
Abstract
Diffuse axonal injury (DAI) is an important cause of morbidity in patients with traumatic brain injury (TBI). There is currently no simple and reliable technique for early identification of patients with DAI, or to prognosticate long-term outcome in this patient group. In the present study, we examined acute serum concentrations of neurofilament light (NFL) in nine patients with severe TBI and DAI using a novel ultrasensitive single molecule array (Simoa) assay. The relationships between the NFL concentrations and MRI in the acute stage as well as clinical outcome and magnetic resonance diffusion tensor imaging (MR-DTI) parameters at 12 months were analyzed. We found that the mean NFL concentrations among the patients displayed a 30-fold increase compared with controls, and that NFL completely discriminated between the patients and controls. We also found a relationship between serum NFL and MR-DTI parameters, with higher NFL concentrations in patients with higher trace (R2 = 0.79) and lower fractional anisotropy (FA) (R 2 = 0.83). These results suggest that serum NFL may be a valuable blood biomarker for TBI, reflecting the severity of DAI.
Introduction
D
There is a lack of reliable techniques to identify and quantify DAI in TBI patients. Conventional neuroimaging such as CT is considered inadequate for the evaluation of DAI, and standard MRI techniques lack sensitivity and are, therefore, criticized for underestimating the extent of injury. 5 Magnetic resonance diffusion tensor imaging (MR-DTI) is increasingly used to detect DAI. DTI can indirectly evaluate the integrity of white matter tracts by measuring water diffusion, its directionality in three dimensions, and the diffusion anisotropy. 6 A large number of studies have shown that DTI can be used to detect alterations in the white matter ultrastructure after TBI (for a recent review see Studerus-Germann and coworkers 7 ). However, MR-DTI is still mainly used in research studies and not in clinical routine. Further, it is not known how sensitive MR-DTI is in detecting DAI in mild TBI cases, and the technique has not been cross-validated against postmortem histology measures of axonal injury in humans. The analysis often needs time-consuming manual calculations, different hospitals use different methods for analysis, and it is difficult to compare DTI parameters among research groups.
The search for a useful biomarker has been an alternative way to try to diagnose and quantify DAI. An ideal blood biomarker should have increased serum levels in the acute stage related to TBI-induced DAI and persistent brain dysfunction. Further, because DAI by definition involves damage to the long myelinated white matter axons, neuronal proteins enriched in these structures are top candidates as fluid biomarkers. A number of proteins have been evaluated as candidate blood biomarkers for TBI but none has so far proved to be of prognostic value regarding DAI.
NFL (neurofilament light) protein is an important structural protein of the axonal cytoskeleton. 8 Upon axonal injury, NFL leaks from disrupted axons into the brain interstitial fluid, cerebrospinal fluid (CSF), and blood. In the present prospective longitudinal study, we have examined NFL as a potential blood-based biomarker for DAI using an ultrasensitive single molecule array (Simoa) assay in a cohort of patients with DAI, and compared it with the 12 month outcome and MR-DTI parameters.
Methods
This study was approved by the Regional Ethical Review Board at the University of Gothenburg, and informed consent was obtained from all participants or their next of kin. All patients were referred to Sahlgrenska University Hospital during the period June 2006 through September 2009, and had sustained TBI. Patients were included based on the criterion that DAI had been suspected because of affected consciousness and/or focal neurological symptoms without an obvious explanation seen on the CT scan of the brain. On admission, the initial level of consciousness was assessed using the Reaction Level Scale (RLS). 9 The RLS can be translated to the Glasgow Coma Scale (GCS) and the translated GCS is presented here. 10 The type of trauma was also recorded.
The extended Glasgow Outcome Scale (GOSE) was used for global evaluation of outcome. 11 The assessment of GOSE scores was based on interviews with the patients or their next of kin by a nurse at 12 months post-injury.
The first MRI was performed within 9 days (range 4–9 days) post-injury, and sequences including T1, T2, T2*, and fluid-attenuated inversion recovery (FLAIR) were analyzed by a radiologist (M.M.), and the presence of signs of DAI was classified according to Adams and coworkers.
12
The follow-up MRI was performed at 12 months post-injury and for these examinations, the DTI parameters were analyzed. MR-DTI was performed on a Philips Gyroscan Intera 1.5 T, release 9. The DTI method used was high angular resolution diffusion imaging (HARDI) (Philips, Eindhoven, the Netherlands). For the DTI analysis, the corpus callosum was chosen for study in this investigation as it is prone to DAI,
12
and it is anatomically easy to define using MR-DTI. Fiber tracking was performed using the fiber assignment by continuous tracking (FACT) algorithm in DTIStudio V 2.4 (Johns Hopkins Medical Institute, Laboratory of Brain Anatomical MRI,
Blood samples from the patients were obtained within 6 days post-injury, as well as from 22 healthy age-matched controls. Serum NFL concentrations were measured using an ultrasensitive Simoa assay as previously described. 15 S100 calcium-binding protein B (S100B) concentrations were measured on the Cobas e601 instrument using the Elecsys S100 test (Roche Diagnostics, Mannheim, Germany).
Statistical analysis
The results are expressed as mean ± standard deviation. Age in the patient group and the control group was compared using a t test, NFL concentrations were compared using the Mann–Whitney U test, and DTI-parameters were analysed using Fisher's nonparametric permutation test. P < 0.05 was considered significant. The relationship between NFL concentrations and DTI parameters was explored using simple linear regression, and the goodness of fit is presented as R2 .
Results
Nine patients, seven men and two women, were included. The mean age of the patients was 40.4 years (range 19–69 years). The initial GCS scores of the patients ranged from 3 to 14. None of the patients had any intracranial mass lesions requiring evacuation that could explain their loss of consciousness.
One patient died, and the outcomes of the surviving patients, measured by the GOSE at 12 months, ranged from 3 to 6. In summary, five patients had a severe disability and three patients a disability of moderate severity. Using conventional MRI in the acute stage, all patients had signs of DAI, with a majority of patients classified as Adams' 2–3 and displaying signs of axonal injury in the hemispheres and the corpus callosum as well as in the brainstem. Clinical characteristics and the outcome scores of the patients are presented in Table 1.
Trace expressed as × 10−3 mm2/sec.
GCS, Glasgow Coma Scale on admission; GOSE, Glasgow Outcome Scale extended; Adams, classification of diffuse axonal injury based on MRI; NFL, serum level of neurofilament light protein; S100B, serum level of S-100B; FA, fractional anisotropy.
Serum NFL concentrations of the patients ranged from 87.5 to 851.6 pg/mL, and were markedly higher than serum levels in controls (10.8 ± 5.4; Fig. 1). Serum S100B concentrations of the patients ranged from 0.03 to 0.10 μg/L (reference value <0.10 μg/L).
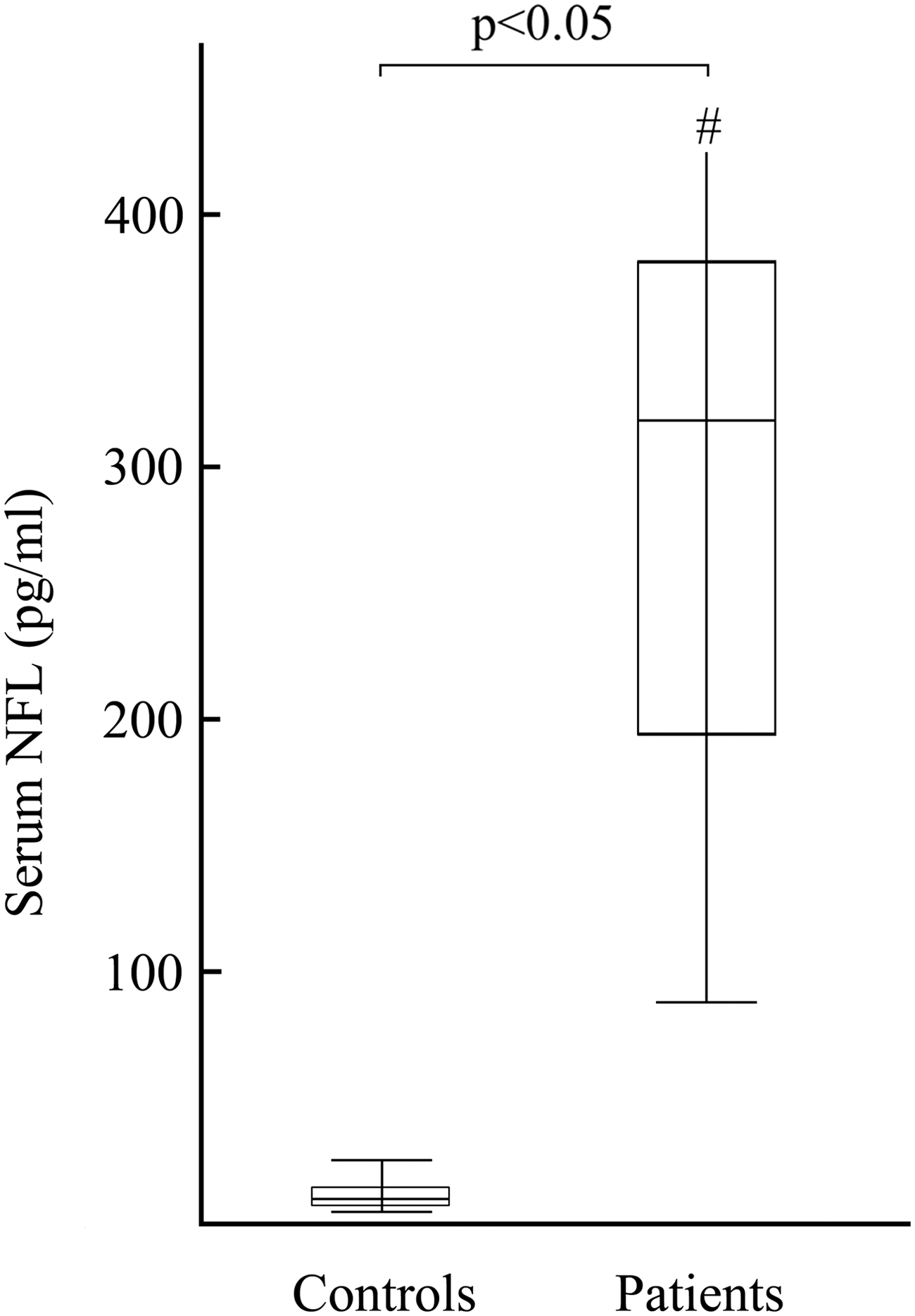
Diagram showing the levels of serum neurofilament light (NFL) for the control group and the patients. Whisker bars represent range of data; top and bottom of boxes represent first and third quartiles, respectively; midline through box represents median. # the whisker bar representing the maximum NFL level among the patients has been truncated (NFL for this patient was 852 pg/mL).
For seven patients, it was possible to analyze the MR-DTI performed at 12 months (two examinations were missing because one patient died and one examination was lost as a result of technical problems). For the diffusion parameters, a significant reduction in FA in the corpus callosum was seen compared with the controls (0.51 ± 0.07 vs. 0.62 ± 0.04) as well as a significant increase in trace (2.87 ± 0.34 vs. 2.28 ± 0.12).
When dichotomizing the patients into two groups based on their outcome at 12 months, five patients had a severe disability (GOSE 3–4) and three patients a disability of moderate severity (GOSE 5–6). The mean serum NFL concentration in the patients with severe disability was 411 ± 263 and in the patients with a disability of moderate severity it was 277 ± 80. The difference was not significant.
When plotting the acute serum NFL concentrations versus the DTI parameters at 12 months post-injury, we found a linear relationship. A positive relationship was found between trace and the serum NFL (R2 = 0.79), and a negative relationship was found between the FA and the serum NFL (R2 = 0.83; Fig. 2).

Diffusion tensor imaging (DTI) parameters at 12 months plotted versus the acute serum levels of neurofilament light (NFL). Dotted lines indicate 95% confidence interval.
Discussion
In the present prospective longitudinal study, we have examined a novel biomarker, serum NFL, in a cohort of patients with DAI. The acute serum NFL concentrations were significantly higher for patients compared with controls, and we found a correlation between the increased NFL concentrations and affected MR-DTI parameters at 12 months post-injury. S100B concentrations were not significantly increased for the patients; however, blood samples were taken 4–9 days post-injury, and it is possible that S100B could have normalized.
CSF NFL is a well-established biomarker for axonal injury, and clearly elevated concentrations are seen in patients with cerebrovascular insults and mild to severe TBI. 16,17 However, an obvious limitation of CSF NFL is the requirement for lumbar puncture. For this reason, a sensitive and reliable blood biomarker of CNS injury would be preferred. Recent developments in ultrasensitive measurement techniques have made it possible to establish a sensitive and specific NFL assay for serum and plasma measurements, 15,18 and it has been shown that serum/plasma NFL correlates with CSF NFL with a correlation coefficient of 0.89. 15
In the current study, we used this NFL assay on a cohort of TBI patients with a clinical suspicion of DAI because of loss of consciousness that could not be explained by CT findings, and signs of DAI classified as Adams' grade 2–3 on the acute MRI. The outcomes at 12 months with GOSE scores ranging from 1 to 6 indicate that the patients were severely injured.
We found that the mean NFL concentrations among the patients displayed a 30-fold increase compared with the controls, and that NFL concentrations completely discriminated between the patients and the controls. However, although it is likely that the increase in NFL is caused by DAI, it is also possible that axonal injury caused by hypoxic ischemic change and/or swelling might be reflected by the marker. Although the number of patients in our study is small, our result indicates that NFL may be a useable biomarker of TBI.
A recent study showed that measurement of another axonal protein, microtubule-associated protein tau, in interstitial fluid collected by microdialysis catheters, correlates with DTI measurements. 19 However, not only does collection of interstitial fluid require craniotomy, but tau protein also seems to be a less sensitive biomarker for mild TBI than NFL. 20,21 In the present study, we analyzed NFL in blood samples and found a relationship between the increased serum concentration and the DTI parameters. A number of studies have shown a relationship among the severity of TBI, affected DTI parameters, and clinical outcome. TBI, and especially DAI, reduces FA and increases trace, and the affected DTI parameters correlate to clinical outcome. 7,14 The positive relationship between NFL and trace, and the negative relationship between NFL and FA, indicate that serum NFL might be an indicator of the severity of the DAI.
We currently plan studies with larger number of patients to further investigate the possible role of serum NFL as a valuable biomarker in TBI. Further studies will show if NFL also is increased in patients with mild TBI, if it is specifically sensitive to DAI, and if it is directly correlated to outcome.
Footnotes
Acknowledgments
This work was supported by grants from the Health and Medical Care Committee of Västra Götaland, the Foundation for Medical Imaging in Memory of Erik Lysholm, the Swedish Research Council, the European Research Council, the Knut and Alice Wallenberg Foundation, and the Torsten Söderberg Foundation. We thank Dr. Asgeir Jakola for his support with the statistical analysis.
Author Disclosure Statement
H.Z. and K.B. are co-founders of Brain Biomarker Solutions in Gothenburg AB, a GU Venture-based platform company at the University of Gothenburg. The other authors have nothing to disclose.