ± 5.3 vs. Nx: −7.1 ± 2.8 sec, p = 0.03) but not at week 4 (p = 0.54) (Fig.2A). A 2-week follow-up showed that both IH and Nx groups maintained a walking speed significantly faster than baseline (p < 0.05), and differences between groups approached statistical significance (p = 0.06, Fig.2A).
Within-group comparisons showed that overall, the IH group had a significant decrease in 10MWT time from day 5 to week 2 (−10.2 ± 3.0 vs. −15.5 ± 4.8 sec, p = 0.03; Fig.2A), which was maintained up to the 2-week follow-up (-15.5 ± 4.8 vs. −20.3 ± 6.9 s, p = 0.09). Thus, exposure to IH three times per week combined with BWSTT extends the walking speed gains elicited by 5 days of IH.
Repetitive IH combined with BWSTT does not enhance TUG test
The TUG test, expressed as a decrease in TUG time versus baseline, was assessed at baseline, 5 days after daily IH (day 5), weekly (weeks 2–4), and 2 weeks after the completion of the study (follow-up) (Fig. 2B). There were no significant differences in baseline mean (Student t test, p = 0.68) and variance (Levene test, p = 0.80) of TUG time between groups.
Between-group comparisons showed that although there was a greater decrease in TUG time in the IH group, it was not statistically different from that of the control group at day 5 (IH: −8.7 ± 3.7 vs. Nx: −2.4 ± 2.3 sec, p = 0.16), week 2 (−15.2 ± 8.3 vs. −6.6 ± 5.7 sec, p = 0.32) and week 3 (−22.8 ± 11.5 vs. −8.75 ± 7.2 sec, p = 0.07). A statistically significant difference between groups was found at week 4 (−23.9 ± 11.1 vs. −5.2 ± 6.1 sec, p = 0.03, Fig. 2B), but it was not maintained at the 2-week follow-up (−23.7 ± 11.1 vs. −13.8 ± 6.6 sec, p = 0.07).
Within-group comparisons showed that exposure to IH three times per week combined with BWSTT elicits a progressive decrease in TUG time from day 5 to week 4 (Fig. 2B), which was statistically significant between weeks 2 and 3 (−15.5 ± 8.3 vs. −22.8 ± 11.5 sec, p = 0.002, Fig. 2B). The decrease in TUG time was maintained up to the 2-week follow-up (−22.8 ± 11.5 vs. −23.7 ± 11.1 sec, p = 0.59).
Repetitive IH combined with BWSTT enhanced walking endurance
The 6MWT, expressed as an increase in distance (m) compared with the baseline, was assessed 5 days after daily IH (day 5), weekly (weeks 2–4), and 2 weeks after the completion of the study (follow-up) (Fig. 3). There were no significant differences in baseline mean (Student t test, p = 0.32) and variance (Levene test, p = 0.81) of walking endurance between groups.

(
Between-group comparisons showed that there was a greater walking endurance in the IH group compared with the control group at day 5 (IH: 43.1 ± 10.7 vs. Nx: 6.1 ± 3.4 m, p = 0.012, Fig. 3A,C) and at later time points (Fig. 3A). The greatest difference between groups was observed at week 4 (IH: 70.5 ± 13.2 vs. Nx: 22.4 ± 10.6 m, p = 0.005).
Within-group comparisons showed that the IH group had a progressive increase in walking distance from day 5 to week 4 (43.1 ± 10.7 vs. 70.5 ± 13.2 m, p = 0.007, 3A), meaning that exposure to IH three times per week enhanced walking endurance elicited by daily IH and BWSTT for 3 additional weeks. The repetitive IH-induced greater walking endurance persisted for 2 weeks after the completion of the study (70.5 ± 13.2 vs. 65.7 ± 11.5, p = 0.49).
Repetitive IH enhances walking function in ASIA C/D and young/old subjects
Subgroup analysis demonstrated that IH enhances walking speed, endurance, and up and go time in both ASIA C and D subjects, with no statistical differences between ASIA subgroups at all time points (p > 0.05).
There was a similar effect of IH on walking speed and TUG time in subjects ≤35-years-old vs. >35-years-old (p > 0.05); however, there was a greater 6MWT distance in subjects younger than 35-years-old (Fig. 3B). At week 2, <35-year-old subjects showed a greater walking distance than older subjects (66.8 ± 15.2 vs. 21.7 ± 5.7 m, p = 0.043). This difference was maintained at week 3 but not at later time points (Fig. 3B).
Discussion
This study confirms previous findings of a greater walking function in persons with iSCI after 5 days of IH (daily IH) combined with locomotor training. 13 Specifically, this study showed that daily IH, along with BWSTT, elicited a greater walking speed and endurance, but not up and go time, in ASIA C and D subjects with iSCI. The enhanced walking endurance elicited by daily IH is greater in younger (<35 years), compared with older (≥35 years) persons. Further, exposure to IH three times per week (repetitive IH) and BWSTT maintained the walking speed and increased the walking endurance elicited by daily IH and BWSTT for 3 additional weeks. The beneficial effect of repetitive IH was maintained for at least 2 weeks after the completion of the study.
Repetitive IH and BWSTT enhance walking speed but not up and go time
The selected outcome measures of ambulation (10MWT, 6MWT, and TUG) showed the best test-retest and inter-observer reliability, as well as responsiveness to change, in ambulatory subjects with iSCI. 37 A previous study showed that daily IH and overground walking training elicits a greater walking endurance (measured with the 6MWT), than walking speed (measured with the 10MWT). 13 In this study, however, the 10 MWT was selected as a primary outcome based on the difficulty of estimating a pre-study effect size with the 6MWT. Half of the study participants were ASIA D (fast walkers) and, among fast walkers, the 6MWT does not significantly correspond with a clinically relevant change. Therefore, a reliable MCID could not be determined. 38
Participants reported that they did not perform other physical exercises apart from the interventions during this study, so we can reasonably assume that the changes found here were because of the intervention. We compared walking function of subjects exposed to IH plus BWSTT, versus BWSTT alone, because treadmill-based locomotor treatment has demonstrated to increase walking function in subjects with iSCI 39 and is the standard treatment in our research sites. The present study demonstrated that a protocol of daily IH (cycling 9%/21% O2 for 1.5 min each, 15 cycles/day, for 5 days), combined with BWSTT, improved walking speed and endurance in ASIA C and D persons with iSCI, which is consistent with a previous study. 13
Although it was demonstrated previously that daily IH elicits a greater walking function when combined with overground walking training, 13 here we showed that BWSTT can elicit a similar effect. Subjects receiving Nx (placebo) plus BWSTT improved the 10-m walking speed from 0.53 ± 0.12 m/sec (baseline) to 0.69 ± 0.15 m/sec at day 5 (after 5 days of daily Nx + BWSTT), whereas the IH group increased from 0.54 ± 0.11 m/sec (baseline) to 0.74 ± 0.14 m/sec (after 5 days of daily IH + BWSTT).
According to categories of ambulation, 40 subjects receiving IH and BWSTT should be able to pass from the category “walking with aid” to “walking without aid.” We asked all participants to use their regular walking assistive devices throughout the assessments and, thus, we could not confirm whether subjects receiving IH actually could walk without walking assistive devices at the end of the trial. Participants were contacted 4 weeks after the completion of the trial, however, and 3 of 17 subjects of the IH + BWSTT group reported walking without aids (canes), and 1 of them stopped using his ankle-foot orthosis, which was not reported in the control group. Because gait in subjects with iSCI is influenced by lower-limb paresis, poor coordination, increased spasticity, and impaired balance, 41 we may speculate that although IH and locomotor training improved walking speed and endurance, it had limited effect on other factors influencing the use of walking assistive devices.
The increased walking speed observed in the IH group was significantly greater than the control group at weeks 2 and 3. Although there were no significant differences between groups at week 4 and at the 2-week follow-up, this may be because of type-II error because the difference between groups at the follow-up was close to statistical significance (p = 0.06), and a greater sample size would have led to a greater statistical difference. Within-group comparisons in persons with iSCI receiving IH plus BWSTT show a significant increase in walking speed from day 5 to week 2, suggesting that exposure to IH three times per week (repetitive IH) enhanced the therapeutic effect of 5 days of IH. Further, repetitive IH maintains the beneficial effect of daily IH up to 2 weeks after the completion of the study. The overall duration of the repetitive IH-induced walking speed recovery remains to be investigated.
Based on 10MWT pre-study mean change that we considered statistically significant (0.4 m/sec), five subjects from the IH + BWSTT group and no subject from the control group achieved this goal after 5 consecutive days of IH/Nx plus BWSTT. Thus, the absolute risk-reduction ratio was 0.29 (confidence interval: 0.08–0.51), meaning that the absolute risk of achieving a clinically significant faster walking speed is 29% greater in those subjects receiving IH and BWSTT than in those receiving Nx and BWSTT. Accordingly, the number needed to treat was 4 (2–13), which is in the range of effective treatment. 42
Although construct validity between timed measures of ambulation (10MWT and TUG) is very strong, 30,37 here we observed different results between TUG and 10MWT. Whereas IH plus BWSTT significantly enhanced walking speed with the 10 MWT, it did not translate into a faster TUG speed. We speculate that although both tests assess walking speed, TUG additionally requires adequate dynamic balance to stand up from the chair and later to turn, come back, and sit. In fact, the TUG test has been shown to reflect balance deficits in the elderly 43 and persons with stroke. 44 Considering that BWSTT focuses on training speed and endurance, not balance, the reduced TUG time may be partially explained by the lack of task-specific balance training.
Repetitive IH and BWSTT enhance walking endurance
The greatest difference between groups was observed in walking endurance, measured with the 6MWT. The IH group showed a progressive increase in 6MWT distance from day 5 to week 4, which was maintained up to 2 weeks after the completion of the study. In contrast, the control group showed a mild increase in walking endurance over time, suggesting that 4 weeks of BWSTT alone was not capable of significantly increasing walking endurance, which may be attributed to an insufficient dose of locomotor training.
Studies showing the effectiveness of BWSTT in subjects with iSCI regularly use at least 12 weeks of training. 45,46 Thus, 4 weeks of locomotor training may be insufficient to elicit an increase in walking endurance. Moreover, a previous study in persons with iSCI showed that when daily IH was combined with overground walking, the effect on walking endurance was greater than with IH alone. 13 A study in rats demonstrated that 7 days of IH initiated 4 weeks after cervical iSCI improved foot-slip performance on a ladder-walking task only when combined with daily ladder-task training. 47 These studies suggest that either IH or locomotor training alone (≤4 weeks) is not sufficient to elicit a significant motor recovery; only when both are combined is a greater response achieved.
Mechanisms underlying IH-induced walking recovery
The mechanisms underlying IH-induced walking recovery in persons with iSCI remain to be investigated. IH induces plasticity in spared spinal pathways to respiratory and nonrespiratory motor neurons, 48 improving respiratory and nonrespiratory (forelimb) motor function in rats with chronic cervical injuries. 11,47 Although there is extensive literature explaining the mechanisms underlying respiratory motor plasticity, 49 mechanisms underlying somatic motor recovery in rats and humans are yet to be investigated.
Thus, we cannot establish a direct cause-effect relationship between IH-induced plasticity and an increased walking performance. Assuming that IH elicits the same cascade of events documented in phrenic motor neurons (increased BDNF, TrkB activation, and increased glutamatergic transmission), it is not known yet whether this is a steady phenomenon or IH “prime” motor neurons initially, allowing further motor unit recruitment through additional mechanisms.
Finally, exposure to IH three times per week may enhance IH-induced somatic and respiratory motor recovery. Studies in rats have demonstrated that exposure to repetitive IH (10, 5 min 10.5% O2 interspersed with 5 min Nx, 3 days/week, for 4 weeks) elicits enhanced phrenic LTF, 50,51 increased respiratory and nonrespiratory somatic motor recovery, 11 and increased plasticity (i.e., metaplasticity) after cervical spinal injury. 48 Further studies are needed to determine the cellular mechanisms underlying IH-induced metaplasticity in nonrespiratory somatic motor neurons.
Repetitive IH enhances walking function in ASIA C/D and young/old subjects
The potential for IH to induce functional recovery may be affected by variables such as the completeness of injury, onset of injury, and age of subjects. A previous study demonstrated that combined IH and overground training improved walking speed and endurance in subjects with two ASIA C iSCI. 13 We confirm those findings; all ASIA C subjects receiving IH plus BWSTT (n = 6) showed a greater walking speed and endurance. Subgroup analysis showed that both ASIA C and D subjects benefited from a repetitive protocol of IH. The potential therapeutic effect of repetitive IH in ASIA B subjects with iSCI remains to be investigated.
Animal studies suggest that repetitive IH may be most effective in chronic spinal injury, after serotonergic function has been partially restored below the injury 15 and that the extent of functional recovery correlates with the serotonergic innervation below the injury. 52 We showed that repetitive IH combined with BWSTT enhanced walking speed and endurance in chronic iSCI. In our sample, the shortest time post-injury was 13 months; thus, it is reasonable to assume that at this time, there is a considerable extent of descending serotonergic innervation below the site of injury.
Age affects the expression of IH-induced neuroplasticity. In rats, respiratory LTF, a form of respiratory plasticity, is greater in 1-month-old rats and decreases significantly in 6-month-old male rats. 53 It has been proposed that normal testosterone levels are necessary for the expression of spinal plasticity, because gonadectomy diminishes phrenic and hypoglossal LTF in male rats. 54 Based on the plasma total testosterone (PTT) levels reported by Simon and colleagues, 55 the first major drop in PTT levels in men occurs at the age range of 35–39 years (6.24 ng/mL).
In this study, we did not find significant differences between young (<35 years old) and old (≥35 years old) subjects in walking speed. There was a greater walking endurance in younger (<35 years) subjects receiving IH plus BWSTT, however, which suggests that hormonal and/or other age-related influences may affect IH-induced walking endurance. For instance, in elderly subjects, the training effects of physical activity outweigh the effect of IH on strength-endurance measures. 56
Study limitations
Some points of the study protocol have to be critically discussed as limitations, such as the lack of control over additional locomotor training, a placebo effect, unpowered sample size, genetic variability, and gender bias.
Participants were instructed not to perform additional physical activity during the trial. Subjects showed a favorable attitude toward the protocol, however, and some of them expressed the need for extra training sessions; thus, we cannot assure that subjects fulfilled the protocol instructions.
In our study, no unwanted side effects were reported. Both the exposure to IH/Nx protocols and the physical training were well tolerated. Although a quality-of-life questionnaire was not applied, subjects from both groups expressed beneficial effects such as good mood, physical agility, and a high motivation to complete the protocol, preventing us from ruling out a placebo effect.
Sample sizes involving chronic SCI subjects are usually small. 57 In this study, the dropout rate was low (8.5%), and 33 subjects completed all of the sessions of the protocol. According to our pre-study power analysis, 32 subjects (16 subjects per group) was the goal for a two-arm parallel clinical trial with a 0.05 alpha error and 80% power; thus, statistical power was achieved. Larger sample sizes, however, would have led to a greater statistical power and further analysis by injury level and gender.
Generalization of our results is limited to ASIA C and D Chilean subjects with iSCI. An important aspect in human studies is the genetic variability 58 that may determine variable effects of IH. For instance, the magnitude of LTF varies among inbred rat strains. 59 Genetically diverse human populations may vary widely in their capacity for achieving functional recovery after repetitive IH; thus, we cannot determine whether genetic variability of enrolled subjects may have influenced our results.
Finally, our study included only four female subjects; thus, we could not investigate sex differences in response to IH. Studies in healthy subjects suggest that no sex differences exist. 60 Fifteen healthy men and women matched for age, race, and body mass index were exposed to eight 4-min episodes of hypoxia (8% O2) during sustained hypercapnia, followed by a 15-min end-recovery period. The study showed that a sustained increase in minute ventilation (i.e., ventilatory LTF), is similar in both men and women after exposure to IH. 60
Conclusions
This study confirms the findings of previous work showing that 5 consecutive days of moderate IH (daily IH) combined with locomotor training improved walking speed and endurance in subjects with iSCI. Further, this study demonstrated that exposure to IH three times per week (repetitive IH) maintained the daily IH-induced walking speed recovery, and progressively increased the daily IH-induced walking endurance recovery for 3 additional weeks. The repetitive IH-induced walking recovery was prolonged for up to 2 weeks after the completion of the study. Finally, the optimal dose to maintain the therapeutic effects of repetitive IH over longer periods remains to be investigated.
The protocol used in this study corresponds to a low-frequency, moderate-dose, and brief exposure to IH, which has extensive evidence of clinical benefits without maladaptive responses. 61 No unwanted side effects were reported after 4 weeks of repetitive IH and, thus, this protocol may represent a safe and effective means of improving walking function in persons with chronic iSCI.
Footnotes
Acknowledgment
The authors thank Pamela San Martin, M.S, for independent statistical analysis and members of the Teletón Institutional Review Board for permanent guidance throughout the execution of the trial. The authors particularly thank all study participants and their families for their commitment and motivation to complete this study.
Financial support for this study was provided by the Fondecyt Grant 11140120, “Comisión Nacional de Investigación Científica y Tecnológica” (CONICYT), Chile.
Author Disclosure Statement
No competing financial interests exist.