
Abstract
Spinal cord injury (SCI) can cause physical disability and psychological distress; however, whether SCI is a risk factor for dementia is unclear. This study evaluated the incidence of dementia in patients with SCI. Study participants were recruited from a nationwide cohort during 2004–2007 and categorized into SCI (patients diagnosed with SCI; n = 941) and non-SCI (age- and sex-matched controls; n = 5060) cohorts. Each participant was followed for 7 years until diagnosis of dementia or December 31, 2010, whichever occurred first. Data were subjected to Kaplan–Meier and Cox regression analyses. The incidence of dementia was significantly higher in the SCI cohort (1106 per 100,000 person-years) than in the non-SCI cohort (p < 0.001). Patients with SCI had a significantly higher risk of dementia than did those without SCI (crude hazard ratio [HR] = 2.14, 95% confidence interval [CI], 1.57–2.92, p < 0.001 vs. adjusted HR = 1.95, 95% CI, 1.43–2.67, p < 0.001). Further analysis found that there is no statistical significance of higher risk for developing Alzheimer's disease among SCI patients, but that SCI patients were at higher risk of developing other types of dementia than the control cohort (crude HR = 1.88, 95% CI, 1.33–2.63, p < 0.001 vs. adjusted HR = 1.90, 95% CI, 1.35–2.68, p < 0.001). In conclusion, patients with SCI are at high risk of dementia, and effective dementia prevention strategies are recommended for comprehensive SCI care.
Introduction
S
Dementia, characterized by global cognitive function loss, is the insidious onset of memory loss, personality changes, abstract-thinking and problem-solving ability loss, and disorientation. 9 The worldwide prevalence of dementia among elderly people (>65 years of age) is estimated to be 4.98–8.50%. In 2010, 35,600,000 people were diagnosed with dementia worldwide, and this number is estimated to nearly double every 20 years: to 65,700,000 in 2030 and 115,400,000 million in 2050. 10 Dementia deteriorates the cognitive and social functioning and interferes with the independent living of patients, and increases the burden on family members and caregivers, 11 particularly in terms of the healthcare costs. 12 Therefore, identifying potential risk factors for dementia and establishing a preventive strategy is essential for public health.
An animal study demonstrated that similar to traumatic brain injury, SCI induces chronic neuroinflammation and neurodegeneration in the brain and is associated with cognitive decline. 13 Moreover, chronic brain neurodegeneration occurs after isolated SCI (excluding concurrent brain injury); this is likely associated with sustained microglial activation mediated through cell cycle activation. 13,14 Moreover, clinical investigation also mentioned that SCI patients perceived the negative impact of cognitive functioning after in injury event, and that cognitive deficits are common among patients with acute ACI. 15 However, the correlation between SCI and dementia has not been examined in a large-scale population-based study. To clarify whether SCI is a risk factor for dementia, we conducted this retrospective large-scale population-based case–control study of patients with SCI.
Methods
Data source
The National Health Insurance Research Database (NHIRD), managed by the National Health Research Institutes, comprises the comprehensive medical claims data—including data on ambulatory care; inpatient care; pharmacy use; date of service; International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnostic codes; and claimed medical expenses—of 23,000,000 residents of Taiwan. The National Health Insurance (NHI) program was established in March 1995, and it covers >99% of the Taiwanese population. In this study, we sampled patients from the Longitudinal Health Insurance Database 2005 (LHID2005), which contains the data of 1,000,000 beneficiaries randomly sampled from the NHIRD. The NHIRD de-identifies and encrypts data, thus ensuring patient privacy and that researchers cannot trace individual patients or health service providers by using the data. Therefore, this study was exempted from a complete review by any institutional review board.
Study samples
An SCI cohort was populated using patients diagnosed with SCI (952 with SCI without evidence of spinal bone injury and 806 with fracture of vertebral column with SCI) between January 1, 2004 and December 31, 2007. To improve SCI diagnostic accuracy, only patients who received at least two consistent diagnoses (according to ICD-9-CM codes) in outpatient clinics or received a primary diagnosis of SCI during hospitalization within 1 year were selected: 1120 SCI patients were initially selected in the SCI cohort; however, 55 were excluded because of missing data or being <18 years of age; in addition, 27 were excluded because they had a previous diagnosis of dementia (ICD-9-CM codes 290, 294, and 331). Then, 1038 patients with SCI were enrolled in the SCI cohort. In the comparison (non-SCI) cohort, 5190 individuals age- and sex-matched to the SCI cohort were randomly extracted from the LHID2005 at a 1:5 case–comparison ratio. For consideration of bias caused by traumatic brain injury, we excluded 91 participants in study cohort and 106 participants in the control cohort because of previous traumatic brain injury diagnosis. And we also excluded those with the vascular dementia diagnosis (ICD-9-CM 290.4) from the SCI cohort (n = 6) and from the control cohort (n = 24). Finally, there were 941 SCI patients in the study cohort and 5060 non-SCI patients in the control cohort in this study (Fig. 1). The patients were followed for up to 7 years: from their entry date until the receipt of two consecutive dementia diagnoses (ICD-9-CM codes 290, 294, and 331.0) in outpatient clinics or one primary diagnosis during hospitalization or until December 31, 2010. Concerning mortality, mortality was defined as occurring if subjects died during the follow-up period and withdrawal from the program of NHI. However, in addition to death, withdrawal from the NHI could also apply to those resident aliens in Taiwan who returned to their country of origin as well as those who cancelled their insurance. It is difficult to define the reason of withdrawal, because an encrypted insurance database was used in this study. Based on the abovementioned reasons, subjects withdrawal applied to both the study and control cohorts.
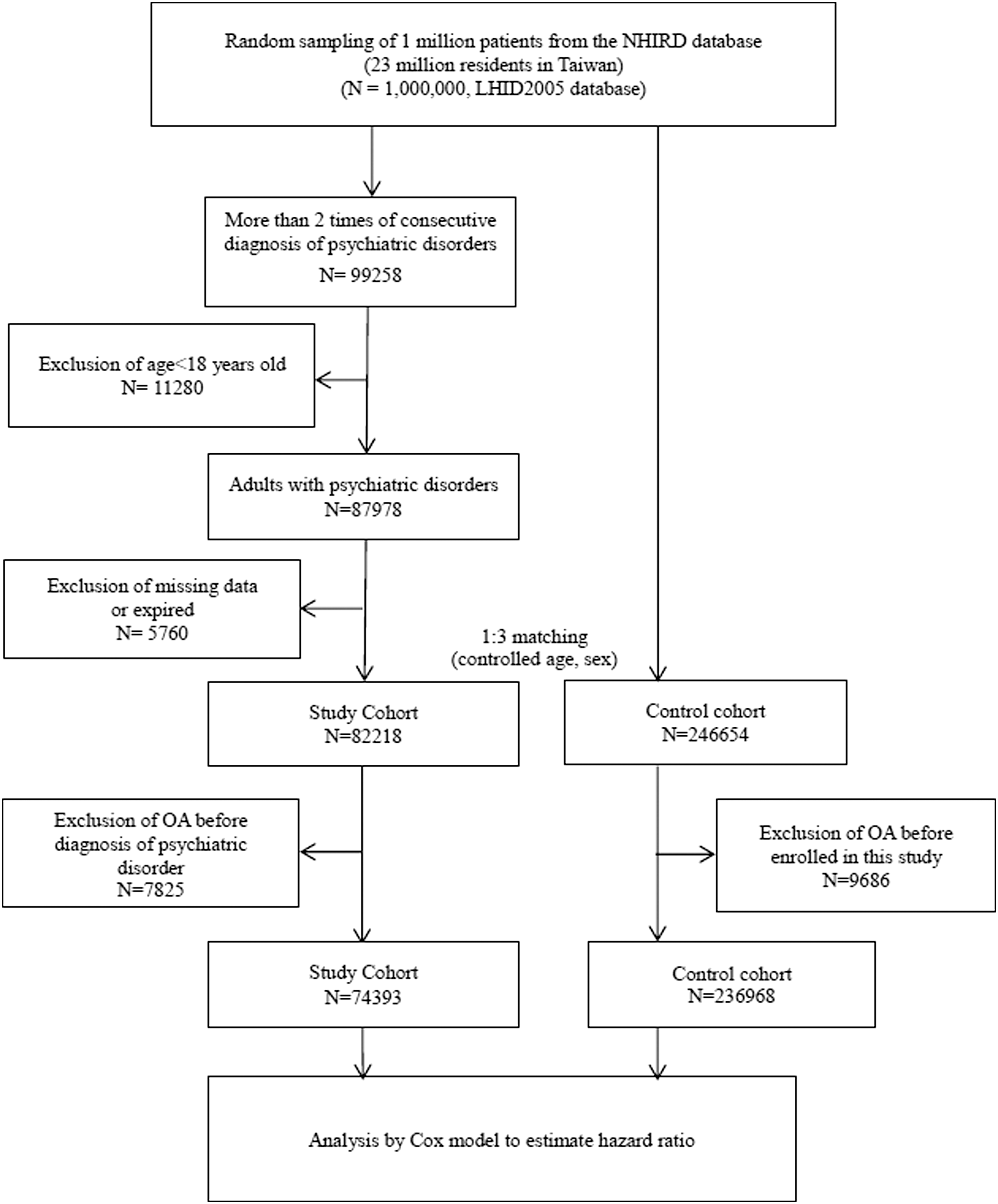
Flow chart diagram of data collection.
Baseline variables and comorbidities
For all patients, we collected data regarding baseline variables such as age, sex, urbanization level (urban, suburban, rural), monthly income (financially dependent, NT$1–20,000; NT$20,001–40,000; ≥ NT$40,001), and comorbidities such as diabetes mellitus (DM) (ICD-9-CM codes 250 and 251), hypertension (ICD-9-CM codes 401–405), hyperlipidemia (ICD-9-CM codes 272.0–272.4), autoimmune disease (rheumatoid arthritis, ICD-9-CM code 714.0; systemic lupus erythematosus, ICD-9-CM code 710.0), affective psychosis (including depression and bipolar disorders; ICD-9-CM code 296), cerebral vascular accident (CVA) (ICD-9-CM codes 430–438), and Parkinson disease (ICD-9-CM code 332). These comorbidities were chosen because some of these diseases could influence the cognitive function for SCI patients and should be taken as confounding factors for adjustment of statistical analysis.
Statistical analysis
The χ2 test was used to examine differences in demographic variables and comorbidities between the SCI and non-SCI cohorts. First, we calculated the dementia crude and adjusted hazard ratios (HRs) for up to 7 years by using the Cox model stratified by age and sex, and examined the differences in the risk of dementia between the SCI and non-SCI cohorts after adjusting for age, sex, and comorbidities. Second, in order to eliminate the bias caused by hospital clustering, we then proposed a frailty model for modeling corrections among the dementia diagnoses of hospital clusters, incorporating a random component for the hazard function to adjust for the hospital cluster random effect. For further analysis of the risk of developing different types of dementia for SCI patients, we analyzed the crude and adjusted HR of Alzheimer's disease (ICD-9-CM 331.0) and other dementias (ICD-9-CM 290, 294) separately. All data analyses were performed using the SAS statistical software (Version 9.1.3; SAS Institute, Cary, NC), and p < 0.05 was considered statistically significant.
The frailty model for hospital clusters
Let our hazard function be
Results
In total, 6001 patients (n = 941 and 5060 in the SCI and non-SCI cohorts, respectively) were sampled from the LHID2005. The prevalence of autoimmune disease, affective psychosis, diabetes mellitus, stroke, and Parkinson disease was higher in the SCI cohort than in the non-SCI cohort. And there was a higher urbanization level and monthly income for the non-SCI cohort than for the SCI cohort (p < 0.001) (Table 1). Figure 2 presents the Kaplan–Meier hazard curve for dementia in the two cohorts over the 7 year follow-up period. Log-rank analysis revealed significantly higher cumulative HRs in the SCI cohort than in the non-SCI cohort (p < 0.001).

Kaplan–Meier hazard curve for dementia in patients with spinal cord injury (SCI) and controls during the 7 year follow-up period (2004–2010).
SCI, spinal cord injury; DM, diabetes mellitus; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus.
Table 2 reveals results from incidences analyses and Cox model stratified by patient age and sex. The incidence of dementia was 1106 and 530 per 100,000 person-years in the SCI and non-SCI cohorts, respectively. In patients with SCI, the crude and adjusted HRs for dementia were 2.14 (95% confidence interval [CI], 1.57–2.92, p < 0.001) and 1.95 (95% CI, 1.43–2.67, p < 0.001), respectively.
Adjusted for age, sex, autoimmune disease, diabetes mellitus, hypertension, hyperlipidemia, coronary heart disease, stroke, affective psychoses, hypotension, and Parkinson disease.
p < 0.001.
CI, confidence interval.
Table 3 shows that the analysis frailty model for hospital clusters revealed that the crude HR for dementia in the SCI cohort compared with the non-SCI cohort during the follow-up period was 1.91 (95% CI, 1.38–2.63). After adjustment for age, sex, DM, hyperlipidemia, hypertension, autoimmune disease, affective psychosis, coronary heart disease, stroke, traumatic brain injuries, and Parkinson disease, the HR for dementia in the SCI cohort during the 7 year follow-up period was 1.94 (95% CI, 1.41–2.67, p < 0.001) compared with the non-SCI cohort, and the adjusted HR for developing dementia for affective psychosis patients was 5.19 (95% CI, 3.24–8.32, p < 0.001), and for stroke patients was 1.64 (95% CI, 1.20–2.23, p < 0.001). DM and hypertension were significant for developing dementia; however, after adjusted potential confounding factors, DM and hypertension were not significant. The cumulative HR for dementia for both cohorts is presented in Figure 3.
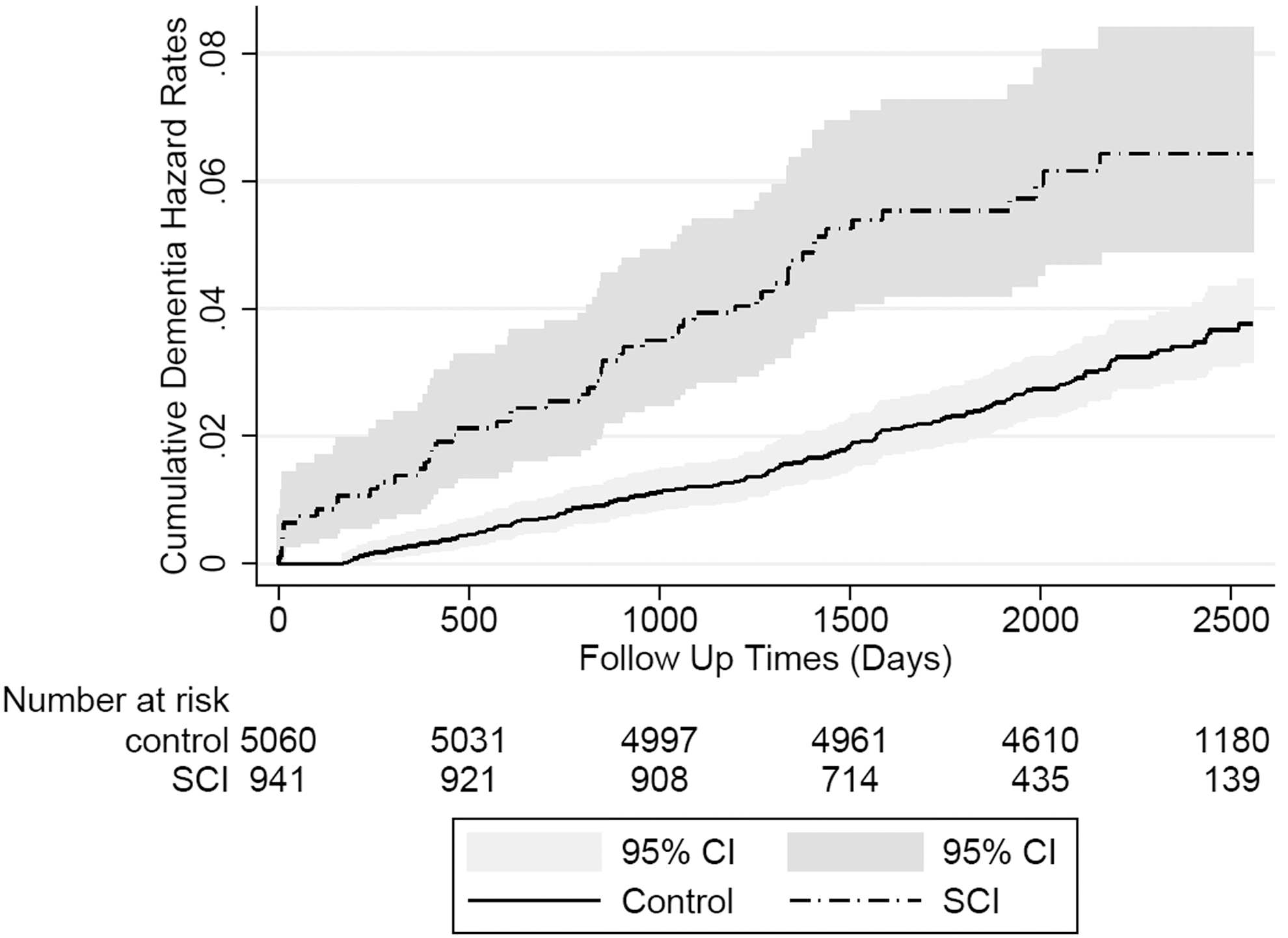
Cumulative dementia hazard rates and number at risk for dementia in spinal cord injury (SCI) and control cohorts during the 7 year follow-up period (2004–2010).
Stratified frailty model by age and sex have been considered. Adjusted HR was adjusted for multivariate model.
SCI, spinal cord injury; HR, hazard ratio; CI, confidence interval; DM, diabetes mellitus.
Table 4 reveals that the crude HR was 1.88 (95% CI, 1.33–2.63, p < 0.001) and that the adjusted HR was 1.90 (95% CI, 1.35–2.68, p < 0.001) for developing other types of dementia (excluding Alzheimer's disease) among the SCI cohort, but there was no statistical difference between the crude HR and the adjusted HR for developing Alzheimer's disease for the SCI and non-SCI cohorts.
Adjusted for age, sex, autoimmune disease, diabetes mellitus, hypertension, hyperlipidemia, coronary heart disease, stroke, affective psychoses, and Parkinson disease.
p < 0.001.
SCI, spinal cord injury; HR, hazard ratio; CI, confidence interval; ICD9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
Discussion
The present study revealed that patients with SCI have a higher risk of dementia than do those without SCI. On the basis of patient perceptions, cognitive function changes following an SCI event. 15 Further, 40–50% of patients with SCI experience different degrees and patterns of cognitive impairment. 6 This retrospective and longitudinal cohort study revealed a temporal association of SCI with dementia and that SCI is a risk factor for dementia. Our study outcome is compatible with previous clinical studies, which mention that long-term cognitive impairments can be developed frequently among SCI patients. 6,19 –22 Many previous studies used a battery of neuropsychological tests for SCI patients, and found that they had impaired performance of memory span, attention, processing speed, learning ability, and executive functioning. 6,7,15,20 –24 In addition, alternations in scalp-recorded late-component event-related potentials were found in SCI patients, and this central psychophysiological finding indicated impairments in integrative cortical/subcortical networks, which engage in stimulus detection, evaluation, and executive functioning. 22
In this study, we used the frailty model because several SCI diagnosis codes at hospitals have similar clustering tendencies, given that hospitals are naturally clustered in the LHID2005. Further, to account for the intracluster dependence and eliminate the bias caused by clustering, we used not only regression parameter estimation in the Cox model by using maximum partial likelihood estimates, but also under consider hospital cluster random effects. This led to an increase in dementia risk among patients with SCI from 1.95 to 1.94 in this study. In addition, there was a potential competing risk in elderly SCI patients because patients >70 years old were more likely to die. To adjust this potential competing risk caused by age, we further analyzed the adjusted HR for developing dementia among SCI patients comparing those ≥70 years old and those <70 years old separately. We found that when SCI patients were ≥70 years old, the adjusted HR was 1.59 (95% CI, 1.08–2.39, p = 0.018) for developing dementia compared with non-SCI patients ≥70 years old. For SCI patients <70 years old, the adjusted HR was 3.64 (95% CI, 2.08–6.37, p < 0.001) for developing dementia compared with non-SCI patients <70 years old. It indicated that younger SCI patients had a higher risk of dementia with less competing risk caused by death. Considering that the demographic variables of urbanization and social economic status could be confounding factors for the study result, we stratified the urbanization level (urban, suburban, and rural), and monthly income, and analyzed the crude and adjusted HR of dementia among SCI and non-SCI cohorts; however, there was no statistical significance in the adjusted HR between these cohorts (Table 5). It appears that these demographic variables would not influence our study outcome, which was that SCI patients were at higher risk of developing dementia than non-SCI patients.
Adjusted HR was adjusted for adjusted for age, sex, autoimmune disease, diabetes mellitus, hypertension, hyperlipidemia, coronary heart disease, stroke, affective psychoses, and Parkinson disease.
SCI, spinal cord injury; HR, hazard ratio; CI, confidence interval.
A possible mechanism underlying the high dementia risk among patients with SCI is neurodegeneration and neuroinflammation after a trauma event. Freund and coworkers conducted an MRI-based study and revealed that SCI not only influences the spinal tract but also induces progressive brain changes. Further, the authors revealed that progressive neural structure reduction in the white matter volume of the cranial corticospinal tracts and the gray matter volume of the sensorimotor cortex occurs at least 40 days after SCI. 25 Wu and coworkers also conducted SCI studies by using animal models, and demonstrated a chronic neuroinflammatory response, a characteristic similar to the neuroinflammatory process caused by a traumatic brain injury. In addition, microglial activation gene expression increased in the hippocampi of the study animals. 13,14 Microglial activation causes chronic neuroinflammation, and is associated with progressive neurodegeneration in the brain regions associated with cognitive decline, 13,14 which is a crucial pathogenic mechanism in neurodegenerative disorders. 26,27
Lack of physical activity is another possible etiology for the increased dementia risk. Impaired physical function and mobility may cause difficulty in performing physical and leisure activities, which are recommended for improving physical capacity and muscular strength. Only 50% of adults with SCI participate in leisure and physical activities such as sports and exercise. 28 Further, most patients with SCI cannot perform adequate levels of physical activity. 29 A systemic review revealed that physical inactivity is associated with an increased risk of cognitive impairment. 30 Further, a recent meta-analysis reviewed prospective studies of physical activities and dementia risk and concluded that physical inactivity is a risk factor for dementia. 31 Therefore, we hypothesized that physical inactivity is a factor contributing to dementia in patients with SCI.
In addition to physical disability, SCI can cause psychological problems such as anxiety and depressive disorders. 32,33 According to a systematic review by Craig and coworkers, 25–30% of community-residing patients with SCI experienced major depressive disorders. 33 The depression symptoms of patients with SCI were persistent, and the prevalence did not change significantly during a longitudinal follow-up study. 34 Depression among patients with SCI negatively affects community mobility and social and leisure activities, 35 potentially predisposing them to dementia. A recent systemic review and meta-analysis demonstrated that patients with a history of depression have an approximately twofold higher risk of dementia later in life than do those without a history of depression. 36 Therefore, depression among patients with SCI can be a risk factor for dementia.
Because patients with SCI have a dementia risk, establishing an effective prevention strategy and identifying the possible pathogenic mechanism of dementia is essential. In this study, neurodegeneration, decreased physical activity levels, and depression were found to be possible pathogenic factors for dementia among patients with SCI. Therefore, appropriate management of these pathogenic factors may reduce the risk of dementia after an SCI event. Moreover, increasing physical activity levels of patients with SCI can prevent dementia; high physical activity levels have been independently associated with a reduced risk of Alzheimer disease. 37 A meta-analysis investigated 15 prospective studies with a follow-up of 1–12 years, and revealed that high levels of physical activity offered 38% protection against cognitive decline, and that low to moderate exercise levels offered 35% protection against cognitive impairment. 38 In addition to decreased dementia risk, high levels of exercise can reduce symptoms of depression. 39 Similarly, depression management can improve the lifestyle of patients; both have been related to the risk of dementia in patients with SCI.
In this large-scale longitudinal population-based study, we statistically controlled for possible confounders, and revealed a temporal relationship between SCI and dementia. However, this study has certain limitations. First, the diagnosis of SCI, dementia, and other comorbidities were based on the ICD-9-CM codes from the LHID2005, the diagnostic accuracy of which affected the study results. For validating diagnostic accuracy, the Bureau of National Health Insurance (BNHI) periodically verifies and reviews charts. In addition, the BNHI claims data determine hospital reimbursement and are, therefore, validated regularly. Moreover, we only enrolled patients with at least two consecutive diagnoses of SCI. Second, patient data regarding daily physical activity, lifestyle factors (e.g., smoking and obesity), psychological conditions, education status, medication use, detailed rehabilitation intensity, and social integration after injury are difficult to obtain from the NHIRD; however, these factors may be critically associated with dementia. In addition, to improve SCI coding accuracy, we included a high number of female patients (44.3%) in the SCI cohort; hence, our study results may not concur with those of other largely male-dominated SCI cohort studies. Third, the influence of traumatic brain injury, accompanied by cervical SCI, could also be considered a potential contributing factor for higher risk of developing dementia. To control this potential bias, we adjusted for traumatic brain injury and cerebral hemorrhage-related ICD-9-CM codes. Previous studies have found that elderly patients with impaired cognitive function and dementia were at risk of sustaining falls. 40 –42 Falls are main cause of injuries, increased morbidity, institutionalization, and mortality in all older people, but particularly in those with dementia. 43,44 It indicated that patients with dementia could have higher risk of falls and therefore increase the risk of SCI. With regard to this, participants with dementia diagnosis before being enrolled in this study were excluded from both the study and control cohorts. However, there could be still some minimal cognitive impairment and dementia in patients without their having been given a diagnosis coding by a clinician in our NHIRD. Finally, the severity and functional status of patients with SCI could not be determined using the ICD-9-CM codes. The functional status of SCI patients with different severities can lead to different physical inactivity statuses and this cannot be determined by the coding system used in this study. Physical inactivity is associated with cognitive impairment and, therefore, is considered as a contributing factor for dementia, 30,31 and SCI patients with disabilities could use more medical resources, which could lead them to have a higher probability of dementia diagnosis. These limitations should be addressed in a prospective study in the future.
Conclusion
The present large-scale longitudinal population-based study revealed that patients with SCI are at a high risk of dementia. To improve the quality of care for these patients by developing a prevention strategy for dementia later in life, identifying potential predisposing factors is crucial. Additional studies exploring alternative interventions for preventing and controlling dementia progression among patients with SCI are warranted.
Footnotes
Acknowledgments
This study was based partly on data from the NHIRD, provided by the BNHI (Department of Health), managed by the Taiwan National Health Research Institutes, and supported by the National Science Council of Taiwan under grant MOST 104-2118-M-031-001. S.W.H. and H.W.L. conceptualized and designed the study, and S.W.H. drafted the manuscript; S.W.H. and H.W.L. analyzed and interpreted the data; S.W.H. critically revised the article for valuable intellectual content; T.H.L. and H.W.L. approved the article; L.C.C. provided study materials and patients; H.W.L. offered statistical expertise; and W.T.W. provided administrative, technical, and logistical support.
Author Disclosure Statement
No competing financial interests exist.