
Abstract
Several recent global traumatic brain injury (TBI) initiatives rely on practice variation in diagnostic and treatment methods to answer effectiveness questions. One of these scientific dilemmas, the surgical management of the traumatic acute subdural hematoma (ASDH) might be variable among countries, among centers within countries, and even among neurosurgeons within a center, and hence be amenable for a comparative effectiveness study. The aim of our questionnaire, therefore, was to explore variations in treatment for ASDH among neurosurgeons in similar centers in a densely populated geographical area. An online questionnaire, involving treatment decisions on six case vignettes of ASDH, was sent to 93 neurosurgeons in The Netherlands and Belgium. Clinical and radiological variables differed per case. Sixty neurosurgeons filled out the questionnaire (response rate 65%). For case vignettes with severe TBI and an ASDH, there was a modest variation in the decision to evacuate the hematoma and a large variation in the decision to combine the evacuation with a decompressive craniectomy. The main reasons for operating were “neurological condition” and “mass effect.” For ASDH and mild/moderate TBI, there was large variation in the decision of whether to operate or not, whereas “hematoma size” was the predominant motivation for surgery. Significant inter-center variation for the decision to evacuate the hematoma was observed (p = 0.01). Most pronounced was that 1 out of 7 (14%) neurosurgeons in one region chose a surgical strategy compared with 9 out of 10 (90%) in another region for the same scenario. In conclusion, variation exists in the neurosurgical management of TBI within an otherwise homogeneous setting. This variation supports the methodology of the international Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) initiative, and shaped the Dutch Neurotraumatology Quality Registry (Net-QuRe) initiative.
Introduction
C
When confronted with a patient with TBI and an accompanying ASDH, (neuro)surgeons are faced with several management dilemmas. The first and most challenging question is whether or not emergency surgery is indicated. The decision whether to evacuate an ASDH is based on a number of factors including the patient's age, Glasgow Coma Score (GCS), pupillary status, comorbidities, CT findings, and whether or not there is subsequent neurological deterioration. 4 Prompt surgical evacuation can successfully decrease mortality, but it is also known that despite surgical and intensive care treatment, many patients die or have an unfavorable functional outcome. 5 –8 On the other hand, a substantial portion of patients managed conservatively may have long-term favorable outcomes. 9 –11
The second question is whether evacuation of the hematoma should be accompanied by a bony decompression (a decompressive craniectomy [DC]). This decision seems to be mainly influenced by the following factors: observation of brain swelling during the surgery, intuitively expected secondary brain swelling by the treating clinicians (neurosurgeon, neurologist, or intensivist), medically intractable intracranial hypertension in the course of intensive care treatment, presence of penetrating (blast) brain injury, or simply, the hospital's protocol. 4,12,13 The known complications of decompressive surgery have to be balanced against the risk of uncontrolled brain swelling. 14,15
Ethical considerations complicate these decisions even more. Treatment decisions do not merely depend on efficacy based on mortality and functional outcome, but should also consider patient autonomy and incorporate perceived cognitive and somatic disability. Evacuation of the hematoma can be life-saving, but at the same time may lead to survival of a patient with a poor quality of life (QoL) or even absence of autonomous cognitive functioning and rational thinking. 16,17
In addition, these complicated decisions often have to be made in far from ideal conditions, constrained by time, and with incomplete information of patients' medical history. And because of the 24/7 occurrence of these traumas, often at difficult moments, such as in the middle of the night or on a weekend when regular consultation between senior staff and colleagues is difficult, important treatment choices frequently have to be made by one medical expert, mostly the neurosurgeon on call.
Society, and, therefore future patients in particular, will have the opinion that these difficult decisions in TBI management follow protocolled schemes and algorithms, thereby excluding doubt. The contrary of this assumption might, however, be more accurate. Surgical decision making is hampered by the lack of evidence-based selection criteria as a consequence of the absence of robust scientific grounds for surgical indications. 18 The most recent and most broadly known guidelines, The Brain Trauma Foundation (BTF) guidelines on the surgical management of ASDH 4 are deduced from studies with a maximum of level 3 evidence. Since then, the only study exceeding this level 19 has also not led to clearly defined surgical indications for procedures for patients with an ASDH. Generally, in TBI, there is a lack of high quality evidence relating surgery to outcome, mostly as a result of methodological constraints. 20,21
Therefore, confronted with a patient with a traumatic ASDH, clinicians have to deal with multiple clinical and radiological variables, in a very limited time frame and with a shortage of data or predictive outcomes. In this setting, the training background of the trauma team, the culture of the way treatment is being performed in that particular hospital, and the intuition of the neurosurgeon on call could be the most important factors that predict surgical decisions. How this echoes into current practice patterns with possibly variation in TBI management protocols has been scarcely investigated.
Hypothetically, no large difference in background and university training of neurosurgeons exists in Belgium and The Netherlands and, therefore, a low practice variation is to be expected. So far, no study has evaluated if this varying trauma management could also be the result of a variable view among neurosurgeons.
Therefore, we performed an online questionnaire study with questions on the clinical management of hypothetical cases, based on real patients with an ASDH, to determine whether variability in view exists among neurosurgeons on treatment of the ASDH, and which potential factors might influence surgical decision making, by presenting cases that varied with regard to the patient's age, severity (in GCS), thickness of the hematoma, and mass effect. The study was conducted in this area with the global goal of evaluating the differences in healthcare provider profiles in a hypothetically homogeneous area.
Methods
The Netherlands and Belgium are small countries with high population densities. Neurosurgical care for patients with TBI is provided at 11 level I trauma centers, serving separate areas according to regional referral policies. Acute trauma care is uniformly organized for all patients, with equal distribution of resources among hospitals. Almost all inhabitants (97.7%) are within 30 min reach from a trauma center (Fig. 1).
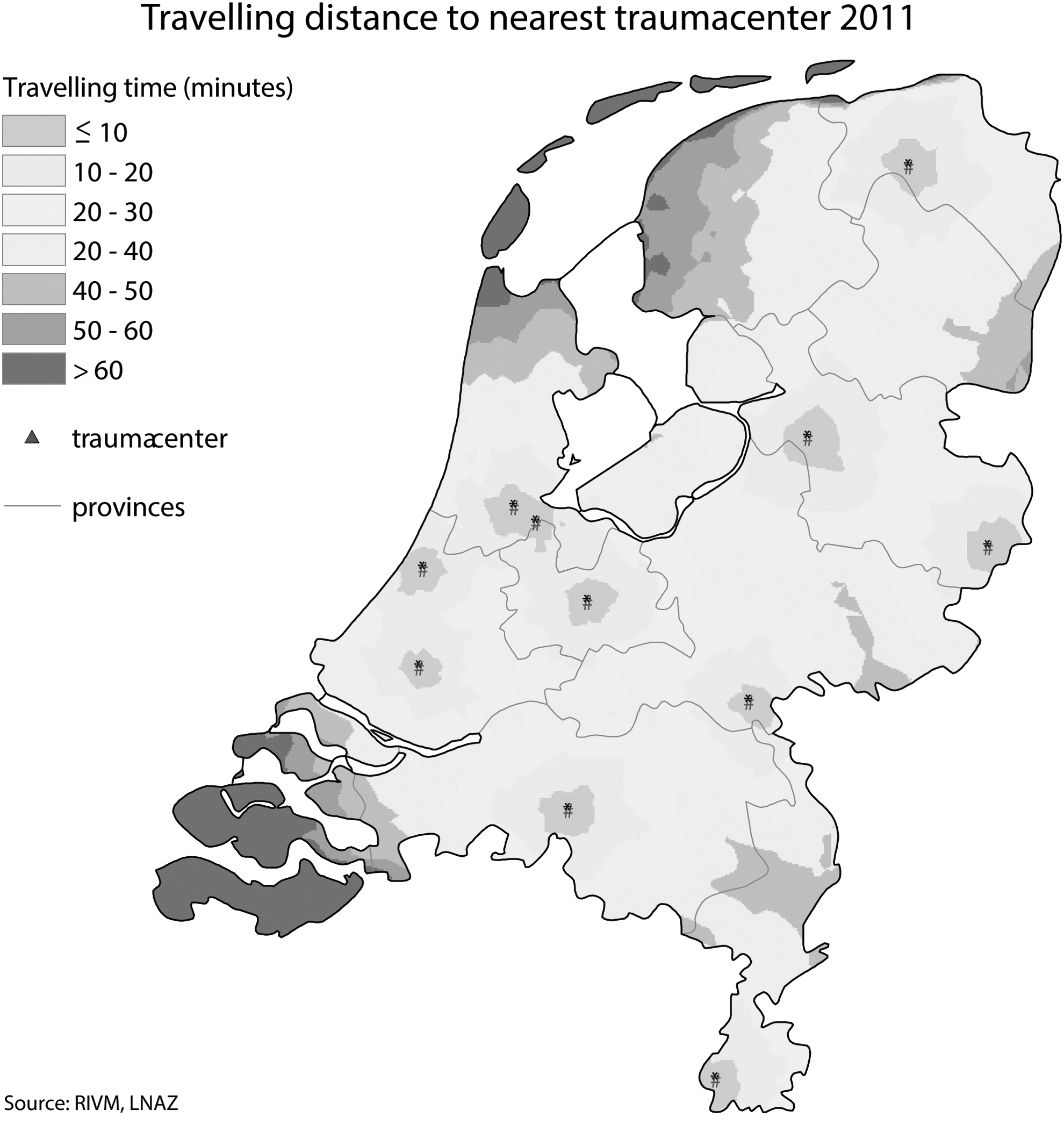
Average traveling time to a trauma center in the Netherlands.
Regular day-to-day cases with TBI and CT brain abnormalities suspected of ASDH were selected. The medical history and CT scans of these patients with traumatic ASDH were retrieved from the medical records of Leiden University Medical Center, Medical Center Haaglanden, and University Hospitals Leuven. We reviewed these cases and selected six cases, based on individual variability among patients, with different medical histories, based on severity, age, and duration between the accident and presentation to the hospital (Fig. 2). In order to examine potential variation in treatment, we selected four cases that evoked discussion a priori in the author group and two cases that did not (as a control group). Cases 1, 2 (control), and 3 represented severe and moderate TBI; that is, GCS 3–12, and cases 4, 5 (control), and 6 represented mild TBI; that is, GCS 13–15. The cases were presented in a fixed random order (i.e., equal for every respondent). The provided information per case consisted of the clinical characteristics depicted in Figure 2 and three axial CT coupes (one of which is shown in the figure). In Table 1 the questions regarding these cases are listed.
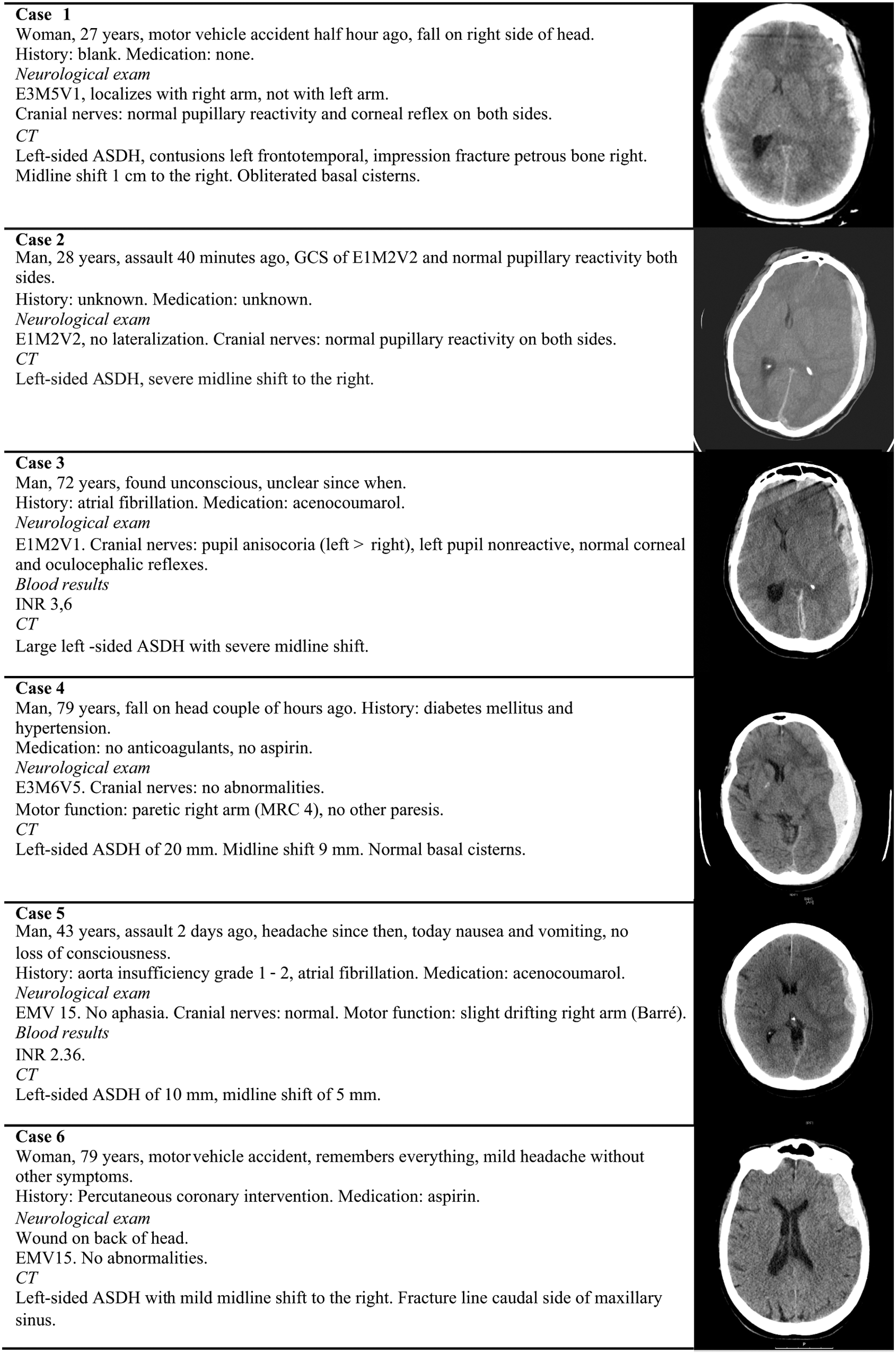
The six case vignettes and the accompanying CT scans.
Numbers do not add up because some respondents did not answer.
For cases 1, 2 and 3, the respondents answered that they would perform a decompressive craniectomy dependent upon intraoperative swelling. For cases 4, 5, and 6 the respondents would start dexamethasone and/or would perform a burr hole drainage at a later stage.
DC, decompressive craniectomy; ICP, intracranial pressure.
Dutch and Belgian neurosurgical department chiefs were asked by email whether we could send them a survey on operative management of the traumatic ASDH to their staff members. An invitation for the online questionnaire was subsequently sent to the staff clinicians, fellows, and chief residents working in the responding neurosurgical departments. The online survey was made and disseminated using the web survey tool SurveyMonkey (SurveyMonkey Inc., Palo Alto, CA,
Collected variables for the neurosurgeon were age, location of residency program, current clinical department, and practicing time (time since finishing residency). The various treatment options were analyzed for each case in general (all neurosurgeons). Whether the responders would have operated or not was also analyzed per center (or geographical region) if more than half of the employed staff clinicians responded. The question of whether to combine the evacuation with a decompressive procedure was also regionally analyzed, but only for the severe TBI cases (1, 2, and 3).
Statistical analysis
Because the outline of this study was descriptive, only a few statistical analyses were employed. Statistical comparisons were limited to the analysis of regional variation using the χ2 test and Fisher's exact test when appropriate. For statistical analysis, SPSS 20.0 (IBM, Chicago, Il, USA) was used. P values <0.05 were considered of statistical significance. The missing values (unanswered questions) for all questions were accepted up to 4% for all questions. Missing data were left out, and observed data were analyzed unless stated otherwise.
Results
Neurosurgeon's characteristics
The survey was completed by 60 respondents (53 neurosurgeons and 7 chief residents) out of a total of 93 invitations sent out (response rate 65%). Of the respondents, 43 work in the Netherlands and 17 in Belgium. The responding neurosurgeons work in, respectively, Amsterdam, Enschede, Leiden/The Hague, Nijmegen, Rotterdam, Tilburg, Antwerp, Brussels, or Leuven. Three clinicians did not report their center. The number of clinicians per center is kept anonymous. The respondents had a mean age of 44 years (range 30–67) with a median time since finishing residency of 12 years (Table 2).
IQR, interquartile range.
Strategy for patients with severe TBI and ASDH
For patients with severe TBI and ASDH (cases 1, 2, and 3) there was variation in the decision to surgically evacuate the hematoma or not; respectively 88%, 100%, and 77% answered “yes” to the question “would you operate or not?” and 23%, 8.3%, and 28%, respectively, answered “yes” to the question “randomize or not?” (Table 1). The question “DC or not?” resulted in, respectively, 74%, 67%, and 17% anwering “yes,” indicating variation in type of surgery per case. In addition, respectively, five (9.4%), six (10%), and two (4.3%) would choose to perform a DC intraoperatively only when the brain was considered to be swollen. For all other neurosurgeons, a craniotomy was the preferred strategy. For the question “intracranial pressure [ICP] measurement?” respectively, 72%, 82%, and 43% of neurosurgeons answered “yes.” For case 1, all other neurosurgeons answered “no,” except for eight neurosurgeons (13%) who chose to place an ICP monitor dependent upon intraoperative brain swelling. For cases 2 and 3, all other neurosurgeons did not choose to place an ICP sensor.
Strategy for patients with mild TBI and ASDH
For the patients with mild TBI and ASDH (cases 4, 5, and 6) there is considerable variation in the decision to surgically evacuate the hematoma or not (Table 1; “operate or not?” respectively, 68%, 5.0%, and 5.0% “yes” answers; positive incentive for randomization, respectively, 48%, 40%, and 20%). DC was never chosen in mild cases. ICP measurement was chosen in three mild TBI cases (5.0% for case 4).
Indications for surgery
For cases with severe TBI, the main reasons for surgery for the ASDH were “neurological condition” and “mass effect.” For the operated mild TBI case, “hematoma size” was the most important variable for the decision to operate (Fig. 3).
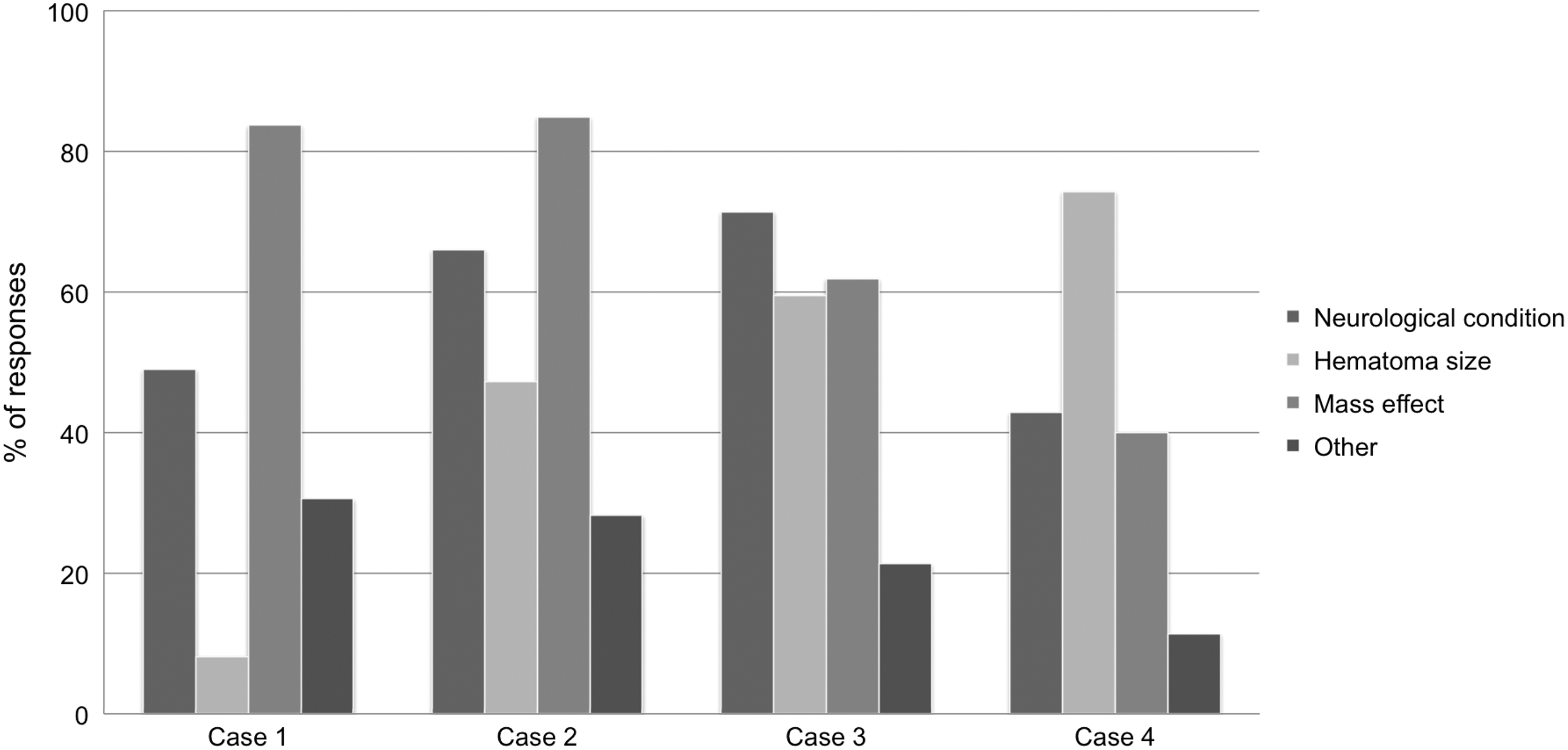
Graph illustrating the reason(s) for evacuation of the acute subdural hematoma, in percentages of responses (proportions). The respondents had the choice to give multiple answers per case. Cases 5 and 6 were not included, because a minority of surgeons chose to operate (see Table 1). The numbered cases refer to the cases shown in Figure 2.
Age and practice variation
There was no association between age and tendency to operate for any of the six cases individually or overall (Table 3).
Five respondents did not report their ages.
Regional variation
Region was associated with the decision to evacuate the hematoma or not (Table 4). For case 1, the proportion of surgical strategies did not differ among regions. For case 3, neurosurgeons in regions A and B were less aggressive, although not significantly, with regard to evacuating the hematoma, than those in regions C, D, and E. For case 4, there was a significant association between region and the decision whether to operate or not. Most notably, 1 out of 7 (14%) of neurosurgeons in one region chose a surgical strategy compared with 9 out of 10 (90%) in another region for this case vignette. The intra-center variability, that is, among neurosurgeons within a center, was most pronounced for region B, as can also be deduced from Table 4. Lastly, there seemed to be a moderate regional variation for the decision to combine the primary evacuation of the hematoma directly with a DC: in case one 57% of region B (n = 7) would perform a primary DC compared with 100% of region C (n = 16).
Discussion
Remarkably, and in contrast to the authors' hypothesis, this study suggests that standard treatment of (severe) TBI is highly variable because of a differing view on neurosurgical management despite the small size of the countries studied, dense population, and similar training curricula of trauma team physicians.
The survey results show that surgical decision making for patients with ASDH varies considerably in the Dutch-speaking part of The Netherlands and Belgium. Practice variation in the treatment of ASDH among countries and within large countries such as the United States is probable, but was not suspected within small countries among hospitals or even among neurosurgeons. The variation in neurosurgical management among regions and among neurosurgeons is quite impressive, and cannot be explained by the lack of evidence alone. Ethical considerations, that is, personal opinions about value of a meaningful life from a humanistic perspective, probably play an important role. It could be true that the reasons and predictions of clinicians in charge of TBI patients, driving life and death decisions, and, similarly, how well a neurosurgeon or neurologist can actually predict the outcome, have a profound impact on the prognosis of TBI patients. Therefore, we feel that the different treatment strategies, reflected by the differing opinions in this study, should be related to the true outcome, which can best be challenged by a comparative observational study of the different strategies with a comprehensive assessment of the long-term outcome (CENTER-TBI and Net-QuRe).
Specifically, this study shows that there seem to be two groups of TBI-ASDH patients that pose a challenging problem in surgical decision making, namely 1) patients with slight decrease in consciousness, that is, mild TBI, combined with a large hematoma, and 2) elderly patients with a seemingly poor prognostic profile. These two groups will be discussed separately. A most remarkable finding was the regional variation (Table 4), which forms an important basis for future research on this subject and will be discussed subsequently.
Mild symptoms but large ASDH
The patients with a slight decrease in consciousness and a large ASDH (thickness >10 mm), such as case 4, appear to be a clinical challenge, because there was a broad variation in the decision whether to operate or not, as well as a high incentive to randomize. Presumably, neurosurgeons in favor of evacuation of the subdural hematoma estimate that acting too slowly when there is a large ASDH leads to neurological deterioration or death. Their suspicion is backed by the BTF guideline, which was devised in 2005 by an international panel of experts, which states that every ASDH with a thickness >10 mm and a midline shift over 5 mm should be evacuated as soon as possible, irrespective of neurological condition. 4 On the other hand, surgeons in favor of a conservative strategy do not want to expose the patient to the risks of a craniotomy without a more precise estimation of the chance of neurological deterioration when withholding an operation. It can be argued that the guideline and the evidence so far should not guide treatment, because good quality comparative studies are lacking. Specifically, the reviewed studies of the BTF guideline were of a low level of evidence, were retrospective, used small or selected study populations, and had been performed >10 years earlier. Since then, the only study exceeding this level is an Austrian prognostic study. 19 Unfortunately, this study included patients with an ASDH caused by severe TBI, whereas patients with an ASDH caused by mild or moderate TBI were not analyzed. This group represents up to 54% of patients with an ASDH. 9 Consequently, these results have not led to a clearly defined subset of surgical indications for procedures for patients with an ASDH.
Elderly patients with a poor prognosis
The second category of ASDH patients that forms a clinical dilemma is the prognostically unfavorable group of the elderly patient with severe TBI (as presented in case 3). Importantly, this clinical dilemma will only become more relevant, because the number of elderly patients with a TBI is rapidly increasing 22 and, specifically, because subdural hematomas are more frequent in older patients. 23
Treating neurosurgeons choose not to operate because they believe that the outcome will still be unfavorable if they operate. On the other hand, the reason to perform surgery could be that a neurosurgeon believes that every patient deserves a chance to survive, however unlikely that may be. This tendency to act in severe TBI cases especially concerns young patients. In elderly patients, some neurosurgeons are more reserved, and abstain from cranial surgery, as is illustrated in case 3, probably because of an estimated poor prognosis. To understand the variation in surgical decision making is to understand the different metrics used to objectify the outcome of patients. Clearly, the estimation of an unfavorable outcome or prognosis critically depends upon how a worthwhile outcome is valued according to the treating neurosurgeon, trauma surgeon, intensivist, or neurologist. Although functional outcome scales are generally used to determine effectiveness in neurotraumatology studies (i.e., the extended Glasgow Outcome Scale [GOSE]), neurosurgeons might consider other factors in the clinical setting. Often the conceptual issue QoL is routinely employed in clinical setting, especially in talking about the expected outcome of patients with a severe TBI. The neurosurgeon might estimate that the life that will be saved is not worth living or will result in a low QoL, and, therefore, an evacuation is not performed.
In this context, it is interesting to see how a validated QoL instrument performs in ASDH patients. Therefore, we performed a 4 year cohort study in Leiden and The Hague in which it was shown that ASDH patients with a presenting GCS >12 do not differ in their long term QoL (as measured by the Qolibri scale 24,25 ) from surviving ASDH patients with a presenting GCS <9. 26 This finding relates to the disability paradox, in which patients with severe disease or disability do not necessarily report a poor QoL. 27
Surgical decision making in ASDH
Making decisions under uncertainty, especially when time constrained, as is the case with patients with traumatic ASDH, is susceptible to bias, 28 and, therefore, can lead to practice variation. Analyzing the factors associated with this variation will let us understand how the decisions are made and can be improved. The challenges in understanding surgical decision making have been described for patients with spontaneous intracerebral hemorrhage. 29 Each of these issues can also more or less hamper surgical decision making in traumatic ASDH. Explicitly, in this investigation, evidence is found for region as an important aggregating factor for the variation in surgical care. The most likely explanation for this result is a differing practice culture among institutions and difference in the training backgrounds of neurosurgeons.
Also, we will elaborate on a possible explanation for the discrepancy in the presented variation between severe and mild cases. There was a higher positive incentive for randomization in cases with mild symptomatology (4, 5, and 6) than in severe cases (1, 2, and 3), possibly reflecting more uncertainty with regard to mild/moderate TBI and ASDH. However, although the percentages of “yesses” for surgery in cases 1, 2, and 3 were relatively high, it is important to realize that variation exists even for severe neurotrauma cases, in which the decision of whether to operate or not often is a matter of life or death. An important explanation could be that neurosurgeons are more convinced of the merits of rapid surgical evacuation in severe cases. In part this might also be explained by a human instinct to act or do something for a patient with a life-threatening condition.
Regional variation in the literature
Although no similar survey has been conducted, other studies have shown that variability in treatment of TBI exists. Rayan and coworkers showed that in only 17% of a random sample of (brain) trauma patients was care delivered according to the BTF guidelines, 30 suggesting a variable approach. In addition, in an international survey, it was shown that there was a difference in point of view among neurosurgeons with respect to combining the evacuation of an ASDH with a DC. 31 Furthermore, inter-center variation in TBI has been shown to exist for referral policy, admission organization, and intensive care management (including ICP treatment). 32 –38
The intercenter or regional variation in surgical treatment of ASDH has not been shown in the literature. For other life-threatening or emergency disorders it has been investigated and confirmed for the ruptured abdominal aneurysm 39 and the spontaneous intracerebral hemorrhage. 40
Strengths and limitations of the study
The main strength of our study is the standardized manner of the questionnaire that was submitted to medical professionals. Although the senior authors (GdR, KHK, WCP) had a strong belief in homogeneous results across neurosurgeons and regions, the study subjects did choose quite different options for the same patient. In the aforementioned studies on current practices in TBI management, variation can be explained by other factors; for example, by different institutional infrastructure or resources, by divergent patient preferences, or by case mix.
In addition, for the first time, the pivotal clinical dilemma of whether “to operate or not” is addressed, because case vignettes are presented across the whole spectrum of TBI (GCS 3–15). Other studies focus on how care is provided for certain patient subgroups; that is, those with large ASDHs and/or severe TBI. Hence, the main approaches that are evaluated involve managing high ICP with DC. 31,41 Therefore, our study provides insight into real-life situations in which neurosurgeons are confronted by ASDH patients with heterogeneous clinical and radiological factors.
A very important but inevitable limitation of this study is its setup as a survey, wherein the actual real-life clinical setting is lacking. In the clinical setting, the studied decisions often have to be made in far from ideal circumstances, with potentially fatal consequences. In contrast, the decisions in this questionnaire are purely complicated by patient characteristics. Nonetheless, although it is acknowledged that this lack of real-life conditions could influence every respondent differently, the main conclusion about variation in ASDH management is most likely justified.
Future direction: Comparative effectiveness research (CER)
An explanation for the apparent lack of a high level of evidence for surgical management for TBI is the difficulty of performing randomized clinical trials. Generally in TBI research, the heterogeneous study population of TBI; that is, the multitude of patient characteristics and treatment variables, together with small patient numbers, make powering clinical trials problematic 21 and, therefore, requires an extensive investment of time and money. Specifically for efficacy research of surgical strategies, randomizing surgical treatments for TBI is difficult to perform because of the ethical concerns of withholding a potentially lifesaving procedure. In the presented study, this is reflected in the low motivation to randomize severe TBI cases. And even if a trial succeeds, it regularly has limited external validity, because the treatment effect has been evaluated in certain subgroups, with management protocols that are sometimes difficult to replicate in the whole population. The randomized controlled trials (RCT) on the surgical treatment of TBI, the Decompressive Craniectomy in Patients with Severe Traumatic Brain Injury (DECRA) study 15 and the Surgical Trial in Traumatic Intracerebral Haemorrhage (STITCH-Trauma) 42 trial are examples illustrative of these methodological difficulties.
Because of these methodological challenges, the focus of much TBI research in the last decades has been on suggestions for optimizing RCT design and new study designs in TBI.
2,3
A promising approach could be the so-called “comparative effectiveness research” (CER). In this design, the heterogeneity and variability, which trouble RCT, are accepted and exploited to study the effectiveness of treatments as they occur in real-life practice. This CER analysis of (surgical) treatment for TBI is currently one of the goals of a Dutch initiative called Net-QuRe and an international research initiative called CENTER-TBI of which the authors are scientific participants (
There is a large variation in management approach for the traumatic ASDH in a medically uniformly trained European region: The Netherlands and Belgium. Interestingly, there was a regional variation in a surgical versus conservative approach. Ultimately, this variation in management should be exploited in a comparative effectiveness study.
Footnotes
Acknowledgments
The authors thank Dr. Johannes Van Loon and Prof. dr. Bart Depreitere (neurosurgeons, Department of Neurosurgery, University Hospitals Leuven, Leuven, Belgium) for their involvement in case selection, all Dutch and Belgian neurosurgeons who participated in filling out the questionnaire, and Dr. Carmen L. Vleggeert-Lankamp (neurosurgeon, Department of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands) for critical appraisal of the first draft of our manuscript. This work was supported by The European Union seventh Framework Program (grant 602150) for Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) and Hersenstichting Nederland (Dutch Brain Foundation) for Neurotraumatology Quality Registry (Net-QuRe).
Portions of this work were presented at the 11th Symposium of the International Neurotrauma Society, Budapest, Hungary, March 19–23, 2014.
Author Disclosure Statement
No competing financial interests exist.