
Abstract
This single-center prospective observational study aims to describe the prevalence of vitamin D deficiency (VDD) in the traumatic brain injury (TBI) population and identify any relationship between vitamin D and severity of head injury or quality of life. One hundred twenty-four TBI patients had serum vitamin D (25-OHD) levels measured at the local post-TBI endocrine screening clinic over 20 months. Quality of Life after Brain Injury questionnaires were completed by the patient concurrently. A multivariate regressional analysis was performed, controlling for age, season, ethnicity, time since injury, TBI severity, and gender. A total of 34% (n = 42) of the cohort were vitamin D deficient (25-OHD <25 nmol/L), with a further 23% (n = 29) having insufficient levels (25-OHD 25–50 nmol/L). Vitamin D was significantly lower in patients with severe TBI than in patients with mild TBI (n = 95; p = 0.03; confidence interval [CI] 95% −23.60 to −1.21; mean effect size 12.40 nmol/L). There was a trend for self-reported quality of life to be better in patients with optimum vitamin D levels than in patients with deficient vitamin D levels, controlling for severity of injury (n = 81; p = 0.05; CI 95% −0.07 to 21.27). This is the first study to identify a significant relationship between vitamin D levels and severity of head injury. Clinicians should actively screen for and treat VDD in head-injured patients to reduce the risk of further morbidity, such as osteomalacia and cardiovascular disease. Future research should establish the natural history of vitamin D levels following TBI to identify at which stage VDD develops and whether vitamin D replacement could have a beneficial effect on recovery and quality of life.
Introduction
T
Although vitamin D is technically misnamed and is in fact a secosteroid, it is still grouped with other vitamins for historical reasons. The main source of vitamin D for humans is sunlight. Ultraviolet B light causes the photolysis of 7-dehydrocholesterol to pre–vitamin D in the skin. 2 Pre–vitamin D undergoes isomerization producing vitamin D3 and is then metabolized twice, first in the hepatic mitochondria to form 25-hydroxyvitamin D3 (25-OHD), then in renal mitochondria to form the active vitamin D molecule 1,25 hydroxyvitamin D3 (1,25-(OH)2D3; Fig. 1). 3 The second source of vitamin D for humans comes from dietary intake. UK food sources of vitamin D include oily fish, eggs and fortified fat spreads, and cereals. 4 In clinical practice, we measure 25-OHD serum levels as 1,25-(OH)2D3 circulates in such a low concentration that assessing levels becomes challenging.
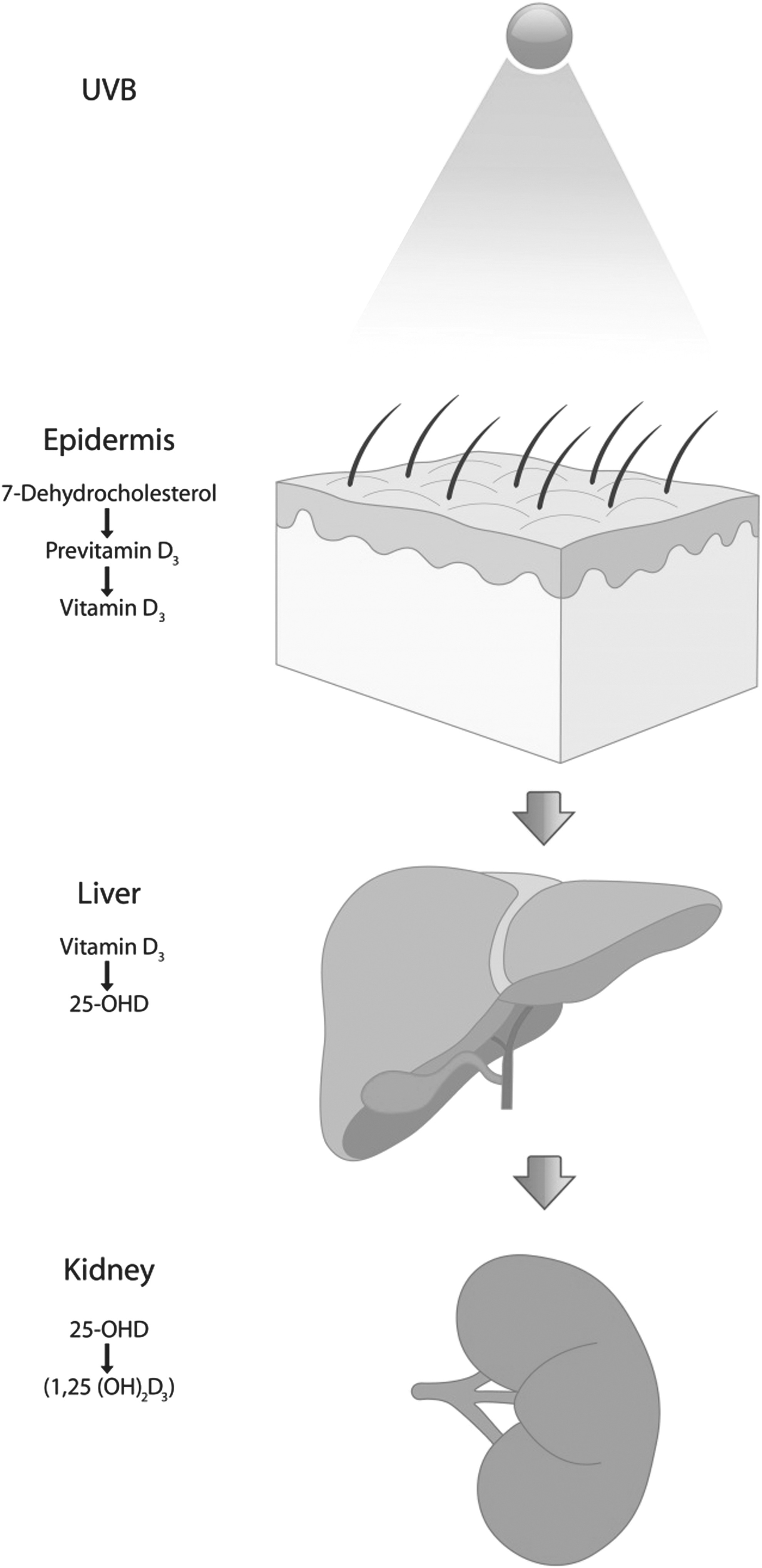
Vitamin D synthesis (with thanks to Mr. A. Dakin of the University of Birmingham Graphics Department).
Given the emerging evidence supporting its role in an increasing number of complex processes, vitamin D has become a hot topic; from discussion on online forums
5
to governmental guidelines. In 2014, the UK National Institute for Health and Care Excellence (NICE) published guidelines with the aim to combat VDD across the general population.
6
They identified the following “at-risk” groups: • infants and children younger than 5 years • pregnant and breastfeeding women • people older than 65 years • people with low sunlight exposure, including those who cover their skin for cultural reasons or are confined to indoors for long periods • people with darker skin (e.g., those of African, African-Caribbean, or South Asian family origin).
6
A UK National Diet and Nutrition Survey was undertaken from 2008 to 2012 and the results were published in 2014. On average, intake of vitamins was adequate, excluding vitamin D. 7 In addition to nutritional questionnaires, serum was sampled from participants. Overall, the survey reported a prevalence of VDD in 22.8% of adults ages 19–64 years, with 21.7% prevalence in males and 24.0% prevalence in females (Table 1).
Vitamin D deficiency contributes to a myriad of diseases and is a risk factor for conditions with significant morbidity. VDD is most commonly known as a cause of rickets in children and osteomalacia in adults. Complications include muscle weakness, skeletal pain, increased fracture risk, and skeletal deformities such as “bowlegs” and thinning of the skull (craniotabes). 8 Vitamin D also has been found to have a complex modulating action within the immune system, 9 –11 has been linked with cardiovascular disease, 12 is known to play a role in multiple cancers, 13 and has been widely investigated in other conditions such as multiple sclerosis, type 1 and 2 diabetes mellitus, pre-eclampsia, rheumatoid arthritis, dementia, and metabolic syndrome. 14,15
Within the context of clinical TBI management, endocrinological deficiency and pituitary malfunction are becoming more familiar as longer-term post-injury sequelae along with pituitary dysfunction and diabetes insipidus, demonstrating a prevalence of 5.4% 16 to 19.0% 17 and 2.9%, 18 respectively. To detect these conditions, our unit developed a collaborative post-TBI endocrine screening clinic, operational since July 2013. In addition to screening for pituitary dysfunction, serum vitamin D levels also were measured following a published study that showed vitamin D supplementation to significantly reduce the incidence of seizures. 19 It appeared that a large proportion of patients screened were found to be either vitamin D insufficient or deficient. This led our team to generate the hypothesis that VDD was more prevalent in TBI patients, compared with the general population. Given the emerging evidence that vitamin D plays important roles within the brain, we also hypothesized that vitamin D levels decrease as severity of injury increases.
This article aims to describe the prevalence of vitamin D deficiency (VDD) in the post-TBI population and quantify the relationship between vitamin D levels and severity of head injury or subsequent quality of life (QoL).
Methods
The Queen Elizabeth Hospital Birmingham, UK, has a well-established post-TBI endocrine screening outpatient clinic. Patients were referred here directly from the consultant lead-neurosurgical TBI clinic for anterior pituitary screening and vitamin D (25-OHD) level testing.
As part of the TBI clinic attendance, patients also completed the Quality of Life after Brain Injury (QOLIBRI) questionnaire. The QOLIBRI is an internationally recognized tool specifically designed for TBI patients. 20 Self-reported scores given by the patient generate a score on a scale from 0–100 where 0 is the lowest QoL and 100 is the best QoL.
Details of 124 patients referred for screening were collected between the dates of September 2013 to July 2015. Demographic, clinical, and laboratory data were collected from the hospital information technology systems. Severity of head injury was categorized by best immediately post-resuscitative Glasgow Coma Scale (GCS) score, categorized as mild (GCS 13–15), moderate (GCS 9–12), and severe (3–8). As some patients were referred to the TBI clinic from local hospitals, post-resuscitative GCS data were not always available. The UK seasons were categorized as spring (March to May), summer (June to August), autumn (September to November) and winter (December to February). There was a wide variability in the time periods between injury and sampling across the cohort. To explore whether this played a significant role in levels of vitamin D, “time since injury” was included as a variable in multivariate analysis. Six months is a widely accepted outcome milestone in TBI and is a broadly used across TBI academia. It is for this reason the authors chose 6 months as the cut-off point.
The UK Scientific Advisory Committee on Nutrition released a draft report on vitamin D in 2015. The report described various reference ranges that have been quoted in the literature, many of which vary. 21 The general consensus on the level considered deficient is 25-OHD <25 nmol/L and this is the cut-off used by NICE guidance on vitamin D. 6 Additional reference ranges we have used in this study (Table 2) are comparable to recent published studies, although we must stress there is no internationally agreed reference range for vitamin D.
25-OHD was measured by the University Hospitals Birmingham laboratories using the gold standard, liquid chromatography-tandem mass spectrometry.
Exclusions criteria
Exclusion criteria included any patient with renal or hepatic failure and patients who received vitamin D supplementation at the time of sampling. Liver and kidney function were assessed simultaneously by serum testing and drug history was documented.
Statistical analysis
The statistical software “R” was used to perform these analyses and cut-off for clinical significance set at p < 0.05. Multiple multivariate regressional analyses were performed with vitamin D treated as both categorical and continuous data. All statistical analyses were performed by a university-affiliated medical statistician.
Results
One-hundred twenty-four clinic patients were included in this study from the dates September 2013 to July 2015. No patients were excluded. The median age was 41 years (range 16–90) and 79% were male. The median time between injury and vitamin D sampling was 285 days (range, 32–939 days).
Twenty-three percent of the cohort had a severe TBI, 14% moderate TBI, and 63% mild TBI. With regard to time of sampling, 27% (n = 33) were taken in the spring, 20% (n = 25) in summer, 27% (n = 34) in autumn, and 26% (n = 32) in the winter. Ethnicity was broken down to Caucasian 73% (n = 91), South Asian 10% (n = 12), and other/unspecified 17% (n = 21).
Overall, 34% (n = 42) of the cohort was vitamin D deficient, with a further 23% (n = 29) demonstrating vitamin D insufficiency. Table 3 provides a detailed breakdown of prevalence within the different groups. The group with the highest percentage of severe TBIs was males ages 19–64 years at 28.0% (n = 23). VDD was present in 48.3% of severe TBI patients, compared with 29.4% of moderate TBI patients, and 26.5% of mild TBI patients (Table 4).
TBI, traumatic brain injury.
Excluding TBI severity data, a multivariable linear regression was performed across all 124 patients. Vitamin D was treated as a continuous variable and was modeled by age, ethnicity, season, time since injury <6 months, and gender (Table 5). This analysis demonstrated that levels of vitamin D taken in the summer and autumn were significantly higher than samples taken in the winter. With regard to significant findings in ethnicity, mean vitamin D was found to be 17.68 nmol/L higher in Caucasians than in South Asians (p = 0.04, CI 95% 0.50 to 34.76). No significant difference in vitamin D was demonstrated between samples taken within 6 months from injury and samples taken more than 6 months from injury (p = 0.44, CI 95% −15.30 to 6.65). No significant differences in vitamin D were found with change in age or gender (Table 5; Fig. 2).

Mean differences in vitamin D modeled by age, ethnicity, season, time of sample, and gender.
Coef, coefficient; SE, standard error; CI, confidence interval.
TBI severity was then included in the multivariate linear regression, controlling again for age, ethnicity, season, time since injury <6 months, and gender. This was a separate analysis as only 95 patients had TBI severity data available. Vitamin D was significantly lower in severe TBI than in mild TBI (p = 0.03, CI 95% −23.60 to −1.21), with mean vitamin D in severe TBI 12.40 nmol/L lower than in mild TBI (Table 6; Fig. 3).
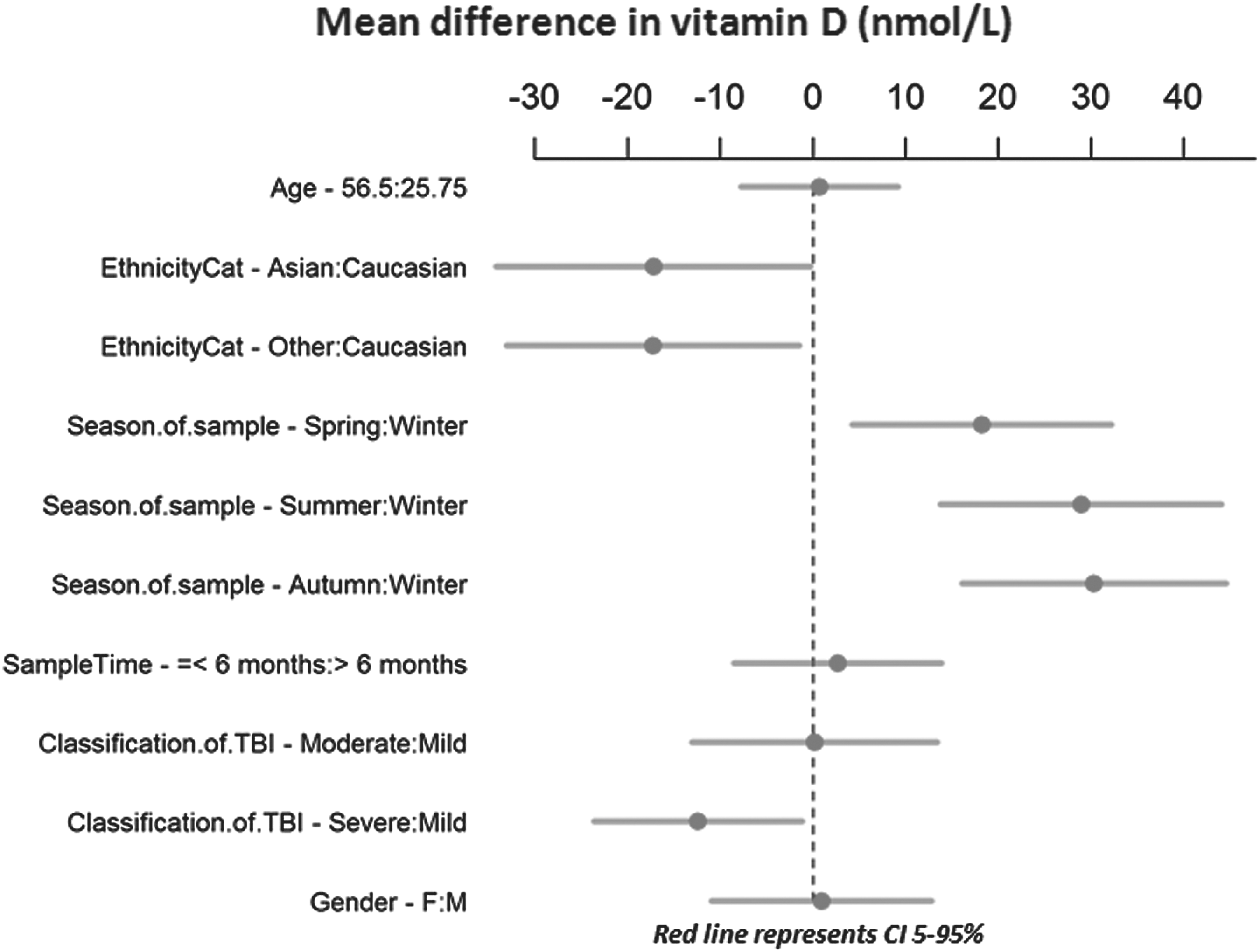
Mean differences in vitamin D modeled by age, ethnicity, season, time of sample, gender, and traumatic brain injury (TBI) severity.
TBI, traumatic brain injury; Coef, coefficient; SE, standard error; CI, confidence interval.
To analyze QoL, QOLIBRI score was modeled by vitamin D as a categorical variable in a univariate linear regression and controlled for TBI severity. This analysis incorporated 81 observations patients as QOLIBRI questionnaires were not completed for all patients. Vitamin D category “deficient” was used as the reference. QOLIBRI was demonstrated to be increased in the patient cohort with optimal vitamin D levels, compared with those with deficient vitamin D levels, although this finding did not quite reach significance (p = 0.05, CI 95% −0.07 to 21.27). Patients with optimal vitamin D scored 10.60 points higher on the QOLIBRI scale, compared with the deficient category. No significant difference in QOLIBRI scores were found between the vitamin D deficient group, compared with insufficient or adequate vitamin D cohorts (Table 7; Fig. 4). When vitamin D is treated as a continuous variable, the correlation between vitamin D levels and QOLIBRI score is 0.165 (95% CI −0.026 to 0.344), which suggests a weak relationship between these variables (Fig. 5). As vitamin D levels increase, there is a weak association with increased QOLIBRI score (p = 0.09), but the magnitude of this is small.
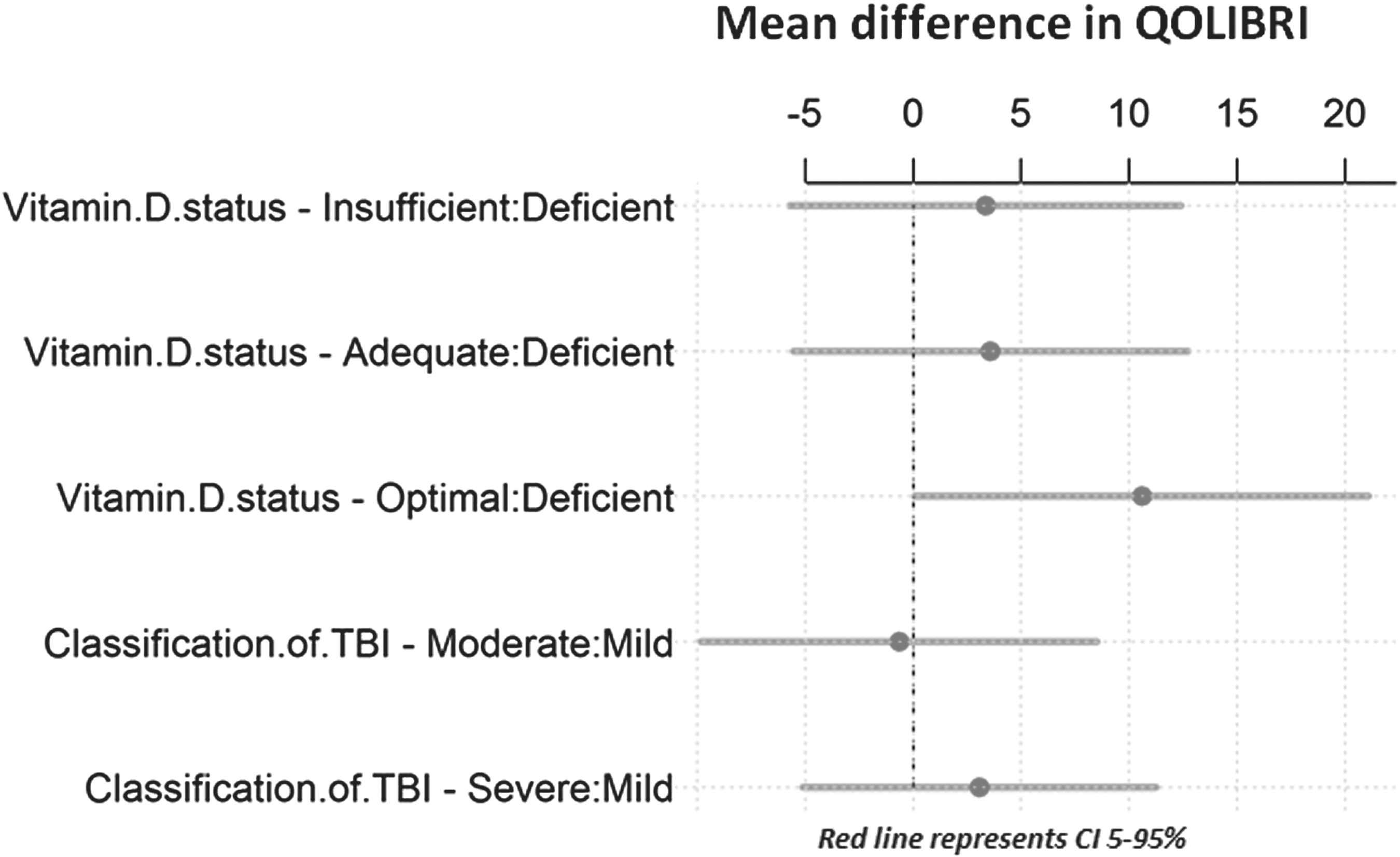
Mean differences in Quality of Life after Brain Injury (QOLIBRI) scores by vitamin D, controlled for severity of injury.
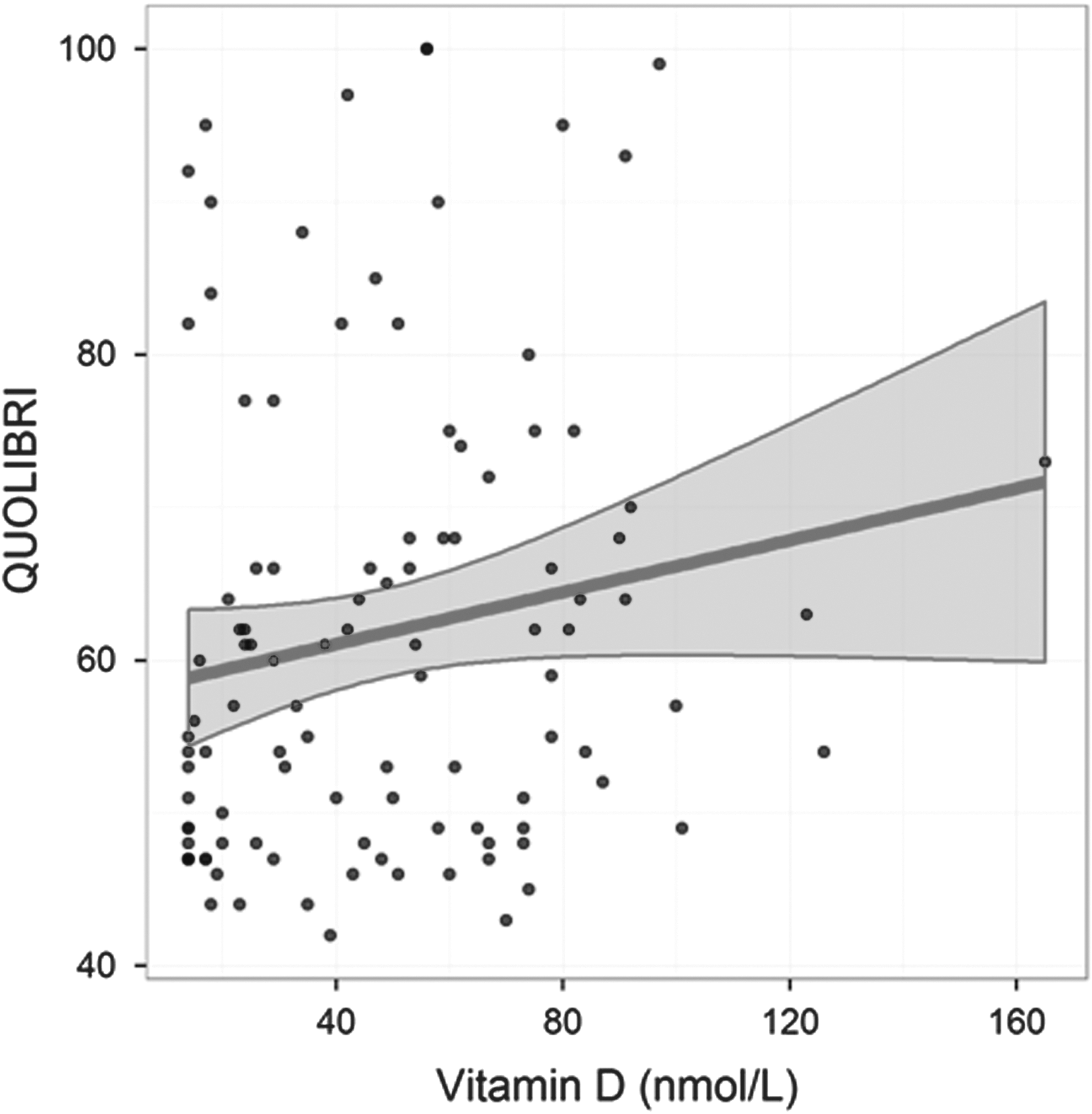
Quality of Life after Brain Injury (QOLIBRI) scores against vitamin D regression output. Dots are observed values. Lines and shaded areas denote predicted values and 95% confidence interval.
TBI, traumatic brain injury; Coef, coefficient; SE, standard error; CI, confidence interval.
Discussion
Overall, the prevalence of VDD in TBI patients was increased, compared with the UK national prevalence and the local prevalence of 24% reported in inner-city Birmingham outpatient services. 22 There are two important finding of this article not previously described in the literature. First, that vitamin D levels demonstrate a significant relationship with severity of TBI and second, that there was a trend for QoL to be higher in patients with optimal vitamin D levels independent of severity of injury.
No data regarding ethnicity or skin color was available from the population sampled for the National Diet and Nutrition Survey. The authors have therefore assumed that patients included in this national survey sample reflect national census 2011 data regarding ethnicity, with 86% of the population being of Caucasian origin. 23 Our study had a lower percentage of Caucasians at 73% and so we would expect to have a higher pre-injury prevalence of VDD, although there is no way to prove this. However, data from a Birmingham-based outpatients article reporting on vitamin D levels are based on a more diverse population, consisting of 38% Caucasian, 15% Afro-Caribbean, 30% Asian, and 17% other. 22 The authors have concluded, therefore, that our pre-injury baseline prevalence of VDD lies somewhere between the UK national average of 22.8% and the Birmingham average of 24%.
The National Diet and Nutrition Survey 2014 demonstrates variation in vitamin D deficiency across different age groups and genders. 7 UK females ages 11–18 years appear to hold the highest percentage of vitamin D deficient individuals of all groups reported at 24.4%. In our study, the highest prevalence of VDD is in males ages 19–64 years. This finding is most likely an epiphenomenon, however, as this group also holds the highest percentage of severely injured patients who, as we have demonstrated, have significantly lower levels of vitamin D.
QoL and functional outcome are notoriously difficult to assess in TBI patients. Our results demonstrate that there is a trend for a higher quality of life in patients with optimal vitamin D levels, compared with those who are deficient. However, the correlation between vitamin D and QOLIBRI score is only weak. The current tools used to establish QoL and function are blunt and do not reflect more subtle changes found within higher functioning individuals. It is for this reason, perhaps, that no significant changes in quality of life have been demonstrated between cohorts with deficient vitamin D and insufficient or adequate vitamin D levels. The aim of this study was not to assess functional outcome and therefore such data were not collected. Any future study design—if the intent is to investigate functional outcome—should include detailed follow-up evaluation with a wider battery of assessments.
A recent retrospective study published by Jamall and colleagues in February 2016 also analyzed vitamin D in TBI patients. 24 While there are plenty of similarities between that study and this, there are several key differences, which may account for different findings. In our study, we defined vitamin D deficiency in accordance with the NICE definition of vitamin D deficiency (< 25 nmol/L), a cut-off that is widely used across the majority of clinical vitamin D studies. 6 Jamall and colleagues defined VDD as serum 25-OHD <40 nmol/L and this explains why the group reported a higher prevalence of VDD in their patient cohort.
Jamall and colleagues used several different self-reported questionnaires to measure outcome against TBI patients' vitamin D status. Where QoL was measured by Nottingham Health Profile 25 and Short Form 36, 26 no significant difference was found between vitamin D and QoL. Sleep was measured using the Epworth Sleepiness Scale 27 and the Pittsburgh Sleep Quality Index, 28 with neither questionnaire demonstrating a relationship between vitamin D status and sleep. However, the group did demonstrate that TBI patients with VDD had increased symptoms of depression when measured using the Beck Depression Inventory II, 29 in addition to poorer cognition, as defined by the Addenbrooke's Cognitive Examination Revised. 30
The study by Jamall and colleagues 24 utilized the Mayo classification of TBI to group severity, whereas we used post-resuscitative GCS to classify groups as mild, moderate or severe. Classifying severity using GCS identified a mild TBI category, which made up the majority of our patient cohort at 63%. Our data demonstrate that although there is a statistically significant difference in VDD between mild and severe TBI, we found no significant difference between moderate and severe cohorts. It may therefore be the case that the Jamall and colleagues study did not include enough patients with a milder severity of injury to detect a significant difference between their different markers of TBI severity. The conflicting findings between these two studies again highlights the need for further research into vitamin D in TBI and a thorough approach to study design.
There are several hypotheses to explain the high prevalence of VDD in TBI clinic patients. Perhaps the simplest explanation is that after a brain injury, there is often a change in behavior. When we refer back to the risk factors for VDD identified by the NICE guidance, 6 it is clear that one large factor is commonplace in patients post-TBI. Those with even mild TBI may become withdrawn, suffer with depression, or take time off work, along with a myriad of other symptoms leading to less time spent outdoors and reduced exposure to sunlight. Patients also may undergo a change in diet, especially those who require long-term nasogastric or percutaneous endoscopic gastrostomy feeding. No doubt these factors play a role in the increased VDD prevalence in the TBI population; however, recent evidence supports the multiple neurological roles of vitamin D. Could these mechanisms somehow be depleting vitamin D stores post-injury?
The role of vitamin D in neurological functioning was first suggested after the discovery of high-affinity vitamin D receptors (VDRs) in the pituitary, forebrain, hindbrain, and spinal cord of rats. 31 In addition to this discovery, the enzyme 1α-hydroxylase also has been identified in multiple areas of the human brain. Classically found in the kidney, 1α-hydroxylase converts 25-OHD into the active vitamin D molecule 1,25(OH)2D3. The enzyme was found in the cytoplasm of glial cells and neurons, both in the presence and absence of VDRs in the nuclei. The abundance of 1α-hydroxylase within the brain suggests that, just like within the kidneys, active vitamin D plays an important local role within the central nervous system, implying autocrine and/or paracrine function. 32
Vitamin D has demonstrated neuroprotective effects via several different mechanisms. Many articles have reported the ability of vitamin D to alter levels of intra-cerebral neurotrophic factors, 33 –40 which in turn have been demonstrated to have both protective and restorative effects. 34 Vitamin D also has been found to reduce oxidative stress by dampening the toxic effects of free radicals and reactive oxygen species. 41 –43
Vitamin D has been proven to influence neuroinflammation processes by altering both amyloid and tau protein pathways 44,45 and altering toll-like receptor 4 expression. 46 Vitamin D receptors also have been recognized as transcription regulation factors since the 1980s 47 and genomic mapping has demonstrated VDR clusters in close proximity to genes coding for neurological autoimmune conditions such as multiple sclerosis. 48 Vitamin D also appears to play a role in neuroplasticity, with upregulation of growth factors and alterations to the developing fetal brain. 39,49,50
Critical illness and admission to the intensive care unit (ICU) have also been extensively studied in relation to VDD. There is increasing evidence that VDD is associated with poorer outcome in ICU patients. Lower serum vitamin D levels on admission to ICU have been associated with increased 28-day mortality in septic patients 51 and increased length of stay. 52 This would suggest that pre-morbid VDD is a risk factor for poorer outcome. Our data demonstrate that patients with a severe TBI have increased rates of VDD in clinic, compared with patients with a mild TBI. Rather than the severity of TBI contributing to the development of VDD, could pre-morbid VDD be leading to prolonged ICU stays and poorer outcome? A small retrospective study conducted in 2014 demonstrated no significant correlation between admission vitamin D and neurological outcome on discharge from ICU in TBI patients; however, the outcome measured was the difference between admission GCS and ICU discharge GCS. The authors highlighted several issues with the study design and commented on the small sample size and recommended a well-designed prospective study. 53
The authors of this article put forward three hypotheses to account for the high prevalence of vitamin D deficiency in TBI clinic patients: 1) that behavioral changes following injury lead to decreased vitamin D intake by changes in diet or exposure to sunlight; 2) that vitamin D stores are depleted through the neuroprotective and restorative processes occurring following brain injury; and 3) that VDD develops following any period of critical illness as a systemic response. There are likely elements at play from all three of these factors.
An intricate interplay may exist between TBI severity and vitamin D levels. Pre-morbid VDD may lead to a more severe head injury, as less vitamin D is available to mount an anti-neuroinflammatory, neuroprotective, or neuroplastic response to injury. Conversely, a more severe injury could theoretically “use-up” available stores of vitamin D, leading to increased rates of deficiency.
Limitations
The most obvious limitation of the study is that no pre-morbid vitamin D status was available to establish baseline percentage of vitamin D deficiency within the patient cohort. As it is impossible to perform venepuncture for research purposes prior to the patient suffering TBI, the authors advise that any future study into vitamin D in TBI aims to take biological samples as close to the time of injury as is possible. Further research, however, is required to establish over what time period post-injury vitamin D levels fall.
We did not collect any data on additional injuries as many of the patients were referred to the clinic from other hospitals and clinical data were sparse. The authors recognize the limitations of categorizing severity of injury by post-resuscitative GCS and advise that future prospective study categorizes severity of injury by additional means such as Injury Severity Score or the New Injury Severity Score collected formally by the UK and Wales Trauma Audit Research Network (TARN).
Body mass index (BMI) was not collected prospectively. As obesity has been identified to influence vitamin D levels, we advise future study designs to include BMI measurement as a variable.
Data were not prospectively recorded for conditions in which vitamin D may be affected such as gastrointestinal disorders, malnutrition, anti-epileptic medication, alcohol abuse, or diabetes mellitus.
Conclusion
Vitamin D deficiency is more prevalent in the TBI population, compared with the UK general population and the local population of Birmingham. Patients suffering a severe TBI have significantly lower levels of vitamin D at follow up, compared with patients suffering mild TBI. There was also a trend for QoL to be poorer in patients with deficient levels of vitamin D, compared with optimal levels, independent of severity of injury.
The implications of data presented in this article and potential for future studies are vast. First, we must establish whether the fall in vitamin D levels following injury are specific to TBI or whether this phenomenon occurs following all trauma and critical illness. Second, the natural history of vitamin D following injury needs to be described and mapped to establish at what stage VDD develops.
Clinicians already know that treating VDD in the community reduces the risk of fractures and cardiovascular disease. It is therefore important that we highlight TBI patients as an additional at-risk group and routinely screen for the condition as we do for pituitary dysfunction. In addition, this article has highlighted the potential use of vitamin D as a therapeutic agent and a randomized control trial of vitamin D therapy in TBI should be investigated.
Footnotes
Acknowledgments
The authors would like to acknowledge the research team at the Surgical Reconstruction and Microbiology Research Centre (SRMRC) for both clinical and logistical support.
Author Disclosure Statement
The National Institute for Health Research (NIHR) SRMRC is a partnership between the NIHR, University Hospitals Birmingham National Health Service (NHS) Foundation Trust, the University of Birmingham, and the Royal Center for Defense Medicine.
This article presents independent research supported by the NIHR. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health, the University of Birmingham, or the Ministry of Defense.
No competing financial interests exist.