
Abstract
The autonomic nervous system can be profoundly affected after spinal cord injury (SCI). Despite its importance to quality of life, autonomic function is rarely systematically assessed in the clinical setting. The International Standards to Document Remaining Autonomic Function after Spinal Cord Injury (ISAFSCI) is an assessment designed to determine which autonomic functions are intact, impaired, or lost after SCI. The psychometric properties of the ISAFSCI have not yet been reported. The objective of this study was to describe the inter-rater reliability of the ISAFSCI. Participants with chronic traumatic SCI (greater than 1 year) able to remain on the same medications for the study period and communicate clearly with the assessor were recruited for the study. A standard protocol minimized variation between the sites. During the first assessment, neurologic examination (ISNCSCI) was performed and ISAFSCI completed. After 10–14 days, the ISAFSCI was repeated. Inter-rater reliability was calculated using percentage agreement, kappa, and weighted kappa statistics. Participants (n = 48) had an average age of 45 ± 12 years. Forty-one (85.4%) were male, 38 (79.2%) had a SCI at or above the T6 level, 24 (50.0%) had a complete SCI. Inter-rater reliability within the general autonomic component was moderate with kappa values ranging 0.41–0.6 (p < 0.05). Within the Lower Urinary Tract, Bowel, and Sexual Function component, agreement was good-strong with weighted kappa values 0.62–0.88 (p < 0.05). Given the results, we conclude that the ISAFSCI can be considered to have at least moderate and up to strong inter-rater reliability, especially in the bladder, bowel, and sexual function component of the assessment.
Introduction
S
Despite this strength, the ISNCSCI has an important limitation in that it focuses on impairments of the motor and sensory systems with omission of an autonomic assessment. 11 This information is absent in the ISNCSCI, despite the significance of autonomic function to the quality of life reported by persons living with SCI. 12 –16
The International Standards to Document Remaining Autonomic Function after Spinal Cord Injury (ISAFSCI) was developed by a working group of the American Spinal Injury Association (ASIA) and International Spinal Cord Society (ISCoS). 17,18 The assessment has been translated into several languages and is in use at numerous rehabilitation centers. The information manual and reporting form is available on the ASIA website. 19 To our knowledge, the psychometric properties of the ISAFSCI have not yet been evaluated. The objective of this study was to evaluate the inter-rater reliability of the ISAFSCI.
Methods
This study was performed in accordance with the Declaration of Helsinki of the World Medical Association. 20 The Hospital and University Research Ethics Committees at each study site approved the study protocol. Individuals were recruited from the SCI community with the use of posters and word of mouth. Persons contacted the study coordinator to become involved in the study. Data collection occurred between June 2011 and April 2014 at two centers.
Investigators evaluated adults with chronic traumatic SCI with no difficulty communicating in English (Table 1). Participants were excluded if there were any recent changes in neurologic function (new motor or sensory changes, bowel or bladder dysfunction) by self-report, or if medication types or doses changed during the study period. This was because some medications can have an effect on lower urinary tract, bowel or sexual function, potentially confounding results.
SCI, spinal cord injury.
The ISAFSCI contains two major components illustrated on the reporting form seen in Figure 1. The first is the General Autonomic Function component and second is the Lower Urinary Tract, Bowel and Sexual Function component. The clinician completes the reporting form during an interview and a minimal physical examination, which includes heart rate and blood pressure measurement.
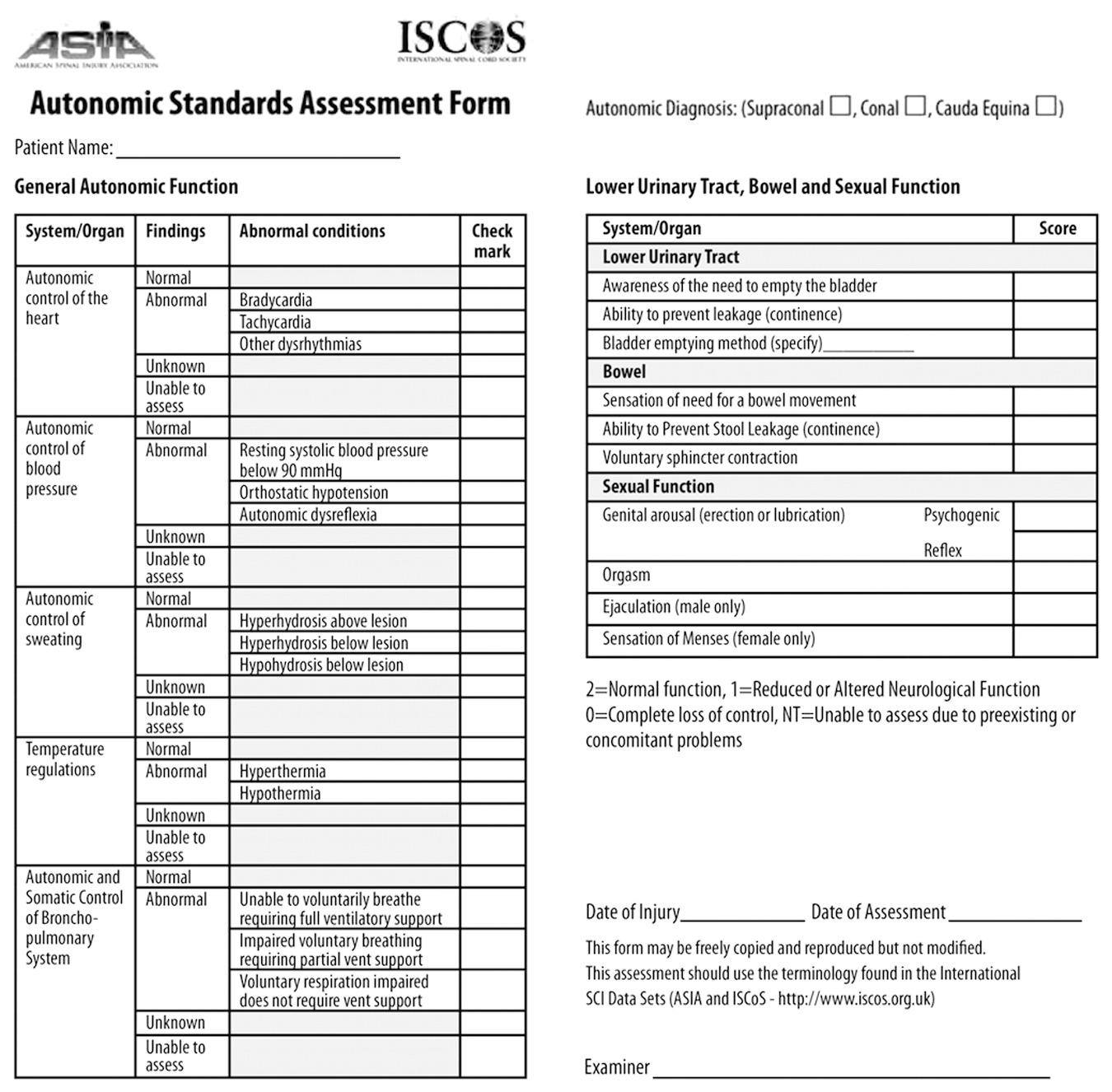
Reporting form for the International Standards to Document Remaining Autonomic function after Spinal Cord Injury (ISAFSCI).
In the General Autonomic Function component (Fig. 1), items are evaluated with a nominal “present” or “absent” response as indicated by a check mark. 18 In addition to information from the interview, data from the physical examination (heart rate and blood pressure) may be used to help the assessor determine responses for the “autonomic control of the heart” and “autonomic control of blood pressure” items on the ISAFSCI reporting form. For example, a participant's baseline bradycardia or hypotension during the assessment may be recorded as a present response for the bradycardia and resting blood pressure below 90 mm Hg. This, however, does not preclude a different response on the reporting form if there is an explanation for the participant's bradycardia or hypotension on that day of the assessment.
In the Lower Urinary Tract, Bowel and Sexual Function component (Fig. 1), each item is scored on an ordinal scale of zero to two, where two represents normal function, one represents reduced or altered neurologic function, and zero represents a complete loss of control. 18 For both components, the response “NT” represents a nontestable field because of a concomitant problem.
To help with the standardization of the study protocol, we developed questions to assist the assessors administering the ISAFSCI (Appendix 1; see online supplementary material at
Study procedures
Two research visits were performed with the assessors. At the first visit, participants discussed the study procedures with the assessor and provided informed consent. Once consent was given, demographic information was collected, heart rate and blood pressure determined, ISNCSCI performed, and the ISAFSCI assessment completed. At the second visit, a different assessor remeasured heart rate and blood pressure and completed the ISAFSCI assessment. Assessors were blinded to each other's results.
The ISAFSCI reporting form (Fig. 1) was filled out by the assessor using the standardized questions (Appendix 1). After discussion with the participant, the assessor decided which response on the form best fit the discussion with the participant.
For certain questions in the ISAFSCI, the assessors prospectively defined time constraints to improve the precision of participant responses. In particular, responses about orthostatic hypotension (OH) for this study were limited to whether or not the participant had OH in the last 6 months. Responses about autonomic dysreflexia (AD) were not time limited, and the assessor added a check mark to the form if the participant had an episode consistent with AD at any time in the past. All other questions were not time limited.
Visits were separated by a period of 10–14 days to avoid a memorized recall of responses on a recommendation published by the ASIA/ISCoS executive committee on the reporting of international standards and data sets. 21
Analysis
Reliability was assessed using percentage agreement, kappa and weighted kappa values. Percentage agreement was calculated for each site by dividing the number of trials the assessors agreed on the response for each item by the total number of trials. 22
Percentage agreement is useful because it is easy to interpret; however, it cannot adjust for agreement occurring because of chance, which could overestimate rater agreement. 23 The kappa statistics are more robust measures of agreement than percentage agreement because they account for the probability of agreement because of chance. 22 Thus, kappa values were chosen to be the primary method of reporting results. It was estimated that a sample size of 50 subjects was needed for an expected kappa coefficient of 0.70 with a 20% margin of error, consistent with other measures. 23
For the General Autonomic Function component, the unweighted kappa statistic was used given that it is a nominal scale, and for the lower urinary tract bowel and sexual function component we used the weighted kappa statistic because this component is an ordinal scale and therefore distribution of the data was expected to differ between components. Acceptable ranges for kappa values were specified according to current literature as:
All analyses were performed using R 3.1 (CRAN: the Comprehensive R Archive Network at
Results
Sixty-five persons were screened, and 48 data sets were entered for final analysis (Fig. 2). The average age of participants was 45 ± 12 years (Table 2) with a bimodal age distribution, one peak occurring in the 20–30 age group and another in the 50–60 age group. Most participants had a neurologic level of injury at or above the T6 spinal segment. Most participants had motor complete SCI according to the standard neurological evaluation (AIS A and B). Average time between two assessments was 15 ± 4.3 days.
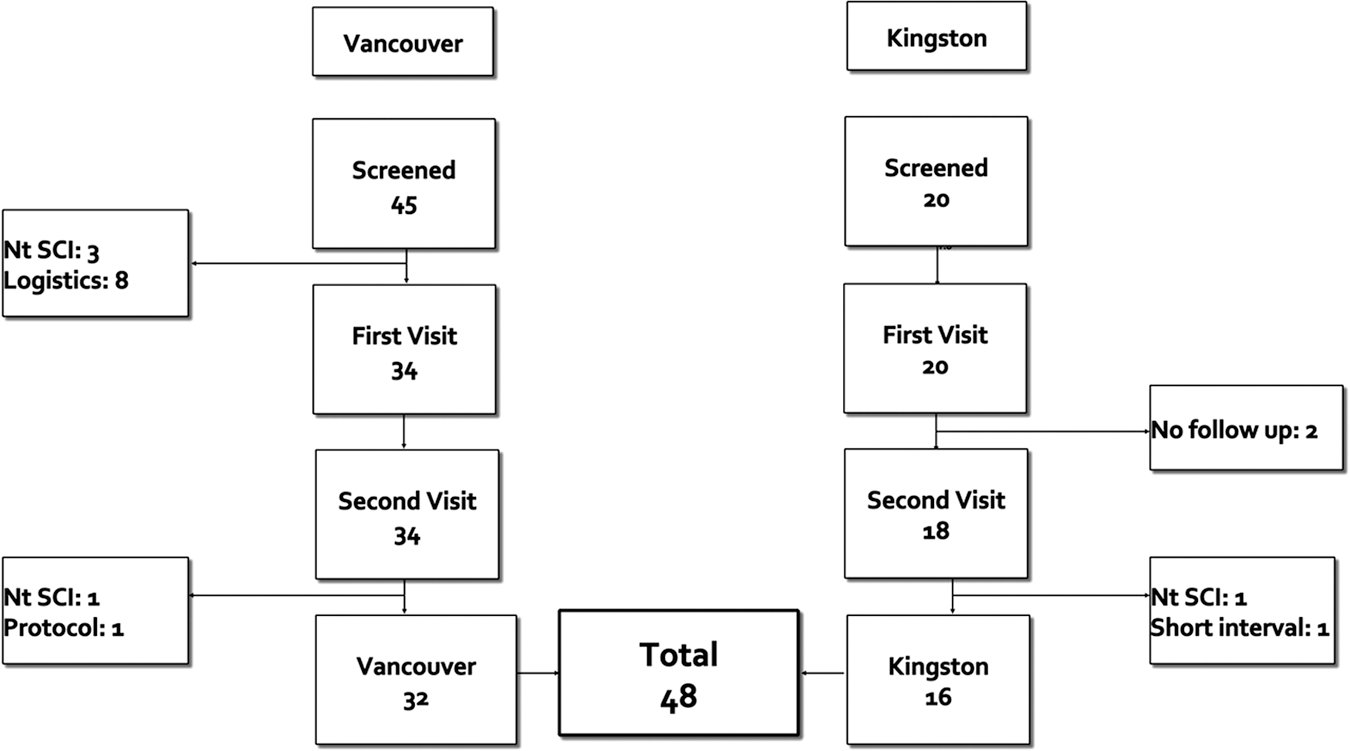
Study flow chart. Nt. SCI—nontraumatic spinal cord injury. Logistics— participant was unable to arrange transportation to and from the center for assessment; No follow-up—participant was not present for the second appointment; Protocol—the study protocol was not properly followed; Short interval—although the participant completed the study protocol, such a short interval between assessments could have resulted in a memorized response.
SD, standard deviation; SCI, spinal cord injury; AIS, American Spinal Injury Association International Standards; T6, 6th thoracic spinal level; conus, conus medullaris; cauda, cauda equina; AIS-A, motor and sensory complete injury; AIS-B, motor complete, sensory incomplete injury; AIS-C, motor and sensory incomplete injury; AIS-D, motor and sensory incomplete injury.
Percentage agreement values
In the General Autonomic Function component, percentage agreement values varied between 59–100%; however, generally they were above 70% with a few exceptions (Appendix 2; see online supplementary material at
Kappa values
Kappa values were observed to be in the “good/strong agreement” range for most questions in the autonomic control of blood pressure, temperature regulation and autonomic and somatic control of the bronchopulmonary system sections (Table 3). This was also the case for the entire Lower Urinary Tract, Bowel and Sexual Function component (Table 3). Kappa values were observed to be in the “moderate agreement” range for all other sections of the form, especially in the autonomic control of the heart, resting systolic blood pressure below 90 mm Hg, autonomic control of sweating and voluntary respiration impaired, not needing ventilator support (Fig. 3).

Inter-rater reliability of the International Standards to Document Remaining Autonomic function after Spinal Cord Injury. Legend in top right corresponds to strength ranges for kappa values. See Table 3 for exact kappa values.
Any cell with ‘-’ denotes that there were too few responses in the sample to compute a meaningful value.
K, Kappa (unweighted); NT, not testable; SBP, systolic blood pressure; mm Hg, millimeters of mercury; OH, orthostatic hypotension; AD, autonomic dysreflexia; Hyperhi., hyperhidrosis; Above, above neurologic level of injury; Below, below neurologic level of injury; Hypohi., hypohidrosis; Resp., respiration; Full vent, full ventilator support; Imp., impaired; No vent, no ventilator support; Partial vent, partial ventilator support; ωK, Kappa (weighted).
Discussion
This prospective study evaluated the inter-rater reliability of the ISAFSCI assessment in persons living with chronic, traumatic SCI. Key findings were that inter-rater reliability of the entire assessment was at least moderate, and in some sections (especially in the Lower Urinary Tract, Bowel and Sexual Function component) were strong. For the General Autonomic Function component, agreement was in the moderate to good range and for the Lower Urinary Tract, Bowel and Sexual Function component, it was consistently in the good to strong range.
Numerous factors likely contribute to the differences between the inter-rater reliability seen in the two components of the ISAFSCI. One of these factors may be how each item is designed and scored. The General Autonomic Function component is scored in a nominal fashion, whereas the Lower Urinary Tract, Bowel and Sexual Function component is scored in an ordinal fashion (Fig. 1). In the latter, more options for describing function may make deciding on a response easier as a wide range of “altered neurological function” is present in those with SCI. Also, “complete loss of control” may be easier to discern for both the participant and assessor.
Another possible explanation is that some persons living with SCI invest significant time learning how to manage bladder, bowel, and sexual function compared with the other general autonomic function and may be well versed in communicating what is normal, altered but present, and complete loss of control.
One unique aspect of the study was the development of standardized questions for each component of the ISAFSCI assessment to provide a unified approach for assessors in the autonomic evaluation of persons living with SCI. These questions were developed and agreed on by the study investigators a priori to standardize the methods. Although both ASIA and ISCoS have developed educational materials 18,25 (ASTeP) for directions and use on the initial version of the ISAFSCI, no explicit questions are provided in this version to guide assessors regarding “how” to conduct the assessment.
The involvement of two assessment sites in the study provides unique insight into the reliability of the ISAFSCI. Despite having standard questions and largely similar populations, each site had slightly different reliability results. Discrepancies between sites were greatest for sections within the General Autonomic component of the ISAFSCI. This was most likely the result of the present design of these sections (examples being autonomic control of the heart, autonomic control of sweating, temperature regulation and autonomic and somatic control of the bronchopulmonary system) that require more guidance for assessors as well as additional information within the ISAFSCI table.
The investigators had to elaborate somewhat on what was considered a positive response for some items. For example, OH is common in the early period after SCI and may resolve in more than 70% of persons within 4 months after inury. 26,27 With the present format of the ISAFSCI, there is no ability to indicate when this condition was present, or if it still exists. The investigators chose to specify the time period as “OH in the last 6 months” to limit positive responses to persons with ongoing, symptomatic OH. With future revisions, it is crucial that the ISAFSCI specify the exact time frame, duration post-injury, or recovery milestone (e.g., discharge from acute care, discharge from rehabilitation) during which symptoms can be considered present or absent.
In contrast to time limits on OH, AD was recorded as a positive response if the person had experienced AD at any time in the past. This may overinclude persons with a positive response and may in part be the reason for perfect agreement for this item of the ISAFSCI.
We also would like to acknowledge the fact that in the present format, documenting events such as OH and AD means relying on subjective information obtained by the clinician from an interview and physical examination that includes heart rate and blood pressure measurement at a single point in time. Unfortunately, this will result in missing persons who have asymptomatic episodes of OH and AD, known to be common after SCI 28 –30 because persons without proper monitoring may be unaware that they have these conditions. The ISAFSCI assessment would benefit in the future with the addition of previously documented episodes of AD and OH even if they were completely asymptomatic.
Certain fields of the ISAFSCI could not be assessed for reliability because of the frequency of responses in that field. For example, most unknown or NT fields in the general autonomic component had such few responses that agreement or kappa could not be calculated. This was also the case for fields such as tachycardia, respiratory function impaired, requiring full time ventilator support. and sensation of menses where such few positive responses were present that a kappa value could not be calculated. As such, conclusion about the inter-rater reliability of these items cannot be drawn at this time.
In the Lower Urinary Tract, Bowel and Sexual Function component of the ISAFSCI, a few unexpected results were obtained. At the outset of the study, the investigators predicted that the inter-rater reliability of questions about sexual function would be marginal, especially that of orgasm given that a universal definition of what orgasm is does not exist. 31 This, however, was not what was shown by the data, where weighted kappa values were found to be in the good to strong range. This could have been because of the standardized nature of the questions, the ordinal nature of this component of the form, participants recalling responses from previous visit, or truly because persons in this study were clear on their sexual abilities and impairments.
Some factors in our study affect the generalizability of this research to the general SCI population. Persons in the study were more likely to be male, with a male to female ratio higher than what is seen in the general SCI population of 70%:20%. 32 Our population had a bimodal age distribution, with one peak occurring around the 20–30 age category and another in the 50–60 age category, which is similar to the recent demographic trend noted in the SCI population in Canada. 33 In contrast to the general SCI population, however, our sample was more likely to have completed high school 34 and included a disproportionate number of persons with a Caucasian background.
A few important limitations are present in this study that include the subjective nature of the responses obtained. Because of this, persons with silent AD and OH were likely missed by the assessment. The inclusion of two sites for assessment could be viewed as a limitation or strength of the study given that the ISAFSCI is applied in diverse geographical settings. Finally, this study was limited to English speaking individuals, limiting the generalizability of these results to other languages.
Conclusions
The ISAFSCI is an assessment designed to document the remaining autonomic function present after SCI. The assessment itself brings attention to the importance of adding an assessment of autonomic function to standard neurological examination of persons with SCI. Under the conditions in this study, the ISAFSCI was shown to have moderate to strong inter-rater reliability. The General Autonomic Function component of the ISAFSCI assessment showed moderate to good inter-rater reliability, whereas in the lower urinary tract, bowel and sexual function component, it was in the good to strong range. Future versions of the ISAFSCI should aim to standardize the assessment and provide a standard training protocol for assessors to improve its reliability.
Footnotes
Acknowledgments
We would like to acknowledge all participants who volunteered time and effort to participate in the study. The BC Rehab Foundation deserves a special acknowledgement for providing start-up funding through their fund for research and innovation. This study was also supported by a grant from the Rick Hansen Institute (PI Dr. A. Krassioukov), which received funding from the Federal Government of Canada (Health Canada, Western Economic Diversification Fund).
Author Disclosure Statement
Dr. Krassioukov is supported by Endowed Chair in Rehabilitation Medicine University of British Columbia, and grants from the Canadian Heart and Stroke Foundation, Canadian Institute of Health Research, Canadian Foundation for Innovation, Craig H. Neilsen Foundation, Christopher and Dana Reeve Foundation, Pfizer, Welspect, and Allergan. Drs. Noonan and Fallah are employees of the Rick Hansen Institute. For the remaining authors, no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.